
HIIT vs. SIT: What Is the Better to Improve

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.2.1. Type of Studies
2.2.2. Participants
2.2.3. Protocols
2.3. Data-Extraction Strategy
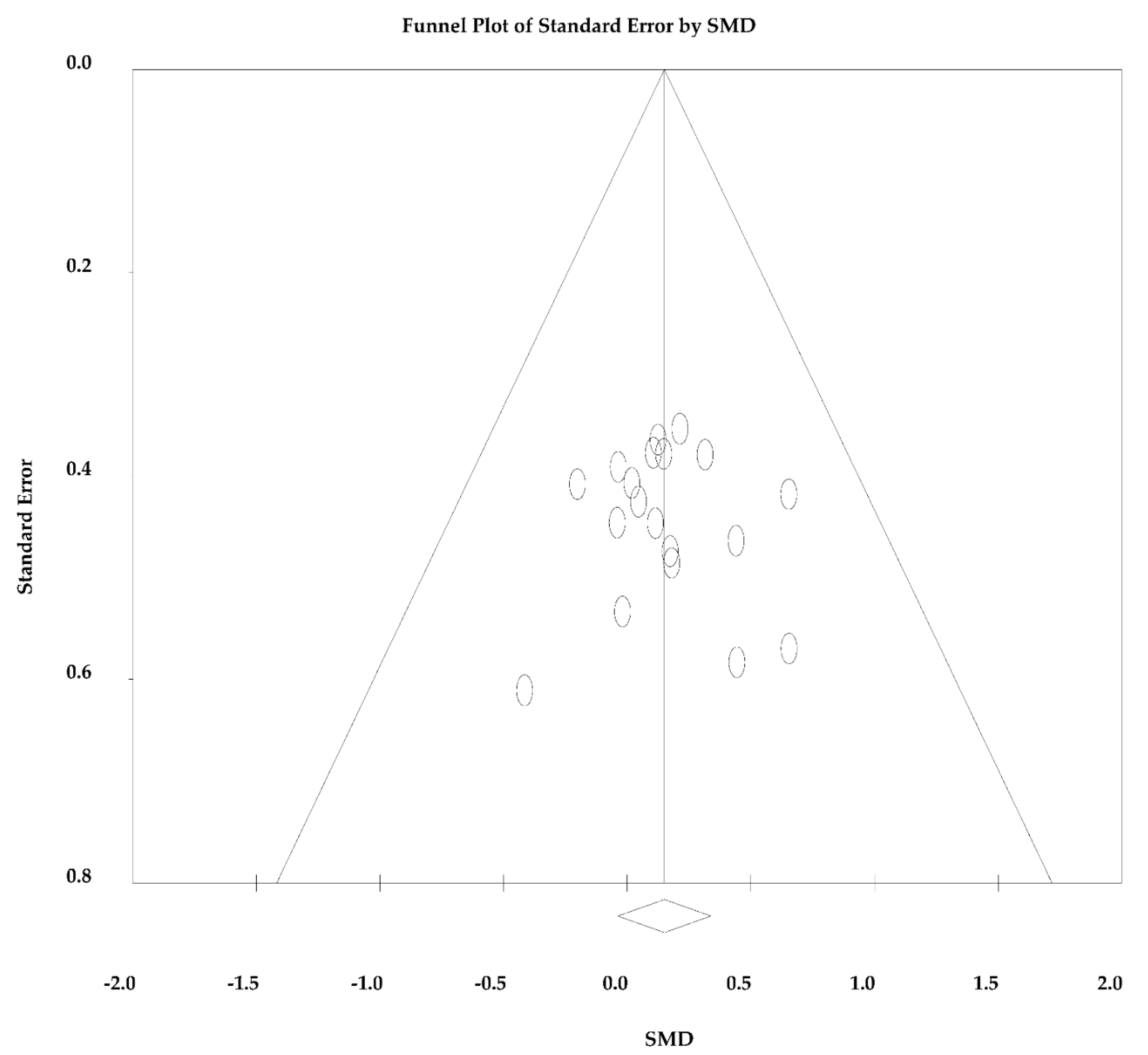
2.4. Quality Assessment and Publication Bias
2.5. Choice of Model and Analysis of Heterogeneity
2.6. Data Analysis
3. Results
SIT vs. HIIT
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Rosenblat, M.A.; Perrotta, A.S.; Thomas Scott, G. Effect of High-Intensity Interval Training Versus Sprint Interval Training on Time-Trial Performance: A Systematic Review and Meta-analysis. Sports Med. 2020, 50, 1145–1161. [Google Scholar] [CrossRef]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: A meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef] [Green Version]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. Quantity and Quality of Exercise for Developing and Maintaining Cardiorespiratory, Musculoskeletal, and Neuromotor Fitness in Apparently Healthy Adults: Guidance for Prescribing Exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- Helgerud, J.; Høydal, K.; Wang, E.; Karlsen, T.; Berg, P.; Bjerkaas, M.; Simonsen, T.; Helgesen, C.; Hjorth, N.; Bach, R.; et al. Aerobic High-Intensity Intervals Improve VO2max More Than Moderate Training. Med. Sci. Sports Exerc. 2007, 39, 665–671. [Google Scholar] [CrossRef] [Green Version]
- Milanović, Z.; Sporis, G.; Weston, M. Effectiveness of High-Intensity Interval Training (HIT) and Continuous Endurance Training for VO2max Improvements: A Systematic Review and Meta-Analysis of Controlled Trials. Sports Med. 2015, 45, 1469–1481. [Google Scholar] [CrossRef] [PubMed]
- Ramos, J.; Dalleck, L.C.; Tjonna, A.E.; Beetham, K.; Coombes, J.S. The Impact of High-Intensity Interval Training Versus Moderate-Intensity Continuous Training on Vascular Function: A Systematic Review and Meta-Analysis. Sports Med. 2015, 45, 679–692. [Google Scholar] [CrossRef]
- Billat, V. Interval Training for Performance: A Scientific and Empirical Practice. Special recommendations for middle- and long-distance running. Part I: Aerobic interval training. Sports Med. 2001, 31, 13–31. [Google Scholar] [CrossRef]
- Fox, E.; Bartels RBillings, C.; Mathews, D.; Bason, R.; Webb, W. Intensity and distance of interval training programs and changes in aerobic power. Med. Sci. Sports 1973, 5, 18–22. [Google Scholar] [PubMed]
