
COVID-19: Marking the Gaps in Migrant and Refugee Health in Some Massive Migration Areas

 , , , ,
, , , , 
{kind=link}
Abstract
:1. Introduction
2. Methods
3. Framing the Analysis
3.1. People and Promises
3.2. Health: Rights, Provisions and Practices
3.3. COVID-19 as an Additional Stress
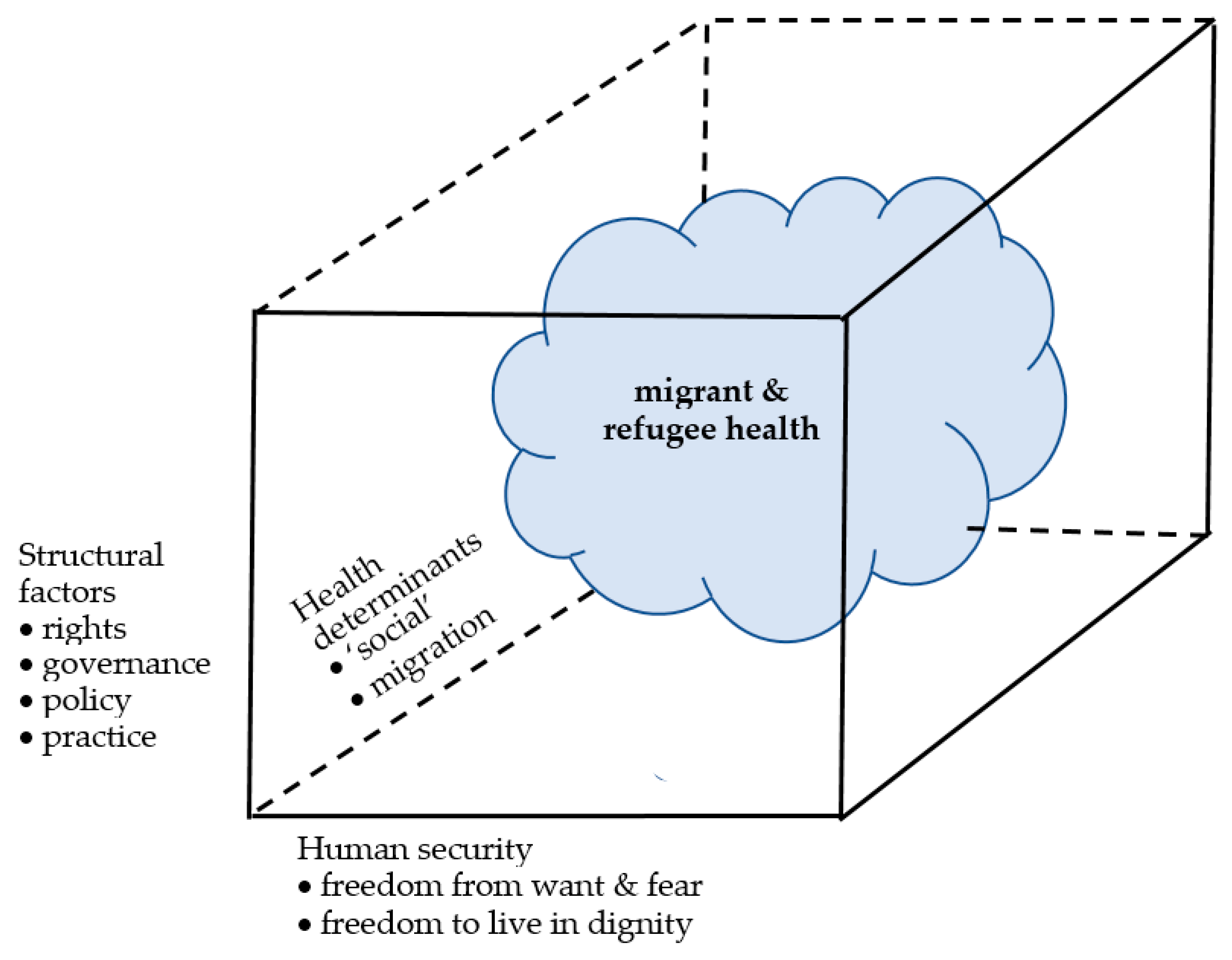
3.4. Perspectives of Enquiry
- Structural factors: Components include rights, governance, policies and practices.
- Health determinants: Frameworks based on the ‘social’ (which includes economic, environmental, social and political) determinants of health have been applied to the health of migrants and refugees. Moreover, migration itself has been recognised as a determinant, with risks to the health of migrants that may arise at every stage along their journeys, from before the migration process starts, during travel and at transit and destination point [1,32,33,34,35].
- Human security: The 1994 Human Development Report (HDR) of the United Nations Development Programme (UNDP) [36] replaced the traditional interpretation of security as relating to national/territorial security with a new one centred on the security of people. The new concept of human security, defined [37] as “freedom from want and fear and freedom to live in dignity” simultaneously broadened the focus of security itself, while also emphasising the role of actors beyond the nation state and the vital importance of collective international responsibility and action, recognizing the multi-sectoral interconnectivity of factors operating across the spectrum of social, economic, and cultural affairs [38,39,40]. The 1994 HDR listed seven main, interactive and interconnected categories of threats to human security: health, food, environmental, economic, personal, community and political.
