
The Effect of Therapeutic Hypothermia after Cardiac Arrest on the Neurological Outcome and Survival—A Systematic Review of RCTs Published between 2016 and 2020

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
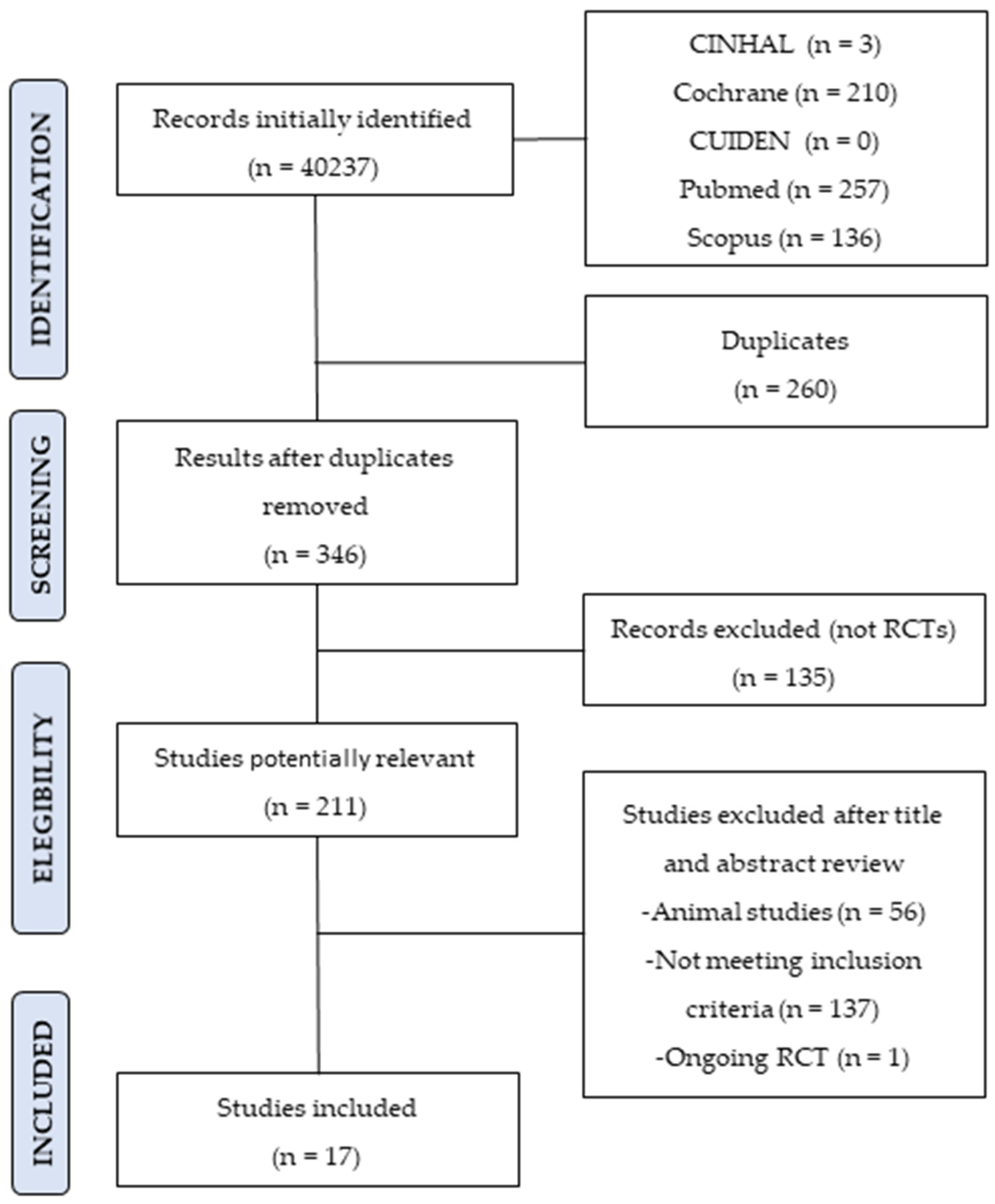
2. Materials and Methods
3. Results
4. Discussion
4.1. Therapeutic Hypothermia in Adults
4.2. Targeted Temperature Management
4.2.1. Adverse Events
4.2.2. Prognostic Factors
4.2.3. Quality of Life in CA Patients
4.3. Targeted Hypothermia in Out-of-Hospital CA Patients
4.3.1. Maintenance Phase
4.3.2. Internal and External Cooling Devices
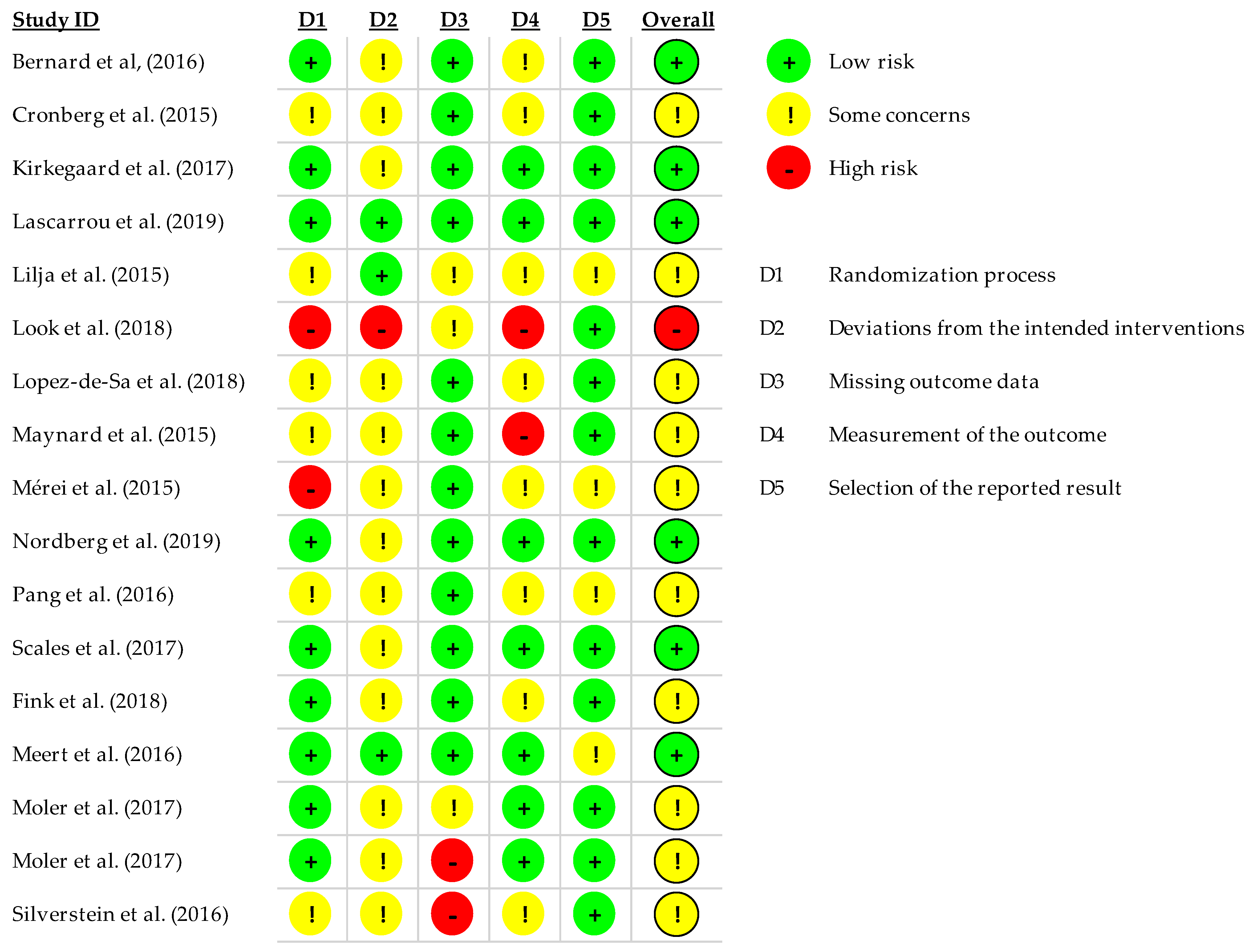
4.3.3. Risk of Bias
4.4. Hypothermia in Pediatric Patients
4.4.1. Targeted Temperature Management (TTM)
4.4.2. Adverse Events
4.4.3. Maintenance Phase Duration
4.4.4. Risk of Bias
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jacobs, I.; Nadkarni, V.; Bahr, J.; Berg, R.A.; Billi, J.E.; Bossaert, L.; Cassan, P.; Coovadia, A.; D’Este, K.; Finn, J.; et al. Cardiac arrest and cardiopulmonary resuscitation outcome reports: Update and simplification of the Utstein templates for resuscitation registries. A statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council. Circulation 2004, 110, 3385–3397. [Google Scholar] [PubMed]
- Berdowskki, J.; Berg, R.A.; Tijssen, J.G.P.; Koster, R.W. Global Incidences of out-of-Hospital Cardiac Arrest and Survival Rates: Systematic Review of 67 Prospective Studies|Elsevier Enhanced Reader. Available online: https://reader.elsevier.com/reader/sd/pii/S0300957210004326?token=D23166ACD16312FBB6319D95402CC4CF28F3350CE5A3CC5791E8B26FEC2E2A58829847F3BAC5070BF5B802BC0223F146 (accessed on 5 September 2020).
- Porzer, M.; Mrazkova, E.; Homza, M.; Janout, V. Out-of-hospital cardiac arrest. Biomed. Pap. 2017, 161, 348–353. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luc, G.; Baert, V.; Escutnaire, J.; Genin, M.; Vilhelm, C.; Di Pompéo, C.; El Khoury, C.; Segal, N.; Wiel, E.; Adnet, F.; et al. Epidemiology of out-of-hospital cardiac arrest: A French national incidence and mid-term survival rate study. Anaesth. Crit. Care Pain Med. 2019, 38, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Nolan, J.P.; Neumar, R.W.; Adrie, C.; Aibiki, M.; Berg, R.A.; Böttiger, B.W.; Callaway, C.; Clark, R.S.B.; Geocadin, R.G.; Jauch, E.C.; et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia the Council on Cardiopulmonary, Perioperative, and Critical Care the Council on Clinical Cardiology. Resuscitation 2008, 79, 350–379. [Google Scholar] [CrossRef] [PubMed]
- Girotra, S.; Chan, P.S.; Bradley, S.M. Post-resuscitation care following out-of-hospital and in-hospital cardiac arrest. Heart 2015, 101, 1943–1949. [Google Scholar] [CrossRef] [Green Version]
- Callaway, C.W.; Soar, J.; Aibiki, M.; Böttiger, B.W.; Brooks, S.C.; Deakin, C.D.; Donnino, M.W.; Drajer, S.; Kloeck, W.; Morley, P.T.; et al. Part 4: Advanced life support: 2015 International consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation 2015, 132, S84–S145. [Google Scholar] [CrossRef] [PubMed]
- Laver, S.; Farrow, C.; Turner, D.; Nolan, J. Mode of death after admission to an intensive care unit following cardiac arrest. Intensive Care Med. 2004, 30, 2126–2128. [Google Scholar] [CrossRef]
- Jennett, B.; Bond, M. Assessment of outcome after severe brain damage. A practical scale. Lancet 1975, 305, 480–484. [Google Scholar] [CrossRef]
- Holzer, M. Targeted temperature management for comatose survivors of cardiac arrest. N. Engl. J. Med. 2010, 363, 1256–1264. [Google Scholar] [CrossRef] [Green Version]
- Madl, C.; Holzer, M. Brain function after resuscitation from cardiac arrest. Curr. Opin. Crit. Care 2004, 10, 213–217. [Google Scholar] [CrossRef]
- Lázaro Paradinas, L. Conocimiento enfermero sobre hipotermia inducida tras parada cardiorrespiratoria: Revisión bibliográfica. Enferm. Intensiva 2012, 23, 17–31. [Google Scholar] [CrossRef] [PubMed]
- McCullough, J.N.; Zhang, N.; Reich, D.L.; Juvonen, T.S.; Klein, J.J.; Spielvogel, D.; Ergin, M.A.; Griepp, R.B. Cerebral metabolic suppression during hypothermic circulatory arrest in humans. Ann. Thorac. Surg. 1999, 67, 1895–1899. [Google Scholar] [CrossRef]