- MacInnis, M.J.; Gibala, M.J. Physiological adaptations to interval training and the role of exercise intensity. J. Physiol. 2017, 595, 2915–2930. [Google Scholar] [CrossRef] [Green Version]
- Buchheit, M.; Laursen, P.B. High-intensity interval training, solutions to the programming puzzle. Sports Med. 2013, 43, 313–338. [Google Scholar] [CrossRef] [PubMed]
- Laursen, P.B.; Shing, C.M.; Peake, J.M.; Coombes, J.; Jenkins, D. Interval training program optimization in highly trained endurance cyclists. Med. Sci. Sports Exerc. 2002, 34, 1801–1807. [Google Scholar] [CrossRef] [Green Version]
- Gibala, M.J.; McGee, S.L. Metabolic adaptations to short-term high-intensity interval training: A little pain for a lot of gain? Exerc. Sport Sci. Rev. 2008, 36, 58–63. [Google Scholar] [CrossRef]
- Gibala, M.J.; Little, J.P.; MacDonald, M.J.; Hawley, J.A. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol. 2011, 590, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Baar, K. The signaling underlying. Appl. Physiol. Nutr. Metab. 2009, 3, 411–419. [Google Scholar] [CrossRef] [PubMed]
- Tjønna, A.E.; Rognmo, Ø.; Stølen, T.; Bye, A.; Haram, P.M.; Loennechen, J.P.; Slørdahl, S.A.; Wisløff, U.; Lee, S.J.; Al-Share, Q.Y.; et al. Response to Letter Regarding Article, “Aerobic Interval Training Versus Continuous Moderate Exercise as a Treatment for the Metabolic Syndrome: A Pilot Study”. Circulation 2009, 119, 226. [Google Scholar] [CrossRef]
- Midgley, A.W.; McNaugton, L.R.; Wilkinson, M. Is there an optimal training intensity for enhancing the maximal oxygen uptake of distance runners? Sports Med. 2006, 36, 117–132. [Google Scholar] [CrossRef]
- Krustrup, P.; Mohr, M.; Bangsbo, J. The slow component of oxygen uptake during intense, sub-maximal exercise in man is associated with additional fibre recruitment. Pflüger’s Archiv. Gesamte Physiol. Menschen Tiere 2004, 447, 855–866. [Google Scholar] [CrossRef] [PubMed]
- Smart, N.A.; Waldron, M.; Ismail, H.; Giallauria, F.; Vigorito, C.; Cornelissen, V.; Dieberg, G. Validation of a new tool for the assessment of study quality and reporting in exercise training studies: TESTEX. JBI Evid. Implement. 2015, 13, 9–18. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Deeks, J.J.; Macaskill, P.; Irwig, L. The performance of tests of publication bias and other sample size effects in systematic reviews of diagnostic test accuracy was assessed. J. Clin. Epidemiol. 2005, 58, 882–893. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Paquette, M.; Bieuzen, F.; Billaut, F. The effect of HIIT vs. SIT on muscle oxygenation in trained sprint kayakers. Graefe’s Arch. Clin. Exp. Ophthalmol. 2021, 121, 2743–2759. [Google Scholar] [CrossRef]
