
Social Capital during the First Wave of the COVID-19 Outbreak: The Case of the Island of Menorca


Abstract
:1. Introduction
2. Materials and Methods
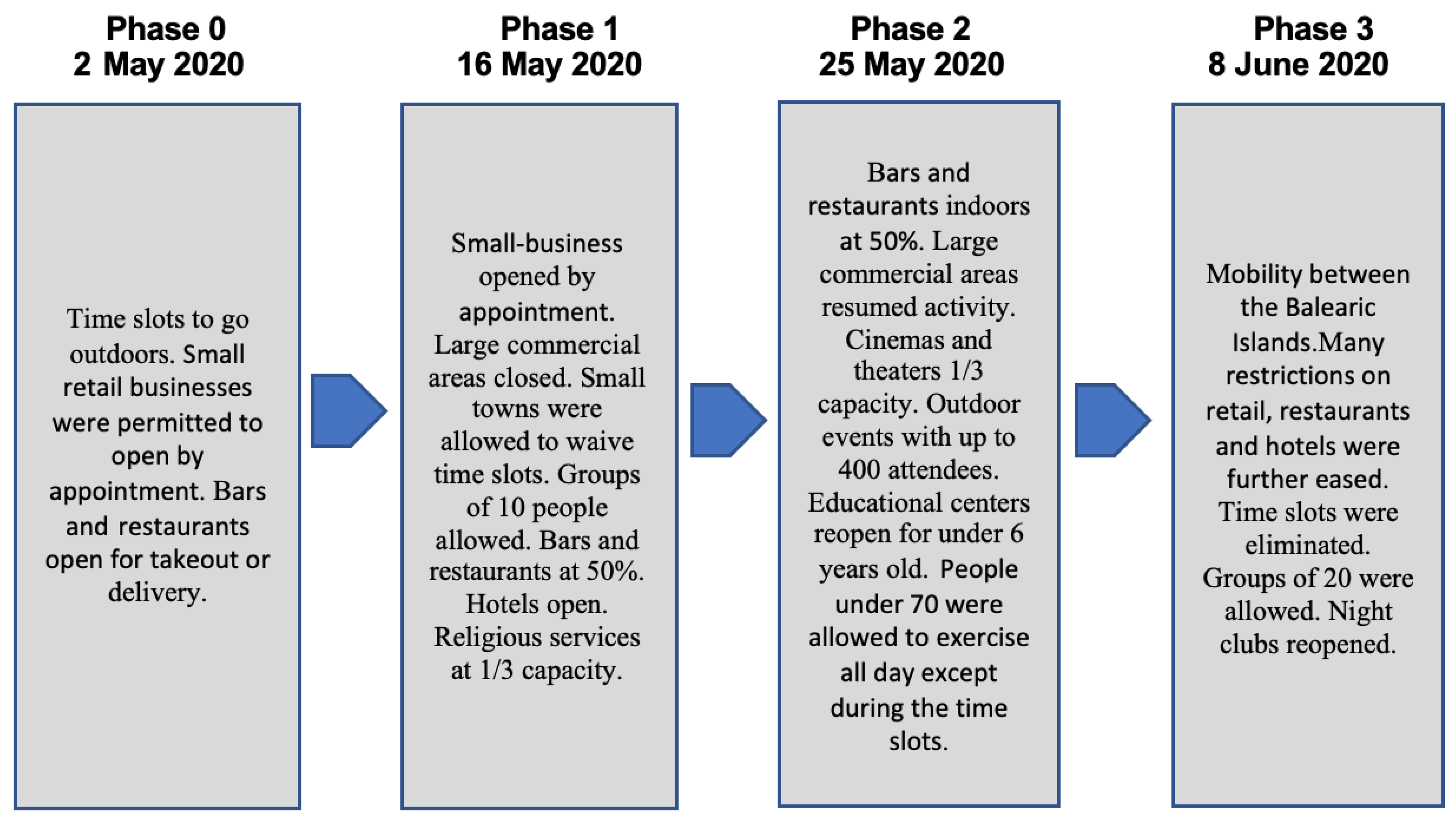
2.1. Sample, Timeline and Recruitment
2.2. Qualitative Study
2.3. Analysis
3. Results
3.1. Emergent Forms of Social Capital: Bounded Solidarity
“The nursing home has not changed anything. It all works the same with the same organization. I have changed some of my jobs—nursing home treasurer— and we cannot leave the nursing home. We used to go out a lot. My activities used to be bingo and dancing. We have a completely different life than the one we had before. I can only speak with my friends over the phone” (Male. 84. Nursing home resident. Interviewed during the lockdown).
