
Fear of COVID-19 and Trust in the Healthcare System Mediates the Association between Individual’s Risk Perception and Preventive COVID-19 Behaviours among Iranians

 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measures
2.2.1. Preventive Behaviour Scale (PBS)
2.2.2. Fear of COVID-19 Scale (FCV-19S)
2.2.3. Risk Perception Scale (RPS)
2.2.4. Revised Health Care System Distrust Scale (RHCSDS)
2.2.5. Sociodemographic Characteristics
2.3. Data Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Acter, T.; Uddin, N.; Das, J.; Akhter, A.; Choudhury, T.R.; Kim, S. Evolution of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) as coronavirus disease 2019 (COVID-19) pandemic: A global health emergency. Sci. Total Environ. 2020, 730, 138996. [Google Scholar] [CrossRef] [PubMed]
- Zhang, N.; Wang, L.; Deng, X.; Liang, R.; Su, M.; He, C.; Hu, L.; Su, Y.; Ren, J.; Yu, F.; et al. Recent advances in the detection of respiratory virus infection in humans. J. Med. Virol. 2020, 92, 408–417. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/table (accessed on 8 June 2021).
- Mahase, E. China coronavirus: What do we know so far? BMJ 2020, 368, m308. [Google Scholar] [CrossRef] [Green Version]
- Chirico, F.; Sacco, A.; Bragazzi, N.L.; Magnavita, N. Can air-conditioning systems contribute to the spread of SARS/MERS/COVID-19 Infection? Insights from a rapid review of the literature. Int. J. Environ. Res. Public Health 2020, 17, 6052. [Google Scholar] [CrossRef]
- Zhu, Y.; Chen, L.; Ji, H.; Xi, M.; Fang, Y.; Li, Y. The risk and prevention of novel coronavirus pneumonia infections among inpatients in psychiatric hospitals. Neurosci. Bull. 2020, 36, 299–302. [Google Scholar] [CrossRef] [Green Version]
- Adhikari, S.P.; Meng, S.; Wu, Y.-J.; Mao, Y.-P.; Ye, R.-X.; Wang, Q.-Z.; Sun, C.; Sylvia, S.; Rozelle, S.; Raat, H.; et al. Epidemiology, causes, clinical manifestation and diagnosis, prevention and control of coronavirus disease (COVID-19) during the early outbreak period: A scoping review. Infect. Dis. Poverty 2020, 9, 29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Velsen, L.; Beaujean, D.J.; van Gemert-Pijnen, J.E.; van Steenbergen, J.E.; Timen, A. Public knowledge and preventive behavior during a large-scale Salmonella outbreak: Results from an online survey in the Netherlands. BMC Public Health 2014, 14, 100. [Google Scholar] [CrossRef] [Green Version]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72,314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A.; et al. First Case of 2019 Novel Coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef]
- Bish, A.; Michie, S. Demographic and attitudinal determinants of protective behaviours during a pandemic: A review. Br. J. Health Psychol. 2010, 15, 797–824. [Google Scholar] [CrossRef] [Green Version]
