
Examination of Self-Esteem, Body Image, Eating Attitudes and Cardiorespiratory Performance in Adolescents

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Measurements
2.3. Questionnaires
2.3.1. Rosenberg Self-Esteem Scale
2.3.2. EAT-26
2.3.3. BAT
2.4. Data Analysis
3. Results
3.1. BMI-for-Age
3.2. The 20 m Shuttle Run Test
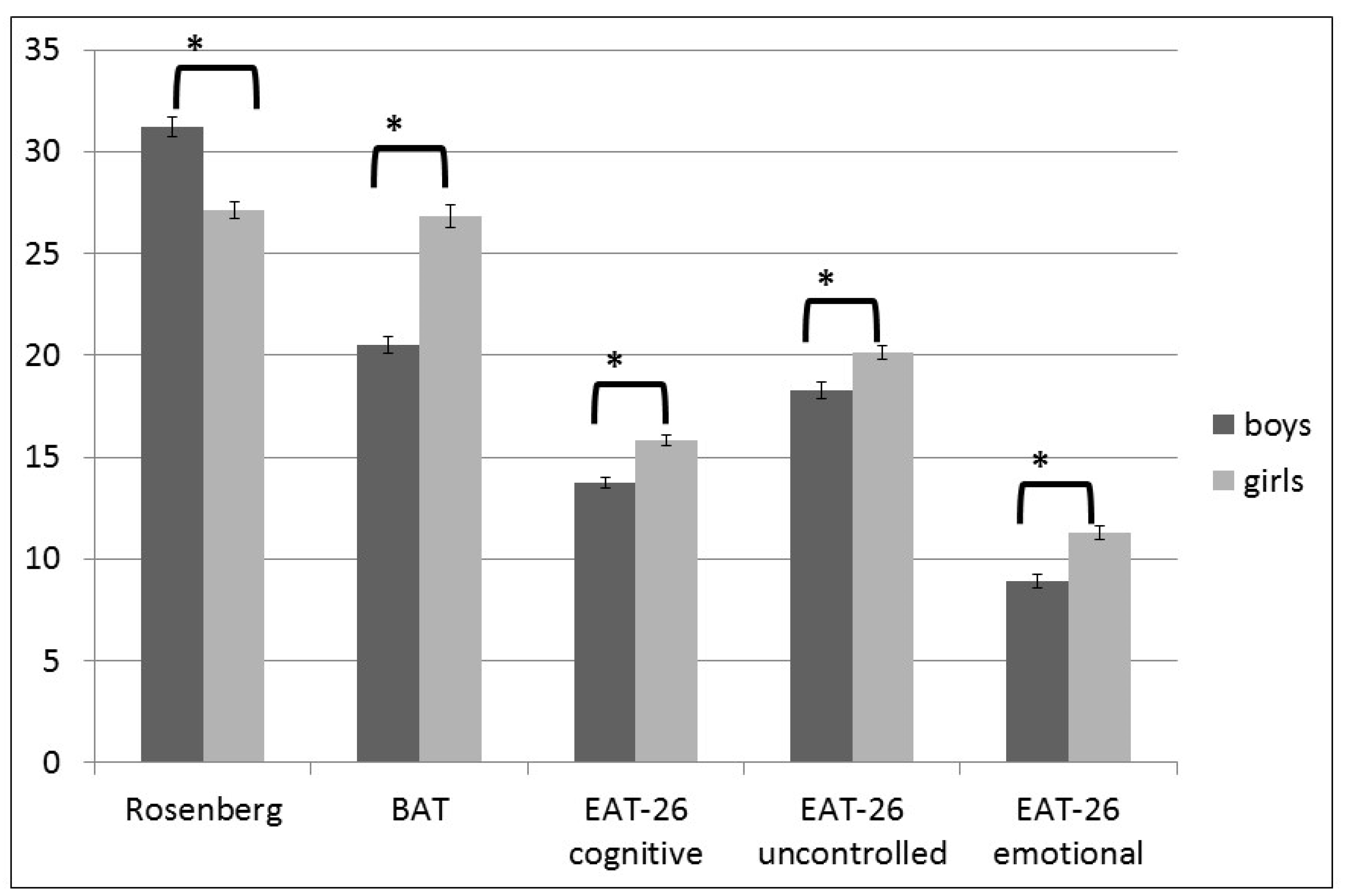
3.3. Psychological Tests Results
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hoyt, L.T.; Chase-Lansdale, P.L.; McDade, T.W.; Adam, E.K. Positive Youth, Healthy Adults: Does Positive Well-being in Adolescence Predict Better Perceived Health and Fewer Risky Health Behaviors in Young Adulthood? J. Adolesc. Health 2012, 50, 66–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McMullin, J.A.; Cairney, J. Self-esteem and the intersection of age, class, and gender. J. Aging Stud. 2004, 18, 75–90. [Google Scholar] [CrossRef]
- McClure, A.C.; Tanski, S.E.; Kingsbury, J.; Gerrard, M.; Sargent, J.D. Characteristics Associated with Low Self-Esteem Among US Adolescents. Acad. Pediatr. 2010, 10, 238–244. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, J.A.; Olnhausen, K.S. Adolescent self-esteem: A foundational disposition. Nurs. Sci. Q. 1999, 12, 62–67. [Google Scholar] [CrossRef]
- Agam, R.; Tamir, S.; Golan, M. Gender Differences in Respect to Self-Esteem and Body Image as Well as Response to Adolescent’s School-Based Prevention Programs. J. Psychol. Clin. Psychiatry 2015, 2, 00092. [Google Scholar]
- Murray, M.; Dordevic, A.L.; Bonham, M. Systematic Review and Meta-Analysis: The Impact of Multicomponent Weight Management Interventions on Self-Esteem in Overweight and Obese Adolescents. J. Pediatr. Psychol. 2017, 42, 379–394. [Google Scholar] [CrossRef] [Green Version]
- Baumeister, R.F.; Campbell, J.D.; Krueger, J.I.; Vohs, K.D. Does High Self-Esteem Cause Better Performance, Interpersonal Success, Happiness, or Healthier Lifestyles? Psychol. Sci. Public Interest 2003, 4, 1–44. [Google Scholar] [CrossRef] [Green Version]
- Knox, E.; Muros, J.J. Association of lifestyle behaviours with self-esteem through health-related quality of life in Spanish adolescents. Eur. J. Pediatr. 2017, 176, 621–628. [Google Scholar] [CrossRef] [Green Version]
- Latzer, Y.; Stein, D. A review of the psychological and familial perspectives of childhood obesity. J. Eat. Disord. 2013, 1, 7. [Google Scholar] [CrossRef] [Green Version]
- Grogan, S. Body Image: Understanding Body Dissatisfaction in Men, Women, and Children, 3rd ed.; Routledge: London, UK, 2016. [Google Scholar]
- Heider, N.; Spruyt, A.; de Houwer, J. Body Dissatisfaction Revisited: On the Importance of Implicit Beliefs about Actual and Ideal Body Image. Psychol. Belg. 2018, 57, 158–173. [Google Scholar] [CrossRef] [Green Version]