“We used to have a lot of social life. I was into a lot of things. I used to go to university courses for seniors and with the “happy” grandmothers, to children’s story theater group, the book club and gym. Now nothing” (Female. 78. Retired. Interviewed during the lockdown).
“Suddenly we have met all our neighbors. Before this we didn’t know them. There are around nine houses on our street. We go out at 8 pm, and we have started to get to know each other. We’ve also had bingo at 7:30 pm with the children in the street. And other activities. Some people are very participative” (Female. 41. Pharmacist; interviewed during the lockdown).
“I have seen the town very empty. And a lot of people clapping after 8 pm. Today some people were pretending to get married wearing costumes, and they were joking from their balconies. At 1 pm. People were having a good time. And this kills time and makes people laugh. I saw a video of it because someone recorded it“ (Female. 61, market cashier; interviewed during Phase 0).
“We have a video call with the family after 8 o’clock. I see my other daughter on the balcony. My children who live in Menorca have been able to go to the hospital and see their father who is hospitalized infected with COVID-19. I have had very bad days. Now I’m calm. We have a neighbor who usually makes a video during summer to celebrate summer festivities. This year he created a video with the neighbors of our village singing, dancing and playing drums. He included pictures of my husband in the hospital saying we should resist and fight against the virus“ (Female. 65. Retired. Husband hospitalized with COVID-19; interviewed during the lockdown).
“Yes, a social network for doing things for others has been created. If someone needed something, they posted it. This was mostly to help people who couldn’t go out (go to the pharmacy, market…). My father-in-law is 81 years old and has no problem using technology. Now there are people that have learnt a lot of stuff“ (Male. 48. Pub owner; interviewed during Phase 1).
“There has been a lot of promotion of local stores, and farmers have been selling produce online. And people have responded to those initiatives. I do believe there have been changes. Some people have been making masks and giving them away“ (Female. 47. Nurse; interviewed during the lockdown).
“My father has COPD and has not been out. I have helped my parents avoid any trips. Total different story with my in-laws, they haven’t been so obedient and have gone out more. In fact, a lot of elderly people in Ciutadella have not respected the stay-at-home orders and have been amongst the people that have gone out more. Especially at the beginning of the lockdown“ (Female. 41. Pharmacist; interviewed during the lockdown).
3.2. Dark Sides of Social Capital: Ambivalence of Island Residents toward Outsiders
“With no health there is no economy. I understand. But with no economy there is no health, either. We would end up with no doctors, no nurses…“ (Male. 68. Business Owner. Interviewed during Phase 2).
“I am in favor of opening the island to tourism. But we need to test travelers and be able to control the situation. There should be a lot of investment in controls, but this is not happening. My father is at high risk since he is diabetic and has had heart attacks and pneumonia. I have brothers living in Madrid, and they will not come to Menorca for this reason“ (Female. 40. Online banking manager; interviewed during Phase 3).
3.3. Trust
“I don’t trust them. I’m not saying they did a bad job. But at the same time they didn’t do it right, because nobody was expecting this. On Monday they gave orders that were the last straw and they had to rectify. They said kids could go to the grocery store and other stuff. They screwed up. I’m not saying others would have done it better“ (Female. 41. Pharmacist; interviewed during the lockdown).
“I don’t trust them. It’s like having a lot of pigs together on a farm. First they fight, then they eat together and they end up rolling around in the same mud“ (Male. 89. Nursing home resident; interviewed during the lockdown).
