
Early Tooth Loss after Periodontal Diagnosis: Development and Validation of a Clinical Decision Model

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
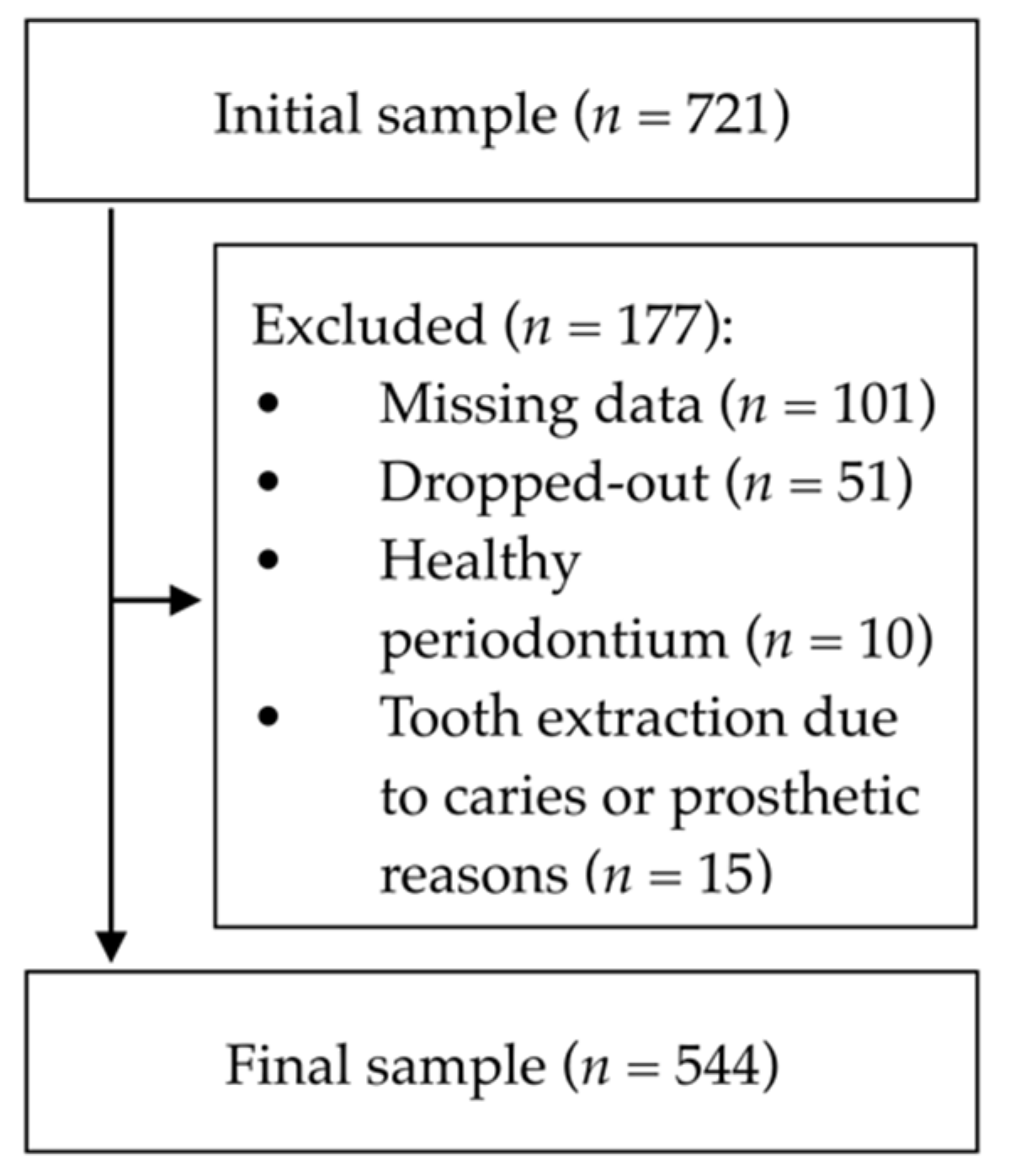
2.1. Source of Data, Participants, Sample Size and Missing Data
2.1.1. Source of Data
2.1.2. Participants and Setting
2.1.3. Sample Size and Missing Data
2.2. Outcome
2.3. Predictors
2.3.1. Periodontal Diagnosis and Measurement Reproducibility
2.3.2. Sociodemographic Variables
2.4. Data Collection
2.5. Statistical Analysis Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Clin. Periodontol. 2018, 45, S162–S170. [Google Scholar] [CrossRef] [PubMed]
- Buset, S.L.; Walter, C.; Friedmann, A.; Weiger, R.; Borgnakke, W.S.; Zitzmann, N.U. Are periodontal diseases really silent? A systematic review of their effect on quality of life. J. Clin. Periodontol. 2016, 43, 333–344. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, M.C.; Dias-Pereira, A.C.; Branco-de-Almeida, L.S.; Martins, C.C.; Paiva, S.M. Impact of periodontal disease on quality of life: A systematic review. J. Periodontal Res. 2017, 52, 651–665. [Google Scholar] [CrossRef] [PubMed]
- Botelho, J.; Machado, V.; Proença, L.; Bellini, D.H.; Chambrone, L.; Alcoforado, G.; Mendes, J.J. The impact of nonsurgical periodontal treatment on oral health-related quality of life: A systematic review and meta-analysis. Clin. Oral Investig. 2020, 24, 585–596. [Google Scholar] [CrossRef] [PubMed]
- Van Dyke, T.E.; Van Winkelhoff, A.J. Infection and inflammatory mechanisms. J. Clin. Periodontol. 2013, 40, S1–S7. [Google Scholar] [CrossRef]
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef]
- Botelho, J.; Machado, V.; Hussain, S.B.; Zehra, S.A.; Proença, L.; Orlandi, M.; Mendes, J.J.; D’Aiuto, F. Periodontitis and circulating blood cell profiles: A systematic review and meta-analysis. Exp. Hematol. 2020, 93, 1–13. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A. How effective is surgical therapy compared with nonsurgical debridement? Periodontol. 2000 2005, 37, 72–87. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A.; Lang, N.P. Surgical and nonsurgical periodontal therapy. Learned and unlearned concepts. Periodontology 2000 2013, 62, 218–231. [Google Scholar] [CrossRef]