- Liao, Q.; Wu, P.; Wing Tak Lam, W.; Cowling, B.J.; Fielding, R. Trajectories of public psycho-behavioural responses relating to influenza A(H7N9) over the winter of 2014–15 in Hong Kong. Psychol. Health 2019, 34, 162–180. [Google Scholar] [CrossRef]
- Oh, S.-H.; Lee, S.Y.; Han, C. The effects of social media use on preventive behaviors during infectious disease outbreaks: The mediating role of self-relevant emotions and public risk perception. Health Commun. 2021, 36, 972–981. [Google Scholar] [CrossRef]
- Prasetyo, Y.T.; Castillo, A.M.; Salonga, L.J.; Sia, J.A.; Seneta, J.A. Factors affecting perceived effectiveness of COVID-19 prevention measures among Filipinos during Enhanced Community Quarantine in Luzon, Philippines: Integrating Protection Motivation Theory and extended Theory of Planned Behavior. Int. J. Infect. Dis. 2020, 99, 312–323. [Google Scholar] [CrossRef]
- Yıldırım, M.; Geçer, E.; Akgül, Ö. The impacts of vulnerability, perceived risk, and fear on preventive behaviours against COVID-19. Psychol. Health Med. 2021, 26, 35–43. [Google Scholar] [CrossRef] [PubMed]
- Breakwell, G.M.; Fino, E.; Jaspal, R. The COVID-19 Preventive Behaviors Index: Development and validation in two samples from the United Kingdom. Eval. Health Prof. 2021, 44, 77–86. [Google Scholar] [CrossRef]
- Chan, H.F.; Brumpton, M.; Macintyre, A.; Arapoc, J.; Savage, D.A.; Skali, A.; Stadelmann, D.; Torgler, B. How confidence in health care systems affects mobility and compliance during the COVID-19 pandemic. PLoS ONE 2020, 15, e0240644. [Google Scholar] [CrossRef] [PubMed]
- Pearson, S.D.; Raeke, L.H. Patients’ trust in physicians: Many theories, few measures, and little data. J. Gen. Intern. Med. 2000, 15, 509–513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, M.A.; Dugan, E.; Zheng, B.; Mishra, A.K. Trust in physicians and medical institutions: What is it, can it be measured, and does it matter? Milbank Q. 2001, 79, 613–639. [Google Scholar] [CrossRef] [Green Version]
- Thom, D.H.; Hall, M.A.; Pawlson, L.G. Measuring Patients’ Trust in Physicians When Assessing Quality Of Care. Health Aff. 2004, 23, 124–132. [Google Scholar] [CrossRef] [Green Version]
- O’Malley, A.S.; Sheppard, V.B.; Schwartz, M.; Mandelblatt, J. The role of trust in use of preventive services among low-income African-American women. Prev. Med. 2004, 38, 777–785. [Google Scholar] [CrossRef]
- Musa, D.; Schulz, R.; Harris, R.; Silverman, M.; Thomas, S.B. Trust in the health care system and the use of preventive health services by older black and white adults. Am. J. Public Health 2009, 99, 1293–1299. [Google Scholar] [CrossRef] [PubMed]
- Chang, K.-C.; Hou, W.-L.; Pakpour, A.H.; Lin, C.-Y.; Griffiths, M.D. Psychometric testing of three COVID-19-related scales among people with mental illness. Int. J. Ment. Health Addict. 2020. ahead of print. [Google Scholar] [CrossRef]
- World Health Organisation. Coronavirus Disease (COVID-19) Situation Report–166. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200704-covid-19-sitrep-166.pdf?sfvrsn=6247972_6 (accessed on 10 June 2021).
