
Relative Lean Body Mass and Waist Circumference for the Identification of Metabolic Syndrome in the Korean General Population


Abstract
:1. Introduction
2. Materials and Methods
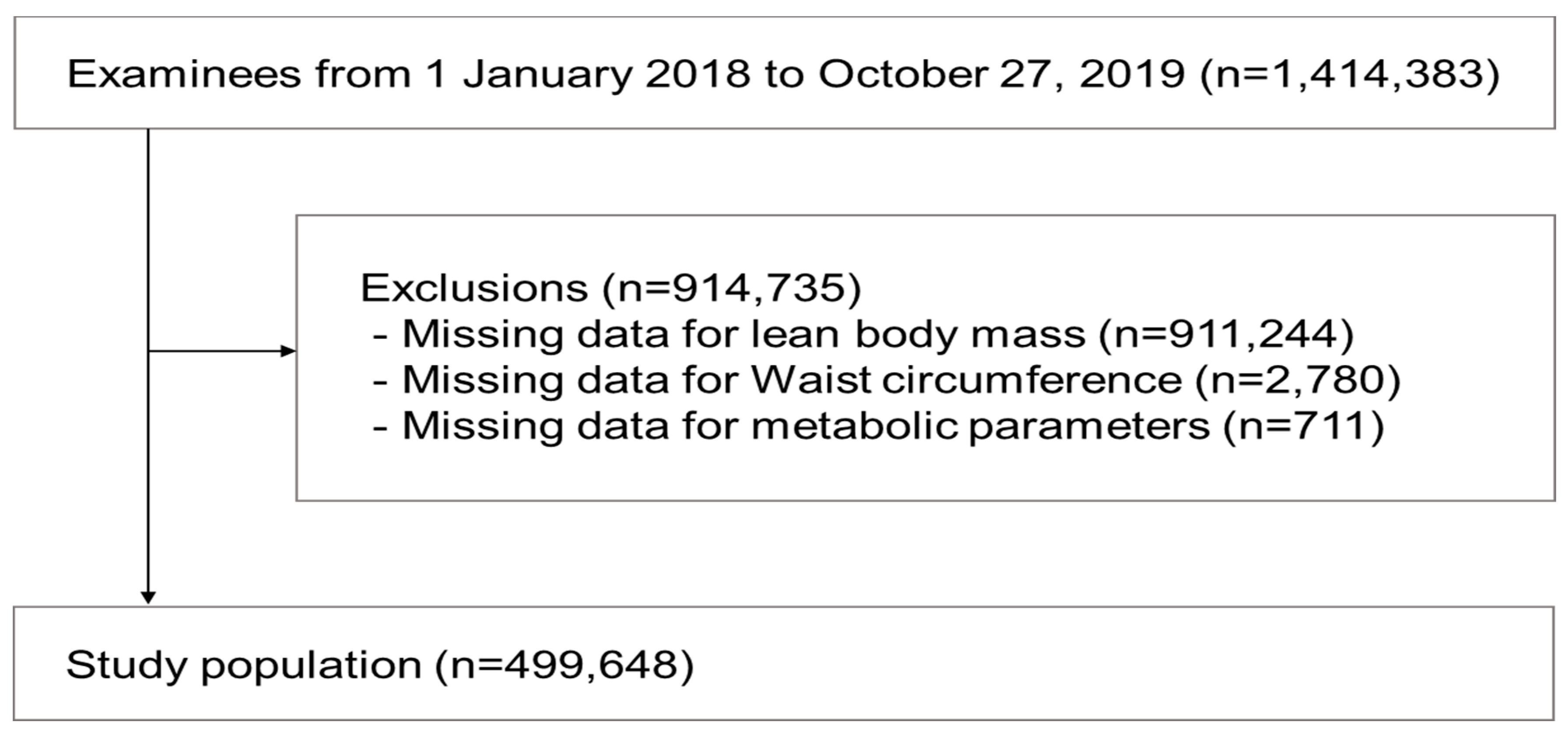
2.1. Study Subjects
2.2. Measurement of Lean Body Mass
2.3. Laboratory Measurements
2.4. Grouping of Study Subjects Using the Combination of LBM and WC
2.5. Definition of Metabolically Unhealthy Status
2.6. Statistical Analysis
3. Results
3.1. Characteristics of the Study Subjects According to Categories of RLBM
3.2. Prevalence of Metabolic Abnormalities in Groups of Subjects
3.3. Association of Metabolic Abnormalities with Groups of Subjects
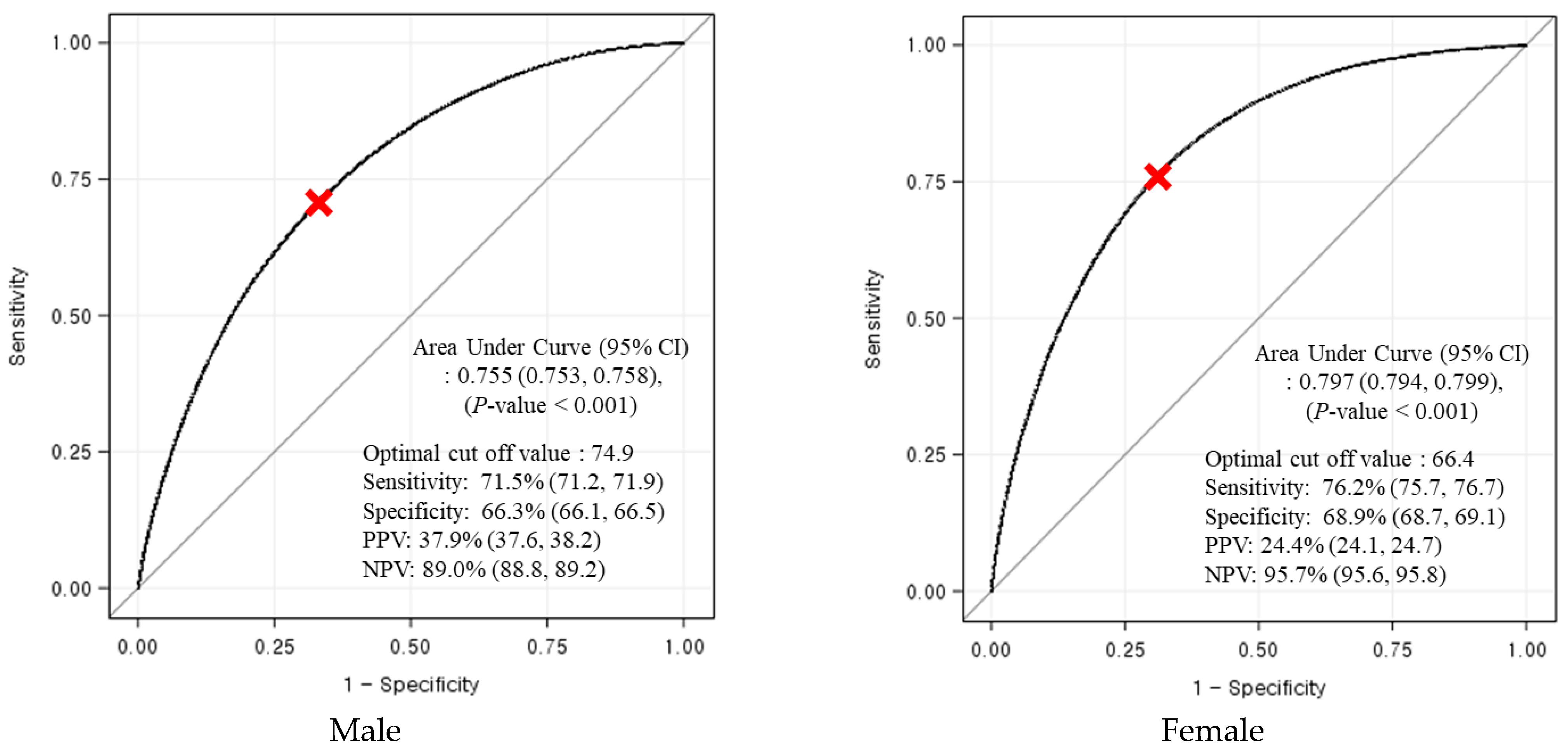
3.4. Determination of the Optimal Cut-Offs of RLBM for Predicting Metabolic Syndrome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Klein, S.; Wadden, T.; Sugerman, H.J. AGA technical review on obesity. Gastroenterology 2002, 123, 882–932. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, N.T.; Magno, C.P.; Lane, K.T.; Hinojosa, M.W.; Lane, J.S. Association of hypertension, diabetes, dyslipidemia, and metabolic syndrome with obesity: Findings from the National Health and Nutrition Examination Survey, 1999 to 2004. J. Am. Coll. Surg. 2008, 207, 928–934. [Google Scholar] [CrossRef] [PubMed]
- GBD 2015 Obesity Collaborators. Health effects of overweight and obesity in 195 countries over 25 years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Physical Status: The Use and Interpretation of Anthropometry. Report of a WHO Expert Consultation; World Health Organization: Geneva, Switzerland, 1995; Available online: https://apps.who.int/iris/handle/10665/37003 (accessed on 1 July 2020).
- Romero-Corral, A.; Somers, V.K.; Sierra-Johnson, J.; Thomas, R.; Collazo-Clavell, M.L.; Korinek, J.; Allison, T.G.; Batsis, J.A.; Kuniyoshi, F.S.; Lopez-Jimenez, F. Accuracy of body mass index in diagnosing obesity in the adult general population. Int. J. Obes. 2008, 32, 959–966. [Google Scholar] [CrossRef] [Green Version]
- Rothman, K.J. BMI-related errors in the measurement of obesity. Int. J. Obes. 2008, 32, S56–S59. [Google Scholar] [CrossRef] [Green Version]
