Measuring Development of Self-Help Organizations for Patients with Chronic Health Conditions in Hong Kong: Development and Validation of the Self-Help Organization Development Scale (SHODS)

 ,
, 
 ,
,  and
and
Abstract
:1. Introduction
1.1. Background: Significance and Challenges of Self-Help Organizations
1.2. The Present Study
1.3. Model Development: Indicators of SHO Development
1.4. Concurrent Validity: Organizational Variables and SHO Development
2. Materials and Methods
2.1. Procedure and Participants
2.2. Measures
2.2.1. Development of Self-Help Organization Development Scale (SHODS)
2.2.2. Measurement of SHO Development Factors
2.2.3. Measurement of Organizational Variables
2.3. Data Analysis
3. Results
3.1. Scale Items and Descriptive Statistics
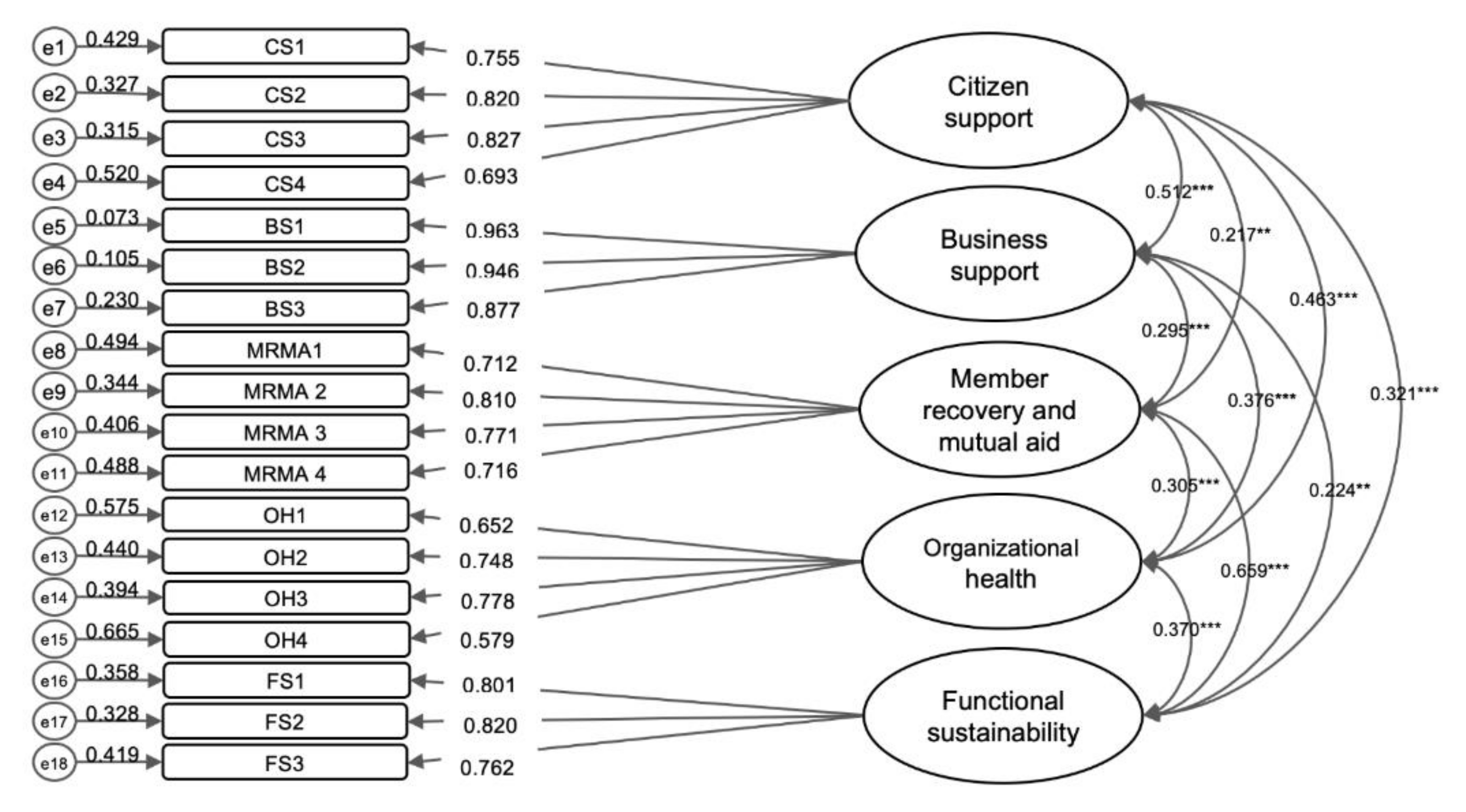
3.2. Confirmatory Factor Analysis
3.3. Reliability and Validity Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Centers for Disease Control and Prevention. About Chronic Illness. Available online: https://www.cdc.gov/chronicdisease/about/index.htm (accessed on 2 November 2020).