“I trust scientific leaders that are not involved in politics. If your salary comes from the state, you cannot tell the truth. And they are also hiding the truth from you“ (Female. 53. Lab technician; interviewed during the lockdown).
“I trust them. These people are very busy. But if they are not able to influence politicians to address the problem based on truth, it’s going to be very complicated. They don’t have the power to decide“ (Male. 48. Policeman; interviewed during Phase 0).
“The privileged got here. They are smart and use their power to get a better life. In Menorca we have privileges compared to other islands. The people that came here came to soil the island, they should have stayed home. People come here and they think they own the place“ (Female. 74, retired; interviewed during the lockdown).
“At first we really resented it. I hear that kind of opinion at the local store. They criticized the fact that people had come. My son was going to come and he didn’t come. It was too late. He wanted to come because he was starting a new job here. I disapprove of what some groups of people did. They should have come taking precautions. But they also spend money and that’s good. There should have been controls much earlier“ (Female. 61, market cashier; interviewed during Phase 0).
3.4. Emergent Themes: Socioeconomic Inequalities
“At the beginning it was overwhelming. There were long lines to access the shop. We had to remind people to keep their distances before accessing the business. Logistics were complicated“ (Female. 58. Supermarket cashier; interviewed during the lockdown).
“I am lucky to work in tech. We develop software. I can work from home. The company is very flexible“ (Male. 37. Software developer; interviewed during Phase 2).
3.5. Mediterranean Familial Culture
“My daughter, who works at a bank, stops by and asks if we need anything. She goes shopping and to the pharmacy for us“ (Female. 78. Retired; interviewed during the lockdown).
“The person who helped me the most was my daughter, who is here next door. She goes shopping. I don’t have a driver’s license. She takes me to the hospital to see my husband. She is healthy and does absolutely everything“ (Female. 65. Retired. Husband hospitalized with COVID-19; interviewed during lockdown).
3.6. Inter-Generational Conflicts
“I guess there are all sorts of cases. A lot of students arrived. At first nobody liked it, but you understand the psychological part of wanting to be with the family. But it could have been done better. The people from Madrid were the first to arrive, because schools, universities, etc. shut down earlier than in other places and they just turned it into holidays. The problem is that they started leaving, leaving, leaving right from the start. You could see them everywhere. All the people that were able to leave and spread it all over Spain“ (Female. 41. Pharmacist; interviewed during the lockdown).
“Very irresponsible. I even think if your son or daughter is studying away from home and comes back, it’s very irresponsible. They have spread the virus to other places. A lot of people didn’t respect the 15-day quarantine“ (Female. 39. Policewoman, interviewed during Phase 0).
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Islam, N.; Khunti, K.; Dambha-Miller, H.; Kawachi, I.; Marmot, M. COVID-19 mortality: A complex interplay of sex, gender, and ethnicity. Eur. J. Public Health 2020, 30, 847–848. [Google Scholar] [CrossRef] [PubMed]
- Porta, M. A Dictionary of Epidemiology, 6th ed.; Oxford University Press: Oxford, NY, USA, 2014. [Google Scholar]
- Aldrich, D.P. Building Resilience: Social Capital in Post-Disaster Recovery, 1st ed.; University of Chicago Press: Chicago, IL, USA, 2012. [Google Scholar]
- Aldrich, D.P.; Kyota, E. Creating Community Resilience Through Elder-Led Physical and Social Infrastructure. Disaster Med. Public Health Prep. 2017, 11, 120–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chamlee-Wright, E.; Storr, V.H. Social Capital as Collective Narratives and Post-Disaster Community Recovery. Sociol. Rev. 2011, 59, 266–282. [Google Scholar] [CrossRef]
- Yila, O.; Weber, E.; Neef, A. The Role of Social Capital in Post-Flood Response and Recovery among Downstream Communities of the Ba River, Western Viti Levu, Fiji Islands. Risks Confl: Local Responses Nat. 2014, 14, 79–107. [Google Scholar] [CrossRef]
- Portes, A. Downsides of social capital. Proc. Natl. Acad. Sci. USA 2014, 111, 18407–18408. [Google Scholar] [CrossRef] [Green Version]
- Villalonga-Olives, E.; Kawachi, I. The dark side of social capital: A systematic review of the negative health effects of social capital. Soc. Sci. Med. 2017, 194, 105–127. [Google Scholar] [CrossRef]
- Gero, K.; Aida, J.; Kondo, K.; Kawachi, I. Evaluation of Trust Within a Community After Survivor Relocation Following the Great East Japan Earthquake and Tsunami. JAMA Netw. Open 2020, 3, e2021166. [Google Scholar] [CrossRef] [PubMed]
- Instituto Nacional de Estadística. Datos Población por Islas y Sexo. 2021. Available online: https://www.ine.es/jaxiT3/Datos.htm?t=2910 (accessed on 4 May 2021).