- Flegal, K.M.; Shepherd, J.A.; Looker, A.C.; Graubard, B.I.; Borrud, L.G.; Ogden, C.L.; Harris, T.B.; Everhart, J.E.; Schenker, N. Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. Am. J. Clin. Nutr. 2008, 89, 500–508. [Google Scholar] [CrossRef] [PubMed]
- Hajian-Tilaki, K.; Heidari, B. Variations in the pattern and distribution of non-obese components of metabolic syndrome across different obesity phenotypes among Iranian adults’ population. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2419–2424. [Google Scholar] [CrossRef]
- Janssen, I.; Katzmarzyk, P.; Ross, R. Waist circumference and not body mass index explains obesity-related health risk. Am. J. Clin. Nutr. 2004, 79, 379–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bigaard, J.; Frederiksen, K.; Tjonneland, A.; Thomsen, B.L.; Overvad, K.; Heitmann, B.L.; Sørensen, T.I.A. Waist circumference and body composition in relation to all-cause mortality in middle-aged men and women. Int. J. Obes. 2005, 29, 778–784. [Google Scholar] [CrossRef] [Green Version]
- Kim, Y.-H.; Kim, S.M.; Han, K.-D.; Jung, J.-H.; Lee, S.-S.; Oh, S.W.; Park, H.S.; Rhee, E.-J.; Lee, W.-Y.; Yoo, S.J. Waist circumference and all-cause mortality independent of body mass index in Korean population from the national health insurance health checkup 2009–2015. J. Clin. Med. 2019, 8, 72. [Google Scholar] [CrossRef] [Green Version]
- Takamura, T.; Kita, Y.; Nakagen, M.; Sakurai, M.; Isobe, Y.; Takeshita, Y.; Kawai, K.; Urabe, T.; Kaneko, S. Weight-adjusted lean body mass and calf circumference are protective against obesity-associated insulin resistance and metabolic abnormalities. Heliyon 2017, 3, e00347. [Google Scholar] [CrossRef] [Green Version]
- Kershaw, E.E.; Flier, J.S. Adipose tissue as an endocrine organ. J. Clin. Endocrinol. Metab. 2004, 89, 2548–2556. [Google Scholar] [CrossRef] [PubMed]
- Wannamethee, S.G.; Atkins, J. Muscle loss and obesity: The health implications of sarcopenia and sarcopenic obesity. Proc. Nutr. Soc. 2015, 74, 405–412. [Google Scholar] [CrossRef]