- Preshaw, P.M.; Alba, A.L.; Herrera, D.; Jepsen, S.; Konstantinidis, A.; Makrilakis, K.; Taylor, R. Periodontitis and diabetes: A two-way relationship. Diabetologia 2012, 55, 21–31. [Google Scholar] [CrossRef] [Green Version]
- Billings, M.; Holtfreter, B.; Papapanou, P.N.; Mitnik, G.L.; Kocher, T.; Dye, B.A. Age-dependent distribution of periodontitis in two countries: Findings from NHANES 2009 to 2014 and SHIP-TREND 2008 to 2012. J. Periodontol. 2018, 89, S140–S158. [Google Scholar] [CrossRef] [PubMed]
- Albandar, J.M. Global risk factors and risk indicators for periodontal diseases. J. Periodontol. 2000 2002, 29, 177–206. [Google Scholar] [CrossRef] [PubMed]
- Keller, A.; Rohde, J.F.; Raymond, K.; Heitmann, B.L. Association Between Periodontal Disease and Overweight and Obesity: A Systematic Review. J. Periodontol. 2015, 86, 766–776. [Google Scholar] [CrossRef] [PubMed]
- Faggion, C.M.; Petersilka, G.; Lange, D.E.; Gerss, J.; Flemmig, T.F. Prognostic model for tooth survival in patients treated for periodontitis. J. Clin. Periodontol. 2007, 34, 226–231. [Google Scholar] [CrossRef]
- Schwendicke, F.; Schmietendorf, E.; Plaumann, A.; Sälzer, S.; Dörfer, C.E.; Graetz, C. Validation of multivariable models for predicting tooth loss in periodontitis patients. J. Clin. Periodontol. 2018, 45, 701–710. [Google Scholar] [CrossRef]
- Avila, G.; Galindo-Moreno, P.; Soehren, S.; Misch, C.E.; Morelli, T.; Wang, H.-L. A Novel Decision-Making Process for Tooth Retention or Extraction. J. Periodontol. 2009, 80, 476–491. [Google Scholar] [CrossRef]
- Fardal, Ø.; Johannessen, A.C.; Linden, G.J. Tooth loss during maintenance following periodontal treatment in a periodontal practice in Norway. J. Clin. Periodontol. 2004, 31, 550–555. [Google Scholar] [CrossRef]
- Nunn, M.E.; Fan, J.; Su, X.; Levine, R.A.; Lee, H.-J.; McGuire, M.K. Development of prognostic indicators using classification and regression trees for survival. Periodontol. 2000 2012, 58, 134–142. [Google Scholar] [CrossRef]
- Chambrone, L.; Chambrone, D.; La, L.; La, C. Predictors of tooth loss during long-term periodontal maintenance: A systematic review of observational studies. J. Clin. Periodontol. 2010, 37, 675–684. [Google Scholar] [CrossRef]