- Webster, C.M.; Kelly, S.; Koike, M.A.; Chock, V.Y.; Giffard, R.G.; Yenari, M.A. Inflammation and NFκB activation is decreased by hypothermia following global cerebral ischemia. Neurobiol. Dis. 2009, 33, 301–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alzaga, A.G.; Cerdan, M.; Varon, J. Therapeutic hypothermia. Resuscitation 2006, 70, 369–380. [Google Scholar] [CrossRef] [PubMed]
- Seder, D.B.; Jarrah, S. Therapeutic Hypothermia for Cardiac Arrest: A Practical Approach. Curr. Neurol. Neurosci. Rep. 2008, 8, 508–517. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Bernard, S.A.; Smith, K.; Finn, J.; Hein, C.; Grantham, H.; Bray, J.E.; Deasy, C.; Stephenson, M.; Williams, T.A.; Straney, L.D.; et al. Induction of Therapeutic Hypothermia during Out-of-Hospital Cardiac Arrest Using a Rapid Infusion of Cold Saline: The RINSE Trial (Rapid Infusion of Cold Normal Saline). Circulation 2016, 134, 797–805. [Google Scholar] [CrossRef]
- Scales, D.C.; Cheskes, S.; Verbeek, P.R.; Pinto, R.; Austin, D.; Brooks, S.C.; Dainty, K.N.; Goncharenko, K.; Mamdani, M.; Thorpe, K.E.; et al. Prehospital cooling to improve successful targeted temperature management after cardiac arrest: A randomized controlled trial. Resuscitation 2017, 121, 187–194. [Google Scholar] [CrossRef] [Green Version]
- Meert, K.; Telford, R.; Holubkov, R.; Slomine, B.S.; Christensen, J.R.; Dean, J.M.; Moler, F.W. Exploring the safety and efficacy of targeted temperature management amongst infants with out-of-hospital cardiac arrest due to apparent life threatening events. Resuscitation 2016, 109, 40–48. [Google Scholar] [CrossRef] [Green Version]
- Lascarrou, J.B.; Merdji, H.; Le Gouge, A.; Colin, G.; Grillet, G.; Girardie, P.; Coupez, E.; Dequin, P.F.; Cariou, A.; Boulain, T.; et al. Targeted temperature management for cardiac arrest with nonshockable rhythm. N. Engl. J. Med. 2019, 381, 2327–2337. [Google Scholar] [CrossRef]
- Lopez-de-Sa, E.; Juarez, M.; Armada, E.; Sanchez-Salado, J.C.; Sanchez, P.L.; Loma-Osorio, P.; Sionis, A.; Monedero, M.C.; Martinez-Sellés, M.; Martín-Benitez, J.C.; et al. A multicentre randomized pilot trial on the effectiveness of different levels of cooling in comatose survivors of out-of-hospital cardiac arrest: The FROST-I trial. Intensive Care Med. 2018, 44, 1807–1815. [Google Scholar] [CrossRef] [PubMed]
- Nordberg, P.; Taccone, F.S.; Truhlar, A.; Forsberg, S.; Hollenberg, J.; Jonsson, M.; Cuny, J.; Goldstein, P.; Vermeersch, N.; Higuet, A.; et al. Effect of Trans-Nasal Evaporative Intra-arrest Cooling on Functional Neurologic Outcome in Out-of-Hospital Cardiac Arrest: The PRINCESS Randomized Clinical Trial. JAMA 2019, 321, 1677–1685. [Google Scholar] [CrossRef]
- Cronberg, T.; Lilja, G.; Horn, J.; Kjaergaard, J.; Wise, M.P.; Pellis, T.; Hovdenes, J.; Gasche, Y.; Åneman, A.; Stammet, P.; et al. Neurologic Function and Health-Related Quality of Life in Patients Following Targeted Temperature Management at 33°C vs. 36°C After Out-of-Hospital Cardiac Arrest. JAMA Neurol. 2015, 72, 634–641. [Google Scholar] [CrossRef]
- Kirkegaard, H.; Søreide, E.; De Haas, I.; Pettilä, V.; Taccone, F.S.; Arus, U.; Storm, C.; Hassager, C.; Nielsen, J.F.; Sørensen, C.A.; et al. Targeted temperature management for 48 vs. 24 hours and neurologic outcome after out-of-hospital cardiac arrest: A randomized clinical trial. JAMA—J. Am. Med. Assoc. 2017, 318, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Lilja, G.; Nielsen, N.; Friberg, H.; Horn, J.; Kjaergaard, J.; Nilsson, F.; Pellis, T.; Wetterslev, J.; Wise, M.P.; Bosch, F.; et al. Cognitive Function in survivors of out-of-hospital cardiac arrest after target temperature management at 33 °C Versus 36 °C. Circulation 2015, 131, 1340–1349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pang, P.Y.K.; Wee, G.H.L.; Hoo, A.E.E.; Sheriff, I.M.T.; Lim, S.L.; Tan, T.E.; Loh, Y.J.; Kerk, K.L.; Sin, Y.K.; Lim, C.H. Therapeutic hypothermia in adult patients receiving extracorporeal life support: Early results of a randomized controlled study. J. Cardiothorac. Surg. 2016, 11, 43. [Google Scholar] [CrossRef] [Green Version]