- Área de Salud de Menorca. 2021. Available online: https://www.ibsalut.es/asme/es/ (accessed on 4 May 2021).
- Kalmijn, M.; Saraceno, C. A comparative perspective on intergenerational support: Responsiveness to parental needs in individualistic and familialistic countries. Int. J. Coop. Inf. Syst. 2008, 10, 479–508. [Google Scholar] [CrossRef]
- Daatlan, S.O.; Herlofson, K.; Lowenstein, A. Old Age and Autonomy. The Role of Service Systems and Intergenerational Family Solidarity. In Report of the Center for Research and Study of Aging; Lowenstein, A., Ogg., J., Eds.; OASIS: Haifa, Israel, 2003. [Google Scholar]
- Bettio, F.; Simonazzi, A.; Villa, P. Change in care regimes and female migration: The ‘care drain’ in the Mediterranean. J. Eur. Soc. Policy 2006, 16, 271–285. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Rodriguez, V.; Rojo-Perez, F.; Fernandez-Mayoralas, G. Family and Social Networks and Quality of Life Among Community-Dwelling Older-Adults in Spain. In Quality of Life in Communities of Latin Countries; Springer International Publishing: Handel, Switzerland, 2017; pp. 227–253. [Google Scholar] [CrossRef]
- TVE. Guía de la Desescalada: ¿Qué Puedo Hacer en Cada Fase? 2020. Available online: https://www.rtve.es/noticias/20200612/guia-fases-desescalada/2013020.shtml (accessed on 24 June 2020).
- Baker, K.D.; Skuse, D.H. Adolescents and young adults with 22qll deletion syndrome: Psychopathology in an at-risk group. Br. J. Psychiatry 2005, 186, 115–120. [Google Scholar] [CrossRef]
- Buer, L.-M.; Havens, J.R.; Leukefeld, C. Does the New Formulation of OxyContin® Deter Misuse? A Qualitative Analysis. Subst. Use Misuse 2014, 49, 770–774. [Google Scholar] [CrossRef] [PubMed]
- Cavaco, A.M.; Dias, J.P.S.; Bates, I.P. Consumers’ perceptions of community pharmacy in Portugal: A qualitative exploratory study. Pharm. World Sci. 2005, 27, 54–60. [Google Scholar] [CrossRef] [Green Version]
- Dworkin, S.L. Sample Size Policy for Qualitative Studies Using In-Depth Interviews. Arch. Sex. Behav. 2012, 41, 1319–1320. [Google Scholar] [CrossRef] [Green Version]
- Bradley, E.H.; Curry, L.A.; Devers, K.J. Qualitative data analysis for health services research: Developing taxonomy, themes, and theory. Health Serv. Res. 2007, 42, 1758–1772. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villalonga-Olives, E.; Kawachi, I. The measurement of bridging social capital in population health research. Health Place 2015, 36, 47–56. [Google Scholar] [CrossRef]
- Bolancé, C.; Caïs, J.; Torrente, D.J. Trust in times of economic crisis in Spain: Paradoxes for social capital theory. Work. Paper 2018, 30, 1–29. [Google Scholar]
- Brehm, J.; Rahn, W. Individual-Level Evidence for the Causes and Consequences of Social Capital. Am. J. Political Sci. 1997, 41, 999–1023. [Google Scholar] [CrossRef] [Green Version]
- Putnam, R.D.; Leonardi, R.; Nanetti, R.Y. Making Democracy Work: Civic Traditions in Modern Italy; Princeton University Press: Princeton, NJ, USA, 1994. [Google Scholar]
- Rothstein, B. Trust, Social Dilemmas and Collective Memories. J. Theor. Politics 2000, 12, 477–501. [Google Scholar] [CrossRef]
- García-Basteiro, A.; Alvarez-Dardet, C.; Arenas, A.; Bengoa, R.; Borrell, C.; Del Val, M.; Franco, M.; Gea-Sánchez, M.; Gestal, J.J.G.; Valcárcel, B.G.L.; et al. The need for an independent evaluation of the COVID-19 response in Spain. Lancet 2020, 396, 529–530. [Google Scholar] [CrossRef]
- Bargain, O.; Aminjonov, U. Trust and compliance to public health policies in times of COVID-19. J. Public Econ. 2020, 192, 104316. [Google Scholar] [CrossRef]
- Woelfert, F.S.; Kunst, J.R. How Political and Social Trust Can Impact Social Distancing Practices During COVID-19 in Unexpected Ways. Front. Psychol. 2000, 11, 572966. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age | Gender | Occupation | Time Interview |
|---|---|---|---|
| 26 | Female | Nurse | Strict lockdown |
| 58 | Female | Supermarket cashier | Strict lockdown |
| 53 | Female | Lab technician | Strict lockdown |
| 84 | Male | Nursing home resident | Strict lockdown |
| 47 | Female | Nurse | Strict lockdown |
| 84 | Female | Nursing home resident | Strict lockdown |