- Hioki, H.; Miura, T.; Motoki, H.; Kobayashi, H.; Kobayashi, M.; Nakajima, H.; Sekimura, N.; Mawatari, E.; Akanuma, H.; Sato, T.; et al. Lean body mass index prognostic value for cardiovascular events in patients with coronary artery disease. Hear. Asia 2015, 7, 12–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kalyani, R.R.; Tra, Y.; Egan, J.M.; Ferrucci, L.; Brancati, F. Hyperglycemia is associated with relatively lower lean body mass in older adults. J. Nutr. Health Aging 2014, 18, 737–743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gupta, P.; Lanca, C.; Gan, A.T.L.; Soh, P.; Thakur, S.; Tao, Y.; Kumari, N.; Man, R.E.K.; Fenwick, E.K.; Lamoureux, E.L. The association between body composition using dual energy X-ray absorptiometry and type-2 diabetes: A systematic review and meta-analysis of observational studies. Sci. Rep. 2019, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Khazem, S.; Itani, L.; Kreidieh, D.; El Masri, D.; Tannir, H.; Citarella, R.; El Ghoch, M. Reduced lean body mass and cardiometabolic diseases in adult males with overweight and obesity: A pilot study. Int. J. Environ. Res. Public Health 2018, 15, 2754. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, G.; Lee, S.-E.; Jun, J.E.; Lee, Y.-B.; Ahn, J.; Bae, J.C.; Jin, S.-M.; Hur, K.Y.; Jee, J.H.; Lee, M.-K.; et al. Increase in relative skeletal muscle mass over time and its inverse association with metabolic syndrome development: A 7-year retrospective cohort study. Cardiovasc. Diabetol. 2018, 17, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, B.S.; Yoon, J.S. Relative skeletal muscle mass is associated with development of metabolic syndrome. Diabetes Metab. J. 2013, 37, 458–464. [Google Scholar] [CrossRef] [Green Version]
- Yoon, Y.S.; Oh, S.W. Optimal waist circumference cutoff values for the diagnosis of abdominal obesity in Korean adults. Endocrinol Metab. 2014, 29, 418–426. [Google Scholar] [CrossRef] [Green Version]
- Campa, F.; Toselli, S.; Mazzilli, M.; Gobbo, L.A.; Coratella, G. Assessment of body composition in athletes: A narrative review of available methods with special reference to quantitative and qualitative bioimpedance analysis. Nutrients 2021, 13, 1620. [Google Scholar] [CrossRef] [PubMed]
- Di Vincenzo, O.; Marra, M.; Di Gregorio, A.; Pasanisi, F.; Scalfi, L. Bioelectrical impedance analysis (BIA) -derived phase angle in sarcopenia: A systematic review. Clin. Nutr. 2021, 40, 3052–3061. [Google Scholar] [CrossRef] [PubMed]