- Heitz-Mayfield, L.J.A. Disease progression: Identification of high-risk groups and individuals for periodontitis. J. Clin. Periodontol. 2005, 32, 196–209. [Google Scholar] [CrossRef]
- CCollins, G.S.; Reitsma, J.B.; Altman, D.G.; Moons, K.G.M. Transparent Reporting of a multivariable prediction model for Individual Prognosis or Diagnosis (TRIPOD): The TRIPOD statement. Ann. Intern. Med. 2015, 162, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landry, R.G.; Jean, M. Periodontal Screening and Recording (PSR) Index: Precursors, utility and limitations in a clinical setting. Int. Dent. J. 2002, 52, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Tonetti, M.S.; Greenwell, H.; Kornman, K.S. Staging and grading of periodontitis: Framework and proposal of a new classification and case definition. J. Clin. Periodontol. 2018, 45, 149–161. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krois, J.; Graetz, C.; Holtfreter, B.; Brinkmann, P.; Kocher, T.; Schwendicke, F. Evaluating Modeling and Validation Strategies for Tooth Loss. J. Dent. Res. 2019, 98, 1088–1095. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Machado, V.; Botelho, J.; Amaral, A.; Proença, L.; Alves, R.; Rua, J.; Cavacas, M.A.; Delgado, A.S.; Mendes, J.J. Prevalence and extent of chronic periodontitis and its risk factors in a Portuguese subpopulation: A retrospective cross-sectional study and analysis of Clinical Attachment Loss. PeerJ 2018, 6, e5258. [Google Scholar] [CrossRef] [PubMed]
- Hamp, S.-E.; Nyman, S.; Lindhe, J. Periodontal treatment of multi rooted teeth. Results after 5 years. J. Clin. Periodontol. 1975, 2, 126–135. [Google Scholar] [CrossRef]
- Lindhe, J.; Nyman, S. Long-term maintenance of patients treated for advanced disease. J. Clin. Periodontol. 1984, 11, 504–514. [Google Scholar] [CrossRef]
- Innes, N.P.T.; Chu, C.H.; Fontana, M.; Lo, E.C.M.; Thomson, W.M.; Uribe, S.; Heiland, M.; Jepsen, S.; Schwendicke, F. A Century of Change towards Prevention and Minimal Intervention in Cariology. J. Dent. Res. 2019, 98, 611–617. [Google Scholar] [CrossRef]