4. Results and Discussion
4.1. Some Regional and Country Experiences of Massive Migration
4.2. Impacts of the COVID-19 Pandemic
4.3. Marking the Gaps
5. Conclusions: Minding the Gaps
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Matlin, S.A.; Depoux, A.; Schütte, S.; Flahault, A.; Saso, L. Migrants’ and refugees’ health: Towards an agenda of solutions. Public Health Rev. 2018, 39, 27. [Google Scholar] [CrossRef] [Green Version]
- Matlin, S.A.; Orcutt, M.; Bojorquez, I.; Karadağ Çaman, O.; Severoni, S.; Spiegel, P.; Veizis, A.; Saso, L. COVID-19 and migrant and refugee health: A pointer to system competence in future pandemic preparedness. Lancet EClin. Med. 2021, 36, 100904. [Google Scholar] [CrossRef] [PubMed]
- Takian, A.; Kiani, M.; Khanjankhani, K. COVID-19 and the need to prioritize health equity and social determinants of health. Int. J. Public Health 2020, 65, 521–523. [Google Scholar] [CrossRef] [PubMed]
- Expert Meeting on Migrant Health Issues in Massive Migration Areas in the COVID Period. Webinar Co-Organized by World Health Summit M8 Alliance (Sapienza University of Rome) and Association of Academic Health Centers International, 22 February 2021. Available online: https://www.worldhealthsummit.org/m8-alliance/migrant-refugee-health.html (accessed on 16 September 2021).
- International Migration 2020 Highlights; International Organization for Migration: Geneva, Switzerland, 2020; Available online: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/undesa_pd_2020_international_migration_highlights.pdf (accessed on 16 September 2021).
- Convention and Protocol Relating to the Status of Refugees; United Nations High Commissioner for Refugees: Geneva, Switzerland, 2010; Available online: https://www.unhcr.org/3b66c2aa10.html (accessed on 16 September 2021).
- Cartegena Declaration on Refugees; United Nations High Commissioner for Refugees: Geneva, Switzerland, 1984; Available online: http://www.unhcr.org/about-us/background/45dc19084/cartagena-declaration-refugees-adopted-colloquium-international-protection.html (accessed on 16 September 2021).
- New York Declaration for Refugees and Migrants; UN General Assembly Resolution A/71/L.1, Adopted 13 September 2016; United Nations: New York, NY, USA, 2016; Available online: https://www.un.org/en/ga/search/view_doc.asp?symbol=A/RES/71/1 (accessed on 16 September 2021).
- Global Compact for Safe, Orderly and Regular Migration. UN General Assembly Document Resolution A/RES/73/195, Adopted 19 December 2018. Available online: https://www.un.org/en/ga/search/view_doc.asp?symbol=A/RES/73/195 (accessed on 16 September 2021).
- Global Compact on Refugees. Report of the United Nations High Commissioner for Refugees, Part II, UN General Assembly Document A/73/12(PartII), 2018. Available online: https://www.unhcr.org/gcr/GCR_English.pdf (accessed on 16 September 2021).
- Takian, A.; Rajaeieh, G. Peace, health, and sustainable development in the Middle East. Arch. Iran Med. 2020, 23 (Suppl. 1), S23–S26. [Google Scholar] [CrossRef] [PubMed]
- 15 Years of Migration in 15 Mesmerizing Maps. World Economic Forum 15 May 2017. Available online: www.weforum.org/agenda/2017/05/15-years-of-migration-in-15-mesmerizing-maps (accessed on 16 September 2021).
- Migration Then and Now. In OECD Insights: International Migration; World Economic Forum: Geneva, Switzerland, 2009; Chapter 2; pp. 18–39. Available online: https://www.oecd.org/migration/internationalmigrationthehumanfaceofglobalisation.htm (accessed on 16 September 2021).
- McAuliffe, M.; Khadria, B. (Eds.) World Migration Report 2020; International Organization for Migration: Geneva, Switzerland, 2020; Available online: https://www.un.org/sites/un2.un.org/files/wmr_2020.pdf (accessed on 16 September 2021).
- Dao, T.H.; Docquier, F.; Maurel, M.; Schaus, P. Global migration in the twentieth and twenty-first centuries: The unstoppable force of demography. Rev. World Econ. 2021, 157, 417–449. [Google Scholar] [CrossRef]
- International Organization for Migration. Glossary on Migration; IML Series No. 34; International Organization for Migration: Geneva, Switzerland, 2019; Available online: https://publications.iom.int/system/files/pdf/iml_34_glossary.pdf (accessed on 16 September 2021).
- Figures at a Glance. United Nations High Commissioner for Refugees, Geneva, 18 June 2020. Available online: https://www.unhcr.org/figures-at-a-glance.html (accessed on 16 September 2021).
- WHO Director-General. Promoting the Health of Refugees and Migrants: Draft Global Action Plan, 2019–2023. Seventy-Second World Health Assembly Document A72/25 Rev.1, 23 May 2019. Available online: https://apps.who.int/gb/ebwha/pdf_files/WHA72/A72_25Rev1-en.pdf (accessed on 16 September 2021).
- Gostin, L.O. WHO Global Action Plan to Promote the Health of Refugees and Migrants. Milbank Q. 2019, 97, 631–635. [Google Scholar] [CrossRef]
- Karadag Caman, O.; Karabey, S. What a pandemic reveals: Health inequalities and their reflection on policies. TESEV Briefs. 11 December 2020. Available online: www.tesev.org.tr/tr/research/what-a-pandemic-reveals-health-inequalities-and-their-reflection-on-policies (accessed on 16 September 2021).