- Vaccari, F.; Giovanelli, N.; Lazzer, S. High-intensity decreasing interval training (HIDIT) increases time above 90% VO2peak. Graefe’s Arch. Clin. Exp. Ophthalmol. 2020, 120, 2397–2405. [Google Scholar] [CrossRef]
- Rønnestad, B.R.; Hansen, J.; Vegge, G.; Tønnessen, E.; Slettaløkken, G. Short intervals induce superior training adaptations compared with long intervals in cyclists—An effort-matched approach. Scand. J. Med. Sci. Sports 2015, 25, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Munoz, I.; Seiler, S.; Alcocer, A.; Carr, N.; Esteve-Lanao, J. Specific Intensity for Peaking: Is Race Pace the Best Option? Asian J. Sports Med. 2015, 6, e24900. [Google Scholar] [CrossRef] [Green Version]
- Huedo-Medina, T.B.; Sanchez-Meca, J.; Marín-Martinez, F.; Botella, J. Assessing heterogeneity in meta-analysis: Q statistic or I2 index? Psychol. Methods 2006, 11, 193. [Google Scholar] [CrossRef] [Green Version]
- Parolin, M.L.; Chesley, A.; Matsos, M.P.; Spriet, L.L.; Jones, N.L.; Heigenhauser, G.J.F. Regulation of skeletal muscle glycogen phosphorylase and PDH during maximal intermittent exercise. Am. J. Physiol. Metab. 1999, 277, E890–E900. [Google Scholar] [CrossRef] [PubMed]
- Niklas, P.; Li, W.; Jens, W.; Michail, T.; Kent, S. Mitochondrial gene expression in elite cyclists: Effects of high-intensity interval exercise. Graefe’s Arch. Clin. Exp. Ophthalmol. 2010, 110, 597–606. [Google Scholar] [CrossRef]
- Sun, S.; Zhang, H.; Kong, Z.; Shi, Q.; Tong, T.K.; Nie, J. Twelve weeks of low volume sprint interval training improves cardio-metabolic health outcomes in overweight females. J. Sports Sci. 2018, 37, 1257–1264. [Google Scholar] [CrossRef]
- Batacan, R.B., Jr.; Duncan, M.J.; Dalbo, V.J.; Tucker, P.S.; Fenning, A.S. Effects of high-intensity interval training on cardiometabolic health: A systematic review and meta-analysis of intervention studies. Br. J. Sports Med. 2017, 51, 494–503. [Google Scholar] [CrossRef] [PubMed]
- Poon, E.T.-C.; Little, J.P.; Sit, C.H.-P.; Wong, S.H.-S. The effect of low-volume high-intensity interval training on cardiometabolic health and psychological responses in overweight/obese middle-aged men. J. Sports Sci. 2020, 38, 1997–2004. [Google Scholar] [CrossRef] [PubMed]