- Rojo, F.; de Cangas, R.; Nicieza, G.; Zamarreno, D. Cross-sectional study on the relation between the phase angle and the musculoskeletal mass: Discriminating phenotypes of body composition addressed to precision nutrition. Bariatr. Metab. Ibero-Am. 2019, 9, 2605–2607. [Google Scholar]
- Gonzalez, M.C.; Heymsfield, S.B. Bioelectrical impedance analysis for diagnosing sarcopenia and cachexia: What are we really estimating? J. Cachexia Sarcopenia Muscle. 2017, 8, 187–189. [Google Scholar] [CrossRef] [PubMed]
- InBody. InBody770 User’s Manual; InBody Co., Ltd.: Seoul, Korea, 2015; pp. 31–33. [Google Scholar]
- Lee, S.Y.; Ahn, S.; Kim, Y.J.; Ji, M.J.; Kim, K.M.; Choi, S.H.; Jang, H.C.; Lim, S. Comparison between dual-energy X-ray absorptiometry and bioelectrical impedance analyses for accuracy in measuring whole body muscle mass and appendicular skeletal muscle mass. Nutrients 2018, 10, 738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Expert Panel on Detection, Evaluation. Executive Summary of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef] [PubMed]
- Laaksonen, D.E.; Lakka, H.-M.; Niskanen, L.K.; Kaplan, G.A.; Salonen, J.T.; Lakka, T. Metabolic Syndrome and Development of Diabetes Mellitus: Application and Validation of recently suggested definitions of the metabolic syndrome in a prospective cohort study. Am. J. Epidemiol. 2002, 156, 1070–1077. [Google Scholar] [CrossRef] [PubMed]
- Ruud, J.; Steculorum, S.; Brüning, J.C. Neuronal control of peripheral insulin sensitivity and glucose metabolism. Nat. Commun. 2017, 8, 15259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shou, J.; Chen, P.-J.; Xiao, W.-H. Mechanism of increased risk of insulin resistance in aging skeletal muscle. Diabetol. Metab. Syndr. 2020, 12, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Srikanthan, P.; Karlamangla, A.S. Relative muscle mass is inversely associated with insulin resistance and prediabetes. findings from The Third National Health and Nutrition Examination Survey. J. Clin. Endocrinol. Metab. 2011, 96, 2898–2903. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleasby, M.E.; Jarmin, S.; Eilers, W.; Elashry, M.; Andersen, D.K.; Dickson, G.; Foster, K. Local overexpression of the myostatin propeptide increases glucose transporter expression and enhances skeletal muscle glucose disposal. Am. J. Physiol. Metab. 2014, 306, E814–E823. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zheng, D.; Liu, J.; Fang, L.; Li, Q. Skeletal muscle mass to visceral fat area ratio is an important determinant associated with type 2 diabetes and metabolic syndrome. Diabetes Metab. Syndr. Obes. Targets Ther. 2019, 12, 1399–1407. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.; Park, S.M. Association of muscle mass and fat mass with insulin resistance and the prevalence of metabolic syndrome in Korean adults: A cross-sectional study. Sci. Rep. 2018, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, S.; Connell, J. The link between abdominal obesity, metabolic syndrome and cardiovascular disease. Nutr. Metab. Cardiovasc. Dis. 2007, 17, 319–326. [Google Scholar] [CrossRef]
- Wajchenberg, B.L. Subcutaneous and visceral adipose tissue: Their relation to the metabolic syndrome. Endocr. Rev. 2000, 21, 697–738. [Google Scholar] [CrossRef] [PubMed]
- Laurens, C.; Moro, C. Intramyocellular fat storage in metabolic diseases. Horm. Mol. Biol. Clin. Investig. 2015, 26, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Sinha, R.; Dufour, S.; Petersen, K.F.; Lebon, V.; Enoksson, S.; Ma, Y.-Z.; Savoye, M.; Rothman, D.L.; Shulman, G.; Caprio, S. Assessment of skeletal muscle triglyceride content by 1H nuclear magnetic resonance spectroscopy in lean and obese adolescents: Relationships to insulin sensitivity, total body fat, and central adiposity. Diabetes 2002, 51, 1022–1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacob, S.; Machann, J.; Rett, K.; Brechtel, K.; Volk, A.; Renn, W.; Maerker, E.; Matthaei, S.; Schick, F.; Claussen, C.D.; et al. Association of increased intramyocellular lipid content with insulin resistance in lean nondiabetic offspring of type 2 diabetic subjects. Diabetes 1999, 48, 1113–1119. [Google Scholar] [CrossRef] [PubMed]
- Donini, L.M.; Poggiogalle, E.; del Balzo, V.; Lubrano, C.; Faliva, M.; Opizzi, A.; Perna, S.; Pinto, A.; Rondanelli, M. How to estimate fat mass in overweight and obese Subjects. Int. J. Endocrinol. 2013, 2013, 285680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, J.-G.; Zhang, Y.; Chen, H.-E.; Li, Y.; Cheng, X.-G.; Xu, L.; Guo, Z.; Zhao, X.-S.; Sato, T.; Cao, Q.-Y.; et al. Comparison of Two Bioelectrical Impedance Analysis Devices with Dual Energy X-ray Absorptiometry and Magnetic Resonance Imaging in the Estimation of Body Composition. J. Strength Cond. Res. 2013, 27, 236–243. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Total | Q1 | Q2 | Q3 | Q4 | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall | |||||||||||