- Mitchell, R.J.; Curtis, K.; Braithwaite, J. Health Outcomes and Costs for Injured Young People Hospitalised With and Without Chronic Health Conditions. Injury 2017, 48, 1776–1783. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Lim, S.S.; Abbafati, C.; Abbas, K.M.; Abbasi, M.; Abbasifard, M.; Abbasi-Kangevari, M.; Abbastabar, H.; Abd-Allah, F.; Abdelalim, A.; et al. Global Burden of 369 Diseases and Injuries in 204 Countries and Territories, 1990–2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation. Findings from the Global Burden of Disease Study 2017; Institute for Health Metrics and Evaluation: Seattle, WA, USA, 2018. [Google Scholar]
- Suhrcke, M.; Nugent, R.A.; Stuckler, D.; Rocco, L.C. Chronic Disease: An Economic Perspective; Oxford Health Alliance: London, UK, 2006. [Google Scholar]
- Kofahl, C.; Trojan, A.; Knesebeck, O.V.D.; Nickel, S. Self-Help Friendliness: A German Approach for Strengthening the Cooperation Between Self-Help Groups and Health Care Professionals. Soc. Sci. Med. 2014, 123, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Rojatz, D.; Forster, R. Self-Help Organisations as Patient Representatives in Health Care and Policy Decision-Making. Health Policy 2017, 121, 1047–1052. [Google Scholar] [CrossRef]
- Nickel, S.; Trojan, A.; Kofahl, C. Involving Self-Help Groups in Health-Care Institutions: The Patients’ Contribution to and Their View of ‘Self-Help Friendliness’ as an Approach to Implement Quality Criteria of Sustainable Co-Operation. Health Expect. 2017, 20, 274–287. [Google Scholar] [CrossRef] [Green Version]
- Markowitz, F.E. Involvement in Mental Health Self-Help Groups and Recovery. Health Sociol. Rev. 2015, 24, 199–212. [Google Scholar] [CrossRef]
- Nayak, A.K.; Panigrahi, P.K.; Swain, B. Self-Help Groups in India: Challenges and a Roadmap for Sustainability. Soc. Responsib. J. 2019, 16, 1013–1033. [Google Scholar] [CrossRef]
- Putnam Rankin, C.; Archibald, M. Specialization and the Survival of Self-Help Organizations. Sociol. Forum 2016, 31, 72–95. [Google Scholar] [CrossRef]
- Martin, C.M.; Peterson, C.; Robinson, R.; Sturmberg, J.P. Care for Chronic Illness in Australian General Practice–Focus Groups of Chronic Disease Self-Help Groups Over 10 Years: Implications for Chronic Care Systems Reforms. Asia Pac. Fam. Med. 2009, 8, 1–14. [Google Scholar] [CrossRef] [Green Version]
- Sandaunet, A.G. The Challenge of Fitting in: Non-Participation and Withdrawal from an Online Self-Help Group for Breast Cancer Patients. Sociol. Health Illn. 2008, 30, 131–144. [Google Scholar] [CrossRef] [Green Version]
- Home Affairs Department. The Demographics: Ethnic Groups. Available online: https://www.had.gov.hk/rru/english/info/info_dem.html (accessed on 8 September 2020).
