
Differences in the Association between Physical Activity and People’s Resilience and Emotions during Two Consecutive Covid-19 Lockdowns in Israel



Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. The Assessment
2.3. Statistical Analysis
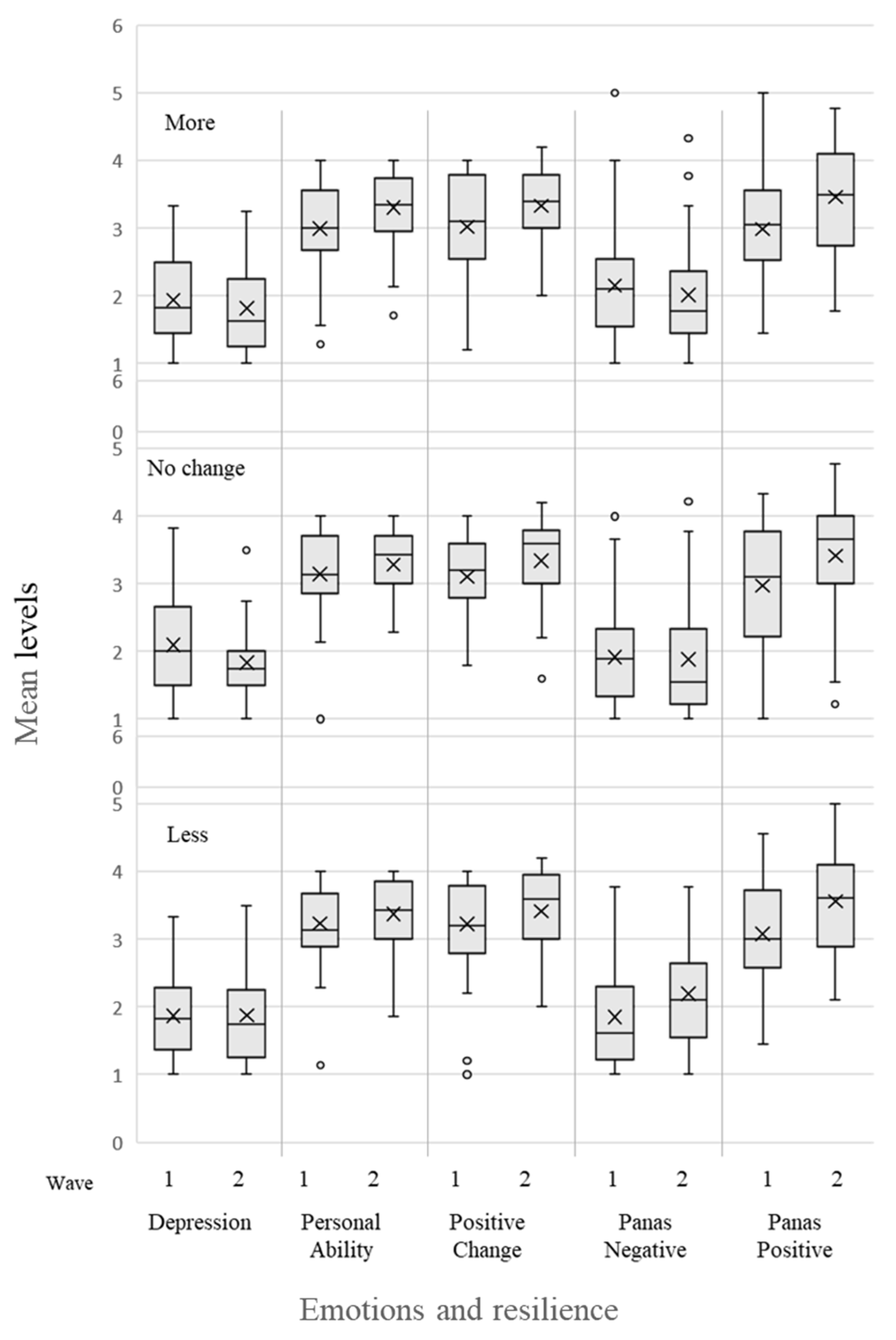
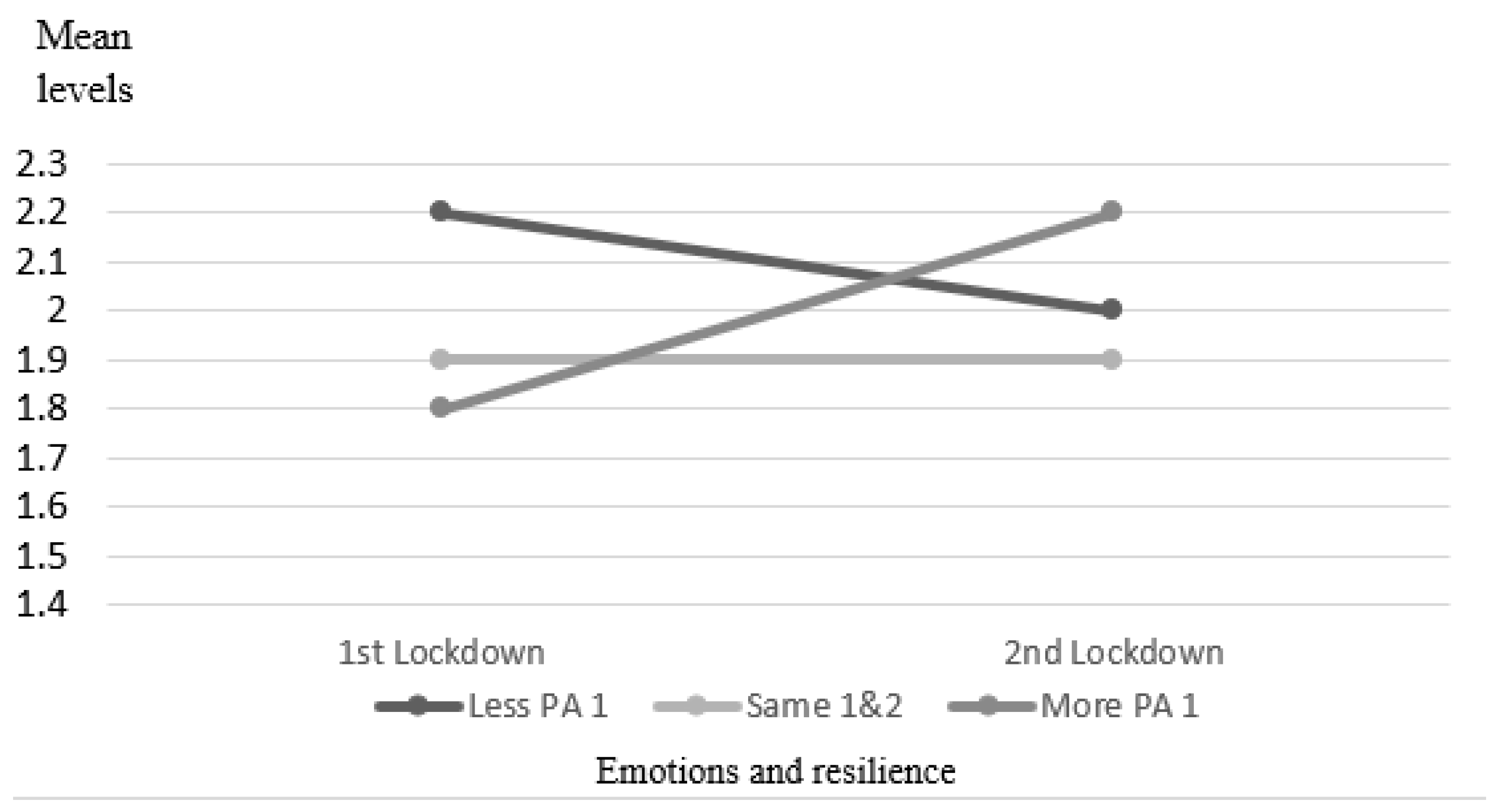
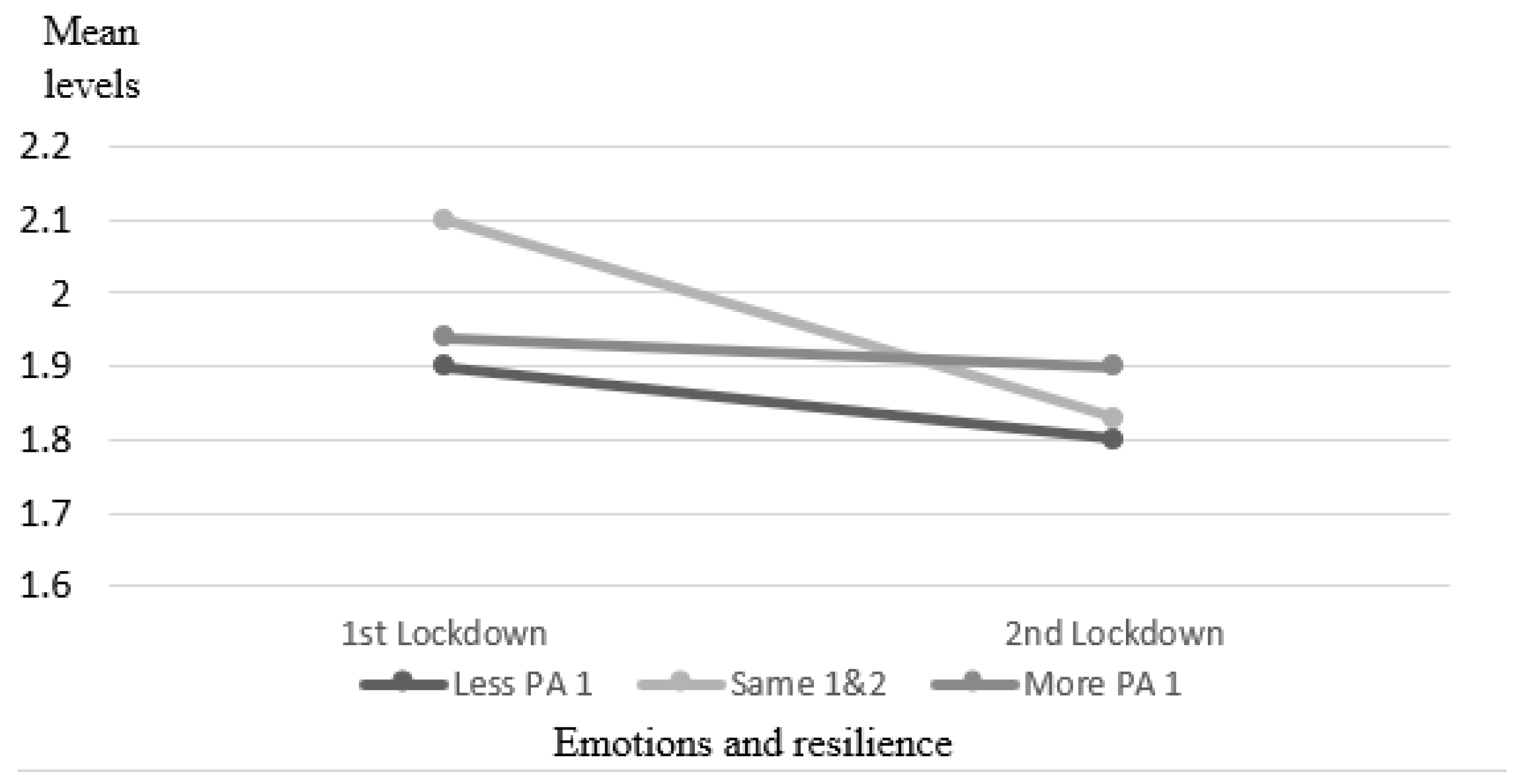
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Harrison, E.; Monroe-Lord, L.; Carson, A.D.; Jean-Baptiste, A.M.; Phoenix, J.; Jackson, P.; Harris, B.M.; Asongwed, E.; Richardson, M.L. COVID-19 pandemic-related changes in wellness behavior among older Americans. BMC Public Health 2021, 21, 755. [Google Scholar] [CrossRef]
- Maltagliati, S.; Rebar, A.; Fessler, L.; Forestier, C.; Sarrazin, P.; Chalabaev, A.; Sander, D.; Sivaramakrishnan, H.; Orsholits, D.; Boisgontier, M.P.; et al. Evolution of physical activity habits after a context change: The case of COVID-19 lockdown. Br. J. Health Psychol. 2021, 26, 1135–1154. [Google Scholar] [CrossRef]
- Farah, B.Q.; Prado, W.L.D.; Malik, N.; Lofrano-Prado, M.C.; de Melo, P.H.; Botero, J.P.; Cucato, G.G.; Correia, M.D.A.; Ritti-Dias, R.M. Barriers to physical activity during the COVID-19 pandemic in adults: A cross-sectional study. Sport Sci. Health 2021, 17, 441–447. [Google Scholar] [CrossRef] [PubMed]
- Stockwell, S.; Trott, M.; Tully, M.; Shin, J.; Barnett, Y.; Butler, L.; McDermott, D.; Schuch, F.; Smith, L. Changes in physical activity and sedentary behaviours from before to during the COVID-19 pandemic lockdown: A systematic review. BMJ Open Sport Exerc. Med. 2021, 7, e000960. [Google Scholar] [CrossRef]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; LaMonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P.; American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Lee, I.