- Ata, R.N.; Ludden, A.B.; Lally, M.M. The Effects of Gender and Family, Friend, and Media Influences on Eating Behaviors and Body Image During Adolescence. J. Youth Adolesc. 2007, 36, 1024–1037. [Google Scholar] [CrossRef]
- Tiggemann, M. Body dissatisfaction and adolescent self-esteem: Prospective findings. Body Image 2005, 2, 129–135. [Google Scholar] [CrossRef]
- Voges, M.M.; Giabbiconi, C.-M.; Schöne, B.; Waldorf, M.; Hartmann, A.S.; Vocks, S. Gender Differences in Body Evaluation: Do Men Show More Self-Serving Double Standards Than Women? Front. Psychol. 2019, 10, 544. [Google Scholar] [CrossRef]
- Wang, S.B.; Haynos, A.F.; Wall, M.M.; Chen, C.; Eisenberg, M.E.; Neumark-Sztainer, D. Fifteen-Year Prevalence, Trajectories, and Predictors of Body Dissatisfaction From Adolescence to Middle Adulthood. Clin. Psychol. Sci. 2019, 7, 1403–1415. [Google Scholar] [CrossRef]
- Bearman, S.K.; Presnell, K.; Martinez, E.; Stice, E. The Skinny on Body Dissatisfaction: A Longitudinal Study of Adolescent Girls and Boys. J. Youth Adolesc. 2006, 35, 217–229. [Google Scholar] [CrossRef]
- Duchesne, A.-P.; Dion, J.; Lalande, D.; Bégin, C.; Émond, C.; Lalande, G.; McDuff, P. Body dissatisfaction and psychological distress in adolescents: Is self-esteem a mediator? J. Health Psychol. 2016, 22, 1563–1569. [Google Scholar] [CrossRef] [PubMed]
- Macêdo Uchôa, F.N.; Uchôa, N.M.; Daniele, T.M.D.C.; Lustosa, R.P.; Nogueira, P.R.C.; Reis, V.M.; Andrade, J.H.C.; Deana, N.F.; Aranha, Á.M.; Alves, N. Influence of Body Dissatisfaction on the Self-Esteem of Brazilian Adolescents: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2020, 17, 3536. [Google Scholar] [CrossRef]
- Groesz, L.M.; Levine, M.P.; Murnen, S.K. The effect of experimental presentation of thin media images on body satisfaction: A meta-analytic review. Int. J. Eat. Disord. 2002, 31, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Holland, G.; Tiggemann, M. A systematic review of the impact of the use of social networking sites on body image and disordered eating outcomes. Body Image 2016, 17, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Blundell, J.E.; Cooling, J. Routes to obesity: Phenotypes, food choices and activity. Br. J. Nutr. 2000, 83, S33–S38. [Google Scholar] [CrossRef]
- Goldschmidt, A.B.; Aspen, V.P.; Sinton, M.M.; Tanofsky-Kraff, M.; Wilfley, D.E. Disordered Eating Attitudes and Behaviors in Overweight Youth. Obesity 2008, 16, 257–264. [Google Scholar] [CrossRef]
- Garner, D.M.; Olmsted, M.P.; Bohr, Y.; Garfinkel, P.E. The Eating Attitudes Test: Psychometric features and clinical correlates. Psychol. Med. 1982, 12, 871–878. [Google Scholar] [CrossRef] [PubMed]
- Hays, N.P.; Roberts, S.B. Aspects of Eating Behaviors “Disinhibition” and “Restraint” Are Related to Weight Gain and BMI in Women. Obesity 2008, 16, 52–58. [Google Scholar] [CrossRef] [Green Version]