| 89 | Male | Nursing home resident | Strict lockdown |
| 65 | Female | Retired with husband hospitalized with COVID-19 | Strict lockdown |
| 78 | Female | Retired living with a couple | Strict lockdown |
| 78 | Female | Nursing home resident | Strict lockdown |
| 78 | Female | Nursing home resident | Strict lockdown |
| 74 | Female | Retired living with a couple | Strict lockdown |
| 41 | Female | Pharmacist | Lockdown with flexibility |
| 84 | Male | Retired living alone | Lockdown with flexibility |
| 61 | Female | Market cashier | Phase 0 |
| 48 | Male | Policeman | Phase 0 |
| 39 | Female | Policewoman | Phase 0 |
| 48 | Male | Pub owner | Phase 1 |
| 54 | Male | Business owner | Phase 1 |
| 37 | Male | Software developer | Phase 2 |
| 61 | Female | City Hall official | Phase 2 |
| 68 | Male | Business owner | Phase 2 |
| 62 | Male | Restaurant owner | Phase 3 |
| 40 | Female | Online banking manager | Phase 3 |
| 43 | Male | Medical doctor | Phase 3 |
| Topics Related to Social Capital | Examples of Quotes | |
|---|---|---|
| Emerging forms of social capital | Bounded solidarity | “The nursing home has not changed anything. It all works the same with the same organization. I have changed some of my jobs –nursing home treasurer- and we cannot leave the nursing home. We used to go out a lot. My activities used to be bingo and dancing. We have a completely different life than the one we had before. I can only speak with my friends over the phone” (Male. 84. Nursing home resident). “We used to have a lot of social life. I was into a lot of things. I used to go to university courses for seniors and with the “happy” grandmothers, to children’s story theater group, the book club and gym. Now nothing” (Female. 78. Retired). “There is a lot of partying and excitement on the street at 8 pm when we thank the medical staff from our window, balcony and terraces. It’s an emotional moment” (Female. 53. Lab technician). “We speak with our family very often. We always use video calling. Something we never did with friends from Menorca. With family, video calling has become a continuum. Grandma is an expert of social media now. Now with some friends we do crafts together by live zooming once a week. Something we could have done before” (Female. 47. Nurse). “My daughter, who works at a bank, stops by and asks if we need anything. She goes shopping and to her pharmacy for us” (Female. 78. Retired). “We have a video call with the family after 8 o’clock. I see my other daughter on the balcony. My children who live in Menorca have been able to go to the hospital and see their father who is hospitalized infected with COVID-19. I have had very bad days. Now I’m calm. We have a neighbor who usually makes a video during summer to celebrate summer festivities. This year he created a video with the neighbors of our village singing, dancing and playing drums. He included pictures of my husband in the hospital saying we should resist and fight against the virus“ (Female. 65. Retired. Husband hospitalized with COVID-19). “Yes, a social network for doing things for others has been created. If someone needed something he/she posted it. This was mostly to help people who couldn’t go out (go to their pharmacy, market…). My father-in-law is 81 years old and has no problem using technology. Now there are people that have learnt a lot of stuff“ (Male. 48. Bar Pub owner). “Suddenly we have met all our neighbors. Before this we didn’t know them. There are around 9 houses on our street. We go out at 8 pm and we have started to get to know each other. We’ve also had bingo at 7:30 pm with the children in the street. And other activities. Some people are very participative” (Female. 41. Pharmacist). “I have seen the town very empty. And a lot of people clapping after 8 pm. Today some people were pretending to get married wearing costumes and they were joking from their balconies. At 1 pm. People were having a good time. And this kills time and makes people laugh. I saw a video of it because someone recorded it” (Female. 61, market cashier). “There has been a lot of promotion of local stores and farmers have been selling produce online. And people have responded to those initiatives. I do believe there have been changes. Some people have been making masks and giving them away” (Female. 