-M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Rebar, A.L.; Stanton, R.; Geard, D.; Short, C.; Duncan, M.J.; Vandelanotte, C. A meta-meta-analysis of the effect of physical activity on depression and anxiety in non-clinical adult populations. Health Psychol. Rev. 2015, 9, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Chastin, S.F.M.; Abaraogu, U.; Bourgois, J.G.; Dall, P.M.; Darnborough, J.; Duncan, E.; Dumortier, J.; Pavón, D.J.; McParland, J.; Roberts, N.J.; et al. Effects of Regular Physical Activity on the Immune System, Vaccination and Risk of Community-Acquired Infectious Disease in the General Population: Systematic Review and Meta-Analysis. Sports Med. 2021, 51, 1673–1686. [Google Scholar] [CrossRef] [PubMed]
- Frontini, R.; Rebelo-Gonçalves, R.; Amaro, N.; Salvador, R.; Matos, R.; Morouço, P.; Antunes, R. The Relationship between Anxiety Levels, Sleep, and Physical Activity During COVID-19 Lockdown: An Exploratory Study. Front. Psychol. 2021, 12, 659599. [Google Scholar] [CrossRef]
- Puccinelli, P.J.; da Costa, T.S.; Seffrin, A.; de Lira, C.A.B.; Vancini, R.L.; Nikolaidis, P.T.; Knechtle, B.; Rosemann, T.; Hill, L.; Andrade, M.S. Correction to: Reduced level of physical activity during COVID-19 pandemic is associated with depression and anxiety levels: An internet-based survey. BMC Public Health 2021, 21, 1. [Google Scholar] [CrossRef]
- Wilke, J.; Hollander, K.; Mohr, L.; Edouard, P.; Fossati, C.; González-Gross, M.; Ramírez, C.S.; Laiño, F.; Tan, B.; Pillay, J.D.; et al. Drastic Reductions in Mental Well-Being Observed Globally During the COVID-19 Pandemic: Results From the ASAP Survey. Front. Med. 2021, 8, 578959. [Google Scholar] [CrossRef]
- Cheval, B.; Sivaramakrishnan, H.; Maltagliati, S.; Fessler, L.; Forestier, C.; Sarrazin, P.; Orsholits, D.; Chalabaev, A.; Sander, D.; Ntoumanis, N.; et al. Relationships between changes in self-reported physical activity, sedentary behaviour and health during the coronavirus (COVID-19) pandemic in France and Switzerland. J. Sports Sci. 2021, 39, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Zach, S.; Zeev, A.; Ophir, M.; Eilat-Adar, S. Physical activity, resilience, emotions, moods, and weight control of older adults during the COVID-19 global crisis. Eur. Rev. Aging Phys. Act. 2021, 18, 5. [Google Scholar] [CrossRef]