| RLBM (%), Range | 13.96–67.77 | 67.78–72.77 | 72.78–77.06 | 77.07–98.86 | |||||||
| Number, N | N = 499,648 | N = 124,912 | N = 124,929 | N = 124,895 | N = 124,912 | ||||||
| Males | |||||||||||
| RLBM (%), Range | 13.96–72.48 | 72.49–75.89 | 75.90–79.33 | 79.34–98.86 | |||||||
| Number, N | 263,735 | 65,941 | 65,927 | 65,947 | 65,920 | <0.001 | |||||
| Age (year) | 47.7 | (12.2) | 47.7 | (12.8) | 48.6 | (11.9) | 48.1 | (11.7) | 46.4 | (12.5) | <0.001 |
| Hypertension, N (%) | 97,368 | (36.9) | 34,160 | (51.8) | 26,093 | (39.6) | 21,564 | (32.7) | 15,551 | (23.6) | <0.001 |
| Type 2 diabetes, N (%) | 29,710 | (11.3) | 10,872 | (16.5) | 7963 | (12.1) | 6294 | (9.5) | 4581 | (6.9) | <0.001 |
| Metabolically unhealthy, N (%) | 94,024 | (35.7) | 35,013 | (53.1) | 26,591 | (40.3) | 20,722 | (31.4) | 11,698 | (17.7) | <0.001 |
| Metabolic syndrome, N (%) | 58,966 | (22.4) | 29,976 | (45.5) | 16,439 | (24.9) | 9134 | (13.9) | 3417 | (5.2) | <0.001 |
| BMI (kg/m2) | 25.1 | (6.1) | 28.2 | (3.1) | 25.7 | (10.6) | 24.2 | (2.1) | 22.3 | (2.2) | <0.001 |
| WC (cm) | 86.6 | (8.4) | 94.6 | (7.7) | 88.2 | (5.5) | 84.5 | (5.4) | 78.9 | (6.1) | <0.001 |
| Systolic BP (mmHg) | 120.3 | (13.1) | 124.4 | (13.2) | 120.9 | (12.9) | 119.2 | (12.6) | 116.8 | (12.3) | <0.001 |
| Diastolic BP (mmHg) | 76.6 | (9.4) | 79.5 | (9.6) | 77.2 | (9.2) | 75.9 | (9.0) | 73.9 | (8.9) | <0.001 |
| FBS (mg/dL) | 100.3 | (22.4) | 104.8 | (25.3) | 101.5 | (22.2) | 99.1 | (20.6) | 96.0 | (20.4) | <0.001 |
| HDL-C (mg/dL) | 50.5 | (11.6) | 47.1 | (10.0) | 48.8 | (10.6) | 50.7 | (11.3) | 55.3 | (12.8) | <0.001 |
| TG (mg/dL) | 145.8 | (106.1) | 177.4 | (118.1) | 158.8 | (109.5) | 140.1 | (99.4) | 106.9 | (80.6) | <0.001 |
| Females | |||||||||||
| RLBM (%), Range | 15.17–64.52 | 64.53–68.46 | 68.47–72.58 | 72.59–97.85 | |||||||
| Number, N | 235,913 | 59,017 | 58,944 | 58,987 | 58,965 | <0.001 | |||||
| Age (year) | 48.3 | (12.9) | 52.4 | (13.1) | 50.5 | (12.5) | 47.5 | (12.1) | 42.9 | (11.7) | <0.001 |