- Kluge, H.H.P.; Jakab, Z.; Bartovic, J.; D’Anna, V.; Severoni, S. Refugee and migrant health in the COVID-19 response. Lancet 2020, 395, 1237–1239. [Google Scholar] [CrossRef]
- Greenaway, C.; Hargreaves, S.; Barkati, S.; Coyle, C.M.; Gobbi, F.; Veizis, A.; Douglas, P. COVID-19: Exposing and addressing health disparities among ethnic minorities and migrants. J. Travel Med. 2020, 27, taaa113. [Google Scholar] [CrossRef] [PubMed]
- Hargreaves, S.; Kumar, B.N.; McKee, M.; Jones, L.; Veizis, A. Europe’s migrant containment policies threaten the response to COVID-19. BMJ 2020, 368, m1213. [Google Scholar] [CrossRef] [Green Version]
- Bempong, N.E.; Sheath, D.; Seybold, J.; Flahault, A.; Depoux, A.; Saso, L. Critical reflections, challenges and solutions for migrant and refugee health: 2nd M8 Alliance Expert Meeting. Public Health Rev. 2019, 40, 3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juárez, S.P.; Honkaniemi, H.; Dunlavy, A.C.; Aldridge, R.W.; Barreto, M.L.; Katikireddi, S.V.; Rostila, M. Effects of non-health-targeted policies on migrant health: A systematic review and meta-analysis. Lancet Glob. Health 2019, 7, e420–e435. [Google Scholar] [CrossRef] [Green Version]
- Competency Standards Framework for Clinicians. Culturally Responsive Clinical Practice: Working with People from Migrant and Refugee Backgrounds. Migrant and Refugee Women’s Health Partnership, Canberra. 2019. Available online: https://culturaldiversityhealth.org.au/wp-content/uploads/2019/02/Culturally-responsive-clinical-practice-Working-with-people-from-migrant-and-refugee-backgrounds-Jan2019.pdf (accessed on 16 September 2021).
- Promoting a Rights-Based Approach to Migration, Health, and HIV and AIDS: A Framework for Action; International Labour Office: Geneva, Switzerland, 2017; Available online: https://www.ilo.org/wcmsp5/groups/public/---dgreports/---gender/documents/publication/wcms_605763.pdf (accessed on 16 September 2021).
- Migration Policy Framework for Africa and Plan of Action (2018–2030). African Union, Addis Ababa. 2018. Available online: https://violenceagainstchildren.un.org/sites/violenceagainstchildren.un.org/files/documents/other_documents/35316-doc-au-mpfa_2018-eng.pdf (accessed on 16 September 2021).
- Promoting the Health of Refugees and Migrants: Framework of Priorities and Guiding Principles to Promote the Health of Refugees and Migrants; WHO: Geneva, Switzerland, 2017; Available online: https://www.who.int/migrants/about/framework_refugees-migrants.pdf (accessed on 16 September 2021).
- Hossin, M.Z. International migration and health: It is time to go beyond conventional theoretical frameworks. BMJ Glob. Health 2020, 5, e001938. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zimmerman, C.; Kiss, L.; Hossain, M. Migration and health: A framework for 21st Century policy-making. PLoS Med. 2011, 8, e1001034. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migration Health 2020 Impact Overview; International Organization for Migration: Geneva, Switzerland, 2021; Available online: https://publications.iom.int/system/files/pdf/MHD-Annual-Report-2020.pdf (accessed on 16 September 2021).
- Castañeda, H.; Holmes, S.M.; Madrigal, D.S.; Young, M.E.; DeTrinidad, B.N.; Quesada, J. Immigration as a social determinant of health. Ann. Rev. Public Health 2015, 36, 375–392. [Google Scholar] [CrossRef] [PubMed]
- Migration and Health. IOM Data Portal, 9 June 2020. Available online: https://migrationdataportal.org/themes/migration-and-health (accessed on 16 September 2021).
- Pavli, A.; Maltezou, H. Health problems of newly arrived migrants and refugees in Europe. J. Travel Med. 2017, 24, tax016. [Google Scholar] [CrossRef]
- UNDP. Human Development Report 1994: New Dimensions of Human Security; United Nations Development Programme: New York, NY, USA, 1994; Available online: http://www.hdr.undp.org/en/content/human-development-report-1994 (accessed on 16 September 2021).
- Human Security: Report of the UN Secretary-General; UN General Assembly Document No. A/64/701; United Nations: New York, NY, USA, 2010; Available online: https://daccess-ods.un.org/access.nsf/Get?Open&DS=A/64/701&Lang=E (accessed on 16 September 2021).
- McGrew, A.; Poku, N.K. Globalization, Development and Human Security; Wiley: Hoboken, NJ, USA, 2006; Available online: https://www.wiley.com/en-gb/Globalization,+Development+and+Human+Security-p-9780745630878 (accessed on 16 September 2021).
- Human Security in Theory and Practice; Human Security Unit, Office for the Coordination of Humanitarian Affairs, United Nations: New York, NY, USA, 2009; Available online: https://www.undp.org/content/dam/turkey/docs/news-from-new-horizons/issue-41/UNDP-TR-HSHandbook_2009.pdf (accessed on 16 September 2021).
- Flores, Y. Human Security. In Handbook of Security Science; Masys, A., Ed.; Springer: Cham, Switzerland, 2018. [Google Scholar] [CrossRef]
- Situation Report on International Migration 2019: The Global Compact for Safe, Orderly and Regular Migration in the Context of the Arab Region; United Nations High Commissioner for Refugees: Geneva, Switzerland, 2019; Available online: https://undocs.org/pdf?symbol=en/E/ESCWA/SDD/2019/3&usg=AOvVaw2Pg0A3p21uPvIR088UDqKF (accessed on 16 September 2021).
- Syria Emergency. United Nations High Commissioner for Refugees, Geneva. 2021. Available online: https://www.unhcr.org/uk/syria-emergency.html (accessed on 16 September 2021).