- Łaszewska, A.; Helter, T.; Simon, J. Perceptions of Covid-19 lockdowns and related public health measures in Austria: A longitudinal online survey. BMC Public Health 2021, 21, 1502. [Google Scholar] [CrossRef] [PubMed]
- Charbonnier, E.; Le Vigouroux, S.; Goncalves, A. Psychological Vulnerability of French University Students during the COVID-19 Pandemic: A Four-Wave Longitudinal Survey. Int. J. Environ. Res. Public Health 2021, 18, 9699. [Google Scholar] [CrossRef]
- Salfi, F.; D’Atri, A.; Tempesta, D.; Ferrara, M. Sleeping under the waves: A longitudinal study across the contagion peaks of the COVID-19 pandemic in Italy. J. Sleep Res. 2021, 30, e13313. [Google Scholar] [CrossRef]
- Conte, F.; Cellini, N.; De Rosa, O.; Rescott, M.L.; Malloggi, S.; Giganti, F.; Ficca, G. Dissociated profiles of sleep timing and sleep quality changes across the first and second wave of the COVID-19 pandemic. J. Psychiatr. Res. 2021, 143, 222–229. [Google Scholar] [CrossRef]
- Adam, D. Special report: The simulations driving the world’s response to COVID-19. Nat. Cell Biol. 2020, 580, 316–318. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Kosinski, M.; Matz, S.C.; Gosling, S.D.; Popov, V.; Stillwell, D. Facebook as a research tool for the social sciences: Opportunities, challenges, ethical considerations, and practical guidelines. Am. Psychol. 2015, 70, 543–556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Brislin, R.W. Back-translation for cross-cultural research. J. Cross Cult. Psychol. 1970, 1, 185–216. [Google Scholar] [CrossRef]
- Georgopoulos, V.C.; Perdikogianni, M.; Mouskenteri, M.; Psychogiou, L.; Oikonomou, M.; Malandraki, G.A. Cross-Cultural Adaptation and Validation of the SWAL-QoL Questionnaire in Greek. Dysphagia 2018, 33, 91–99. [Google Scholar] [CrossRef]