47. Nurse). “Now he (her son) comes to see me through the window and we speak over the phone. They have given us resources to make video calls. My granddaughter can call me. I have grandchildren in Girona and Barcelona and I have been able to see them. This has changed everything. Before we had never done it” (Female. 84. Nursing home resident). “I haven’t been out since the lockdown started on March 14th. My situation is good because the town hall called me during the first week to ask if I needed anything. I’m fortunate because I have four children and I am very well taken care of. I follow the situation on TV. Now I make video calls and that way I can see everybody every day. All my children” (Male. 84. Retired). “The face masks have been the most relevant issue. We have received masks from mainland Spain, that is an example of solidarity. Even retired ladies from all over Spain have been sending them. They have also sent us hand sanitizer. Solidarity with us too. The 8 pm walks. Some drawings they sent us go straight to the heart” (Male. 48. Policeman). “Phone and Skype. We live very close. Grandma died this week and we were able to go and see her, but we were not able to see her before. I have video calls with my mother. A lot of people have called to offer their help to those in need. As law enforcement officers, we just told them that it was already organized and that it wasn’t allowed. There are more volunteers at the Red Cross than ever before” (Female. 39. Policewoman). “My father has COPD and has not been out. I have helped my parents to avoid any trips. Total different story with my in-laws, they haven’t been so obedient and have gone out more. In fact, a lot of elderly people in Ciutadella have not respected the stay-at-home orders and have been amongst the people that have gone out more. Especially at the beginning of the lockdown” (Female. 41. Pharmacist). “I am part of the Association of Restaurants of Menorca. We held meetings to see how we could contribute to different local governments. We have done webinars and teleconferences for training, to solve questions, and so on” (Male. 54. Business owner). “Our small village organized a community fundraiser. Shoes factories stopped their production to produce masks and hospital gowns” (Female. 61. City Hall official). |
| Dark side of social capital | Ambivalence of island residents toward outsiders | “I am in favor of opening the island to tourism. But we need to test travelers and be able to control the situation. There should be a lot of investment in controls, but this is not happening. My father is at high risk since he is diabetic and has had heart attacks and pneumonia. I have brothers living in Madrid and they will not come to Menorca for this reason” (Female. 40. Online banking manager). “All tourists should come with PCR done two days before flying. If not, they shouldn’t be allowed to fly. Right now Menorca is very vulnerable” (Male. 43. Medical Doctor). “The privileged got here. They are smart and use their power to get a better life. In Menorca we have privileges compared to the other islands. The people that came here came to soil the island, they should have stayed home. People come here and they think they own the place” (Female. 74. retired). “I would prefer to keep the island closed to tourists this summer. But of course, I don’t have a business. My family doesn’t depend on tourism” (Male. 37. Software developer). “With no health there is no economy. I understand. But with no economy there is no health, either. We would end up with no doctors, no nurses…” (Male. 68. Business Owner. Interviewed during Phase 2). “People that came here should have taken preventive measures. It is true we need them to come because they spend money here. But the arrival of visitors has not been controlled” (Female. 61, market cashier). “There is economic pressure on health” (Female. 61. City Hall official). “Unfortunately, we have an economy based on tourism. Now, I am afraid that if things are not done properly and there is a resurgence of the pandemic, most businesses will be on bankruptcy” (Male. 62. Restaurant owner). |