- Fink, E.L.; Clark, R.S.B.; Berger, R.P.; Fabio, A.; Angus, D.C.; Watson, R.S.; Gianakas, J.J.; Panigrahy, A.; Callaway, C.W.; Bell, M.J.; et al. 24 vs. 72 hours of hypothermia for pediatric cardiac arrest: A pilot, randomized controlled trial. Resuscitation 2018, 126, 14–20. [Google Scholar] [CrossRef]
- Maynard, C.; Longstreth, W.T.; Nichol, G.; Hallstrom, A.; Kudenchuk, P.J.; Rea, T.; Copass, M.K.; Carlbom, D.; Deem, S.; Olsufka, M.; et al. Effect of prehospital induction of mild hypothermia on 3-month neurological status and 1-year survival among adults with cardiac arrest: Long-term follow-up of a randomized, clinical trial. J. Am. Heart Assoc. 2015, 4, e001693. [Google Scholar] [CrossRef] [Green Version]
- Moler, F.W.; Silverstein, F.S.; Holubkov, R.; Slomine, B.S.; Christensen, J.R.; Nadkarni, V.M.; Meert, K.L.; Clark, A.E.; Browning, B.; Pemberton, V.L.; et al. Therapeutic hypothermia after out-of-hospital cardiac arrest in children. N. Engl. J. Med. 2015, 372, 1898–1908. [Google Scholar] [CrossRef]
- Moler, F.W.; Silverstein, F.S.; Holubkov, R.; Slomine, B.S.; Christensen, J.R.; Nadkarni, V.M.; Meert, K.L.; Clark, A.E.; Browning, B.; Pemberton, V.L.; et al. Therapeutic hypothermia after in-hospital cardiac arrest in children. Supplementary appendix. N. Engl. J. Med. 2017, 376, 318–329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silverstein, F.S.; Slomine, B.S.; Christensen, J.; Holubkov, R.; Page, K.; Dean, J.M.; Moler, F.W. Functional Outcome Trajectories after Out-of-Hospital Pediatric Cardiac Arrest. Crit. Care Med. 2016, 44, e1165–e1174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Look, X.; Li, H.; Ng, M.; Lim, E.T.S.; Pothiawala, S.; Tan, K.B.K.; Sewa, D.W.; Shahidah, N.; Pek, P.P.; Ong, M.E.H. Randomized controlled trial of internal and external targeted temperature management methods in post- cardiac arrest patients. Am. J. Emerg. Med. 2018, 36, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Mérei, Á.; Nagy, B.J.; Woth, G.L.; Zsidó, N.; Lantos, J.; Mühl, D. Effects of therapeutic hypothermia and kinetics of serum protein S100B after cardiopulmonary resuscitation. Signa Vitae—A J. Intensive Care Emerg. Med. 2015, 10, 109–130. [Google Scholar] [CrossRef]
- Meaney, P.A.; Nadkarni, V.M.; Kern, K.B.; Indik, J.H.; Halperin, H.R.; Berg, R.A. Rhythms and outcomes of adult in-hospital cardiac arrest. Crit. Care Med. 2010, 38, 101–108. [Google Scholar] [CrossRef] [PubMed]
- Eisenberg, M.S.; Hallstrom, A.P.; Copass, M.K.; Bergner, L.; Short, F.; Pierce, J. Treatment of Ventricular Fibrillation: Emergency Medical Technician Defibrillation and Paramedic Services. JAMA J. Am. Med. Assoc. 1984, 251, 1723–1726. [Google Scholar] [CrossRef] [Green Version]
- Lopez-De-Sa, E.; Rey, J.R.; Armada, E.; Salinas, P.; Viana-Tejedor, A.; Espinosa-Garcia, S.; Martinez-Moreno, M.; Corral, E.; Lopez-Sendon, J. Hypothermia in comatose survivors from out-of-hospital cardiac arrest: Pilot trial comparing 2 levels of target temperature. Circulation 2012, 126, 2826–2833. [Google Scholar] [CrossRef]
- Stær-Jensen, H.; Sunde, K.; Olasveengen, T.M.; Jacobsen, D.; Drægni, T.; Nakstad, E.R.; Eritsland, J.; Andersen, G.Ø. Bradycardia during therapeutic hypothermia is associated with good neurologic outcome in comatose survivors of out-of-hospital cardiac arrest. Crit. Care Med. 2014, 42, 2401–2408. [Google Scholar] [CrossRef]
- Yu, T.; Barbut, D.; Ristagno, G.; Cho, J.H.; Sun, S.; Li, Y.; Weil, M.H.; Tang, W. Survival and neurological outcomes after nasopharyngeal cooling or peripheral vein cold saline infusion initiated during cardiopulmonary resuscitation in a porcine model of prolonged cardiac arrest. Crit. Care Med. 2010, 38, 916–921. [Google Scholar] [CrossRef]
- Garrett, J.S.; Studnek, J.R.; Blackwell, T.; Vandeventer, S.; Pearson, D.A.; Heffner, A.C.; Reades, R. The association between intra-arrest therapeutic hypothermia and return of spontaneous circulation among individuals experiencing out of hospital cardiac arrest. Resuscitation 2011, 82, 21–25. [Google Scholar] [CrossRef]