- Ahorsu, D.K.; Imani, V.; Lin, C.-Y.; Timpka, T.; Broström, A.; Updegraff, J.A.; Årestedt, K.; Griffiths, M.D.; Pakpour, A.H. Associations between fear of COVID-19, mental health, and preventive behaviours across pregnant women and husbands: An actor-partner interdependence modelling. Int. J. Ment. Health Addict. 2020. ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-Y.; Imani, V.; Majd, N.R.; Ghasemi, Z.; Griffiths, M.D.; Hamilton, K.; Hagger, M.S.; Pakpour, A.H. Using an integrated social cognition model to predict COVID-19 preventive behaviours. Br. J. Health Psychol. 2020, 25, 981–1005. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.-Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and initial validation. Int. J. Ment. Health Addict. 2020. ahead of print. [Google Scholar] [CrossRef] [Green Version]
- Ahorsu, D.K.; Lin, C.-Y.; Pakpour, A.H. The association between health status and insomnia, mental health, and preventive behaviors: The mediating role of fear of COVID-19. Gerontol. Geriatr. Med. 2020, 6, 2333721420966081. [Google Scholar] [CrossRef] [PubMed]
- Shea, J.A.; Micco, E.; Dean, L.T.; McMurphy, S.; Schwartz, J.S.; Armstrong, K. Development of a revised Health Care System Distrust scale. J. Gen. Intern. Med. 2008, 23, 727–732. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ahorsu, D.K.; Lin, C.-Y.; Yahaghai, R.; Alimoradi, Z.; Broström, A.; Griffiths, M.D.; Pakpour, A.H. The mediational role of trust in the healthcare system in the association between generalized trust and willingness to get COVID-19 vaccination in Iran. Hum. Vaccines Immunother. 2021. ahead of print. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Publications: New York, NY, USA, 2018. [Google Scholar]
- Rosseel, Y. Lavaan: An R package for structural equation modeling and more. Version 0.5–12 (BETA). J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]


{kind=link}
| Mean (SD) or n (%) | |
|---|---|
| Age (year) | 34.15 (±12.31) |
| Gender | |
| Male | 1094 (30%) |
| Female | 2558 (70%) |
| Educational status | |
| Primary school | 195 (5%) |
| Secondary school | 759 (21%) |
| Diploma | 891 (24%) |
| University | 1807 (50%) |
| Marital status | |
| Single | 893 (24%) |
| Married | 2759 (76%) |
| Accommodations | |
| Rural | 721 (20%) |
| Urban | 2931 (80%) |
| Risk Perception | Fear of COVID-19 | Trust in the Healthcare System | Preventive COVID-19 Behaviours | ||
|---|---|---|---|---|---|
| Gender | Male | 4.44 ± 0.77 | 19.29 ± 6.89 | 3.88 ± 0.85 | 6.02 ± 0.92 |
| Female | 4.60 ± 063 | 21.68 ± 6.85 | 3.94 ± 0.79 | 6.38 ± 0.68 | |
| Educational status | Primary school | 3.11 ± 0.95 | 20.54 ± 8.05 | 3.69 ± 0.99 | 6.31 ± 0.95 |
| Secondary school | 2.96 ± 0.95 | 20.97 ± 7.20 | 3.87 ± 0.84 | 6.15 ± 0.87 | |
| Diploma | 3.15 ± 0.97 | 21.55 ± 6.97 | 3.91 ± 0.91 | 6.34 ± 0.70 | |