- Mataria, A.; Brennan, R.; Rashidian, A.; Hutin, Y.; Hammerich, A.; El-Adawy, M.; Hajjeh, R. ‘Health for All by All’ during a pandemic: ‘Protect Everyone’ and ‘Keep the Promise’ of Universal Health Coverage in the Eastern Mediterranean Region. East. Mediterr. Health J. 2020, 26, 1436–1439. [Google Scholar] [CrossRef]
- The Role of Inter-State Consultation Mechanisms on Migration in the Global Compact for Safe, Orderly and Regular Migration. International Organization for Migration, Geneva. 2019. Available online: https://publications.iom.int/books/role-inter-state-consultation-mechanisms-migration-global-compact-safe-orderly-and-regular (accessed on 16 September 2021).
- Helke, J. The Contribution of Regional Consultative Processes on Migration to the Global Compact on Safe, Orderly and Regular Migration; International Organization for Migration: Geneva, Switzerland, 2017; Available online: https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/unpd_cm15_201702_sessioniv_helke.pdf (accessed on 16 September 2021).
- Regional Consultative Processes on Migration. International Organization for Migration, Geneva. 2021. Available online: https://www.iom.int/regional-consultative-processes-migration (accessed on 16 September 2021).
- Arab Regional Consultative Process on Migration and Refugees Affairs. I International Organization for Migration, Geneva. 2021. Available online: https://www.iom.int/arab-regional-consultative-process-migration-and-refugee-affairs-arcp (accessed on 16 September 2021).
- Interregional Forums on Migration. International Organization for Migration, Geneva. 2021. Available online: https://www.iom.int/inter-regional-forums-migration (accessed on 16 September 2021).
- 5+5 Dialogue on Migration in the Western Mediterranean. International Organization for Migration, Geneva. 2021. Available online: https://www.iom.int/55-dialogue-migration-western-mediterranean (accessed on 16 September 2021).
- Budapest Process. International Organization for Migration, Geneva. 2021. Available online: https://www.iom.int/budapest-process (accessed on 16 September 2021).
- Regional action plan to promote the health of migrants, refugees and displaced populations. East. Mediterr. Health J. 2019, 25, 366–367. [CrossRef] [PubMed]
- COVID-19 Dominates Discussion of the 67th WHO Regional Committee for the Eastern Mediterranean. WHO News and Press Release, 13 October 2020. Available online: https://reliefweb.int/report/world/covid-19-dominates-discussion-67th-who-regional-committee-eastern-mediterranean (accessed on 16 September 2021).
- Statement of the WHO Regional Director for the Eastern Mediterranean on the Closing of the 67th Session of the Regional Committee. World Health Organization Regional Office for the Eastern Mediterranean, Cairo, 13 October 2020. Available online: http://www.emro.who.int/media/news/statement-of-the-who-regional-director-for-the-eastern-mediterranean-on-the-closing-of-the-67th-session-of-the-regional-committee.html (accessed on 16 September 2021).
- International Organization for Migration. Written Statement Submitted to the 67th Meeting of the WHO Regional Committee for the Eastern Mediterranean, 12–13 October 2020, Cairo, Egypt. WHO Regional Office for the Eastern Mediterranean, Cairo, 2020. Available online: http://www.emro.who.int/about-who/rc67/statements.html (accessed on 16 September 2021).
- El Arnaout, N.; Rutherford, S.; Zreik, T.; Nabulsi, D.; Yassin, N.; Saleh, S. Assessment of the health needs of Syrian refugees in Lebanon and Syria’s neighbouring countries. Confl. Health 2019, 13, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, M.; Luo, Z.; Zhou, D.; Ji, L.; Zhang, H.; Ghose, B.; Tang, S.; Wang, R.; Feng, D. Determinants of health insurance ownership in Jordan: A cross-sectional study of population and family health survey 2017–2018. BMJ Open 2021, 11, e038945. [Google Scholar] [CrossRef] [PubMed]
- El Arab, R.; Sagbakken, M. Healthcare services for Syrian refugees in Jordan: A systematic review. Eur. J. Public Health 2018, 28, 1079–1087. [Google Scholar] [CrossRef] [Green Version]
- What We Do: Health. United Nations Relief and Works Agency for Palestine Refugees in the Near East. 2021. Available online: https://www.unrwa.org/what-we-do/health (accessed on 16 September 2021).
- Jordan Health. United Nations Relief and Works Agency for Palestine Refugees in the Near East. 2021. Available online: https://www.unrwa.org/jordan-health (accessed on 16 September 2021).
- Kitamura, A.; Jimba, M.; McCahey, J.; Paolucci, G.; Shah, S.; Hababeh, M.; Shahin, Y.; Seita, A. Health and dignity of Palestine refugees at stake: A need for international response to sustain crucial life services at UNRWA. Lancet 2018, 392, 2736–2744. [Google Scholar] [CrossRef]
- Alduraidi, H.; Aqel, A.A.; Saleh, Z.; Almansour, I.; Darawad, M. UNRWA’s role in promoting health outcomes of Palestinian refugees in Jordan: A systematic literature review. Public Health Nurs. 2021, 38, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Amin, K. Health Status of Palestine Refugees from Syria in Jordan: Situation Analysis; Final Report; John Snow, Inc.: Boston, USA, 2017; Available online: https://www.jsi.com/JSIInternet/Inc/Common/_download_pub.cfm?id=18395&lid=3&usg=AOvVaw1ajboFkndIWrLV62PVMUtP (accessed on 16 September 2021).
