
An Ergonomic Assessment of Different Postures and Children Risk during Evacuations


Abstract
:1. Introduction
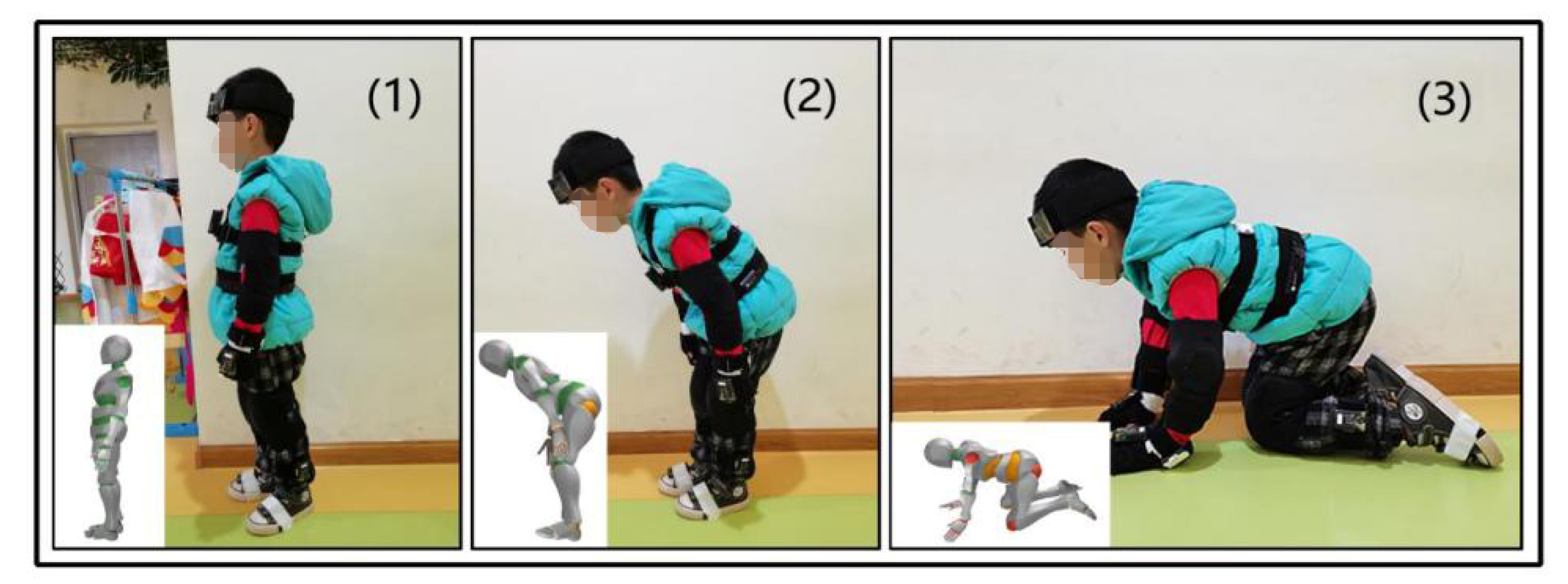
1.1. Evacuation Postures
1.2. Motion Capture System
1.3. Aims and Contributions
2. Methodology
2.1. Participants
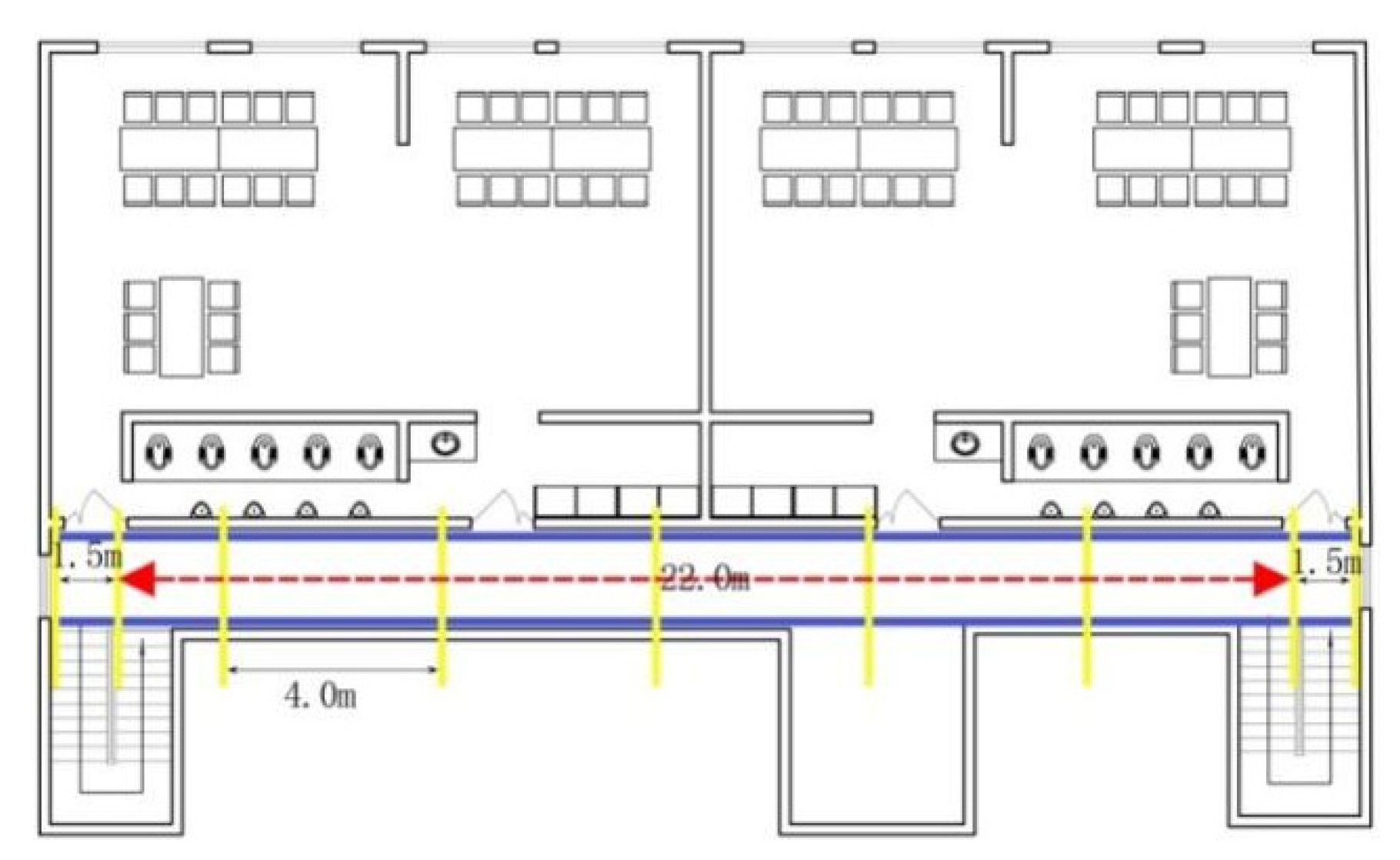
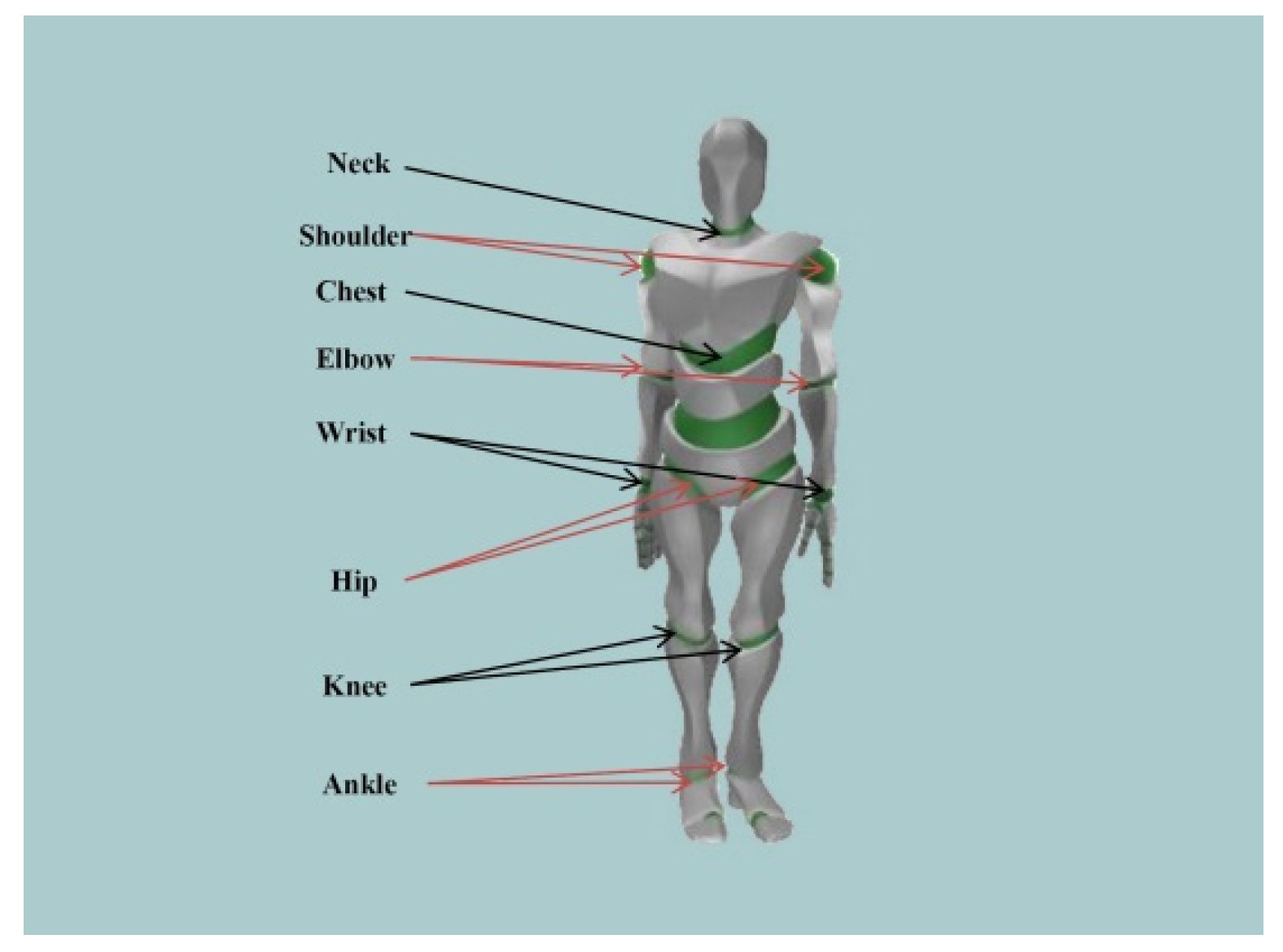
2.2. Experimental Setting and Equipment
2.3. Experimental Procedure
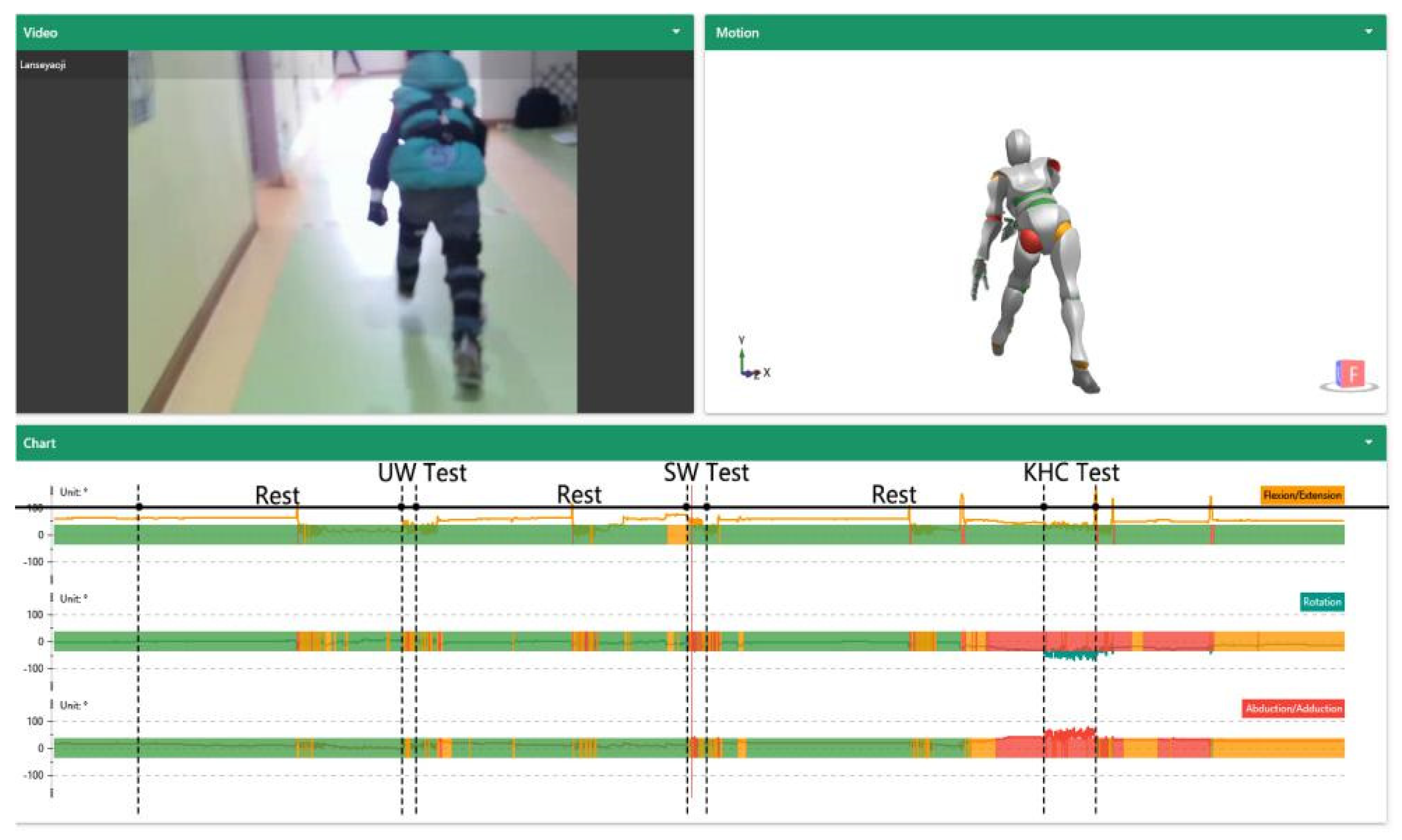
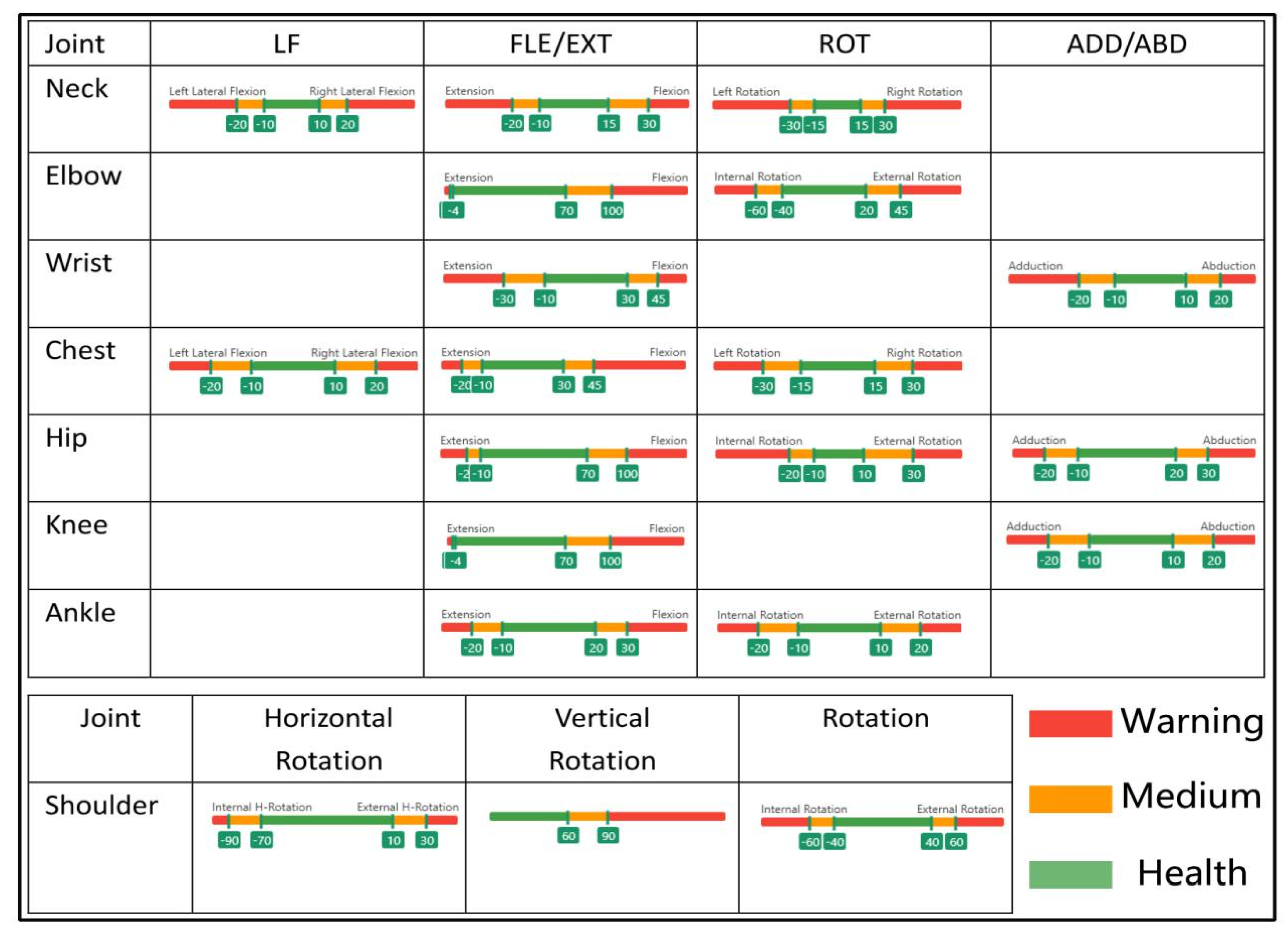
2.4. Data Analysis
3. Results
3.1. Evacuation Postures
3.1.1. Upright Walking
3.1.2. Stoop Walking
3.1.3. Knee and Hand Crawling
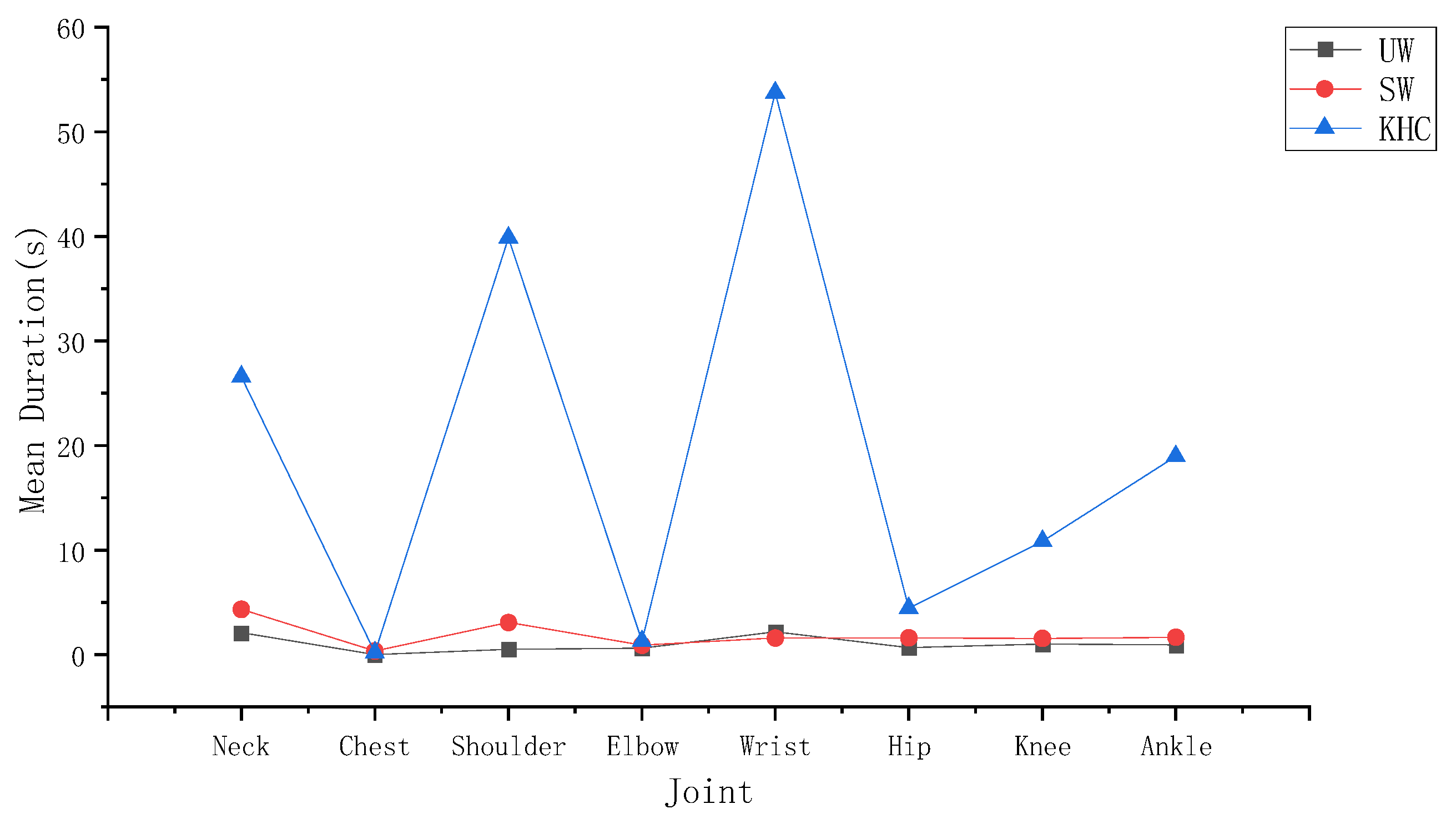
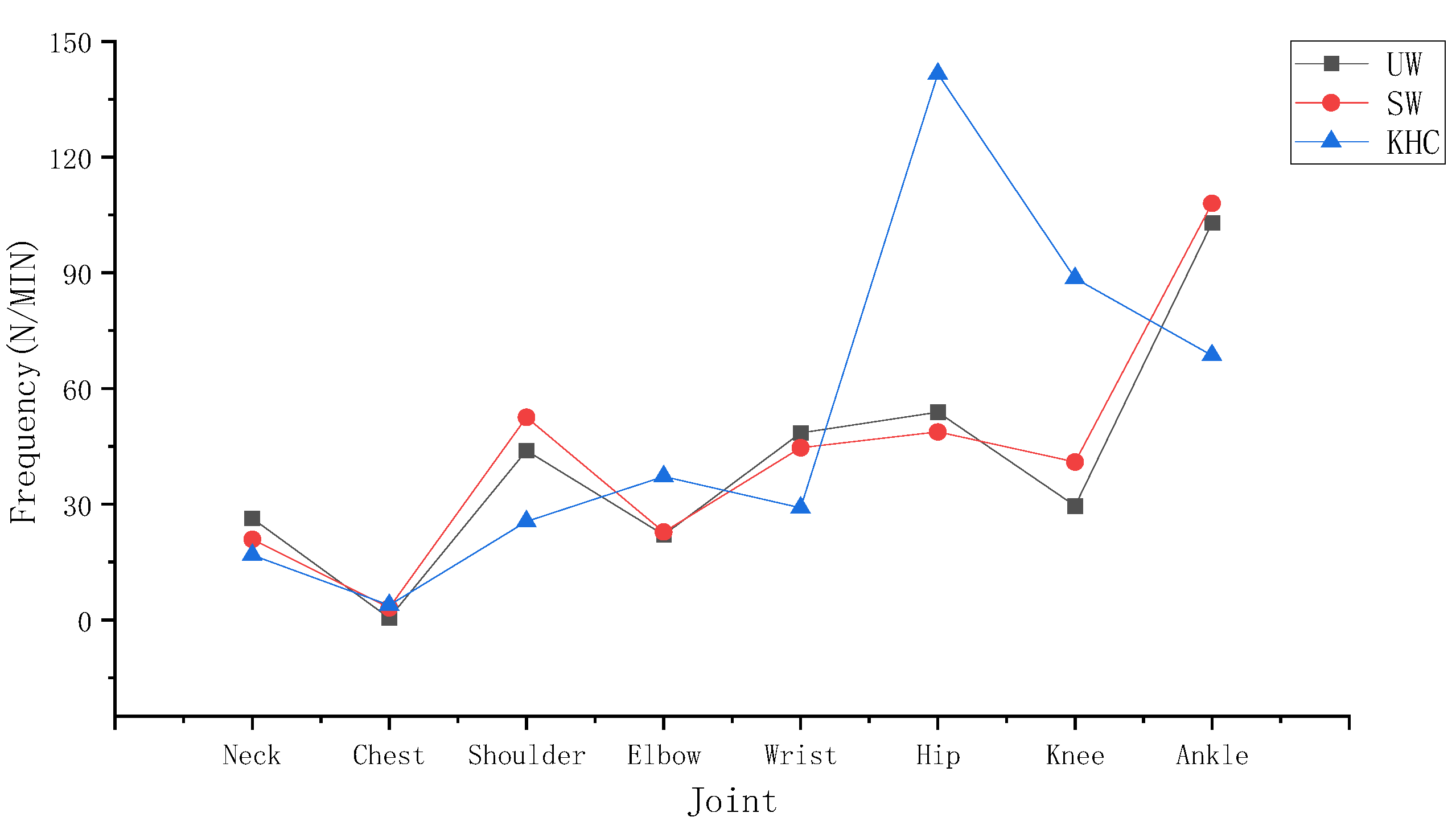
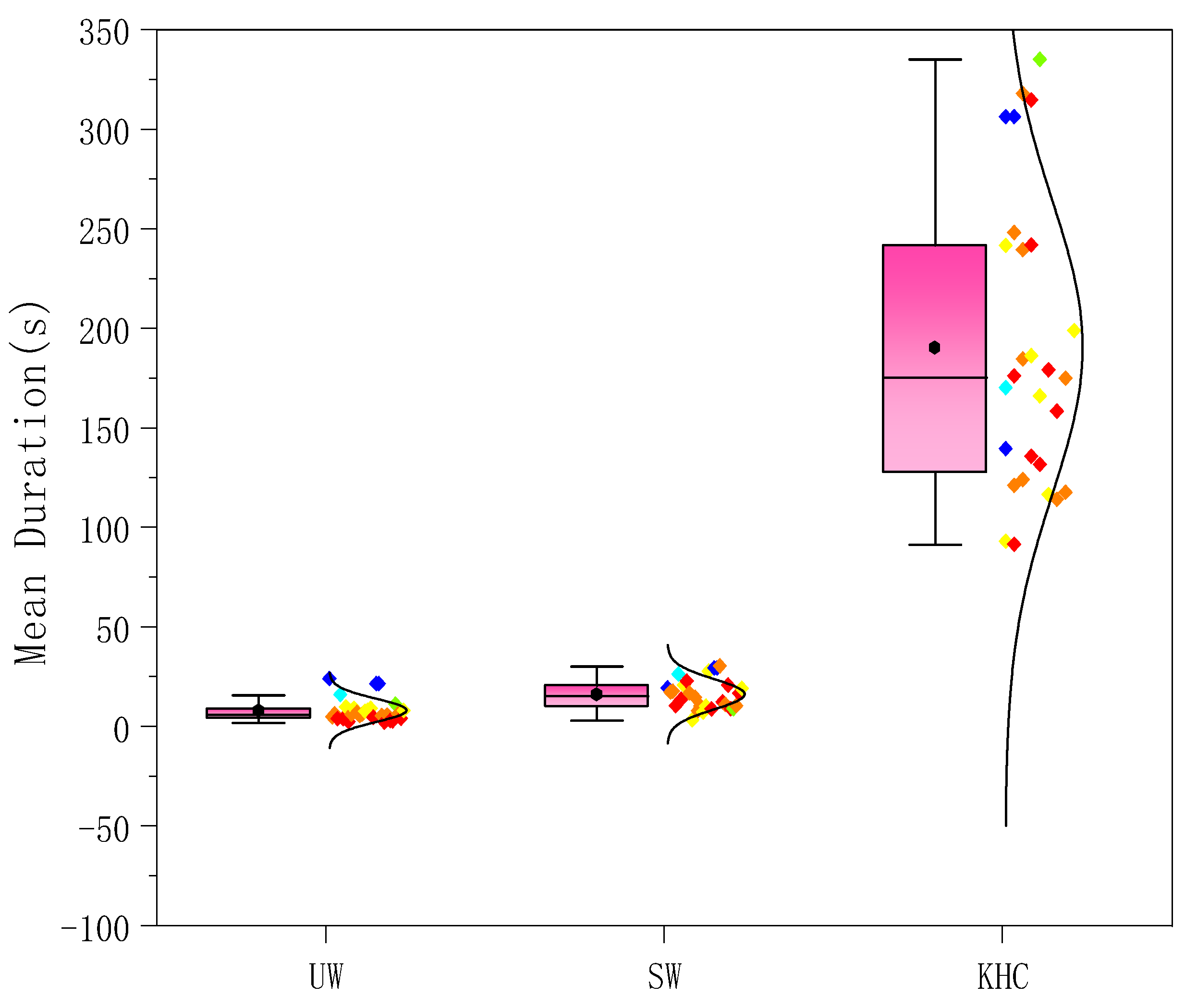
3.1.4. Comparison of the Three Situations
3.2. The Effect of Age/Gender on Children’s Joints
