Menstrual Cycle Phases Influence on Cardiorespiratory Response to Exercise in Endurance-Trained Females

 , , , , , , , and
, , , , , , , and
Abstract
:1. Introduction
2. Material and Methods
2.1. Participants
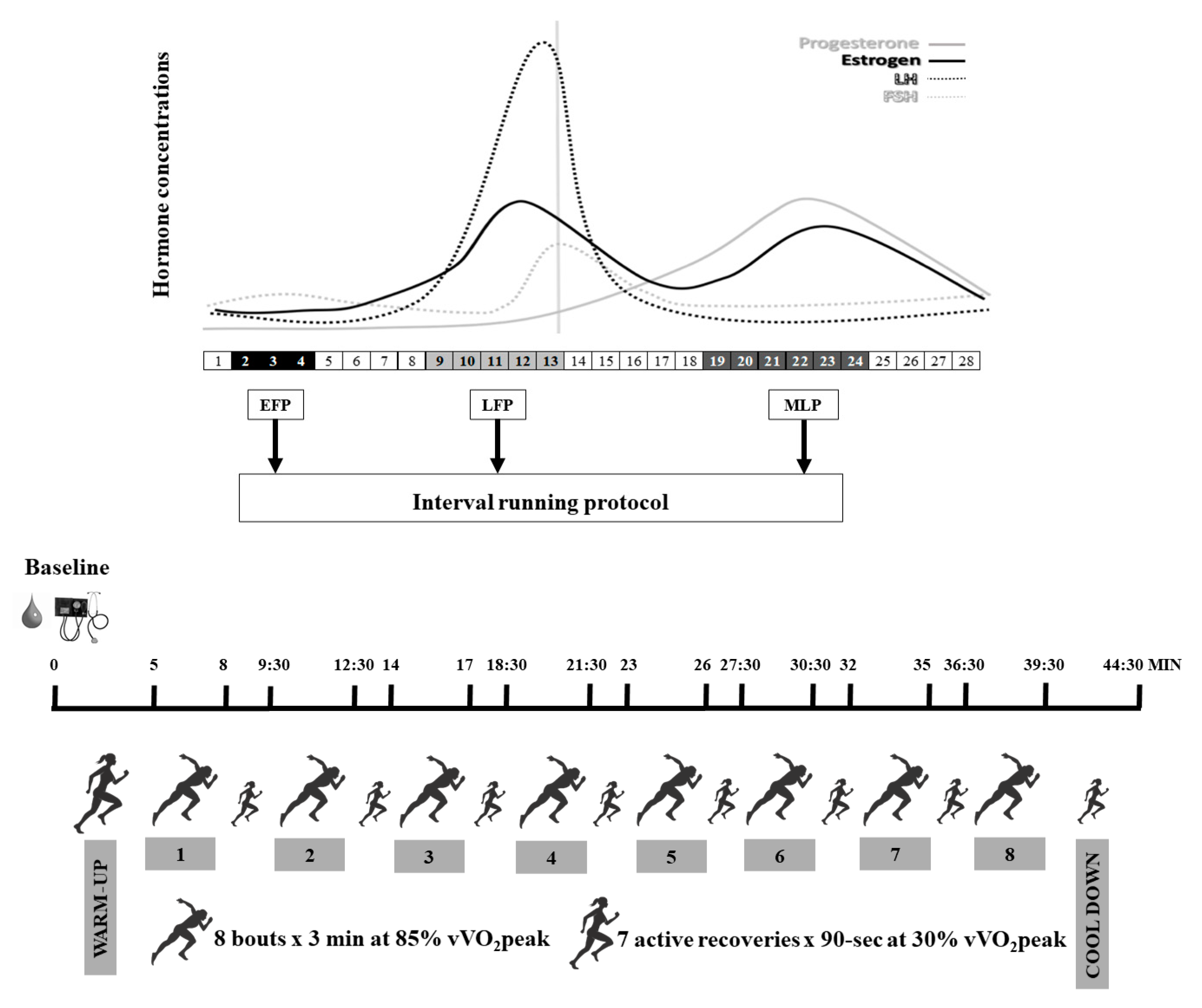
2.2. Study Design
2.3. Interval Running Protocol
2.4. Menstrual Cycle Monitoring and Phase Determination
2.5. Blood Samples Analyses
2.6. Statistical Analysis
3. Results
3.1. Baseline
3.2. Warm-Up
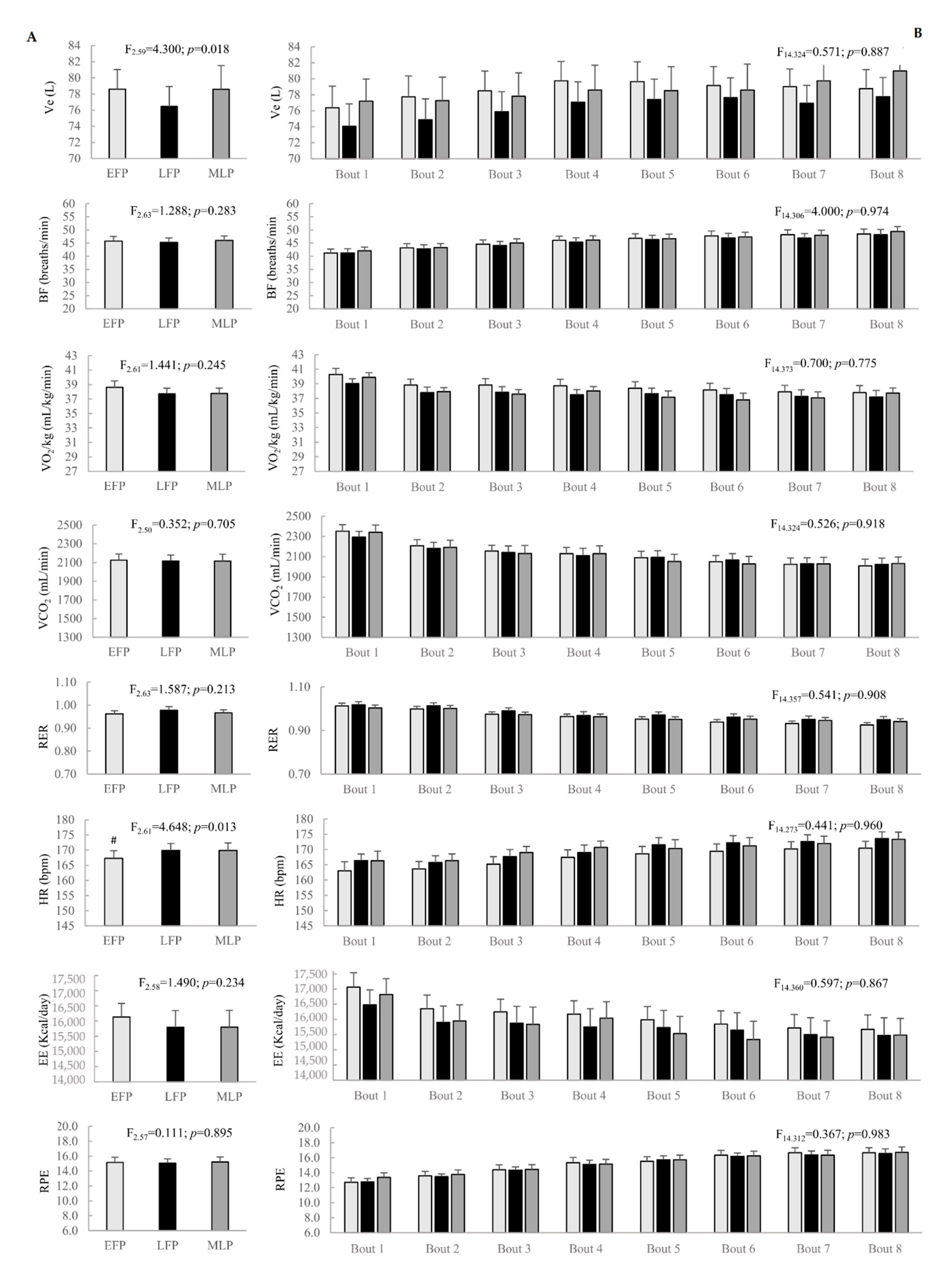
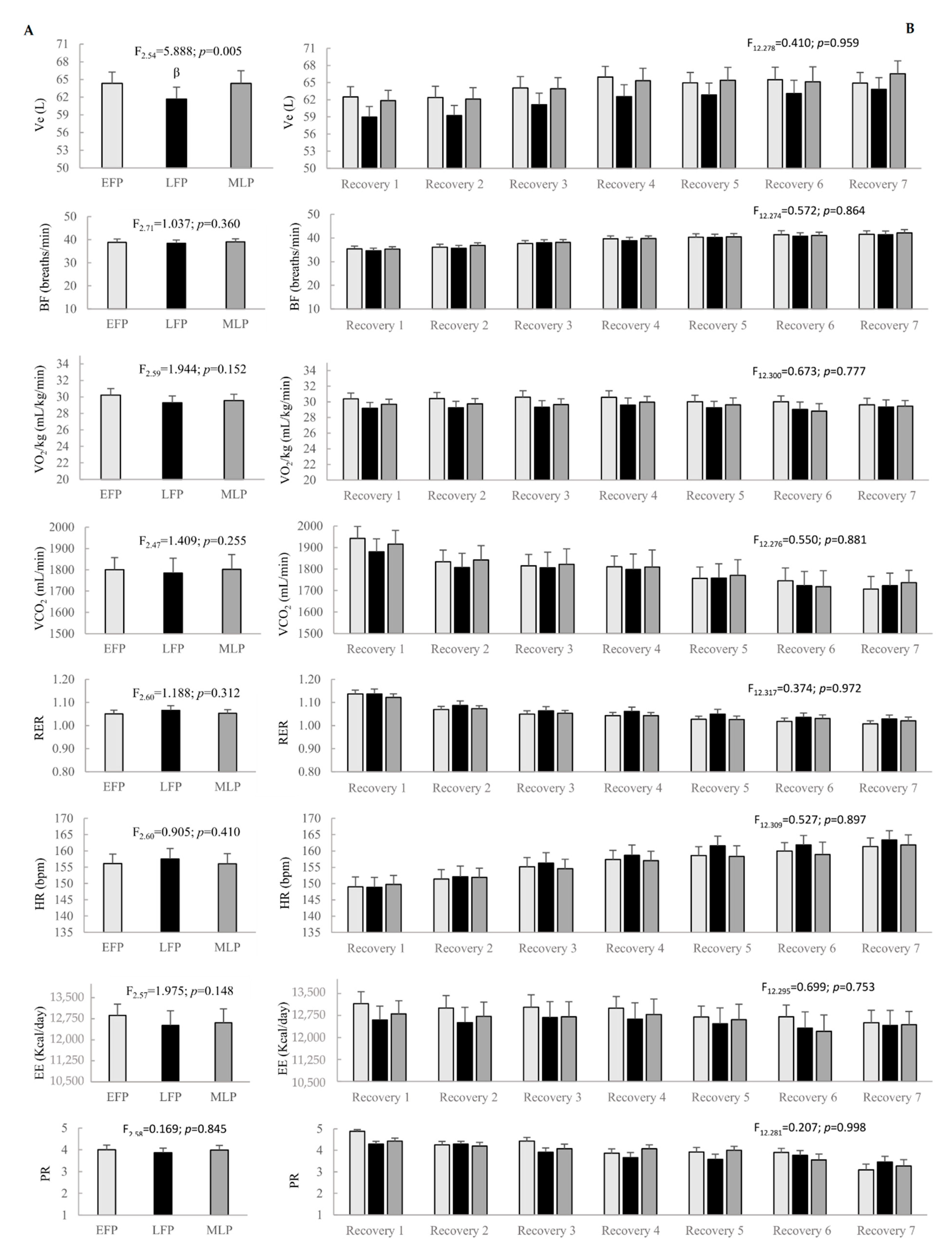
3.3. Interval Running Protocol
3.4. Cool Down
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Constantini, N.W.; Dubnov, G.; Lebrun, C.M. The menstrual cycle and sport performance. Clin. Sports Med. 2005, 24, 51–82. [Google Scholar] [CrossRef]
- Thompson, B.; Han, A. Methodological Recommendations for Menstrual Cycle Research in Sports and Exercise. Med. Sci. Sport Exerc. 2019. [Google Scholar] [CrossRef]
- De Jonge, X.A.J. Effects of the menstrual cycle on exercise performance. Sports Med. 2003, 33, 833–851. [Google Scholar] [CrossRef] [PubMed]
- Ashley, C.D.; Bishop, P.; Smith, J.F.; Reneau, P.; Perkins, C. Menstrual Phase Effects on Fat and Carbohydrate Oxidation During Prolonged Exercise in Active Females. J. Exerc. Physiol. 2000, 3, 67–73. [Google Scholar]
- Oosthuyse, T.; Bosch, A.N. The effect of the menstrual cycle on exercise metabolism. Sports Med. 2010, 40, 207–227. [Google Scholar] [CrossRef] [PubMed]
- MacNutt, M.J.; De Souza, M.J.; Tomczak, S.E.; Homer, J.L.; Sheel, A.W. Resting and exercise ventilatory chemosensitivity across the menstrual cycle. J. Appl. Physiol. 2012, 112, 737–747. [Google Scholar] [CrossRef]