- Arnow, B.; Kenardy, J.; Agras, W.S. The Emotional Eating Scale: The development of a measure to assess coping with negative affect by eating. Int. J. Eat. Disord. 1995, 18, 79–90. [Google Scholar] [CrossRef]
- Koenders, P.G.; van Strien, T. Emotional Eating, Rather Than Lifestyle Behavior, Drives Weight Gain in a Prospective Study in 1562 Employees. J. Occup. Environ. Med. 2011, 53, 1287–1293. [Google Scholar] [CrossRef]
- Braden, A.; Flatt, S.W.; Boutelle, K.N.; Strong, D.; Sherwood, N.E.; Rock, C.L. Emotional eating is associated with weight loss success among adults enrolled in a weight loss program. J. Behav. Med. 2016, 39, 727–732. [Google Scholar] [CrossRef] [Green Version]
- Camilleri, G.M.; Méjean, C.; Kesse-Guyot, E.; Andreeva, V.; Bellisle, F.; Hercberg, S.; Péneau, S. The Associations between Emotional Eating and Consumption of Energy-Dense Snack Foods Are Modified by Sex and Depressive Symptomatology. J. Nutr. 2014, 144, 1264–1273. [Google Scholar] [CrossRef]
- O’Connor, D.B.; Jones, F.; Conner, M.; McMillan, B.; Ferguson, E. Effects of daily hassles and eating style on eating behavior. Health Psychol. 2008, 27, S20–S31. [Google Scholar] [CrossRef] [Green Version]
- Furnham, A.; Badmin, N.; Sneade, I. Body Image Dissatisfaction: Gender Differences in Eating Attitudes, Self-Esteem, and Reasons for Exercise. J. Psychol. 2002, 136, 581–596. [Google Scholar] [CrossRef] [PubMed]
- Limbers, C.A.; Cohen, L.A.; Gray, B.A. Eating disorders in adolescent and young adult males: Prevalence, diagnosis, and treatment strategies. Adolesc. Health Med. Ther. 2018, 9, 111–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingstone, B. Epidemiology of childhood obesity in Europe. Eur. J. Nucl. Med. Mol. Imaging 2000, 159, S14–S34. [Google Scholar] [CrossRef]
- Ruiz, J.R.; Rizzo, N.S.; Hurtig-Wennlöf, A.; Ortega, F.B.; Àrnberg, J.W.; Sjöström, M. Relations of total physical activity and intensity to fitness and fatness in children: The European Youth Heart Study1–3. Am. J. Clin. Nutr. 2006, 84, 299–303. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.E.; Baker, J.S.; Davies, B. Established and Recently Identified Coronary Heart Disease Risk Factors in Young People. Sports Med. 2003, 33, 633–650. [Google Scholar] [CrossRef] [PubMed]
- Brage, S.; Wedderkopp, N.; Ekelund, U.; Franks, P.W.; Wareham, N.J.; Andersen, L.B.; Froberg, K. Features of the Metabolic Syndrome Are Associated with Objectively Measured Physical Activity and Fitness in Danish Children: The European Youth Heart Study (EYHS). Diabetes Care 2004, 27, 2141–2148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Platat, C.; Wagner, A.; Klumpp, T.; Schweitzer, B.; Simon, C. Relationships of physical activity with metabolic syndrome features and low-grade inflammation in adolescents. Diabetologia 2006, 49, 2078–2085. [Google Scholar] [CrossRef] [Green Version]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is Muscular Fitness Associated with Future Health Benefts in Children and Adolescents? A Systematic Review and Meta Analysis of Longitudinal Studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. 