| Trust | Trust in politicians | “I don’t trust politicians. They are the worst scum. I am apolitical” (Female. 74, retired). “I don’t trust them. Some people see the situation earning 100,000 euros, while we see it with an empty pocket” (Male. 84. Nursing home resident). “I don’t trust them. I’m not saying they did a bad job. But at the same time, they didn’t do it right, because nobody was expecting this. On Monday they gave orders that were the last straw, and they had to rectify. They said kids could go to the grocery store and other stuff. They screwed up. I’m not saying others would have done it better” (Female. 41. Pharmacist). “I don’t trust them. It’s like having a lot of pigs together on a farm. First they fight, then they eat together and they end up rolling around in the same mud” (Male. 89. Nursing home resident). “No, they are all the same. They didn’t build a team to help each other. They have just fought each other. They are not politicians, they are nothing. This situation will get a lot of politicians out of the way, after this they will have to go back home” (Male. 84. Retired). “Not anymore. At first I did. Now I can’t see them well-balanced. There are too many people wanting to call the shots” (Female. 61, market cashier). “I want to trust them. Maybe too much. Everyone wants to do things and go forward. That is the problem, and they are not coordinated” (Female. 84. Nursing home resident). “I don’t trust them, I see a lot of improvisation. And they change their minds with social media” (Male. 48. Policeman). “The quality is low and it’s happening in all countries. In Spain we could fire practically all of them. One can’t see people that are capable of doing things right. Two weeks ago, the Labor Minister said that bars would not be able to reopen until New Year’s Eve. Eight Months closed? I can go and die” (Male. 48. Pub owner). |
| Trust | Trust in scientific leaders | “I trust scientific leaders that are not involved to politics. If your salary comes from the state, you cannot tell the truth. And they are also hiding the truth from you” (Female. 53. Lab technician). “Yes, I do trust them. It is because of them that the outcome will be good. It is an honor for them” (Female. 84. Nursing home resident). “I want to trust them. We need to trust someone. But I don’t trust them completely” (Female. 58. Supermarket cashier). “I trust them. These people are very busy. But if they are not able to influence politicians to address the problem based on truth, it’s going to be very complicated. They don’t have the power to decide” (Male. 48. Policeman). “Yes, I do trust them. But I have my reservations about them. I believe that sometimes the decisions they make as scientists should be made taking into account what is best for the economy. To increase their decision power, sometimes their decisions are too close to the people they favor. If politicians are not skilled enough to interpret things right, they don’t make good decisions” (Male. 48. Pub owner). “Yes. But unfortunately we are a country that cuts back on research and the best scientists we have end up working in countries where they have a lot more help to develop their work. I have relatives that are University Professors who, 15 years ago, had teams of 15 people working on very promising projects. All these projects stopped and could not be finalized” (Male. 62. Restaurant owner). |
| Trust in the military | “I don’t trust them, they are just another arm of the politicians” (Female. 47. Nurse). “I do, my husband was in the military. They have done a lot of work disinfecting” (Female. 65. Retired. Husband hospitalized with COVID-19). | |
| Trust in the neighbors and co-workers | “I don’t trust them. I’ve had a problem with one of them. During the lockdown, she waited (referring to her neighbor) for me in our parking garage and she coughed on me on purpose, and she was not wearing a mask. I recorded everything. I recorded it and I reported her to the police. We’ll see what happens with our lawyers. I’m not a person that lives on the staircase” (Female. 53. Lab technician). “There are all sorts of people (“talking about neighbors”). Some of them have just ignored the lockdown” (Male. 48. Pub owner). “I only trust my co-workers at the lab. I don’t know about the rest of the staff at the hospital. I have to fight to get the samples in the right conditions. The problem is that people from outside the lab don’t provide the samples in the right conditions and I have to argue with them so they do it right. I have to decontaminate the samples. It could be done better” (Female. 53. Lab technician). | |