- McKell, C.; Hankir, A.; Abu-Zayed, I.; Al-Issa, R.; Awad, A. Barriers to accessing and consuming mental health services for Palestinians with psychological problems residing in refugee camps in Jordan. Psychiatr. Danub. 2017, 29 (Suppl. 3), S157–S163. Available online: https://pubmed.ncbi.nlm.nih.gov/28953757/ (accessed on 16 September 2021).
- Tittle, V.; Bennett, D.L.; Hajat, S.; Shishtawi, A.; Zeidan, W.; Abuzabaida, F.; Ballout, G.; Abu-Zayed, I.; Hababeh, M.; Khade, A.; et al. Antenatal care among Palestine refugees in Jordan: Factors associated with UNRWA attendance. East. Mediterr. Health J. 2019, 25, 98–103. [Google Scholar] [CrossRef] [PubMed]
- Health of Refugees and Migrants: Situation Analysis and Practices in Addressing the Health Needs of Refugees and Migrants: Examples of Public Health Interventions and Practices; WHO Regional Office for the Eastern Mediterranean: Cairo, Egypt, 2018; Available online: https://www.who.int/migrants/publications/EMRO-report.pdf?ua=1 (accessed on 16 September 2021).
- Frenk, J.; Moon, S. Governance challenges in global health. N. Engl. J. Med. 2013, 368, 936–942. [Google Scholar] [CrossRef] [Green Version]
- 5th Brussels Conference on Syria: UNRWA Calls for Support to Help Palestine Refugees. UNRWA, 29 March 2021. Available online: https://reliefweb.int/report/jordan/5th-brussels-conference-syria-unrwa-calls-support-help-palestine-refugees (accessed on 16 September 2021).
- Jordan Fact Sheet. United Nations High Commissioner for Refugees, Geneva, February 2021. Available online: https://reliefweb.int/sites/reliefweb.int/files/resources/Jordan%20country%20factsheet%20-%20Feb%202021.pdf (accessed on 16 September 2021).
- Tyler, F. Characteristics and Challenges of the Health Sector Response in Lebanon. Ennonline 2014. Available online: https://www.ennonline.net/page/renderforpdf/4734 (accessed on 16 September 2021).
- Lebanon: Economic and Social Impact Assessment of the Syrian Conflict. World Bank, Washington DC, 20 September 2013. Available online: http://documents1.worldbank.org/curated/en/816911468266440541/pdf/889690ESW0Whit0385254B00PUBLIC00ACS.pdf (accessed on 16 September 2021).
- Chen, B.; Cammett, M. Informal politics and inequity of access to health care in Lebanon. Internat. J. Equity Health 2012, 11, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hannah-Amodio, C. Syrian Refugee Access to Healthcare in Lebanon. Relief Web 2020. Available online: https://reliefweb.int/report/lebanon/syrian-refugee-access-healthcare-lebanon (accessed on 16 September 2021).
- Lebanon: Shelter. United Nations High Commissioner for Refugees, Geneva. 2021. Available online: https://www.unhcr.org/lb/shelter (accessed on 16 September 2021).
- Hunter, P. The refugee crisis challenges national health care systems. EMBO Rep. 2016, 17, 492–495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alliance for Health Policy and Systems Research. Primary Health Care Systems (PRIMASYS): Comprehensive Case Study from Lebanon; WHO: Geneva, Switzerland, 2017; Available online: https://www.who.int/alliance-hpsr/projects/AHPSR-PRIMASYS-Lebanon-comprehensive.pdf (accessed on 16 September 2021).
- Diab, J.L.; Fouad, F.M. Navigating Access to Healthcare in Lebanon: The Political Economy of Health across Conflict, Revolution and Applicability; E-International Relations, 2020; ISSN 2053-8626. Available online: https://www.e-ir.info/2020/03/20/navigating-access-to-healthcare-in-lebanon-the-political-economy-of-health-across-conflict-revolution-and-applicability/ (accessed on 16 September 2021).
- Health Update. United Nations High Commissioner for Refugees, Lebanon, March 2014. Available online: https://reliefweb.int/report/lebanon/unhcr-lebanon-health-update-march-2014 (accessed on 16 September 2021).
- Lebanon Fact Sheet; United Nations High Commissioner for Refugees: Geneva, Switzerland, 2019; Available online: https://www.unhcr.org/lb/wp-content/uploads/sites/16/2019/04/Health-Factsheet.pdf (accessed on 16 September 2021).
- Report on the Health of Refugees and Migrants in the WHO European Region: No Public Health without Refugee and Migrant Health; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2018; Available online: https://apps.who.int/iris/bitstream/handle/10665/311347/9789289053846-eng.pdf?sequence=1&isAllowed=y&ua=1 (accessed on 16 September 2021).
- Turkey. United Nations High Commissioner for Refugees, Geneva, 2021. Available online: https://reporting.unhcr.org/turkey (accessed on 16 September 2021).
- Turkey: Refugee Response. International Organization for Migration, Geneva. 2021. Available online: https://turkey.iom.int/refugee-response (accessed on 16 September 2021).
- Turkey. International Committee of the Red Cross, Geneva. 2021. Available online: https://www.icrc.org/en/resource-centre/result?t=Turkey (accessed on 16 September 2021).
- Turkey. International Federation of Red Cross and Red Crescent Societies, Geneva. 2021. Available online: https://media.ifrc.org/ifrc/press-release/campaign-showcases-cash-assistance-helps-refugees-turkey-regain-control-lives/ (accessed on 16 September 2021).
- Turkey: Fact Sheet. European Civil Protection and Humanitarian Aid Operations, European Commission, Brussels. 2021. Available online: https://ec.europa.eu/echo/printpdf/where/europe/turkey_en (accessed on 16 September 2021).