- Pun, Y.W. Tantao Bingren Zizhu Zuzhi De Fazhan: Lichengbei Huigu Yu Zhanwang [Exploration of the Development of Patient Self-Help Organizations: Milestone Retrospect and Prospect]. Available online: http://www.socsc.hku.hk/ExCEL3/wp-content/uploads/2014/03/3YauWai28March2014.pdf (accessed on 22 October 2020).
- Xianggang Zizhu Zuzhi Ji Xiaozu Mingdan [Hong Kong Self-Help Organization/Group List]; Hong Kong Society for Rehabilitation: Hong Kong, China, 2019; unpublished raw data.
- Pun, Y.W.; Leung, Y.M.C. Exploratory Study of Development Characteristics and New Challenges of Self-Help Groups for Chronic Ill Patients in Hong Kong; Patient Mutual Support Center, Community Rehabilitation Network, The Hong Kong Society for Rehabilitation: Hong Kong, China, 2010.
- Cameron, K.S.; Quinn, R.E. Diagnosing and Changing Organizational Culture: Based on the Competing Values Framework; John Wiley & Sons: San Francisco, CA, USA, 2011. [Google Scholar]
- Liket, K.C.; Maas, K. Non-Profit Organizational Effectiveness: Analysis of Best Practices. Nonprofit Volunt. Sect. Q. 2015, 44, 268–296. [Google Scholar] [CrossRef]
- Bray, I. Effective Fundraising for Nonprofits: Real-World Strategies That Work, 4th ed.; Nolo: Berkeley, CA, USA, 2013. [Google Scholar]
- Chan, R.K.H.; Cheung, C.K. An Evaluation Study on the Outcome of the Community Investment and Inclusion Fund (CIIF); Community Investment and Inclusion Fund, Labor and Welfare Bureau: Hong Kong, China, 2012.
- Hung, J.Y.; Chen, M.M.C. A Study on the Current Situation and Problem for Social Service Institutes in Taiwan. J. China Inst. Technol. 2005, 32, 273–302. [Google Scholar]
- Hyde, B. Mutual Aid Group Work: Social Work Leading the Way to Recovery-Focused Mental Health Practice. Soc. Work Groups 2013, 36, 43–58. [Google Scholar] [CrossRef]
- Mok, B.H.; Cheung, C.K.; Ngai, S.Y.S. Final Report for Evaluating the Outcomes and Impact of the Community Investment and Inclusion Fund (CIIF): Professional Contribution to the Sustainability of Self-Help Groups and Their Social Capital Created in CIIF Projects; Community Investment and Inclusion Fund, Labor and Welfare Bureau: Hong Kong, China, 2006.
- Netting, F.E. Including and Excluding Volunteers: Challenges of Managing Groups That Depend on Donated Talent. In Handbook of Community Movements and Local Organizations; Cnaan, R.A., Milofsky, C., Eds.; Springer: New York, NY, USA, 2008; pp. 410–425. [Google Scholar]
- Powell, T.; Perron, B.E. Self-Help Groups and Mental Health/Substance Use Agencies: The Benefits of Organizational Exchange. Subst. Use Misuse 2010, 45, 315–329. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, D.M. Mutual Aid: A Contribution to Best-Practice Social Work. Soc. Work Groups 2010, 33, 53–68. [Google Scholar] [CrossRef]
- Wong, S.W.; Lee, S.T. A Survey on Needs and Future Development of Self-Help Groups for Persons with Chronic Illness; City University of Hong Kong: Hong Kong, China, 2003. [Google Scholar]
- Hsieh, W.C.; Cheng, S.F.; Leung, Y.M. Xianggang Diqu Bingren Zizhu Zuzhi Zhuanzhi Renyuan Dui Renli Ziyuan Guanli Xuqiu Zhi Tantao: Yi Jieshou Xianggang Fukanghui Shehui Fukang Wangluo Jihua Peili Zhi Bingren Zizhu Zuzhi Wei Li [A Study of Staff’S Needs of Human Resources Management in Hong Kong’s Self-Help Organizations: Taking Self-Help Organizations Within CRN Empowerment Program as an Example]. Shequ Fazhan Jikan [Community Dev. Q.] 2009, 15, 432–455. [Google Scholar]