| Emergent themes: socioeconomic differences | Frontline workers versus being allowed to work from home | “At the beginning it was overwhelming. There were long lines to access the shop. We had to remind people to keep their distances before accessing the business. Logistics were complicated” (Female. 58. Supermarket cashier). “I am lucky to work in tech. We develop software. I can work from home. The company is very flexible” (Male. 37. Software developer). |
| Mediterranean familial culture | My daughter, who works at a bank, stops by and asks if we need anything. She goes shopping and to her pharmacy for us (Female. 78. Retired). “The person who helped me the most was my daughter who is here next door. She goes shopping. I don’t have a driver’s license. She takes me to the hospital to see my husband. She is healthy and does absolutely everything” (Female. 65. Retired. Husband hospitalized with COVID-19). “Older adults are the ones who have been most affected. I don’t take care of older adults now. I used to take care of my granddaughter. Now I can’t. But I will do it again after the lockdown” (Female. 58. Supermarket cashier). “My mother was very worried. She is 86 years old. She worked a lot in the garden. She received phone calls from the City Council. My daughter took care of everything. Now with my grandson we do not take any preventive measure. I wore a mask on the first day I saw him after the lockdown. The other days we have had a normal life” (Female. 61. City Hall official). | |
| Inter-generational conflicts | “I guess there are all sorts of cases. A lot of students arrived. At first nobody liked it, but you understand the psychological part of wanting to be with the family. But it could have been done better. The people from Madrid were the first to arrive, because schools, universities, etc. shut down earlier than in other places and they just turned it into holidays. The problem is that they started leaving, leaving, leaving right from the start. You could see them everywhere. All the people that were able to leave and spread it all over Spain” (Female. 41. Pharmacist). “I have mixed feelings. It’s very wrong that they came to Menorca. But I also have friends that are studying away from home that came back before everything shut down. I understand them. But they contaminated us. It was wrong” (Female. 26. Nurse. Ex-COVID-19). “Honestly, I don’t think it was right. The students that were in Barcelona or in Madrid wanted to return home. They might be OK. But not the other ones” (Female. 65. Retired. Husband hospitalized with COVID-19). “Very irresponsible. I even think if your son or daughter is studying away from home and comes back, it’s very irresponsible. They have spread the virus to other places. A lot of people didn’t respect the 15-day quarantine” (Female. 39. Policewoman). | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villalonga-Olives, E.; Kawachi, I.; Hernández-Aguado, I. Social Capital during the First Wave of the COVID-19 Outbreak: The Case of the Island of Menorca. Int. J. Environ. Res. Public Health 2021, 18, 12720. https://doi.org/10.3390/ijerph182312720
Villalonga-Olives E, Kawachi I, Hernández-Aguado I. Social Capital during the First Wave of the COVID-19 Outbreak: The Case of the Island of Menorca. International Journal of Environmental Research and Public Health. 2021; 18(23):12720. https://doi.org/10.3390/ijerph182312720
Chicago/Turabian StyleVillalonga-Olives, Ester, Ichiro Kawachi, and Ildefonso Hernández-Aguado. 2021. "Social Capital during the First Wave of the COVID-19 Outbreak: The Case of the Island of Menorca" International Journal of Environmental Research and Public Health 18, no. 23: 12720. https://doi.org/10.3390/ijerph182312720