2007, 32, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Padilla-Moledo, C.; Fernández-Santos, J.D.; Izquierdo-Gómez, R.; Esteban-Cornejo, I.; Rio-Cozar, P.; Carbonell-Baeza, A.; Castro-Piñero, J. Physical Fitness and Self-Rated Health in Children and Adolescents: Cross-Sectional and Longitudinal Study. Int. J. Environ. Res. Public Health 2020, 17, 2413. [Google Scholar] [CrossRef]
- Fryar, C.D.; Carroll, M.D.; Ogden, C.L. Prevalence of Obesity among Children and Adolescents: United States, Trends 1963–1965 through 2009–2010; National Center for Health Statistics: Hyattsville, MD, USA, 2012. [Google Scholar]
- Tomkinson, G.R.; Lang, J.J.; Tremblay, M.S.; Dale, M.; LeBlanc, A.G.; Belanger, K.; Ortega, F.B.; Léger, L. International normative 20 m shuttle run values from 1,142,026 children and youth representing 50 countries. Br. J. Sports Med. 2017, 51, 1545–1554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sallay, V.; Martos, T.; Földvári, M.; Szabó, T.; Ittzés, A. Hungarian version of the Rosenberg Self-esteem Scale (RSES-H): An alternative translation, structural invariance, and validity. J. Ment. Health Psychosom. 2014, 15, 259–275. [Google Scholar] [CrossRef] [Green Version]
- Probst, M.; Vandereycken, W.; van Coppenolle, H.; Vanderlinden, J. The Body Attitude Test for Patients with an Eating Disorder: Psychometric Characteristics of a New Questionnaire. Eat. Disord. 1995, 3, 133–144. [Google Scholar] [CrossRef]
- Dupont, W.D.; Plummer, W.D. Power and sample size calculations: A review and computer program. Control. Clin. Trials 1990, 11, 116–128. [Google Scholar] [CrossRef]
- Dupont, W.D.; Plummer, W.D. Power and Sample Size Calculations for Studies Involving Linear Regression. Control. Clin. Trials 1998, 19, 589–601. [Google Scholar] [CrossRef]
- GBD 2015 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 79 behavioural, envi-ronmental and occupational, and metabolic risks or clusters of risks, 1990–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1659–1724. [Google Scholar] [CrossRef] [Green Version]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Gakidou, E.; Mullany, E.C.; Stan, B.; Abbafati, C.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 1289 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Tomkinson, G.R.; Carver, K.D.; Atkinson, F.; Daniell, N.D.; Lewis, L.K.; Fitzgerald, J.S.; Lang, J.J.; Ortega, F.B. European normative values for physical fitness in children and adolescents aged 9–17 years: Results from 2,779,165 Eurofit performances representing 30 countries. Br. J. Sports Med. 2018, 52, 1445–1456. [Google Scholar] [CrossRef] [Green Version]