- Chan, R.K.H. Self-Help Groups for Men in Hong Kong: Experiences and Prospects. Int. Soc. Work 2009, 52, 343–356. [Google Scholar] [CrossRef]
- Goncalves, D.C.; Byrne, G.J. Sooner or Later: Age at Onset of Generalised Anxiety Disorder in Older Adults. Depress. Anxiety 2012, 29, 39–46. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus New Alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Nunnally, J.C.; Bernstein, I.H. Psychometric Theory, 3rd ed.; McGraw-Hill: New York, NY, USA, 1994. [Google Scholar]
- White, W.L.; Kelly, J.F. Recovery Management: What if We Really Believed That Addiction was a Chronic Disorder. In Addiction Recovery Management; White, W.L., Kelly, J.F., Eds.; Humana Press: Totowa, NJ, USA; Springer: Boston, MA, USA, 2011; pp. 67–84. [Google Scholar]
- Baird, S.L.; Alaggia, R. Trauma-Informed Groups: Recommendations for Group Work Practice. Clin. Soc. Work J. 2019, 1–10. [Google Scholar] [CrossRef]
- Zhang, C. ‘Nothing About Us Without Us’: The Emerging Disability Movement and Advocacy in China. Disabil. Soc. 2017, 32, 1096–1101. [Google Scholar] [CrossRef]
- Allred, C.A.; Burns, B.J.; Phillips, S.D. The Assertive Community Treatment Team as a Complex Dynamic System of Care. Admin. Pol. Ment. Health 2005, 32, 220–221. [Google Scholar] [CrossRef] [PubMed]
- Batti, R.C. Development Project Management within Local NGOs: 10 Recommendations to Meet 10 Challenges. Glob. Bus. Organ. Excell. 2015, 34, 21–29. [Google Scholar] [CrossRef]
- Clark, W.; Welch, S.N.; Berry, S.H.; Collentine, A.M.; Collins, R.; Lebron, D.; Shearer, A.L. California’s Historic Effort to Reduce the Stigma of Mental Illness: The Mental Health Services Act. Am. J. Public Health 2013, 103, 786–794. [Google Scholar] [CrossRef]
- Ditlev-Simonsen, C.D. Beyond Sponsorship-Exploring the Impact of Cooperation Between Corporations and NGOs. Int. J. Corp. Soc. Responsib. 2017, 2, 1–11. [Google Scholar] [CrossRef]
- Kim, K.M. The Accomplishments of Disabled Women’s Advocacy Organizations and Their Future in Korea. Disabil. Soc. 2010, 25, 219–230. [Google Scholar] [CrossRef]
- Markus, K.A.; Borsboom, D. Frontiers of Test. Validity Theory: Measurement, Causation, and Meaning; Routledge: New York, NY, USA, 2013. [Google Scholar]


{kind=link}
| Factor | N | Mean | SD |
|---|---|---|---|
| Citizen support | 229 | 33.93 | 20.41 |
| Business support | 229 | 36.17 | 28.88 |
| Member recovery and mutual aid | 231 | 66.47 | 17.23 |
| Organizational health | 230 | 46.86 | 19.22 |
| Functional sustainability | 230 | 59.75 | 16.19 |
| Model Fit Indices | CFA of Total Sample Model (n = 232) | SHO Establishment Duration in Months (Median = 240) | Affiliation with Another SHO/NGO | ||
|---|---|---|---|---|---|
| Below or Equal to Median (n = 114) | Above Median (n = 107) | Affiliated (n = 115) | Not Affiliated (n = 117) | ||
| CFI | 0.959 | 0.934 | 0.930 | 0.929 | 0.942 |
| TLI | 0.950 | 0.919 | 0.914 | 0.914 | 0.928 |
| RMSEA | 0.056 | 0.075 | 0.070 | 0.077 | 0.067 |
| SRMR | 0.052 | 0.071 | 0.068 | 0.062 | 0.068 |
| Factor | Item | CFA | Cronbach’s Alpha |
|---|---|---|---|
| Citizen support | CS1 Receiving donations from citizens | 0.755 | 0.851 |
| CS2 Citizens collaborating with the SHO to advocate for patient rights | 0.820 | ||
| CS3 Citizens participating in the SHO’s volunteer service | 0.827 | ||