- Guarascio, F.; Gumrukcu, T. EU, Turkey in stand-off over funds to tackle new migrant crisis. Reuters. 6 March 2020. Available online: https://www.reuters.com/article/us-syria-security-turkey-eu-idUSKBN20T1RH (accessed on 16 September 2021).
- Refugees in Iran. United Nations High Commissioner for Refugees, Geneva. 2021. Available online: https://www.unhcr.org/ir/refugees-in-iran/ (accessed on 16 September 2021).
- Operations: Islamic Republic of Iran. United Nations High Commissioner for Refugees, Geneva, 2021. Available online: https://reporting.unhcr.org/node/2527 (accessed on 16 September 2021).
- Kiani, M.M.; Khanjankhani, K.; Takbiri, A.; Takian, A. Refugees and sustainable health development in Iran. Arch. Iran. Med. 2021, 24, 27–34. [Google Scholar] [CrossRef]
- Dadras, O.; Taghizade, Z.; Dadras, F.; Alizade, L.; SeyedAlinaghi, S.; Ono-Kihara, M.; Kihara, M.; Nakayama, T. “It is good, but I can’t afford it …” potential barriers to adequate prenatal care among Afghan women in Iran: A qualitative study in South Tehran. BMC Pregnancy Childbirth 2020, 20, 274. [Google Scholar] [CrossRef] [PubMed]
- Doshmangir, L.; Bazyar, M.; Rashidian, A.; Gordeev, V.S. Iran health insurance system in transition: Equity concerns and steps to achieve universal health coverage. Int. J. Equity Health 2021, 20, 37. [Google Scholar] [CrossRef] [PubMed]
- Sajadi, H.S.; Goodarzi, Z.; Takian, A.; Mohamadi, E.; Olyaeemanesh, A.; Lotfi, F.H.; Sharafi, H.; Hekmat, S.N.; Jowett, M.; Majdzadeh, R. Assessing the efficiency of Iran health system in making progress towards universal health coverage: A comparative panel data analysis. Cost Eff. Resour. Alloc. 2020, 18, 20. [Google Scholar] [CrossRef]
- Roozbeh, N.; Sanati, A.; Abdi, F. Afghan refugees and immigrants health status in Iran: A systematic review. J. Clin. Diagn. Res. 2018, 12, 1–4. [Google Scholar] [CrossRef]
- 120,000 Refugees Assisted to Access Iran’s Health Insurance Scheme. United Nations High Commissioner for Refugees, Geneva, 6 April 2021. Available online: https://www.unhcr.org/uk/news/briefing/2021/4/606c19ad4/120000-refugees-assisted-access-irans-health-insurance-scheme.html (accessed on 16 September 2021).
- Takbiri, A.; Takian, A.; Rahimi Foroushani, A.; Jaafaripooyan, E. The challenges of providing primary health care to Afghan immigrants in Tehran: A key global human right issue. Int. J. Human Rights Healthc. 2020, 13, 259–273. [Google Scholar] [CrossRef]
- Divkolaye, N.S.H.; Burkle, F.M. The enduring health challenges of Afghan immigrants and refugees in Iran: A Systematic Review. PLoS Curr. 2017, 9. [Google Scholar] [CrossRef] [Green Version]
- Heydari, A.; Amiri, R.; Nayeri, N.; AboAli, V. Afghan refugees’ experience of Iran’s health service delivery. Int. J. Human Rights Healthc. 2016, 9, 75–85. [Google Scholar] [CrossRef]
- Salmani, I.; Seddighi, H.; Nikfard, M. Access to health care services for Afghan refugees in Iran in the COVID-19 pandemic. Disaster. Med. Public Health Prep. 2020, 14, 13–14. [Google Scholar] [CrossRef]
- Sánchez-Alonso, B. The age of mass migration in Latin America. Econ. Hist. Rev. 2019, 72, 3–31. [Google Scholar] [CrossRef]
- Estevadeordal, A. Latin America: The Opportunity of Migration. Global Americans, 14 June 2019. Available online: https://theglobalamericans.org/2019/06/latin-america-the-opportunity-of-migration/ (accessed on 16 September 2021).
- Rapporteurship on the Rights of Migrants: Inter-American Commission on Human Rights, Organization of American States, Washington DC, 2021. Available online: https://www.oas.org/en/IACHR/jsForm/?File=/en/iachr/r/DM/default.asp (accessed on 16 September 2021).
- Guidance Document on Migration and Health. Pan-American Health Organization, Washington DC, 2019. Available online: https://www.paho.org/hq/index.php?option=com_docman&view=download&slug=guidance-document-on-migration-and-health&Itemid=270&lang=en (accessed on 16 September 2021).
- Health of Refugees and Migrants: Regional Situation Analysis, Practices, Experiences, Lessons Learned and Ways Forward. Pan-American Health Organization, Washington DC, 2018. Available online: https://www.who.int/migrants/publications/PAHO-report.pdf?ua=1 (accessed on 16 September 2021).
- Migration Data in South America. Migration Data Portal, 9 March 2021. Available online: https://migrationdataportal.org/regional-data-overview/migration-data-south-america (accessed on 16 September 2021).
- Venezuela Situation. United Nations High Commissioner for Refugees, Geneva. 2021. Available online: https://www.unhcr.org/uk/venezuela-emergency.html (accessed on 16 September 2021).
- Venezuelan Migrants and Refugees in Latin America and the Caribbean: A Regional Profile. Relief Web 2021. Available online: https://reliefweb.int/report/colombia/venezuelan-migrants-and-refugees-latin-america-and-caribbean-regional-profile (accessed on 16 September 2021).