| University | 3.22 ± 0.90 | 20.73 ± 6.70 | 3.85 ± 0.89 | 6.29 ± 0.75 | |
| Marital status | Single | 4.42 ± 0.79 | 19.40 ± 7.12 | 3.84 ± 0.85 | 4.42 ± 0.79 |
| Married | 3.95 ± 0.79 | 21.47 ± 6.82 | 4.59 ± 0.64 | 6.32 ± 0.72 | |
| Accommodation | Rural | 4.46 ± 0.69 | 20.14 ± 7.25 | 3.99 ± 0.74 | 6.11 ± 0.90 |
| Urban | 4.56 ± 0.68 | 21.17 ± 6.86 | 3.91 ± 0.82 | 6.31 ± 0.73 | |
| Fear of COVID-19 | Risk Perception | Trust in Healthcare System | Preventive COVID-19 Behaviours | Mean | SD | Range | |
|---|---|---|---|---|---|---|---|
| Fear of COVID-19 | - | 0.321 ** | 0.170 ** | 0.125 ** | 21.00 | 6.95 | 7–35 |
| Risk perception | - | - | 0.110 ** | 0.091 ** | 3.14 | 0.94 | 1–5 |
| Trust in healthcare system | - | - | - | 0.228 ** | 3.88 | 0.89 | 1–5 |
| Preventive COVID-19 behaviours | - | - | - | - | 6.27 | 0.78 | 1–7 |
| Model | Coefficient | SE | t | p |
|---|---|---|---|---|
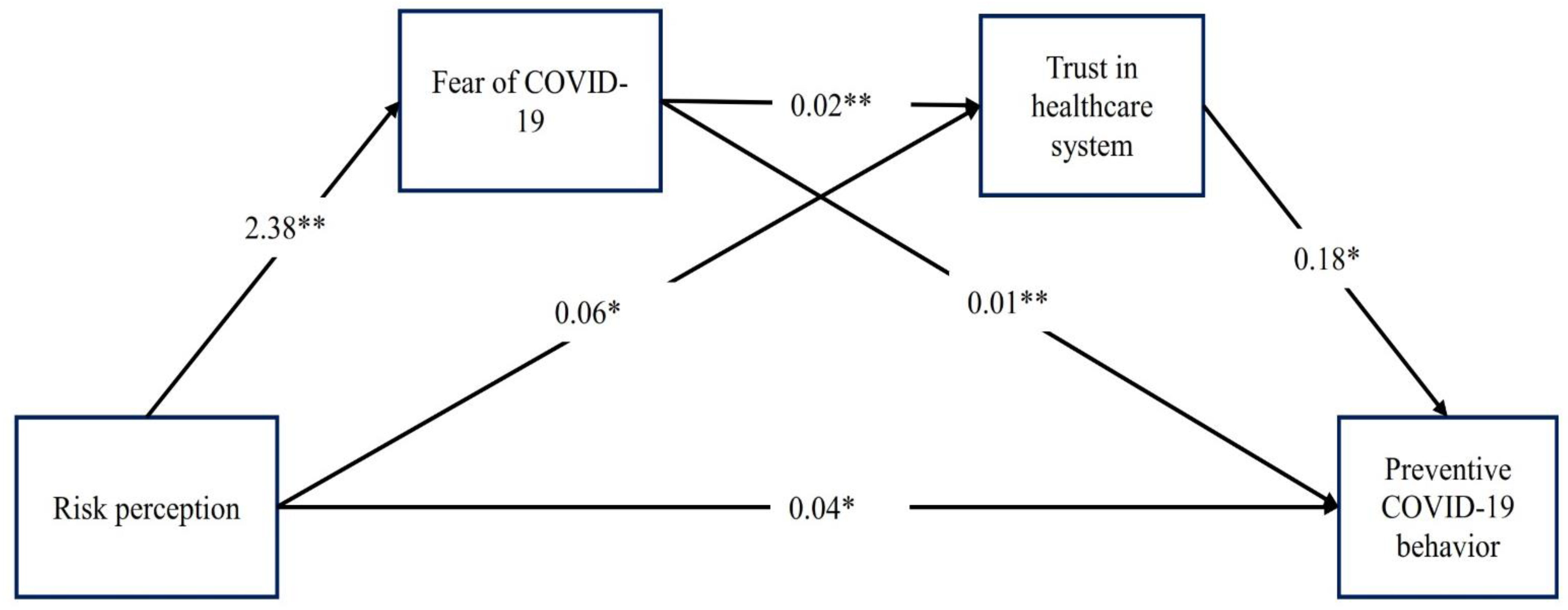
| Total effect of risk perception on preventive COVID-19 behaviours | 0.075 | 0.014 | 5.493 | <0.001 |
| Direct effect of risk perception on preventive COVID-19 behaviours in mediated model | 0.036 | 0.014 | 2.559 | 0.0105 |
| Indirect effect of risk perception on preventive COVID-19 behaviours | Effect | Boot SE | Boot LLCI | Boot ULCI |
| Total indirect effect | 0.039 | 0.007 | 0.027 | 0.052 |
| Indirect effect via fear of COVID-19 | 0.020 | 0.005 | 0.010 | 0.030 |
| Indirect effect via trust in healthcare system | 0.011 | 0.003 | 0.004 | 0.018 |
| Indirect effect via fear of COVID-19 and trust in healthcare system | 0.008 | 0.001 | 0.006 | 0.012 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alijanzadeh, M.; Ahorsu, D.K.; Alimoradi, Z.; Mahmoudi, N.; Griffiths, M.D.; Lin, C.-Y.; Liu, H.-K.; Pakpour, A.H. Fear of COVID-19 and Trust in the Healthcare System Mediates the Association between Individual’s Risk Perception and Preventive COVID-19 Behaviours among Iranians. Int. J. Environ. Res. Public Health 2021, 18, 12146. https://doi.org/10.3390/ijerph182212146
Alijanzadeh M, Ahorsu DK, Alimoradi Z, Mahmoudi N, Griffiths MD, Lin C-Y, Liu H-K, Pakpour AH. Fear of COVID-19 and Trust in the Healthcare System Mediates the Association between Individual’s Risk Perception and Preventive COVID-19 Behaviours among Iranians. International Journal of Environmental Research and Public Health. 2021; 18(22):12146. https://doi.org/10.3390/ijerph182212146
Chicago/Turabian StyleAlijanzadeh, Mehran, Daniel Kwasi Ahorsu, Zainab Alimoradi, Narges Mahmoudi, Mark D. Griffiths, Chung-Ying Lin, Hsien-Kuan Liu, and Amir H. Pakpour. 2021. "Fear of COVID-19 and Trust in the Healthcare System Mediates the Association between Individual’s Risk Perception and Preventive COVID-19 Behaviours among Iranians" International Journal of Environmental Research and Public Health 18, no. 22: 12146. https://doi.org/10.3390/ijerph182212146