- Esfarjani, F.; Laursen, P.B. Manipulating high-intensity interval training: Effects on VO2max, the lactate threshold and 3000 m running performance in moderately trained males. J. Sci. Med. Sport 2007, 10, 27–35. [Google Scholar] [CrossRef]
- Astorino, T.A.; Edmunds, R.M.; Clark, A.; King, L.; Gallant, R.A.; Namm, S.; Fischer, A.; Wood, K.M. High-intensity interval training increases cardiac output and VO2max. Med. Sci. Sports Exerc. 2017, 49, 265–273. [Google Scholar] [CrossRef]
- Matsuo, T.; Saotome, K.; Seino, S.; Shimojo, N.; Matsushita, A.; Iemitsu, M.; Ohshima, H.; Tanaka, K.; Mukai, C. Effects of a low-volume aerobic-type interval exercise on VO2max and cardiac mass. Med. Sci. Sports Exerc. 2014, 46, 42–50. [Google Scholar] [CrossRef]
- Aktaş, H.Ş.; Uzun, Y.E.; Kutlu, O.; Pençe, H.H.; Özçelik, F.; Çil, E.Ö.; Irak, L.; Altun, Ö.; Özcan, M.; Özsoy, N.; et al. The effects of high intensity-interval training on vaspin, adiponectin and leptin levels in women with polycystic ovary syndrome. Arch. Physiol. Biochem. 2019, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Coll-Risco, I.; Aparicio, V.A.; Nebot, E.; Camiletti-Moirón, D.; Martínez, R.; Kapravelou, G.; López-Jurado, M.; Porres, J.M.; Aranda, P. Effects of interval aerobic training combined with strength exercise on body composition, glycaemic and lipid profile and aerobic capacity of obese rats. J. Sports Sci. 2015, 34, 1452–1460. [Google Scholar] [CrossRef]
- Vincent, S.; Berthon, P.; Zouhal, H.; Moussa, E.; Catheline, M.; Bentu-Ferrer, D.; Gratas-Delamarche, A.; Vincent, S.; Berthon, P. Plasma Glucose, Insulin and Catecholamine Responses to a Wingate Test in Physically Active Women and Men. Eur. J. Sport Sci. 2004, 91, 15–21. [Google Scholar] [CrossRef]
- Khalafi, M.; Symonds, M.E. The impact of high-intensity interval training on inflammatory markers in metabolic disorders: A meta-analysis. Scand. J. Med. Sci. Sports 2020, 30, 2020–2036. [Google Scholar] [CrossRef] [PubMed]
- Su, L.; Fu, J.; Sun, S.; Zhao, G.; Cheng, W.; Dou, C.; Quan, M. Effects of HIIT and MICT on cardiovascular risk factors in adults with overweight and/or obesity: A meta-analysis. PLoS ONE 2019, 14, e0210644. [Google Scholar] [CrossRef]
- Maillard, F.; Pereira, B.; Boisseau, N. Effect of high-intensity interval training on total, abdominal and visceral fat mass: A meta-analysis. Sports Med. 2018, 48, 269–288. [Google Scholar] [CrossRef] [PubMed]