- Burrows, M.; Bird, S. The Physiology of the Highly Trained Female Endurance Runner. Sports Med. 2000, 30, 281–300. [Google Scholar] [CrossRef]
- Goldsmith, E.; Glaister, M. The effect of the menstrual cycle on running economy. J. Sports Med. Phys. Fit. 2020. [Google Scholar] [CrossRef]
- Brar, T.K.; Singh, K.; Kumar, A. Effect of different phases of menstrual cycle on heart rate variability (HRV). J. Clin. Diagn. Res. 2015, 9, CC01. [Google Scholar] [CrossRef]
- Barba-Moreno, L.; Cupeiro, R.; Romero-Parra, N.; Janse de Jonge, X.A.K.; Peinado, A.B. Cardiorespiratory Responses to Endurance Exercise Over the Menstrual Cycle and With Oral Contraceptive Use. J. Strength Cond. Res. 2019. [Google Scholar] [CrossRef]
- Gordon, D.; Scruton, A.; Barnes, R.; Baker, J.; Prado, L.; Merzbach, V. The effects of menstrual cycle phase on the incidence of plateau at and associated cardiorespiratory dynamics. Clin. Physiol. Funct. Imaging 2018, 38, 689–698. [Google Scholar] [CrossRef] [PubMed]
- Packard, K.A.; Lenz, T.L.; Elder, B.; Godfrey, C.; Holcomb, R.; Windle, E. Oral contraceptive use may attenuate menstrual cycle-induced ventilatory changes in endurance trained runners. Open Access J. Sports Med. 2011, 5, 19–25. [Google Scholar] [CrossRef]
- Vaiksaar, S.; Jürimäe, J.; Mäestu, J.; Purge, P.; Kalytka, S.; Shakhlina, L.; Jürimäe, T. No Effect of Menstrual Cycle Phase and Oral Contraceptive Use on Endurance Performance in Rowers. J. Strength Cond. Res. 2011, 25, 1571–1578. [Google Scholar] [CrossRef] [PubMed]