- Torres, J.R.; Castro, J.S. Venezuela’s migration crisis: A growing health threat to the region requiring immediate attention. J. Travel Med. 2019, 269, tay141. [Google Scholar] [CrossRef] [PubMed]
- Chaves-González, D.; Echeverría-Estrada, C. Venezuelan Migrants and Refugees in Latin America and the Caribbean; A Regional Profile. Migration Policy Institute and International Organization for Migration, August 2020. Available online: https://data2.unhcr.org/en/documents/download/78709 (accessed on 16 September 2021).
- ress Release: New Colombia Migration Policy. Word Vision, 16 March 2021. Available online: https://www.wvi.org/newsroom/venezuela-crisis/press-release-new-colombia-migration-policy (accessed on 16 September 2021).
- Farha, L.; Jaoude, J.A. Lebanese Healthcare System: How will the aftermath look? Cureus 2020, 12, e10270. [Google Scholar] [CrossRef]
- Ali, M.A.; Al-Khani, A.-M.; Sidahmed, L.A. Migrant health in Saudi Arabia during the COVID-19 pandemic. East. Mediterr. Health J. 2020, 26, 879–880. [Google Scholar] [CrossRef]
- Jordan: Operational Update. United Nations High Commissioner for Refugees, Geneva, March 2021. Available online: https://reporting.unhcr.org/sites/default/files/Jordan%20Operational%20Update%20March%202021.pdf (accessed on 16 September 2021).
- UNHCR Jordan COVID-19 Response. United Nations High Commissioner for Refugees, Geneva, 17 April 2021. Available online: https://reporting.unhcr.org/sites/default/files/Jordan%20COVID-19%20response%20-%2017%20April%202021.pdf (accessed on 16 September 2021).
- Salameh, P. COVID-19 in the Eastern Mediterranean Region: Testing frequency, cumulative cases and mortality analysis. East. Mediterr. Health J. 2020, 26, 1005–1010. [Google Scholar] [CrossRef] [PubMed]
- Karadag Caman, O.; Cinar, E.N.; Cevik, M.; Mardin, F.D.; Nergiz, A.I.; Karabey, S. Situational brief: Report on forced migrants and COVID-19 pandemic response in Turkey. Lancet Migr. Health 2020. Available online: https://1bec58c3-8dcb-46b0-bb2a-fd4addf0b29a.filesusr.com/ugd/188e74_55166625ed6440f680bb3bb0a7e6b9d5.pdf?index=true (accessed on 16 September 2021).
- Watson, H.; Wadha, K. Why Is Human Security Important? Trilateral Research, Waterford, Ireland, 7 April 2020. Available online: https://www.trilateralresearch.com/why-is-human-security-important/ (accessed on 16 September 2021).
- COVID-19 Coronavirus Pandemic. Worldometer, 16 September 2021. Available online: https://www.worldometers.info/coronavirus/?utm_campaign=homeAdUOA?Si#countries (accessed on 16 September 2021).
- Schwab, J. Fighting COVID-19 Could Cost 500 Times as Much as Pandemic Prevention Measures. World Economic Forum, 3 August 2020. Available online: https://www.weforum.org/agenda/2020/08/pandemic-fight-costs-500x-more-than-preventing-one-futurity/ (accessed on 16 September 2021).
- Elliott, L. IMF Estimates Global Covid Cost at $28tn in Lost Output. The Guardian, 13 October 2020. Available online: https://www.theguardian.com/business/2020/oct/13/imf-covid-cost-world-economic-outlook (accessed on 16 September 2021).
- World Economic Outlook: A Long and Difficult Ascent; International Monetary Fund: Washington, DC, USA, 2020; ISSN 0256-6877. Available online: https://www.imf.org/-/media/Files/Publications/WEO/2020/October/English/text.ashx (accessed on 16 September 2021).
- What Is the Impact of the COVID-19 Pandemic on Immigrants and Their Children? Organization for Economic Cooperation and Development, 19 October 2020. Available online: https://read.oecd-ilibrary.org/view/?ref=137_137245-8saheqv0k3&title=What-is-the-impact-of-the-COVID-19-pandemic-on-immigrants-and-their-children%3F (accessed on 16 September 2021).
- Global Preparedness Monitoring Board. A World at Risk: Annual Report on Global Preparedness for Health Emergencies. World Health Organization, Geneva. 2019. Available online: https://apps.who.int/gpmb/assets/annual_report/GPMB_annualreport_2019.pdf (accessed on 16 September 2021).
- Leal Filho, W.; Brandli, L.L.; Salvia, A.L.; Rayman-Bacchus, L.; Platje, J. COVID-19 and the UN Sustainable Development Goals: Threat to solidarity or an opportunity? Sustainability 2020, 12, 5343. [Google Scholar] [CrossRef]
- The Sustainable Development Goals: Our Framework for COVID-19 Recovery. United Nations, New York. 2021. Available online: https://www.un.org/sustainabledevelopment/sdgs-framework-for-covid-19-recovery/ (accessed on 16 September 2021).
- Operations: Bangladesh. United Nations High Commissioner for Refugees, Geneva. 2021. Available online: https://reporting.unhcr.org/bangladesh (accessed on 16 September 2021).
- Impact of COVID-19 on Bangladesh’s Overseas Migrant Workers: Responses and Recommendations. ILO Migration Programme, Dhaka, Bangladesh, 30 April 2020. Available online: https://www.ilo.org/wcmsp5/groups/public/---asia/---ro-bangkok/---ilo-dhaka/documents/meetingdocument/wcms_762473.pdf (accessed on 16 September 2021).
- Siddiqui, T. International Labour Migration from Bangladesh: A Decent Work Perspective; Working Paper No 66; International Labour Office: Geneva, Switzerland, 2005; Available online: https://www.ilo.org/wcmsp5/groups/public/---dgreports/---integration/documents/publication/wcms_079174.pdf (accessed on 16 September 2021).