- Keating, S.E.; Johnson, N.; Mielke, G.; Coombes, J.S. A systematic review and meta-analysis of interval training versus moderate-intensity continuous training on body adiposity. Obes. Rev. 2017, 18, 943–964. [Google Scholar] [CrossRef] [PubMed]
- Martin-Smith, R.; Cox, A.; Buchan, D.S.; Baker, J.S.; Grace, F.; Sculthorpe, N. High Intensity Interval Training (HIIT) Improves Cardiorespiratory Fitness (CRF) in Healthy, Overweight and Obese Adolescents: A Systematic Review and Meta-Analysis of Controlled Studies. Int. J. Environ. Res. Public Health 2020, 17, 2955. [Google Scholar] [CrossRef]
- Guiraud, T.; Labrunee, M.; Gaucher-Cazalis, K.; Despas, F.; Meyer, P.; Bosquet, L.; Gales, C.; Vaccaro, A.; Bousquet, M.; Galinier, M.; et al. High-Intensity Interval Exercise Improves Vagal Tone and Decreases Arrhythmias in Chronic Heart Failure. Med. Sci. Sports Exerc. 2013, 45, 1861–1867. [Google Scholar] [CrossRef] [PubMed]
- Grace, F.; Herbert, P.; Elliott, A.D.; Richards, J.; Beaumont, A.; Sculthorpe, N. High intensity interval training (HIIT) improves resting blood pressure, metabolic (MET) capacity and heart rate reserve without compromising cardiac function in sedentary aging men. Exp. Gerontol. 2018, 109, 75–81. [Google Scholar] [CrossRef]
- Leal, J.M.; Galliano, L.M.; Del Vecchio, F.B. Effectiveness of High-Intensity Interval Training Versus Moderate-Intensity Continuous Training in Hypertensive Patients: A Systematic Review and Meta-Analysis. Curr. Hypertens. Rep. 2020, 22, 1–13. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Eligibility Criteria Specified | Randomization Specified | Allocation Concealment | Groups Similar at Baseline | Blinding of Assessor | Assessed in 85% of Patients | Intention-to-Treat Analysis | Between-Group Statistical Comparisons Reported | Variability Reported Outcome Measures | Activity Monitoring in Control Group | Relative Exercise Intensity Remained Constant | Exercise Volume and Energy Expenditure | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Astorino et al., 2017 | 1 | 0 | 0 | 1 | 0 | 2 | 0 | 2 | 1 | 1 | 1 | 0 | 9 |
| Smith-Ryan et al., 2016 | 1 | 1 | 0 | 1 | 0 | 3 | 0 | 2 | 1 | 1 | 1 | 0 | 11 |
| Helgerud et al., 2007 | 1 | 1 | 0 | 1 | 0 | 2 | 0 | 2 | 1 | 0 | 1 | 0 | 9 |
| Bækkerud et al., 2016 | 1 | 1 | 0 | 1 | 0 | 2 | 0 | 2 | 1 | 0 | 1 | 0 | 9 |
| Matsuo et al., 2014 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 2 | 1 | 1 | 1 | 1 | 11 |
| Reljic et al., 2018 | 1 | 1 | 0 | 1 | 0 | 2 | 0 | 2 | 1 | 0 | 1 | 0 | 9 |
| Franch et al., 1998 | 1 | 0 | 0 | 1 | 0 | 1 | 0 | 2 | 1 | 1 | 1 | 0 | 8 |