- Maher, J.P.; Hevel, D.J.; Reifsteck, E.J.; Drollette, E.S. Physical activity is positively associated with college students’ positive affect regardless of stressful life events during the COVID-19 pandemic. Psychol. Sport Exerc. 2021, 52, 101826. [Google Scholar] [CrossRef] [PubMed]
- Hamama, L.; Ronen, T.; Shachar, K.; Rosenbaum, M. Links between Stress, Positive and Negative Affect, and Life Satisfaction Among Teachers in Special Education Schools. J. Happiness Stud. 2013, 14, 731–751. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R.T. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Kandel, D.B. Epidemiology of Depressive Mood in Adolescents. Arch. Gen. Psychiatry 1982, 39, 1205–1212. [Google Scholar] [CrossRef] [PubMed]
- Cecchini, J.A.; Carriedo, A.; Fernández-Río, J.; Méndez-Giménez, A.; González, C.; Sánchez-Martínez, B.; Rodríguez-González, P. A longitudinal study on depressive symptoms and physical activity during the Spanish lockdown. Int. J. Clin. Health Psychol. 2021, 21, 100200. [Google Scholar] [CrossRef] [PubMed]
- Moradian, S.; Bäuerle, A.; Schweda, A.; Musche, V.; Kohler, H.; Fink, M.; Weismüller, B.; Benecke, A.-V.; Dörrie, N.; Skoda, E.-M.; et al. Differences and similarities between the impact of the first and the second COVID-19-lockdown on mental health and safety behaviour in Germany. J. Public Health 2021. [Google Scholar] [CrossRef]
- Davidovitz, M.; Cohen, N. Playing defence: The impact of trust on the coping mechanisms of street-level bureaucrats. Public Manag. Rev. 2020, 220, 1–22. [Google Scholar] [CrossRef]
- Milgram, N. (Noach) Stress and Coping in Israel during the Persian Gulf War. J. Soc. Issues 1993, 49, 103–123. [Google Scholar] [CrossRef]
- Bleich, A. Exposure to Terrorism, Stress-Related Mental Health Symptoms, and Coping Behaviors among a Nationally Representative Sample in Israel. JAMA 2003, 290, 612–620. [Google Scholar] [CrossRef] [Green Version]