3.2.1. Gender
3.2.2. Age
4. Discussion and Limitation
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Adams, A.P.M.; Galea, E.R.T. An experimental evaluation of movement devices used to assist people with reduced mobility in high-rise building evacuations. In Pedestrian and Evacuation Dynamics; Peacock, R.D., Kuligowski, E.D., Averill, J.D., Eds.; Springer: Boston, MA, USA, 2011. [Google Scholar]
- Kholshevnikov, V.V.; Samoshin, D.A.; Istratov, R. The problems of elderly people safe evacuation from senior citizen health care buildings in case of fire. In Proceedings of the 5th International Symposium on Human Behavior in Fire, Cambridge, UK, 19–21 September 2012; pp. 587–592. [Google Scholar]
- Kecklund L, Andrée K, Bengtson S, Willander S, Siré E How do people with disabilities consider fire safety and evacuation possibilities in historical buildings?—A Swedish case study. Fire Technol. 2012, 48, 27–41. [CrossRef]
- Kuligowski, E.; Peacock, R.; Wiess, E.; Hoskins, B. Stair evacuation of older adults and people with mobility impairments. Fire Saf. J. 2013, 62, 230–237. [Google Scholar] [CrossRef]
- Larusdottir, A.R.; Dederichs, A.S. A step towards including children’s evacuation parameters and behavior in fire safe building design. Fire Saf. Sci. 2011, 10, 187–195. [Google Scholar] [CrossRef]
- Larusdottir, A.R.; Dederichs, A.S. Evacuation of children: Movement on stairs and on horizontal plane. Fire Technol. 2012, 48, 43–53. [Google Scholar] [CrossRef]
- Campanella, M.C.; Larusdottir, A.R.; Daamen, W.; Dederichs, A. Empirical data analysis and modelling of the evacuation of children from three multi-storey day-care