- Carter, J.; Jeukendrup, A.E. Validity and reliability of three commercially available breath-by-breath respiratory systems. Eur. J. Appl. Physiol. 2002, 86, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Foss, Ø.; Hallen, J. Validity and stability of a computerized metabolic system with mixing chamber. Int. J. Sports Med. 2005, 26, 569–575. [Google Scholar] [CrossRef] [PubMed]
- Billat, V.; Renoux, J.C.; Pinoteau, J.; Petit, B.; Koralsztein, J. Reproducibility of running time to exhaustion at VO, in subelite runners. Med. Sci. Sports Exerc. 1994, 26, 254–257. [Google Scholar]
- Nolan, P.; Beaven, M.; Dalleck, L. Comparison of intensities and rest periods for VO2max verification testing procedures. Int. J. Sports Med. 2014, 35, 1024–1029. [Google Scholar] [CrossRef]
- Poole, D.C.; Jones, A.M. Measurement of the maximum oxygen uptake VO2max: VO2peak is no longer acceptable. J. Appl. Physiol. 2017, 122, 997–1002. [Google Scholar] [CrossRef]
- Borg, G. Perceived exertion as an indicator of somatic stress. Scand. J. Rehabil. Med. 1970, 2, 92–98. [Google Scholar]
- Nurmekivi, A.; Pihl, E.; Jürimäe, T.; Karu, T.; Lemberg, H. Blood lactate recovery and perceived readiness to start a new run in middle-distance runners during interval training. Percept. Mot. Skills 2001, 93, 397–404. [Google Scholar] [CrossRef]
- Schaumberg, M.A.; Jenkins, D.G.; de Jonge, X.A.J.; Emmerton, L.M.; Skinner, T.L. Three-step method for menstrual and oral contraceptive cycle verification. J. Sci. Med. Sport 2017, 20, 965–969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Jonge, X.A.J.; Thompson, M.; Chuter, V.; Silk, L.; Thom, J. Exercise performance over the menstrual cycle in temperate and hot, humid conditions. Med. Sci. Sport Exerc. 2012, 44, 2190–2198. [Google Scholar] [CrossRef] [PubMed]