- Machado, V.; Botelho, J.; Proença, L.; Alves, R.; Oliveira, M.J.; Amaro, L.; Águas, A.; Mendes, J.J. Periodontal status, perceived stress, diabetes mellitus and oral hygiene care on quality of life: A structural equation modelling analysis. BMC Oral Health 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Botelho, J.; Machado, V.; Proença, L.; Oliveira, M.J.; Cavacas, M.A.; Amaro, L.; Águas, A.; Mendes, J.J. Perceived xerostomia, stress and periodontal status impact on elderly oral health-related quality of life: Findings from a cross-sectional survey. BMC Oral Health 2020, 20, 199. Available online: https://bmcoralhealth.biomedcentral.com/articles/10.1186/s12903-020-01183-7 (accessed on 15 October 2020). [CrossRef]
- Burt, B. Position paper-Epidemiology of periodontal diseases. J. Periodontol. 2005, 76, 1406–1419. Available online: http://www.ncbi.nlm.nih.gov/pubmed/16945041 (accessed on 12 October 2020). [PubMed]
- Ramseier, C.A.; Anerud, A.; Dulac, M.; Lulic, M.; Cullinan, M.P.; Seymour, G.J.; Faddy, M.J.; Bürgin, W.; Schätzle, M.; Lang, N.P. Natural history of periodontitis: Disease progression and tooth loss over 40 years. J. Clin. Periodontol. 2017, 44, 1182–1191. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kundu, S.; Mazumdar, M.; Ferket, B. Impact of correlation of predictors on discrimination of risk models in development and external populations. BMC Med. Res. Methodol. 2017, 17, 63. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variable | Development Cohort (n = 455) | Validation Cohort (n = 99) | p-Value 1 |
|---|---|---|---|
| Gender, n (%) | |||
| Male | 248 (54.5) | 56 (56.6) | 0.709 |
| Female | 207 (46.5) | 43 (43.4) | |
| Age (years), mean (SD) | 54.8 (12.5) | 45.8 (16.3) | <0.001 |
| Periodontitis, n (%) | |||
| Stage I (Mild) | 16 (3.5) | 5 (5.1) | 0.378 |
| Stage II (Moderate) | 140 (30.8) | 36 (36.4) | |
| Stage III/IV (Severe/Advanced) | 299 (65.7) | 58 (58.6) | |
| Smoking status, n (%) | |||
| Smoker | 241 (53.0) | 44 (44.4) | 0.124 |
| Non-smoker | 214 (47.0) | 55 (55.6) | |
| Teeth with mobility (n), mean (SD) | 0.2 (0.5) | 0.1 (0.3) | 0.467 |
| Missing teeth (n), mean (SD) | 6.8 (5.6) | 5.6 (5.5) | 0.078 |
| PD (mm), mean (SD) | 2.3 (1.6) | 2.2 (1.5) | 0.218 |
| Recession (mm), mean (SD) | 0.6 (1.0) | 0.4 (0.8) | 0.167 |
| CAL (mm), mean (SD) | 2.8 (2.1) | 2.3 (1.6) | 0.109 |
| Teeth extracted, n (% from total) | 103 (1.1) | 12 (0.6) | 0.057 |
| Confounder | p-Value 1 |