- Bernard, S.A.; Gray, T.W.; Buist, M.D.; Jones, B.M.; Silvester, W.; Gutteridge, G.; Smith, K. Treatment of Comatose Survivors of Out-of-Hospital Cardiac Arrest with Induced Hypothermia. N. Engl. J. Med. 2002, 346, 557–563. [Google Scholar] [CrossRef] [PubMed]
- Hypothermia after Cardiac Arrest Study Group. Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N. Engl. J. Med. 2002, 346, 549–556. [Google Scholar] [CrossRef] [PubMed]
- Kagawa, E.; Dote, K.; Kato, M.; Sasaki, S.; Oda, N.; Nakano, Y.; Miura, K.; Inoue, I.; Kihara, Y. Do Lower Target Temperatures or Prolonged Cooling Provide Improved Outcomes for Comatose Survivors of Cardiac Arrest Treated with Hypothermia? J. Am. Heart Assoc. 2015, 4, e002123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tømte, Ø.; Drægni, T.; Mangschau, A.; Jacobsen, D.; Auestad, B.; Sunde, K. A comparison of intravascular and surface cooling techniques in comatose cardiac arrest survivors. Crit. Care Med. 2011, 39, 443–449. [Google Scholar] [CrossRef] [PubMed]
- Pittl, U.; Schratter, A.; Desch, S.; Diosteanu, R.; Lehmann, D.; Demmin, K.; Hörig, J.; Schuler, G.; Klemm, T.; Mende, M.; et al. Invasive versus non-invasive cooling after in- and out-of-hospital cardiac arrest: A randomized trial. Clin. Res. Cardiol. 2013, 102, 607–614. [Google Scholar] [CrossRef]
- Nielsen, N.; Wetterslev, J.; Cronberg, T.; Erlinge, D.; Gasche, Y.; Hassager, C.; Horn, J.; Hovdenes, J.; Kjaergaard, J.; Kuiper, M.; et al. Targeted temperature management at 33 °C vs. 36 °C after cardiac arrest. N. Engl. J. Med. 2013, 369, 2197–2206. [Google Scholar] [CrossRef] [Green Version]
- Bray, J.E.; Stub, D.; Bloom, J.E.; Segan, L.; Mitra, B.; Smith, K.; Finn, J.; Bernard, S. Changing target temperature from 33 °C to 36 °C in the ICU management of out-of-hospital cardiac arrest: A before and after study. Resuscitation 2017, 113, 39–43. [Google Scholar] [CrossRef]
- Rittenberger, J.C.; Raina, K.; Holm, M.B.; Kim, Y.J.; Callaway, C.W. Association between Cerebral Performance Category, Modified Rankin Scale, and discharge disposition after cardiac arrest. Resuscitation 2011, 82, 1036–1040. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Author (Year) | N | Baseline Characteristics | Cooling System | Mean Time Reaching Target Temperature | Target Temperature | Inclusion Criteria | Exclusion Criteria | Time of Evaluating Survival | Time of Evaluating Neurological Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Bernard et al. (2016) [19] | 1198 | ≥18 years, IV access, and were still in CA after CPR | Rapid IV infusion of large-volume (30 mL/kg), cold saline vs. Standard Care | 22.6 ± 11.5 vs. 20.0 ± 10.6 min | 33 °C in the ICU | ≥18 years of age, in cardiac arrest, had IV access established, and still in CA result of trauma (including hanging), suspected of intracranial bleeding | Pregnant women, to be already hypothermic (<34.5 °C), or inpatients in a hospital and documenting limitations in resuscitation. | Hospital discharge | Serum neuron-specific enolase concentration at 24 h |
| Cronberg et al. (2015) [25] | 939 | Unconscious (GCS < 8) | Ice-cold fluids, ice-packs, and intravascular or surface T° management devices at the discretion of the site. | 20 (15–27) vs. 20 (14–30) min | 33 °C | ≥18 years of age, OHCA of cardiac cause with ROSC | ROSC > 240 min, CA with asystole as the initial rhythm, acute intracranial hemorrhage or stroke, and T° < 30°C | 6 months | 6 months |
| Kirkegaard et al. (2017) [26] | 355 | OHCA of cardiac origin | Invasive cooling with intravascular catheter | 48-h group: 281 (IQR, 217–360) vs. 24-h group: 320 (IQR 241–410) min (p = 0.01) | 33 °C | 17–80 years, ROSC > 20 min, GCS > 8, shockable and non shockable rhythms | Patients with unwitnessed asystole | 6 months | 6-months (CPC) |
| Lascarrou et al. (2019) [22] | 584 | Iintrahospitalary: 27.4%; OHCA: 72.6%; non-cardiac cause: 66%; circulatory shock: 58% | NR | NR | 33 °C ± 0.5 °C for 24 h | >18 years, resuscitated from OHCA with a non shockable rhythm, GCS > 8 | Low-flow > 60 min; hemodynamic instability, CA > 300 min, moribund condition, cirrhosis, pregnancy, previous inclusion in RCT, no health insurance | 3 months | 3 months (CPC) |