- Clarfield, A.M.; Manor, O.; Bin Nun, G.; Shvarts, S.; Azzam, Z.S.; Afek, A.; Basis, F.; Israeli, A. Health and health care in Israel: An introduction. Lancet 2017, 389, 2503–2513. [Google Scholar] [CrossRef]
- Muhsen, K.; Cohen, D. COVID-19 vaccination in Israel. Clin. Microbiol. Infect. 2021, 27, 1570–1574. [Google Scholar] [CrossRef]
- Guidetti, M.; Averna, A.; Castellini, G.; Dini, M.; Marino, D.; Bocci, T.; Ferrucci, R.; Priori, A. Physical Activity during COVID-19 Lockdown: Data from an Italian Survey. Healthcare 2021, 9, 513. [Google Scholar] [CrossRef] [PubMed]
- Gierc, M.; Riazi, N.A.; Fagan, M.J.; Di Sebastiano, K.M.; Kandola, M.; Priebe, C.S.; Weatherson, K.A.; Wunderlich, K.B.; Faulkner, G. Strange Days: Adult Physical Activity and Mental Health in the First Two Months of the COVID-19 Pandemic. Front. Public Health 2021, 9, 567552. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Variable | Factors | 1st Wave | 2nd Wave | p |
|---|---|---|---|---|
| Mean (SD) or N(%) | ||||
| Age (years) | 48.9 (14.5) | |||
| BMI (Kg/m2) | 25.1 (4.3) | |||
| Men (%) | 42 (31) | |||
| Resilience | Positive acceptance of change | 0.31 (0.7) | 3.4 (0.6) | <0.01 |
| Personal ability, self-competence, and self-control | 3.1 (0.5) | 3.3 (0.7) | <0.01 | |
| Emotions (PANAS) | Positive | 3.0 (0.8) | 3.5 (0.8) | <0.01 |
| Negative | 1.9 (0.8) | 2.1 (0.8) | 0.42 | |
| Depression | 2.0 (0.6) | 1.8 (0.6) | 0.02 | |
| Significance | 2nd Wave [n (%)] | 1st Wave [n (%)] | PA Quantity |
|---|---|---|---|
| Not at all | (17.8) 24 | (23.0) 31 | p = 0.28 |
| Less than recommended | (22.2) 30 | (26.7) 36 | |
| In line with or higher than recommendations | (60.0) 81 | (50.4) 68 |
| Category I Increased PA Mean (SD) | Category II No Change in PA Mean (SD) | Category III Decreased PA Mean (SD) | p Time X Group | p between Times | p between Groups | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | 1st | 2nd | p | d | 1st | 2nd | p | d | 1st | 2nd | p | d | ||||