- Petrovics, P.; Sandor, B.; Palfi, A.; Szekeres, Z.; Atlasz, T.; Toth, K.; Szabados, E. Association between Obesity and Overweight and Cardiorespiratory and Muscle Performance in Adolescents. Int. J. Environ. Res. Public Health 2020, 18, 134. [Google Scholar] [CrossRef]
- Deforche, B.; Lefevre, J.; de Bourdeaudhuij, I.; Hills, A.P.; Duquet, W.; Bouckaert, J. Physical Fitness and Physical Activity in Obese and Nonobese Flemish Youth. Obes. Res. 2003, 11, 434–441. [Google Scholar] [CrossRef]
- Morales, P.F.; Sánchez-López, M.; Moya-Martínez, P.; García-Prieto, J.C.; Martínez-Andrés, M.; García, N.L.; Martínez-Vizcaíno, V. Health-related quality of life, obesity, and fitness in schoolchildren: The Cuenca study. Qual. Life Res. 2013, 22, 1515–1523. [Google Scholar] [CrossRef]
- Olive, L.; Byrne, D.; Cunningham, R.; Telford, R. Effects of physical activity, fitness and fatness on children’s body image: The Australian LOOK longitudinal study. Ment. Health Phys. Act. 2012, 5, 116–124. [Google Scholar] [CrossRef]
- Rankin, J.; Matthews, L.; Cobley, S.; Han, A.; Sanders, R.; Wiltshire, H.D.; Baker, J.S. Psychological consequences of childhood obesity: Psychiatric comorbidity and prevention. Adolesc. Health Med. Ther. 2016, 7, 125–146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swallen, K.C.; Reither, E.N.; Haas, S.A.; Meier, A.M. Overweight, Obesity, and Health-Related Quality of Life Among Adolescents: The National Longitudinal Study of Adolescent Health. Pediatrics 2005, 115, 340–347. [Google Scholar] [CrossRef] [Green Version]
- Viner, R.M.; Haines, M.M.; Taylor, S.; Head, J.; Booy, R.; Stansfeld, S. Body mass, weight control behaviours, weight perception and emotional well being in a multiethnic sample of early adolescents. Int. J. Obes. 2006, 30, 1514–1521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Franklin, J.; Denyer, G.; Steinbeck, K.S.; Caterson, I.D.; Hill, A.J. Obesity and Risk of Low Self-esteem: A Statewide Survey of Australian Children. Pediatrics 2006, 118, 2481–2487. [Google Scholar] [CrossRef] [PubMed]
- French, S.A.; Story, M.; Perry, C.L. Self-Esteem and Obesity in Children and Adolescents: A Literature Review. Obes. Res. 1995, 3, 479–490. [Google Scholar] [CrossRef]
- Friedman, K.E.; Reichmann, S.K.; Costanzo, P.R.; Musante, G.J. Body Image Partially Mediates the Relationship between Obesity and Psychological Distress. Obes. Res. 2002, 10, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Probst, M.; Pieters, G.; Vanderlinden, J. Body experience assessment in non-clinical male and female subjects. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2009, 14, e16–e21. [Google Scholar] [CrossRef]
- Ghaznavi, J.; Taylor, L.D. Bones, body parts, and sex appeal: An analysis of #thinspiration images on popular social media. Body Image 2015, 14, 54–61. [Google Scholar] [CrossRef]