| Lilja et al. (2015) [27] | 652 | Unconscious, ≥18 years, OHCA of cardiac origin, Controls were patients with STEMI with percutaneous coronary intervention | 4 °C intravenous solutions, ice-packs, and cooling devices | 20 (15–30) 21 (13–30) min | 33 °C for 24 h | >18 years, OHCA of cardiac cause, unconsciousness after ROSC | Bleeding diathesis, acute intracranial bleeding, stroke, asystole, therapy limitations and Do Not Resuscitate order, CPC = 3 or 4, T° < 30 °C, SBP < 80 mmHg | 3 months | 3 months |
| Look et al. (2018) [34] | 87 | Controls: 42.9% initial rhythm, 33.3% PEA, 9.5% VF/VT. TTM: initial rhythm: 26.1% vs. 36.4% for asystole, 34.8% vs. 31.8% for PEA, 13.0% vs. 9.1% for VF/VT | External cooling: four water-circulating gel-coated energy transfer pads placed on the patient’s back, abdomen, and both thighs. Surface area ranges: 0.60–0.77 m2 connected to an automatic thermostat | Median time in minutes to first ROSC (Mean, IQR) Control 24.0 (13.5, 42.0), Intervention external 25.0 (15.3, 39.3), internal 26.0 (12.3, 40.3) min | 34 °C, after which, they were maintained at that temperature for 24 h before rewarming passively at 1 °C every 4 h (0.25 °C/h) to 36.5 °C | Sustained ROSC after CA for >30 min, Age: 18–80 years, hemodynamically stable, SBP > 90 mmHg | Comatose or unresponsive post-resuscitation, hypotension, pregnancy, premorbid status, bedbound and uncommunicative | Hospital discharge | Hospital discharge |
| Lopez-de-Sa et al. (2018) [23] | 150 | AED differed among groups: 32 °C group: 13.5% vs. 33 °C group: 34.7% vs. 34 °C group: 28.6%, (p = 0.03), Invasive coronary angiography: 61.5% vs. 81.6% vs. 73.5% (p = 0.08). | NR | 32 °C 28.9 ± 15.9, 33 °C 26.3 ± 14.1, 34 °C 25.7 ± 11.6 min | 32 °C, 33 °C, 34 °C | Signed consent, 18–80 years old, OHCA of cardiac cause, sustained ROSC, initial shockable cardiac rhythm, lack of meaningful response at arrival to hospital, non-traumatic CA, SBP > 90 Hgmm for 30 min post-ROSC | Traumatic/toxicological CA, pregnancy, Do Not Resuscitate order, femoral venous access contraindication, neuromuscular blocking agents prior to assesment, incomplete neurological evaluation, T° < 34 °C, current IVC filter, neurological illness, functional disabilities, intracranial bleeding, acute stroke, terminal illness, other RCT | 3 months | 3 months |
| Maynard et al. (2015) [30] | 508 | 37% were discharged alive from the hospital, 58% had CPC = 1 or 2, 50% had MRS: slight disability or better | Rapid infusion of 2 L of 4 oC normal saline, Drug: Rapid infusion of cold normal saline | NR | 33 °C vs. 36 °C | Successful resuscitation from OHCA (palpable pulse) | Traumatic cause | 12 months | Hospital discharge (CPC) |
| Mérei et al. (2015) [35] | 57 | 33% female, mean age: 62 years, CPR: 14.5 min, TH: 38% | 2 L of intravascular saline at 4 °C vs. standard care and additional external cooling (cooler blocks over great blood vessels) | NR | 33 °C vs. 36 °C for 24 h | Patients treated on the ICU of University of Pécs between June 2009–February 2012 after CPR, ROSC | NR | NR | 1 month |
| Nordberg et al. (2019) [24] | 677 | Median time: 25 min after ROSC, median T°: intervention group: 34.6 °C vs. control group 35.8 °C (p < 0.001) | Mixture of air or oxygen and a liquid coolant via nasal catheters | Intervention group: 105 vs. 182 min in the control group (p < 0.001) | 33 ± 1 °C | Witnessed CA, 18–80 years | Trauma cause, bleeding, drug overdose, cerebrovascular accident, drowning, smoke inhalation, electrocution, hanging, hypothermic, nasal anatomic barrier, Do Not Resuscitate order, terminal disease, pregnancy, coagulopathy, supplemental oxygen, EMS > 15 min | 3 months | 3 months (CPC 1 or 2) |