| Hypertension, N (%) | 55,714 | (23.6) | 24,129 | (40.9) | 15,538 | (26.4) | 10,214 | (17.3) | 5833 | (9.9) | <0.001 |
| Type 2 diabetes, N (%) | 15,917 | (6.7) | 7306 | (12.4) | 4431 | (7.5) | 2740 | (4.6) | 1440 | (2.4) | <0.001 |
| Metabolically unhealthy, N (%) | 48,066 | (20.4) | 22,312 | (37.8) | 14,051 | (23.8) | 8274 | (14.0) | 3429 | (5.8) | <0.001 |
| Metabolic syndrome, N (%) | 27,430 | (11.6) | 17,016 | (28.8) | 6877 | (11.7) | 2732 | (4.6) | 805 | (1.4) | <0.001 |
| BMI (kg/m2) | 23.2 | (3.4) | 26.9 | (3.4) | 23.8 | (2.1) | 22.0 | (1.7) | 20.0 | (1.6) | <0.001 |
| WC (cm) | 76.9 | (9.4) | 85.6 | (8.5) | 78.7 | (7.1) | 74.3 | (5.8) | 69.0 | (6.6) | <0.001 |
| Systolic BP (mmHg) | 114.7 | (14.4) | 121.5 | (14.4) | 116.2 | (13.8) | 112.4 | (13.4) | 108.6 | (12.5) | <0.001 |
| Diastolic BP (mmHg) | 71.8 | (9.2) | 75.5 | (9.3) | 72.6 | (8.9) | 70.5 | (8.6) | 68.5 | (8.2) | <0.001 |
| FBS (mg/dL) | 94.4 | (17.3) | 99.9 | (20.9) | 95.7 | (17.4) | 92.5 | (15.1) | 89.3 | (13.0) | <0.001 |
| HDL-C (mg/dL) | 60.1 | (13.5) | 55.7 | (12.2) | 58.2 | (12.8) | 61.0 | (13.2) | 65.5 | (13.6) | <0.001 |
| TG (mg/dL) | 96.4 | (63.6) | 119.3 | (72.1) | 105.0 | (67.5) | 89.5 | (57.6) | 71.8 | (43.2) | <0.001 |
| Total | H-RLBM/N-WC | L-RLBM/N-WC | H-RLBM/A-WC | L-RLBM/A-WC | p-Value | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Overall | 499,648 | (100.0) | 323,960 | (64.8) | 46,039 | (9.2) | 50,730 | (10.2) | 78,919 | (15.8) | |
| Males | 263,735 | (100.0) | 160,394 | (60.8) | 17,662 | (6.7) | 37,400 | (14.2) | 48,279 | (18.3) | |
| BP ≥ 130/85 mmHg | 80,619 | (30.6) | 38,458 | (24.0) | 6604 | (37.4) | 13,618 | (36.4) | 21,939 | (45.4) | <0.001 |
| FBS ≥ 100 mg/dL | 95,286 | (36.1) | 48,150 | (30.0) | 7278 | (41.2) | 16,358 | (43.7) | 23,500 | (48.7) | <0.001 |
| TG ≥ 150 mg/dL | 92,662 | (35.1) | 42,879 | (26.7) | 7457 | (42.2) | 17,032 | (45.5) | 25,294 | (52.4) | <0.001 |
| HDL-C < 40 mg/dL | 41,108 | (15.6) | 18,564 | (11.6) | 3049 | (17.3) | 7921 | (21.2) | 11,574 | (24.0) | <0.001 |
| Metabolically unhealthy | 94,024 | (35.7) | 41,459 | (25.8) | 7728 | (43.8) | 17,552 | (46.9) | 27,285 | (56.5) | <0.001 |
| Females | 235,913 | (100.0) | 163,566 | (69.3) | 28,377 | (12.0) | 13,330 | (5.7) | 30,640 | (13.0) | |