- Romero-Parra, N.; Barba-Moreno, L.; Rael, B.; Alfaro-Magallanes, V.M.; Cupeiro, R.; Díaz, Á.E.; Calderón, F.J.; Peinado, A.B. Influence of the Menstrual Cycle on Blood Markers of Muscle Damage and Inflammation Following Eccentric Exercise. Int. J. Environ. Res. Public Health 2020, 17, 1618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenthal, R. Applied social research methods series. In Survey Research; Sage Publications, Inc.: Southend Oaks, CA, USA, 1991. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic press: Cambridge, MA, USA, 2013. [Google Scholar]
- Williams, T.J.; Krahenbuhl, G.S. Menstrual cycle phase and running economy. Med. Sci. Sports Exerc. 1997, 29, 1609–1618. [Google Scholar] [CrossRef] [PubMed]
- Boukari, R.; Laouafa, S.; Ribon-Demars, A.; Bairam, A.; Joseph, V. Ovarian steroids act as respiratory stimulant and antioxidant against the causes and consequences of sleep-apnea in women. Respir. Physiol. Neurobiol. 2017, 239, 46–54. [Google Scholar] [CrossRef] [PubMed]
- Godbole, G.; Joshi, A.; Vaidya, S.M. Effect of female sex hormones on cardiorespiratory parameters. J. Fam. Med. Prim. Care 2016, 5, 822. [Google Scholar] [CrossRef] [Green Version]
- Samsudeen, N.; Rajagopalan, A. Effect of different phases of menstrual cycle on cardio-respiratory efficiency in normal, overweight and obese female undergraduate students. J. Clin. Diagn. Res. 2016, 10, CC01. [Google Scholar] [CrossRef]
- Lebrun, C.M. Effect of the Different Phases of the Menstrual Cycle and Oral Contraceptives on Athletic Performance. Sports Med. 1993, 16, 400–430. [Google Scholar] [CrossRef]