|---|---|
| Gender | 0.115 |
| Smoking status | 0.006 |
| Quadrant | 0.360 |
| Sextant | 0.636 |
| Tooth type | <0.001 |
| Mobility | NA |
| Furcation | NA |
| Variable | Surgery | p-Value 1 | |
|---|---|---|---|
| Yes | No | ||
| PD (mm), mean (SD) | 4.99 (1.43) | 2.97 (1.08) | <0.001 |
| Recession (mm), mean (SD) | 2.02 (1.72) | 0.71 (1.20) | <0.001 |
| CAL (mm), mean (SD) | 7.01 (2.26) | 3.67 (1.59) | <0.001 |
| Missing Teeth (n), mean (SD) | 7.38 (4.84) | 5.16 (4.59) | <0.001 |
| Variable | OR (95% CI) | p-Value | OR (95% CI) | B 1 | p-Value |
|---|---|---|---|---|---|
| Smoking | |||||
| Non-smoker | 1 | - | - | - | - |
| Smoker | 0.58 (0.39–0.86) | 0.007 | - | - | - |
| Tooth Type | |||||
| Incisor | 2.10 (1.25–3.54) | 0.005 | 1.80 (1.04–3.12) | 0.589 | 0.037 |
| Canine | 0.46 (0.19–1.18) | 0.108 | - | - | - |
| Premolar | 1 | - | - | - | - |
| Molar | 1.70 (0.95–3.04) | 0.073 | - | - | - |
| PD (mm) | 2.92 (2.55–3.34) | <0.001 | - | - | - |
| Recession (mm) | 1.94 (1.76–2.15) | <0.001 | - | - | - |
| CAL (mm) | 1.88 (1.75–2.03) | <0.001 | 1.94 (1.78–2.10) | 0.661 | <0.001 |
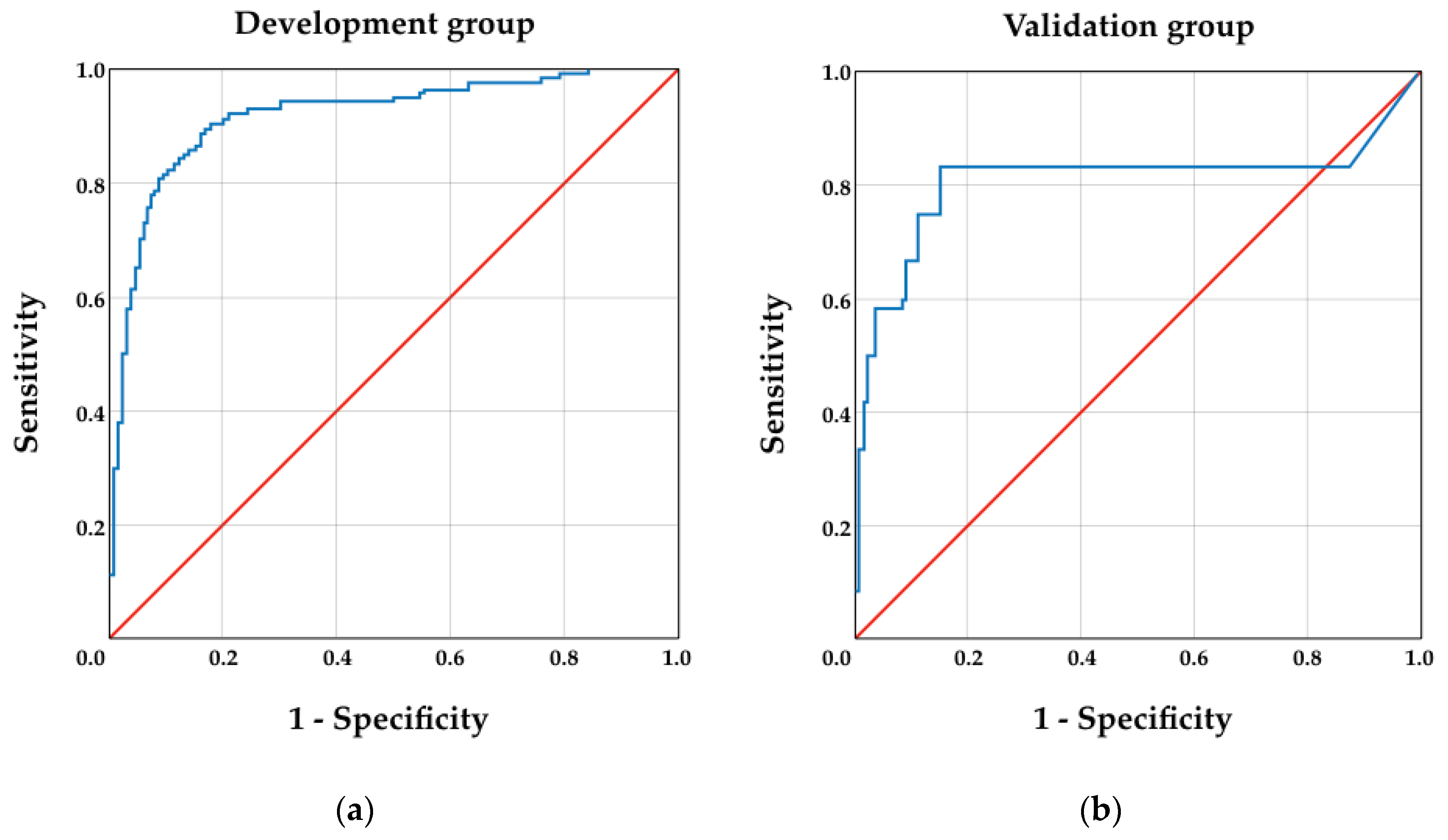
| Group | AUC | 95% CI | |
|---|---|---|---|
| Lower Limit | Upper Limit | ||
| Development | 0.920 | 0.891 | 0.950 |
| Validation | 0.809 | 0.629 | 0.989 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Santos, F.; Beato, F.; Machado, V.; Proença, L.; Mendes, J.J.; Botelho, J. Early Tooth Loss after Periodontal Diagnosis: Development and Validation of a Clinical Decision Model. Int. J. Environ. Res. Public Health 2021, 18, 1363. https://doi.org/10.3390/ijerph18031363
Santos F, Beato F, Machado V, Proença L, Mendes JJ, Botelho J. Early Tooth Loss after Periodontal Diagnosis: Development and Validation of a Clinical Decision Model. International Journal of Environmental Research and Public Health. 2021; 18(3):1363. https://doi.org/10.3390/ijerph18031363
Chicago/Turabian StyleSantos, Francisco, Frederico Beato, Vanessa Machado, Luís Proença, José João Mendes, and João Botelho. 2021. "Early Tooth Loss after Periodontal Diagnosis: Development and Validation of a Clinical Decision Model" International Journal of Environmental Research and Public Health 18, no. 3: 1363. https://doi.org/10.3390/ijerph18031363