| Pang et al. (2016) [28] | 21 | Ventricular tachycardia/ventricular fibrillation: 33.3%, pulseless: 47.6%, asystole: 19.0%, CPR and ECLS duration: 25.7 min and 4.4 days | ECLS via percutaneous cannulation of the common femoral artery. Extracorporeal centrifugal pump, oxygenator and heat exchanger | NR | 34 °C for 24 h | ≥21 years, CA with ECLS, Ventricular fibrillation, Downtime <45 min, Comatose patients, Patients not responding to verbal after ROSC, ACLS < 60 min, mechanical ventilation | Responding to verbal commands after ROSC, CPR > 45 min, coagulopathy, pregnancy, premorbid status, uncommunicative, T° < 30 °C | 6 months, | Hospital discharge (CPC) of 1–2 |
| Scales et al. (2017) [20] | 585 | OHCA patients | Cold saline and ice packs applied to neck, axillae, and both groins and infusion of up to 2 L of cold saline at 4 °C | Median (IQR) cooling group 5.4 h (3.0–8.2) vs. control 4.8 h (2.8–7.7) (p = 0.45) | 32–34 °C for 6 h | EMS-treated OHCA, age ≥18 years, ROSC of ≥5 min, SBP ≥ 100 mmHg, unresponsive to verbal stimuli, endotracheal intubation | Trauma, burn, or exposure HT, bleeding, sepsis, coagulopathy, Do Not Resuscitate order, pregnancy, or prisoner status | Hospital discharge | Hospital discharge |
| Author (Year) | N | Baseline Characteristics | Cooling System | Mean Time Reaching Target Temperature | Target Temperature | Inclusion Criteria | Exclusion Criteria | Time of Evaluating Survival | Time of Evaluating Neurological Outcome |
|---|---|---|---|---|---|---|---|---|---|
| Fink et al. (2018) [29] | 34 | 88% asphyxia, 82% OHCA, CPR duration: 20 (11.5, 30.0) min | Cooling blanket, cold saline infusion, cold packs, room T° regulation, and tepid bath | 30 (27–33) (30.8 ± 5.0) h and 78 (75–79) (76.6 ± 24.1) h for the 24 and 72 h groups, respectively | 33 ± 1°C | Arterial or venous catheter, GCS ≤ 8, HT initiated | Do Not Resuscitate status, pregnancy, contraindication for MRI, acute brain disease, brain death evaluation, metabolic disease affecting brain, active hemorrhage, coagulation defect | 6 months | Neuron-specific enolase on day 7 (post-rewarming) |
| Meert et al. (2016) [21] | 54 | 48 h-18 years, OHCA with CPR ≥ 2 min, required mechanical ventilation after ROSC | Surface cooling using a Blanketrol III cooling unit | Median (Q1, Q3) HT Group 5.8 (5.3, 6.3), Normothermia Group 6.1 (5.3, 7.0) (hours) | 33 °C for 48 h | <1 year at OHCA and ALTE as the aetiology of arrest | Inability to be randomised within six hours of return of circulation, GCS = 5 or 6.21, aggressive treatment, trauma cause CA. | 28 days | 12 months (VABS-II) |
| Moler et al. (2015) [31] | 295 | Ventricular fibrillation or ventricular tachycardia: 8% | Pharmacological HT (paralyzed and sedated), Blanketrol III temperature management unit (blankets applied anteriorly and posteriorly) | HT group: 5.9 h (IQR: 5.2–6.7) vs. normothermia group: 5.8 h (IQR: 5.0–6.4) | 33.0 °C (32.0–34.0) for 48 h | 48 h, 18 years of age, CA with CPR = 2 min and mechanical ventilation after ROSC | Inability to randomization within 6 h after ROSC, GCS motor-response subscale: 5 or 6 | 12 months | 12 months (VABS-II) |
| Moler et al. (2017) [32] | 329 | Median age: 1 year, 60% male, 91% preexisting medical condition, 57% bradycardia, 10% fibrillation or ventricular tachycardia, 93% hospital CA | Blanketrol III temperature-management unit applied anteriorly and posteriorly | CPR median duration 22.0 min (IQR 7.0–47.0) | 33.0 °C (32.0–34.0) for 48 h | 48 h, 18 years of age CA in a hospital, RCP > 2 min with mechanical ventilation after ROSC | GCS motor-response subscale = 5 or 6, inability to randomization 6 h after ROSC, bleeding, a preexisting illness, life expectancy <12 months, aggressive treatment | 12 months | 12 months (VABS-II) |
| Silverstein et al. (2016) [33] | 295 | CA etiology: respiratory (66%), initial EKG rhythm: asystole (66%), bradycardia (34%), pulseless electrical activity (36%) | Blanketrol III temperature-management unit applied anteriorly and posteriorly | NR | 33 °C ± 1 °C for 48 h | CPR >2 min with ROSC, 48 h, 18 years, continuous mechanical ventilation requirement unplanned CA | Speaking barriers, ECMO when CA ≥2 ug/kg/minute infusion of epinephrine or norepinephrine, GCS = 5–6, prior CA with CPR > 2 min, life expectancy < 12 months, Do Not Resuscitate order | 1 year | 12 months (VABS-II score ≥70) |