- Mattu, A.T.; Iannetta, D.; MacInnis, M.J.; Doyle-Baker, P.K.; Murias, J.M. Menstrual and oral contraceptive cycle phases do not affect submaximal and maximal exercise responses. Scand. J. Med. Sci. Sports 2019, 30, 472–484. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| EFP | LFP | MLP | c2 | p | |
|---|---|---|---|---|---|
| LH (mUI/mL) | 7.27 ± 3.91 | 12.56 ± 8.29 | 5.96 ± 3.26 | 9.810 | 0.007 1 |
| FSH (mUI/mL) | 9.14 ± 8.49 | 6.17 ± 2.95 | 3.44 ± 1.53 | 30.095 | <0.001 2 |
| E2 (pg/mL) | 38.78 ± 30.39 | 186.67 ± 154.56 | 138.11 ± 71.99 | 25.810 | <0.001 3 |
| Progesterone (ng/mL) | 0.33 ± 0.19 | 0.75 ± 1.79 | 11.99 ± 5.37 | 27.494 | <0.001 4 |
| E2/progesterone ratio | 0.15 ± 0.17 | 0.53 ± 0.54 | 0.03 ± 0.08 | 26.571 | <0.001 5 |
| EFP | LFP | MLP | c2 | p | |
|---|---|---|---|---|---|
| V̇e (L/min) | 48.2 ± 8.7 | 46.7 ± 8.3 | 49.0 ± 8.5 | 13.900 | 0.001 β |
| BF (breaths/min) | 32.6 ± 6.4 | 32.7 ± 5.6 | 33.3 ± 5.9 | 1.200 | 0.549 |
| V̇O2/Kg (mL/kg/min) | 29.1 ± 2.6 | 28.0 ± 2.3 | 28.5 ± 2.3 | 8.100 | 0.017 # |
| V̇CO2 (mL/min) | 1481.2 ± 215.6 | 1426.7 ± 202.4 | 1443.7 ± 189.8 | 3.600 | 0.165 |
| RER | 0.88 ± 0.05 | 0.88 ± 0.05 | 0.88 ± 0.05 | 0.105 | 0.949 |
| HR (bpm) | 136.0 ± 12.8 | 136.6 ± 12.2 | 136.1 ± 16.2 | 2.923 | 0.232 |
| EE (Kcal/day) | 11834.8 ± 1521.8 | 11377.7 ± 1598.5 | 11571.3 ± 1574.3 | 9.100 | 0.011 # |
| RPE | 9.3 ± 1.8 | 9.3 ± 2.0 | 9.5 ± 2.3 | 0.847 | 0.655 |
| PR | 4.9 ± 0.3 | 4.6 ± 0.5 | 4.6 ± 0.5 | 8.970 | 0.011 |
| EFP | LFP | MLP | c2 | p | |
|---|---|---|---|---|---|
| Ve (L/min) | 43.2 ± 6.4 | 42.6 ± 6.1 | 45.9 ± 6.0 | 10.048 | 0.007 £ |
| BF (breaths/min) | 37.2 ± 6.5 | 37.7 ± 6.4 | 38.9 ± 6.1 | 6.723 | 0.035 γ |
| VO2/Kg (mL/kg/min) | 19.5 ± 2.7 | 19.0 ± 2.5 | 1975 ± 2.0 | 3.900 | 0.142 |