centres. In Advanced Research Workshop Evacuation and Human Behavior in Emergency Situations; Universidad de Cantabria: Santander, Spain, 2011; pp. 223–226. [Google Scholar]
- Kholshevnikov, V.V.; Samoshin, D.A. Pre-school and school children building evacuation. In Proceedings of the 4th International Symposium on Human Behavior in Fire, Cambridge, UK, 13–15 July 2009; pp. 243–254. [Google Scholar]
- Cao, L.; Davis, J.; Gallagher, S. The impact of posture on evacuation speed. In Proceedings of the 2nd International Tall Building Fire Safety Conference, London, UK, 17–20 June 2014; pp. 111–121, ISBN 978-1-904521-85-3. [Google Scholar]
- Kady, R.; Davis, J. The effect of occupant characteristics on crawling speed in evacuation. Fire Saf. J. 2009, 44, 451–457. [Google Scholar] [CrossRef]
- Cao, L.; Davis, G.A.; Gallagher, S.; Schall, M.C.; Sesek, R.F. Characterizing posture and associated physiological demand during evacuation. Saf. Sci. 2018, 104, 1–9. [Google Scholar] [CrossRef]
- Najmanová, H.; Ronchi, E. An experimental data-set on pre-school children evacuation. Fire Technol. 2017, 53, 1509–1533. [Google Scholar] [CrossRef]
- Fang, Z.M.; Jiang, L.X.; Li, X.L.; Qi, W.; Chen, L.Z. Experimental study on the movement characteristics of 5–6 years old Chinese children when egressing from a pre-school building. Saf. Sci. 2019, 113, 264–275. [Google Scholar] [CrossRef]
- Larusdottir, A.R.; Dederichs, A.S. Evacuation dynamics of children walking speeds, flows through doors in daycare centers. In Pedestrian and Evacuation Dynamics; Springer: Boston, MA, USA, 2011; pp. 139–147. [Google Scholar]
- Zhou, J.; Jia, X.; Xu, G.; Jia, J.; Hai, R.; Gao, C.; Zhang, S. The Relationship between Different Types of Alarm Sounds and Children’s Perceived Risk Based on Their Physiological Responses. Int. J. Environ. Res. Public Health 2019, 16, 5091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Q.; Song, W.; Zhang, J.; Ye, R.; Ma, J. Experimental study on knee and hand crawling evacuation for different age group students. Int. J. Disaster Risk Reduct. 2020, 48, 101613. [Google Scholar] [CrossRef]
- Cockcroft, J.; Scheffer, C. Determining the feasibility of measuring outdoor road cycling kinematics using inertial motion capture technology. SAIEE Afr. Res. J. 2011, 102, 31–39. [Google Scholar] [CrossRef]
- Xsens MVN User Manual. Xsens 3D Motion Tracking. Available online: https://www.xsens.com/hubfs/Downloads/usermanual/MVN_User_Manual.pdf (accessed on 29 May 2020).