| Author (Year) | N | Aim | Intervention | Results |
|---|---|---|---|---|
| Bernard et al. (2016) [19] | 1198 | To measure survival rate at hospital discharge and time to return to a spontaneous circulation after CA | CPR + TTM vs. CPR + 2 L of cold saline perfusion during an out-of-hospital CRP | TTM during CPR has no effect on survival rate and may decrease spontaneous circulation recovery in patients with shockable rhythms |
| Cronberg et al. (2015) [25] | 939 | To evaluate the effects of TTM on survival rate, cognitive status, functionality, and quality of life | TTM at 33–36 °C. CPC, mRS, MMSE, ALFI, IQCODE, and SF-36 scales were measured at 6 months of follow-up in CA survivors | Survival rate and quality of life were similar in both groups |
| Kirkegaard et al. (2017) [26] | 355 | To evaluate effectiveness of 48 and 24 h of TTM | 48 h of TTM at 33 °C vs. 24 h of TTM at 33 °C + 0.5 °C per hour rewarming | There were no differences in mortality between groups. Patients in 48 h of TTM group showed more adverse events |
| Lascarrou et al. (2019) [22] | 584 | To measure the effectiveness of TTM in patients in a non-shockable rhythm | Patients were assigned to 33 °C TTM for 24 h vs. normothermia treatment at 37 °C | TTM group patients showed higher survival and better neurological status rates than the normothermia group |
| Lilja et al. (2015) [27] | 652 | To assess 6-month neurological status in patients who received TTM at 33–36 °C [19] compared to MINOCA patients. | RBMT-3, FAB, Symbols and Digits Test, and HADS scales were used to compare neurological status between groups. | Cognitive function was comparable in CA survivors and MINOCA groups |
| Look et al. (2018) [34] | 87 | To analyze survival rate after hospital discharge and neurological status in survivors of CA after undergoing intravascular and surface cooling devices for TTM. | Patients were randomized to intravascular and surface cooling devices for TTM or to non- therapeutic hypothermia treatment. | Intravascular TTM showed more accurate temperature control, and non-significant higher rates of survival were found in comparison with surface cooling. |
| Lopez-de-Sa et al. (2018) [23] | 150 | To compare the effect of different temperatures of TTM on neurological status in out-of-hospital CA | Comatose patients underwent to TTM of 32 °C, 33 °C, and 34 °C for 24 h. | There was no significant impact on neurological status and survival rate. |
| Maynard et al. (2015) [30] | 508 | Effect of prehospital induction of mild hypothermia on 3-month neurological status and 1-year survival among out-of-hospital CA treated with out-of-hospital TTM. | Cerebral Performance Category (CPC) and Modified Rankin Scale (mRS) were measured by telephone call to compare neurological status between patients treated with out-of-hospital TTM (2 L of intravascular saline at 4 °C after CPR) vs. standard care after resuscitation from CA. | TTM showed no improvement on the neurological status and survival rate. |
| Mérei et al. (2015) [35] | 57 | To evaluate 30-day survival, TTM efficacy and serum levels of S100B protein as a prognostic biomarker. | Blood samples of 20 CA patients randomly selected from TTM of 32–34 °C and standard care groups were taken at admission and after 12 and 36 h after recovery to measure S100B levels. | TTM showed no improvement on survival and S100B serum levels. |
| Nordberg et al. (2019) [24] | 677 | To determine whether prehospital trans-nasal evaporative intra-arrest cooling improves survival with good neurologic outcomes compared with cooling initiated after hospital arrival. | Patients were randomly assigned to receive trans-nasal evaporative intra-arrest cooling or standard care. Both groups received TTM at 32 °C to 34 °C for 24 h. | Trans-nasal evaporative intra-arrest cooling did not result in a statistically significant improvement in survival with good neurologic outcome, however, those patients reached target T° earlier. |