- Access to Justice for Bangladeshi Migrant Workers: Opportunities and Challenges. Ovibashi Karmi Unnayan Program, Dhaka. 2019. Available online: https://cafod.org.uk/content/download/50452/636829/version/1/file/Access_Justice_Report_2019-1.pdf (accessed on 16 September 2021).
- Karim, M.R.; Islam, M.T.; Talukder, B. COVID-19′s impacts on migrant workers from Bangladesh: In search of policy intervention. World Dev. 2020, 136, 105123. [Google Scholar] [CrossRef]
- Bodrud-Doza, M.; Mashura, S.; Bahlman, L.; Abu Reza, M.; Towfiqul, I.; Rahman, M.M. Psychosocial and socio-economic crisis in Bangladesh due to COVID-19 pandemic: A perception-based assessment. Front. Public Health 2020. [Google Scholar] [CrossRef]
- Migrant Vulnerability in Bangladesh, India, and Nepal: COVID-19 and Labour Migration, Thematic Series: Migration. Relief Web, 13 October 2020. Available online: https://reliefweb.int/report/bangladesh/migrant-vulnerability-bangladesh-india-and-nepal-covid-19-and-labour-migration (accessed on 16 September 2021).
- COVID-19 Crisis through a Migration Lens. World Bank, Washington DC, Migration and Development Brief 32, April 2020. Available online: https://documents.worldbank.org/en/publication/documents-reports/documentdetail/989721587512418006/covid-19-crisis-through-a-migration-lens (accessed on 16 September 2021).
- Das, B.C.; Sutradhar, R. The Impact of COVID-19 Pandemic on the Inflow of Remittances: Perspective of Bangladesh; MPRA Paper 101083; Munich Personal RePEc Archive: Munich, Germany, 2020; Available online: https://ideas.repec.org/p/pra/mprapa/101083.html (accessed on 16 September 2021).
- Onarheim, K.H.; Rached, D.H. Searching for accountability: Can the WHO global action plan for refugees and migrants deliver? BMJ Glob. Health 2020, 5, e002095. [Google Scholar] [CrossRef]
- Gilbert, G. Not bound but committed: Operationalizing the Global Compact on Refugees. Int. Migr. 2019, 57, 27–42. [Google Scholar] [CrossRef]
- Egli-Gany, D.; Aftab, W.; Hawkes, S.; Abu-Raddad, L.; Buse, K.; Rabbani, F.; Low, N.; Onarheim, K.H. The social and structural determinants of sexual and reproductive health and rights in migrants and refugees: A systematic review of reviews. East. Mediterr. Health J. 2020, 26. [Google Scholar] [CrossRef]
- Health of Migrants: Resetting the Agenda. International Organization for Migration, Geneva. 2017. Available online: https://www.iom.int/sites/default/files/our_work/DMM/Migration-Health/Health-of-Migrants-resetting-the-agenda.pdf (accessed on 16 September 2021).
- New Pact on Migration and Asylum. European Commission, Brussels, 23 September 2020. Available online: https://ec.europa.eu/info/publications/migration-and-asylum-package-new-pact-migration-and-asylum-documents-adopted-23-september-2020_en (accessed on 16 September 2021).
- Daszak, P.; Neves, C.d.; Amuasi, J.; Hayman, D.; Kuiken, T.; Roche, B.; Zambrana-Torrelio, C.; Buss, P.; Dundarova, H.; Feferholtz, Y.; et al. Workshop Report on Biodiversity and Pandemics of the Intergovernmental Platform on Biodiversity and Ecosystem Services; IPBES Secretariat: Bonn, Germany, 2020; p. 5. [Google Scholar] [CrossRef]
- Kickbusch, I. Global Health Security: A Cosmopolitan Moment? The Global Governance Project, 1 June 2015. Available online: https://www.globalgovernanceproject.org/global-health-security-cosmopolitan-moment/ (accessed on 16 September 2021).
- Di Marco, M.; Baker, M.L.; Daszak, P.; De Barro, P.; Eskew, E.A.; Godde, C.M.; Harwood, T.D.; Herrero, M.; Hoskins, A.J.; Johnson, E.; et al. Sustainable development must account for pandemic risk. Proc. Nat. Acad. Sci. USA 2020, 117, 3888–3892. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matlin, S.A.; Karadag, O.; Brando, C.R.; Góis, P.; Karabey, S.; Khan, M.M.H.; Saleh, S.; Takian, A.; Saso, L. COVID-19: Marking the Gaps in Migrant and Refugee Health in Some Massive Migration Areas. Int. J. Environ. Res. Public Health 2021, 18, 12639. https://doi.org/10.3390/ijerph182312639
Matlin SA, Karadag O, Brando CR, Góis P, Karabey S, Khan MMH, Saleh S, Takian A, Saso L. COVID-19: Marking the Gaps in Migrant and Refugee Health in Some Massive Migration Areas. International Journal of Environmental Research and Public Health. 2021; 18(23):12639. https://doi.org/10.3390/ijerph182312639
Chicago/Turabian StyleMatlin, Stephen A., Ozge Karadag, Claudio R. Brando, Pedro Góis, Selma Karabey, Md. Mobarak Hossain Khan, Shadi Saleh, Amirhossein Takian, and Luciano Saso. 2021. "COVID-19: Marking the Gaps in Migrant and Refugee Health in Some Massive Migration Areas" International Journal of Environmental Research and Public Health 18, no. 23: 12639. https://doi.org/10.3390/ijerph182312639