- Nweke, H.F.; Teh, Y.W.; Mujtaba, G.; Al-garadi, M.A. Data fusion and multiple classifier systems for human activity detection and health monitoring: Review and open research directions. Inf. Fusion 2019, 46, 147–170. [Google Scholar] [CrossRef]
- Chen, C.; Jafari, R.; Kehtarnavaz, N. A survey of depth and inertial sensor fusion for human action recognition. Multimed. Tools 2017, 76, 4405–4425. [Google Scholar] [CrossRef]
- Liu, L.; Wang, H.; Qiu, S.; Zhang, Y.; Hao, Z.-D. Paddle Stroke Analysis for Kayakers Using Wearable Technologies. Sensors 2021, 21, 914. [Google Scholar] [CrossRef] [PubMed]
- Wu, B.; Wu, Y.; Aoki, Y.; Nishimura, S. Mowing Patterns Comparison: Analyzing the Mowing Behaviors of Elderly Adults on an Inclined Plane via a Motion Capture Device. IEEE Access 2020, 8, 216623–216633. [Google Scholar] [CrossRef]
- Lanovaz, J.L.; Oates, A.R.; Treen, T.T.; Unger, J.; Musselman, K.E. Validation of a commercial inertial sensor system for spatiotemporal gait measurements in children. Gait Posture 2017, 51, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Mytton, J.; Goodenough, T.; Novak, C. Children and young people’s behavior in accidental dwelling fires: A systematic review of the qualitative literature. Saf. Sci. 2017, 96, 143–149. [Google Scholar] [CrossRef]
- Kinateder, M.; Ronchi, E.; Nilsson, D.; Kobes, M.; Müller, M.; Pauli, P.; Mühlberger, A. Virtual reality for fire evacuation research. In Proceedings of the 2014 Federated Conference on Computer Science and Information Systems, Warsaw, Poland, 7–10 September 2014; pp. 313–321. [Google Scholar]
- Zou, H.; Li, N.; Cao, L. Emotional response–based approach for assessing the sense of presence of subjects in virtual building evacuation studies. J. Comput. Civ. Eng. 2017, 31, 04017028. [Google Scholar] [CrossRef]
- Taciuc, A.; Dederichs, A.S. Determining Self-Preservation Capability in Pre-School Children; The Fire Protection Research Foundation; Technical Note Final Report, Technical Note Final Report; Technical University of Denmark: Copenhagen, Denmark, 2013. [Google Scholar]
- Zhou, J.; Jia, X.; Jia, J. Effects of Different Staircase Design Factors on Evacuation of Children from Kindergarten Buildings Analyzed via Agent-Based Simulation. Healthcare 2020, 8, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Council, I.C. International Building Code 2018; Intl Code Council: Washington, DC, USA, 2018. [Google Scholar]
- Ministry of Housing and Urban-Rural Development of the People’s Republic of China (MOHURD). Code for Fire Protection Design of Buildings; Ministry of Housing and Urban-Rural Development of the People’s Republic of China: Beijing, China, 2018; GB 50016-2014.
- Hulshof, C.T.J.; Pega, F.; Neupane, S.; Colosio, C.; Daams, J.G.; Kc, P.; Kuijer, P.P.F.M.; Mandic-Rajcevic, S.; Masci, F.; van der Mole, H.F.; et al. The effect of occupational exposure to ergonomic risk factors on osteoarthritis of hip or knee and selected other musculoskeletal diseases: A systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury. Environ. Int. 2021, 150, 106349. [Google Scholar]
- Patruno, C.; Marani, R.; Cicirelli, G.; Stella, E.; D’Orazio, T. People re-identification using skeleton standard posture and color descriptors from RGB-D data. Pattern Recognit. 2019, 89, 77–90. [Google Scholar] [CrossRef]
- David, G.C. Ergonomic methods for assessing exposure to risk factors for work-related musculoskeletal disorders. Occup. Med. 2005, 55, 190–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Beek, A.J.; Frings-Dresen, M.H.W. Assessment of mechanical exposure in ergonomic epidemiology. Occup. Health Ind. Med. 1998, 39, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dockrell, S.; O’Grady, E.; Bennett, K.; Mullarkey, C.; Connell, R.M.; Ruddy, R.; Twomey, S.; Flannery, C. An investigation of the reliability of Rapid Upper Limb Assessment (RULA) as a method of assessment of children’s computing posture. Appl. Ergon. 2012, 43, 632–636. [Google Scholar] [CrossRef]
- Sers, R.; Forrester, S.; Zecca, M.; Ward, S.; Moss, E. The impact of patient body mass index on surgeon posture during simulated laparoscopy. Appl. Ergon. 2020, 97, 103501. [Google Scholar] [CrossRef]
- Humadi, A.; Nazarahari, M.; Ahmad, R.; Rouhani, H. Instrumented Ergonomic Risk Assessment Using Wearable Inertial Measurement Units: Impact of Joint Angle Convention. IEEE Access 2021, 9, 7293–7305. [Google Scholar] [CrossRef]
- Valero, E.; Sivanathan, A.; Bosché, F.; Mohamed, A.-W. Musculoskeletal disorders in construction: A review and a novel system for activity tracking with body area network. Appl. Ergon. 2016, 54, 120–130. [Google Scholar] [CrossRef]
- Jebelli, H.; Changbum, R.A.; Stentz, T.L. Comprehensive Fall-Risk Assessment of Construction Workers Using Inertial Measurement Units: Validation of the Gait-Stability Metric to Assess the Fall Risk of Iron Workers. J. Comput. Civ. Eng. 2016, 30, 1–11. [Google Scholar] [CrossRef]