| Hu et al., 2012 | 1 | 1 | 0 | 0 | 0 | 3 | 0 | 2 | 1 | 0 | 1 | 0 | 9 |
| Esfarjani et al., 2007 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 2 | 1 | 1 | 1 | 0 | 7 |
| Camacho-Cardenosa et al., 2020 | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 1 | 7 |
| Sun et al., 2019 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 2 | 1 | 0 | 1 | 0 | 8 |
| Ferley, Hopper and Vukovich, 2016 | 1 | 1 | 0 | 1 | 0 | 2 | 0 | 2 | 1 | 0 | 1 | 0 | 9 |
| Naroa et al., 2013 | 1 | 1 | 0 | 1 | 0 | 3 | 0 | 2 | 1 | 0 | 1 | 0 | 10 |
| Overend et al., 1992 | 1 | 1 | 0 | 1 | 0 | 2 | 0 | 2 | 1 | 0 | 1 | 0 | 9 |
| Firat and Dicle, 2015 | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 2 | 1 | 0 | 1 | 0 | 7 |
| Shengyan et al., 2018 | 1 | 1 | 0 | 1 | 0 | 1 | 0 | 2 | 1 | 0 | 1 | 0 | 8 |
| Lunt et al., 2014 | 1 | 1 | 0 | 1 | 0 | 3 | 0 | 2 | 1 | 0 | 1 | 0 | 10 |
| Muñoz et al., 2015 | 1 | 0 | 0 | 1 | 0 | 3 | 0 | 2 | 1 | 0 | 1 | 0 | 9 |
| Paul et al., 2002 | 1 | 0 | 0 | 1 | 0 | 3 | 0 | 2 | 1 | 1 | 1 | 0 | 10 |
| Study | Protocol | Population | Age (years) | BW (kg) | Height (m) | Baseline | Duration (Weeks) | No. of Sessions | Exercise Intensity | No of Reps (Start/End) | Reps Duration | Work/Rest Ratio | Δ O2max% | Outcomes |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Smith-Ryan et al., 2016 | HIIT | 32-♀ sedentary | 33 ± 12 | 88.1 ± 15.9 | 1.66 ± 0.53 | 24 ± 7 | 3 | 9 | O2max | 5 | 120 s | 2 | 8.83 | O2 Peak was encountered in both groups. |
| SIT | 90% Power output | 10 | 60 s | 1 | 6.45 | |||||||||
| Helgerud et al., 2007 | HIIT | 40-♀ engaged in endurance training 3x/week | 25 ± 4 | 82 ± 12 | 1.82 ± 0.6 | 55.5 ± 7.4 | 8 | 24 | 90–95% HRmax | 4 | 4 min | 1.3 | 8.96 | Both groups ↑ absolute |
| SIT | 60.5 ± 5.4 | 90–95%Hrmax | 15 | 15 s | 1 | 7.98 | ||||||||
| Ferley; Hopper; Vukovich, 2016 | HIIT | 24: 16-♀ and 8-♂; running experience | 28 ± 7 | 68.4 ± 8.8 | 1.72 ± 0.54 | 50.2 ± 7.2 | 6 | 18 | 68% Vmax | 4–6 | 60% Tmax | NR | 4.58 | O2max. There was a small effect size for SIT > HIIT. |
| SIT | 26 ± 5 | 73.2 ± 12.5 | 1.74 ± 0.84 | 50.2 ± 6.9 | Vmax | 10–14 | 30 s | NR | 4.98 | |||||
| Astorino et al., 2017 | HIIT | 71: 34-♂ and 37-♀ active healthy | 22 ± 5.4 | 69.6 ± 11.4 | 1.74 ± 10 | 39.6 ± 5.6 | 3–4 | 10 | 70–110% PPO | 5–10 | 150 s | 1.3 | 9 | O2max. |
| SIT | 68.5 ± 10.3 | 1.72 ± 8 | All out | 8–12 | 60 s | 0.2 | 7.7 | |||||||