| BP ≥ 130/85 mmHg | 43,709 | (18.5) | 20,571 | (12.6) | 7198 | (25.4) | 3893 | (29.2) | 12,047 | (39.3) | <0.001 |
| FBS ≥ 100 mg/dL | 52,269 | (22.2) | 26,071 | (15.9) | 7976 | (28.1) | 4705 | (35.3) | 13,517 | (44.1) | <0.001 |
| TG ≥ 150 mg/dL | 32,416 | (13.7) | 15,483 | (9.5) | 5140 | (18.1) | 3210 | (24.1) | 8583 | (28.0) | <0.001 |
| HDL-C < 50 mg/dL | 51,003 | (21.6) | 27,366 | (16.7) | 7634 | (26.9) | 4471 | (33.5) | 11,532 | (37.6) | <0.001 |
| Metabolically unhealthy | 48,066 | (20.4) | 20,928 | (12.8) | 7849 | (27.7) | 4826 | (36.2) | 14,463 | (47.2) | <0.001 |
| Metabolic Abnormality | H-RLBM/N-WC | L-RLBM/N-WC | H-RLBM/A-WC | L-RLBM/A-WC | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| OR | (95%CI) | p-Value | OR | (95%CI) | p-Value | OR | (95%CI) | p-Value | ||
| High BP | Ref | 1.891 | (1.849–1.934) | <0.001 | 1.936 | (1.896–1.977) | <0.001 | 3.110 | (3.057–3.163) | <0.001 |
| High FBS | Ref | 1.598 | (1.563–1.634) | <0.001 | 1.928 | (1.889–1.967) | <0.001 | 2.714 | (2.669–2.761) | <0.001 |
| High TG | Ref | 1.989 | (1.943–2.036) | <0.001 | 2.411 | (2.362–2.461) | <0.001 | 3.195 | (3.140–3.250) | <0.001 |
| Low HDL-C | Ref | 1.638 | (1.599–1.678) | <0.001 | 2.117 | (2.068–2.166) | <0.001 | 2.560 | (2.513–2.609) | <0.001 |
| Metabolically unhealthy | Ref | 2.170 | (2.122–2.218) | <0.001 | 2.713 | (2.659–2.769) | <0.001 | 4.400 | (4.326–4.475) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kwon, E.; Nah, E.-H.; Kim, S.; Cho, S. Relative Lean Body Mass and Waist Circumference for the Identification of Metabolic Syndrome in the Korean General Population. Int. J. Environ. Res. Public Health 2021, 18, 13186. https://doi.org/10.3390/ijerph182413186
Kwon E, Nah E-H, Kim S, Cho S. Relative Lean Body Mass and Waist Circumference for the Identification of Metabolic Syndrome in the Korean General Population. International Journal of Environmental Research and Public Health. 2021; 18(24):13186. https://doi.org/10.3390/ijerph182413186
Chicago/Turabian StyleKwon, Eunjoo, Eun-Hee Nah, Suyoung Kim, and Seon Cho. 2021. "Relative Lean Body Mass and Waist Circumference for the Identification of Metabolic Syndrome in the Korean General Population" International Journal of Environmental Research and Public Health 18, no. 24: 13186. https://doi.org/10.3390/ijerph182413186