| VCO2 (mL/min) | 1069.4 ± 180.8 | 1058.4 ± 164.9 | 1109.6 ± 132.0 | 9.300 | 0.010 £ |
| RER | 0.94 ± 0.06 | 0.97 ± 0.08 | 0.97 ± 0.07 | 2.947 | 0.229 |
| HR (bpm) | 137.9 ± 15.2 | 138.5 ± 13.6 | 137.3 ± 13.6 | 0.824 | 0.662 |
| EE (Kcal/day) | 8046.8 ± 1304.3 | 7865.7 ± 1390.3 | 8136.7 ± 1117.6 | 7.300 | 0.026 £ |
| RPE | 9.8 ± 2.9 | 9.4 ± 2.0 | 10.0 ± 2.5 | 2.596 | 0.273 |
| PR | 4.1 ± 1.1 | 4.3 ± 0.7 | 4.0 ± 1.0 | 5.056 | 0.080 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rael, B.; Alfaro-Magallanes, V.M.; Romero-Parra, N.; Castro, E.A.; Cupeiro, R.; Janse de Jonge, X.A.K.; Wehrwein, E.A.; Peinado, A.B.; IronFEMME Study Group. Menstrual Cycle Phases Influence on Cardiorespiratory Response to Exercise in Endurance-Trained Females. Int. J. Environ. Res. Public Health 2021, 18, 860. https://doi.org/10.3390/ijerph18030860
Rael B, Alfaro-Magallanes VM, Romero-Parra N, Castro EA, Cupeiro R, Janse de Jonge XAK, Wehrwein EA, Peinado AB, IronFEMME Study Group. Menstrual Cycle Phases Influence on Cardiorespiratory Response to Exercise in Endurance-Trained Females. International Journal of Environmental Research and Public Health. 2021; 18(3):860. https://doi.org/10.3390/ijerph18030860
Chicago/Turabian StyleRael, Beatriz, Víctor M. Alfaro-Magallanes, Nuria Romero-Parra, Eliane A. Castro, Rocío Cupeiro, Xanne A. K. Janse de Jonge, Erica A. Wehrwein, Ana B. Peinado, and IronFEMME Study Group. 2021. "Menstrual Cycle Phases Influence on Cardiorespiratory Response to Exercise in Endurance-Trained Females" International Journal of Environmental Research and Public Health 18, no. 3: 860. https://doi.org/10.3390/ijerph18030860