| Pang et al. (2016) [28] | 21 | To evaluate safety and efficacy of TTM in patients undergoing ECLS after CA. | Comparison of a control group of patients with ECLS treated with normothermia (37 °C) vs. TTM at 34 °C for 24 h. | TTM can be applied safely in ECLS patients. No significant differences were found in terms of survival or neurological status. |
| Scales et al. (2017) [20] | 585 | To evaluate if pre-hospital cooling (target temperature of 32–34 °C within 6 h of hospital arrival) leads to higher rates of successful TTM. | Patients were randomized to receive prehospital cooling (initiated 5 min after ROSC) or usual resuscitation and transport. Both groups received TTM in the critical care unit. | Prehospital cooling after ROSC did not increase rates of achieving a target temperature of 32–34 °C within 6 h of hospital arrival, but it was safe and increased application of TTM in hospital. |
| Author (Year) | N | Aim | Intervention | Results |
|---|---|---|---|---|
| Fink et al. (2018) [29] | 34 | To measure effect of TTM at 33 °C in pediatric patients for 24 h vs. 72 h on 6-month mortality and different biomarkers. | Children with CA were randomized to TH for 24 or 72 h. Serum was collected twice daily on days 1–4 and once on day 7. Mortality was assessed at 6 months. | Serum NSE and S100b protein concentration was increased in the 24 h group. Significant difference was not shown in mortality. |
| Meert et al. (2016) [21] | 54 | To explore the safety and efficacy of TTM amongst infants with out-of-hospital CA. | Patients were allocated to TTM at 33 °C or at 36.8 °C (normothermia) for 48 h within six hours of return of circulation. 12-month survival was measured though VABS-II scale. | No differences in survival rates or neurologic status were found between groups. |
| Moler et al. (2015) [31] | 295 | To assess TH efficacy on survival and functional outcome in out-of-hospital CA pediatric patients. | TH at 33.0 °C was compared to therapeutic normothermia at 36.8 °C. One-year survival with a good neurobehavioral was estimated thought the VABS-II scale. | Survival at 12 months did not differ significantly between groups. |
| Moler et al. (2017) [32] | 329 | To assess TH efficacy on survival and functional outcome in out-of-hospital CA pediatric patients. | TH at 33.0 °C was compared to therapeutic normothermia at 36.8 °C. One-year survival with a functional outcome was estimated through the VABS-II scale. | Trial was stopped because of assessment of futility before attainment of the target trial enrollment. |
| Silverstein et al. (2016) [33] | 295 | To assess functionality in out-of-hospital CA pediatric patients. | TH at 33 °C was compared to normothermia at 36.8 °C. Functionality was measured though VABS-II, PCPC, and POPC scales. | No differences were found between the groups in terms of functional status. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Colls Garrido, C.; Riquelme Gallego, B.; Sánchez García, J.C.; Cortés Martín, J.; Montiel Troya, M.; Rodríguez Blanque, R. The Effect of Therapeutic Hypothermia after Cardiac Arrest on the Neurological Outcome and Survival—A Systematic Review of RCTs Published between 2016 and 2020. Int. J. Environ. Res. Public Health 2021, 18, 11817. https://doi.org/10.3390/ijerph182211817
Colls Garrido C, Riquelme Gallego B, Sánchez García JC, Cortés Martín J, Montiel Troya M, Rodríguez Blanque R. The Effect of Therapeutic Hypothermia after Cardiac Arrest on the Neurological Outcome and Survival—A Systematic Review of RCTs Published between 2016 and 2020. International Journal of Environmental Research and Public Health. 2021; 18(22):11817. https://doi.org/10.3390/ijerph182211817
Chicago/Turabian StyleColls Garrido, Christian, Blanca Riquelme Gallego, Juan Carlos Sánchez García, Jonathan Cortés Martín, María Montiel Troya, and Raquel Rodríguez Blanque. 2021. "The Effect of Therapeutic Hypothermia after Cardiac Arrest on the Neurological Outcome and Survival—A Systematic Review of RCTs Published between 2016 and 2020" International Journal of Environmental Research and Public Health 18, no. 22: 11817. https://doi.org/10.3390/ijerph182211817