- Lin, J.F.; Kulić, D. Human pose recovery using wireless inertial measurement units. Physiol. Meas. 2012, 33, 2099–2115. [Google Scholar] [CrossRef]
- Zechner, M. Beginning Android Games; Apress: New York, NY, USA, 2011. [Google Scholar]
- Ghasemia, F.; Mahdavib, N. A new scoring system for the Rapid Entire Body Assessment (REBA) based on fuzzy sets and Bayesian networks. Int. J. Ind. Ergon. 2020, 80, 103058. [Google Scholar] [CrossRef]
- Abobakr, A.; Nahavandi, D.; Hossny, M.; Iskander, J.; Attia, M.; Nahavandi, S.; Smets, M. RGB-D ergonomic assessment system of adopted working postures. Appl. Ergon. 2019, 80, 75–88. [Google Scholar] [CrossRef] [PubMed]
- Siebers, H.L.; Eschweiler, J.; Quack, V.M.; Tingart, M.; Betsch, M. Inertial measurement units for the detection of the effects of simulated leg length inequalities. J. Orthop. Surg. Res. 2021, 16, 142. [Google Scholar] [CrossRef] [PubMed]
- Hulshof, C.T.J.; Pega, F.; Neupane, S.; van der Molen, F.H.; Colosio, C.; Daams, J.G.; Descatha, A.; Kc, P.; Kuijer, P.P.F.M.; Mandic-Rajcevic, S.; et al. The prevalence of occupational exposure to ergonomic risk factors: A systematic review and meta-analysis from the WHO/ILO Joint Estimates of the Work-related Burden of Disease and Injury. Environ. Int. 2021, 146, 106157. [Google Scholar] [CrossRef] [PubMed]
- Kee, D.; Karwowski, W. LUBA: An assessment technique for postural loading on the upper body based on joint motion discomfort and maximum holding time. Appl. Ergon. 2001, 32, 357–366. [Google Scholar] [CrossRef]
- Naddeo, A.; Cappetti, N.; D’Oria, C. Proposal of a new quantitative method for postural comfort evaluation. Int. J. Ind. Ergon. 2015, 48, 25–35. [Google Scholar] [CrossRef]
- Kilbom, A. Assessment of physical exposure in relation to work-related musculoskeletal disorders--what information can be obtained from systematic observations. Scand. J. Work. Environ. Health 1994, 20, 30–45. [Google Scholar] [PubMed]
- Belli, A.; Kyröläinen, H.; Komi, P.V. Moment and power of lower limb joints in running. Int. J. Sports Med. 2002, 23, 136–141. [Google Scholar] [CrossRef]
- Zhang, L.; Deng, C.F.; Xiong, Q.L.; Wu, X.Y.; Chen, Y.X.; Liu, Y.; Mu, C.L.; Yi, Z.J.; Hou, W.S. Analysis of the Inter-Joints Synergistic Patterns of Limbs in Infant Crawling. In Proceedings of the 2019 41st Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Berlin, Germany, 23–27 July 2019; pp. 4156–4159. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Gender | Number | Age (Years) | Height (cm) | Weight (kg) | BMI (kg/m2) | ||||
|---|---|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | ||
| Boys | 13 | 5.0 | 0.82 | 116.31 | 6.84 | 22.07 | 4.48 | 16.17 | 1.71 |
| Girls | 15 | 5.4 | 0.91 | 116.20 | 5.85 | 20.75 | 2.93 | 15.34 | 1.42 |
| Posture | Joint | Action | Mean | p |
|---|---|---|---|---|
| UW | Wrist | ADD/ABD | 1.50 | 0.40 |
| FLE/EXT | 1.29 | |||
| Ankle | ROT | 21.87 | 0.00 | |
| FLE/EXT | 83.55 | |||
| SW | Neck | FLE/EXT | 4.14 | 0.00 |
| ROT | 0.22 | |||
| LF | 0.22 | |||
| Ankle | ROT | 25.34 | 0.00 | |
| FLE/EXT | 85.13 | |||
| KHC | Wrist | FLE/EXT | 59.70 | 0.00 |
| ADD/ABD | 28.56 | |||
| Hip | ADD/ABD | 40.25 | 0.18 | |
| FLE/EXT | 45.65 | |||
| ROT | 56.85 |
| Motion Indicators | UW-SW | UW-KHC | SW-KHC | KHC-SW-UW |
|---|---|---|---|---|
| p | p | p | p | |
| Mean Duration | 0.484 | 0.000 | 0.000 | 0.000 |
| Frequency | 0.378 | 0.006 | 0.054 | 0.018 |
| Motion Indicators | Gender | UW | SW | KHC | |||
|---|---|---|---|---|---|---|---|
| Mean | p | Mean | p | Mean | p | ||
| Mean Duration (S) | Boy | 9.58 | 0.637 | 41.01 | 0.689 | 138.01 | 0.146 |
| Girl | 8.39 | 31.38 | 194.70 | ||||
| Frequency (N/MIN) | Boy | 382.04 | 0.157 | 384.83 | 0.065 | 406.65 | 0.648 |
| Girl | 317.13 | 298.67 | 429.99 | ||||
| Behavioral Indicators | Age | UW | SW | KHC | |||
|---|---|---|---|---|---|---|---|
| Mean | p | Mean | p | Mean | p | ||
| Mean Duration (S) | 4 | 6.47 | 0.388 | 36.32 | 0.610 | 176.98 | 0.125 |
| 5 | 11.27 | 58.57 | 123.58 | ||||
| 6 | 8.71 | 18.09 | 60.84 | ||||
| Frequency (N/MIN) | 4 | 315.89 | 0.673 | 288.50 | 0.429 | 370.72 | 0.119 |
| 5 | 383.03 | 345.10 | 410.89 | ||||
| 6 | 348.28 | 369.21 | 472.81 | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jia, X.; Zhang, B.; Gao, X.; Zhou, J. An Ergonomic Assessment of Different Postures and Children Risk during Evacuations. Int. J. Environ. Res. Public Health 2021, 18, 12029. https://doi.org/10.3390/ijerph182212029
Jia X, Zhang B, Gao X, Zhou J. An Ergonomic Assessment of Different Postures and Children Risk during Evacuations. International Journal of Environmental Research and Public Health. 2021; 18(22):12029. https://doi.org/10.3390/ijerph182212029
Chicago/Turabian StyleJia, Xiaohu, Bo Zhang, Xiaoyu Gao, and Jiaxu Zhou. 2021. "An Ergonomic Assessment of Different Postures and Children Risk during Evacuations" International Journal of Environmental Research and Public Health 18, no. 22: 12029. https://doi.org/10.3390/ijerph182212029