- Tiggemann, M.; Zaccardo, M. ‘Strong is the new skinny’: A content analysis of #fitspiration images on Instagram. J. Health Psychol. 2016, 23, 1003–1011. [Google Scholar] [CrossRef]
- McBride, C.; Costello, N.; Ambwani, S.; Wilhite, B.; Austin, S.B. Digital Manipulation of Images of Models’ Appearance in Advertising: Strategies for Action Through Law and Corporate Social Responsibility Incentives to Protect Public Health. Am. J. Law Med. 2019, 45, 7–31. [Google Scholar] [CrossRef] [PubMed]
- Lin, L.; Soby, M. Is listening to fat talk the same as participating in fat talk? Eat. Disord. 2016, 25, 165–172. [Google Scholar] [CrossRef]
- Berge, J.M.; Winkler, M.R.; Larson, N.; Miller, J.; Haynos, A.F.; Neumark-Sztainer, D. Intergenerational Transmission of Parent Encouragement to Diet From Adolescence Into Adulthood. Pediatrics 2018, 141, e20172955. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hartman-Munick, S.M.; Gordon, A.R.; Guss, C. Adolescent body image: Influencing factors and the clinician’s role. Curr. Opin. Pediatr. 2020, 32, 455–460. [Google Scholar] [CrossRef]
- Loth, K.A.; Watts, A.W.; Berg, P.V.D.; Neumark-Sztainer, D. Does Body Satisfaction Help or Harm Overweight Teens? A 10-Year Longitudinal Study of the Relationship Between Body Satisfaction and Body Mass Index. J. Adolesc. Health 2015, 57, 559–561. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrew, R.; Tiggemann, M.; Clark, L. Predictors and health-related outcomes of positive body image in adolescent girls: A prospective study. Dev. Psychol. 2016, 52, 463–474. [Google Scholar] [CrossRef]
- Gillen, M.M. Associations between positive body image and indicators of men’s and women’s mental and physical health. Body Image 2015, 13, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Devonport, T.J.; Nicholls, W.; Fullerton, C. A systematic review of the association between emotions and eating behaviour in normal and overweight adult populations. J. Health Psychol. 2017, 24, 3–24. [Google Scholar] [CrossRef]
- Macht, M. How emotions affect eating: A five-way model. Appetite 2008, 50, 1–11. [Google Scholar] [CrossRef]
- Van Strien, T.; Konttinen, H.; Homberg, J.R.; Engels, R.C.; Winkens, L.H. Emotional eating as a mediator between depression and weight gain. Appetite 2016, 100, 216–224. [Google Scholar] [CrossRef] [PubMed]
- Nguyen-Michel, S.T.; Unger, J.; Spruijt-Metz, D. Dietary correlates of emotional eating in adolescence. Appetite 2007, 49, 494–499. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wardle, J.; Marsland, L.; Sheikh, Y.; Quinn, M.; Fedoroff, I.; Ogden, J. Eating style and eating behaviour in adolescents. Appetite 1992, 18, 167–183. [Google Scholar] [CrossRef]