| Esfarjani, Laursen, 2007 | HIIT | 17-♂ moderately trained runners | 23 ± 5 | 69.6 ± 11.4 | NR | 39.6 ± 5.6 | 10 | 20 | 60% Tmax | 8 | 60% Tmax | 1 | 9.16 | O2max. |
| SIT | 68.5 ± 10.3 | 30 s | 12 | 30 s | 0.11 | 6.19 | ||||||||
| Matsuo et al., 2014 | HIIT | 42-♂ sedentary | 26.5 ± 6.2 | 63 ± 7 | 1.72 ± 5 | 41.9 ± 5.6 | 8 | 40 | 3 min | 3 | 3 min | 1.5 | 21.96 | O2max. There was a larger effect size to HIIT > SIT. |
| SIT | 62.4 ± 5.4 | 171 ± 5 | 43.9 ± 6.7 | 30 s | 7 | 30 s | 1.5 | 15.72 | ||||||
| Overend; Cunningham, 1992 | HIIT | 17-♂ active young | 25 ± 3 | 75 ± 9 | 1.77 ± 7 | 3.49 ± 0.26 | 10 | 40 | O2max | NR | 3 min | 1.5 | 9.46 | O2max. |
| SIT | 3.15 ± 0.22 | O2max | NR | 30 s | 1 | 16.51 | ||||||||
| Firat; Dicle, 2015 | HIT | 20-♂ national level lightweight collegiate rowers | 21 ± 2 | 67 ± 3 | 1.78 ± 6 | 56.6 ± 5.7 | 4 | 8 | 90%PPO | 8 | 2.5 min | 0.833 | 4.91 | O2max for all groups. |
| SIT | 150% PPO | 10 | 30 s | 0.11 | 5.53 | |||||||||
| Franch et al., 1998 | HIIT | 36-♀ running experience | 30.4 ± 4.8 | NR | NR | 54.8 ± 3.0 | 6 | NR | O2max | 3–6 | 4 min | 2 | 6 | O2max. |
| SIT | O2max | 30–40 | 15 s | 1 | 3.6 | |||||||||
| Sun et al., 2019 | HIIT | 42-♀ overweight but healthy | 22 ± 2 | 69 ± 6 | 1.63 ± 5 | 31.5 ± 2.2 | 12 | 36 | 90%PPO | 8–10 | 4 min | 1.33 | 26.67 | O2max for all groups. |
| SIT | 68 ± 7 | 68 ± 7 | 1.62 ± 3.9 | 31.1 ± 3.6 | 150% PPO | 80 | 6 s | 0.67 | 25.08 | |||||
| Camacho-Cardenosa et al., 2019 | HIIT | 36-♀ running experience | 30.4 ± 4.8 | NR | NR | 25.50 ± 4.93 | 12 | 57 | 90% Wmax | 3–6 | 3 min | 1 | −0.47 | O2max. |
| SIT | 25.33 ± 4.62 | all-out | 3–6 | 30 s | 0.16 | 2.88 | ||||||||
| Shengyan et al., 2019 | HIIT | 48-♀ overweight female | 21.5 ± 1.8 | 21.5 ± 1.8 | NR | 31.5 ± 2.2 | 12 | 36 | o2peak | 80 | 4 min | 0.66 | 8.4 | O2max. |
| SIT | 21.4 ± 1.1 | 31.1 ± 3.6 | 100 rpm with 1.5 kg | NR | 6 s | 1.33 | 7.8 | |||||||
| Reljic; Wittmann; Fischer, 2018 | HIIT | 34: 23-♀ and 11-♂ sedentary | 30 ± 7.1 | 71 ± 14.2 | 1.67 ± 0.11 | 29.3 ± 7.7 | 8 | 16 | 85–95% HRmax | 2 | 4 min | 2 | 16.5 | O2max. |
| SIT | 75.6 ± 15.4 | 1.73 ± 0.10 | 85–95% HRmax | 5 | 1 min | 1 | 24.14 | |||||||
| Hu et al., 2021 | HIIT | 66-♀ and ♂ sedentary | 21.2 ± 1.4 | 26 ± 3 | NR | 31.9 ± 6.9 | 12 | 36 | O2peak | NR | 4 min | 1.3 | 20.5 | O2max ↑ HIIT and SIT |
| SIT | 34.7 ± 8.7 | 1 kg 100 rpm | 10 | 6 s | 0.6 | 21.5 | ||||||||
| Etxebarria et al., 2014 | HIIT | 14-♂ moderately trained | 33 ± 8 | 78 ± 10 | 1.82 ± 8 | 58.7 ± 8.1 | 3 | 6 | O2peak | O2peak. | ||||