| CS4 Citizens having adequate understanding of the SHO | 0.693 | ||
| Business support | BS1 Having good relationships with businesses and enterprises | 0.963 | 0.950 |
| BS2 Businesses and enterprises having a good understanding of the SHO | 0.946 | ||
| BS3 Receiving funding support from businesses and enterprises | 0.877 | ||
| Member recovery and mutual aid | MRMA1 Good self-help and mutual support among members | 0.712 | 0.840 |
| MRMA2 Positive change in members’ sense of hope and resilience in the face of the chronic health condition | 0.810 | ||
| MRMA3 Members’ stress has been reduced | 0.771 | ||
| MRMA4 Members are appreciated by others | 0.716 | ||
| Organizational health | OH1 Stable funding | 0.652 | 0.783 |
| OH2 Stable supplies, such as wheelchairs, computers, and recreational facilities | 0.748 | ||
| OH3 Stable human resources | 0.778 | ||
| OH4 Adapting to the changing environment | 0.579 | ||
| Functional sustainability | FS1 Members gain more knowledge about self-care and their chronic health condition | 0.801 | 0.837 |
| FS2 Members express fulfilment of their needs | 0.820 | ||
| FS3 Members recognize their own values | 0.762 |
| Factor | Citizen Support | Business Support | Member Recovery and Mutual Aid | Organizational Health | Functional Sustainability |
|---|---|---|---|---|---|
| Citizen support | 1 | ||||
| Business support | 0.463 *** | 1 | |||
| Member recovery and mutual aid | 0.197 ** | 0.263 *** | 1 | ||
| Organizational health | 0.362 *** | 0.316 *** | 0.265 *** | 1 | |
| Functional sustainability | 0.280 *** | 0.199 ** | 0.555 *** | 0.307 *** | 1 |
| Factor | Organizational Variables | ||||
|---|---|---|---|---|---|
| Staff Understanding | Staff Supervision | Networking | Advocating | Educating the Public and Patients | |
| Citizen support | 0.229 ** | 0.259 ** | 0.579 *** | 0.542 *** | 0.573 *** |
| Business support | 0.166 * | 0.262 ** | 0.463 *** | 0.500 *** | 0.407 *** |
| Member recovery and mutual aid | 0.276 *** | 0.377 *** | 0.327 *** | 0.349 *** | 0.439 *** |
| Organizational health | 0.460 *** | 0.467 *** | 0.496 *** | 0.361 *** | 0.393 *** |
| Functional sustainability | 0.283 *** | 0.328 *** | 0.299 *** | 0.307 *** | 0.323 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ngai, S.S.-y.; Jiang, S.; Cheung, C.-k.; Tang, H.-y.; Ngai, H.-l.; Ng, Y.-h. Measuring Development of Self-Help Organizations for Patients with Chronic Health Conditions in Hong Kong: Development and Validation of the Self-Help Organization Development Scale (SHODS). Int. J. Environ. Res. Public Health 2021, 18, 1351. https://doi.org/10.3390/ijerph18031351
Ngai SS-y, Jiang S, Cheung C-k, Tang H-y, Ngai H-l, Ng Y-h. Measuring Development of Self-Help Organizations for Patients with Chronic Health Conditions in Hong Kong: Development and Validation of the Self-Help Organization Development Scale (SHODS). International Journal of Environmental Research and Public Health. 2021; 18(3):1351. https://doi.org/10.3390/ijerph18031351
Chicago/Turabian StyleNgai, Steven Sek-yum, Shan Jiang, Chau-kiu Cheung, Hon-yin Tang, Hiu-lam Ngai, and Yuen-hang Ng. 2021. "Measuring Development of Self-Help Organizations for Patients with Chronic Health Conditions in Hong Kong: Development and Validation of the Self-Help Organization Development Scale (SHODS)" International Journal of Environmental Research and Public Health 18, no. 3: 1351. https://doi.org/10.3390/ijerph18031351