| Resilience | Positive acceptance of change | 3.0 (0.7) | 3.3 (0.6) | <0.01 | 0.49 | 3.1 (0.7) | 3.3 (0.5) | 0.01 | 0.38 | 3.2 (0.7) | 3.4 (0.6) | 0.08 | 0.25 | 00.74 | <0.01 | 0.43 |
| Personal ability, self-competence, and self-control | 0.30 (0.7) | 0.33 (0.5) | <0.01 | 0.54 | 3.1 (0.6) | 3.3 (0.5) | 0.09 | 0.29 | 3.2 (0.6) | 3.4 (0.5) | 0.14 | 0.21 | 0.33 | <0.01 | 0.39 | |
| Emotions (PANAS) | Positive | 3.0 (0.7) | 3.3 (0.6) | 0.06 | 0.62 | 3.1 (0.7) | 3.3 (0.6) | 0.01 | 0.51 | 3.2 (0.7) | 3.4 (0.6) | 0.08 | 0.52 | 0.67 | <0.01 | 0.98 |
| Negative | 0.22 (0.9) | 1.9 (0.8) | 0.22 | 0.17 | 1.9 (0.7) | 1.9 (0.8) | 0.76 | 0.05 | 1.8 (0.7) | 2.2 (0.7) | <0.01 | 0.52 | <0.01 | 0.42 | 0.47 | |
| Depression | 1.9 (0.6) | 0.18 (0.6) | 0.22 | 0.21 | 2.1 (0.7) | 1.8 (0.6) | 0.001 | 0.39 | 1.9 (0.6) | 1.9 (0.7) | 0.97 | 0.01 | 0.68 | 0.03 | 0.18 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zach, S.; Eilat-Adar, S.; Ophir, M.; Dotan, A. Differences in the Association between Physical Activity and People’s Resilience and Emotions during Two Consecutive Covid-19 Lockdowns in Israel. Int. J. Environ. Res. Public Health 2021, 18, 13217. https://doi.org/10.3390/ijerph182413217
Zach S, Eilat-Adar S, Ophir M, Dotan A. Differences in the Association between Physical Activity and People’s Resilience and Emotions during Two Consecutive Covid-19 Lockdowns in Israel. International Journal of Environmental Research and Public Health. 2021; 18(24):13217. https://doi.org/10.3390/ijerph182413217
Chicago/Turabian StyleZach, Sima, Sigal Eilat-Adar, Miki Ophir, and Avital Dotan. 2021. "Differences in the Association between Physical Activity and People’s Resilience and Emotions during Two Consecutive Covid-19 Lockdowns in Israel" International Journal of Environmental Research and Public Health 18, no. 24: 13217. https://doi.org/10.3390/ijerph182413217