| SIT | Near maximal | |||||||||||||
| Baekkerud et al., 2016 | HIIT | 30: 18-♀ and 13-♂ sedentary | 41 ± 9 | 91 ± 14 | 1.73 ± 0,08 | 31.9 ± 6.9 | 6 | 18 | 85–95% HRmax | O2max was ↑ HIIT then in SIT. | ||||
| SIT | 34.7 ± 8.7 | 90% HRmax | ||||||||||||
| Lunt et al., 2014 | HIIT | 49: 36♀ and 13-♂ sedentary | 48 ± 6 | NR | NR | 24.2 ± 4.8 | 12 | 36 | 85–95% HRmax | 4 | 4 min | 1.3 | 5.79 | O2max for HIIT Walk group, but not for SIT vs. Walk. |
| SIT | 50 ± 8; | NR | NR | 25.0 ± 2.8 | All out | 3 | 30 s | 0.125 | 0.8 | |||||
| Paul et al., 2002 | HIIT | 41-♀ high trained athletes | 25 ± 6 | 75 ± 7 | 1.80 ± 5 | 64.5 ± 5.2 | 4 | 8 | Pmax | 8 | 144 s | 0.5 | 5.20 (G1); 7.98 (G2) | O2max. There was significantly HIIT2 > SIT. |
| SIT | 175% PPO | 12 | 30 s | 0.11 | 3.05 | |||||||||
| Overend; Cunningham, 1992 | HIIT | 17-♂ active young | 25 ± 3 | 75 ± 9 | 1.77 ± 7 | 3.49 ± 0.26 | 10 | 40 | O2max | NR | 3 min | 1.5 | 9.46 | O2max. |
| SIT | 3.15 ± 0.22 | O2max | NR | 30 s | 1 | 16.51 | ||||||||
| Firat; Dicle, 2015 | HIIT | 20-♂ national level lightweight collegiate rowers | 21 ± 2 | 67 ± 3 | 1.78 ± 6 | 56.6 ± 5.7 | 4 | 8 | 90% PPO | 8 | 2.5 min | 0.833 | 4.91 | O2max for all groups. |
| SIT | 150% PPO | 10 | 30 s | 0.11 | 5.53 | |||||||||
| Fahimeh, 2007 | HIIT | 17-♂ moderately trained runners | 23 ± 5 | 69.6 ± 11.4 | NR | 39.6 ± 5.6 | 10 | 20 | O2max | 8 | 60% Tmax | 1 | 9.16 | O2max |
| SIT | 68.5 ± 10.3 | O2max | 12 | 30 s | 0.11 | 6.19 |
| Sex | k | SMD | LL | UL | p-Value | p-Diff |
|---|---|---|---|---|---|---|
| Male | 7 | 0.099 | −0.25 | 0.449 | 0.578 | 0.175 |
| Female | 7 | 0.227 | −0.086 | 0.54 | 0.155 | |
| TESTEX score 10 | ||||||
| ≥10 | 4 | 0.172 | −0.229 | 0.573 | 0.401 | 0.401 |
| PAL | ||||||
| Active | 12 | −0.14 | −0.12 | 0.4 | 0.29 | 0.153 |
| Sedentary | 8 | 0.108 | −0.153 | 0.391 | 0.39 | |
| Duration (weeks) | ||||||
| ≥7 | 7 | 0.129 | −0.174 | 0.431 | 0.404 | 0.175 |
| <7 | 13 | 0.131 | −0.109 | 0.371 | 0.284 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Oliveira-Nunes, S.G.; Castro, A.; Sardeli, A.V.; Cavaglieri, C.R.; Chacon-Mikahil, M.P.T.
HIIT vs. SIT: What Is the Better to Improve
de Oliveira-Nunes SG, Castro A, Sardeli AV, Cavaglieri CR, Chacon-Mikahil MPT.
HIIT vs. SIT: What Is the Better to Improve
de Oliveira-Nunes, Silas Gabriel, Alex Castro, Amanda Veiga Sardeli, Claudia Regina Cavaglieri, and Mara Patricia Traina Chacon-Mikahil.
2021. "HIIT vs. SIT: What Is the Better to Improve