- Rolls, B.J.; Fedoroff, I.C.; Guthrie, J.F. Gender differences in eating behavior and body weight regulation. Health Psychol. 1991, 10, 133–142. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, L.M.; Anderson, L.M.; Simone, M.; O’Connor, S.M.; Zickgraf, H.; Anderson, E.A.; Rodgers, R.F.; Thompson, J.K. Gender-based differential item functioning in measures of eating pathology. Int. J. Eat. Disord. 2019, 52, 1047–1051. [Google Scholar] [CrossRef] [PubMed]
- Murray, S.B.; Griffiths, S.; Mond, J. Evolving eating disorder psychopathology: Conceptualising muscularity-oriented disordered eating. Br. J. Psychiatry 2016, 208, 414–415. [Google Scholar] [CrossRef] [Green Version]
- Trzesniewski, K.H.; Donnellan, M.B.; Moffitt, T.E.; Robins, R.W.; Poulton, R.; Caspi, A. Low self-esteem during adolescence predicts poor health, criminal behavior, and limited economic prospects during adulthood. Dev. Psychol. 2006, 42, 381–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Psychological Variable | Mean | SD | Minimum | Maximum | Skewness/Kurtosis |
|---|---|---|---|---|---|
| Self-esteem (RSES) | 28.91 | 6.32 | 12 | 40 | −0.251/−0.471 |
| Body attitudes (BAT) | 24.02 | 7.70 | 13.13 | 55 | 0.865/0.960 |
| Uncontrolled eating (EAT-UE) | 19.29 | 5.18 | 9 | 33 | 0.339/−0.391 |
| Cognitive restraints (EAT-CR) | 14.92 | 3.74 | 6 | 26 | 0.080/−0.352 |
| Emotional eating (EAT-EE) | 10.24 | 4.98 | 6 | 24 | 0.598/0.725 |
| Dependent Variables | Predictors | ||||
|---|---|---|---|---|---|
| Age | Gender | SBSH | BMI for Age | R2 | |
| Self-esteem (RSES) | 0.09 | −0.31 ** | 0.16 ** | 0.07 | 0.16 ** |
| Body attitudes (BAT) | 0.00 | 0.39 ** | −0.32 ** | 0.01 | 0.28 ** |
| Uncontrolled eating (UE) | −0.06 | 0.18 | 0.06 | −0.02 | 0.04 * |
| Cognitive restraints (CR) | 0.02 | 0.26 ** | −0.22 ** | −0.09 | 0.12 ** |
| Emotional eating (EE) | −0.01 | 0.23 ** | −0.07 | −0.12* | 0.07 ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Petrovics, P.; Nagy, A.; Sandor, B.; Palfi, A.; Szekeres, Z.; Toth, K.; Szabados, E. Examination of Self-Esteem, Body Image, Eating Attitudes and Cardiorespiratory Performance in Adolescents. Int. J. Environ. Res. Public Health 2021, 18, 13172. https://doi.org/10.3390/ijerph182413172
Petrovics P, Nagy A, Sandor B, Palfi A, Szekeres Z, Toth K, Szabados E. Examination of Self-Esteem, Body Image, Eating Attitudes and Cardiorespiratory Performance in Adolescents. International Journal of Environmental Research and Public Health. 2021; 18(24):13172. https://doi.org/10.3390/ijerph182413172
Chicago/Turabian StylePetrovics, Peter, Alexandra Nagy, Barbara Sandor, Anita Palfi, Zsolt Szekeres, Kalman Toth, and Eszter Szabados. 2021. "Examination of Self-Esteem, Body Image, Eating Attitudes and Cardiorespiratory Performance in Adolescents" International Journal of Environmental Research and Public Health 18, no. 24: 13172. https://doi.org/10.3390/ijerph182413172