
The Impact of the COVID-19 Pandemic on Ophthalmology Residents: A Narrative Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
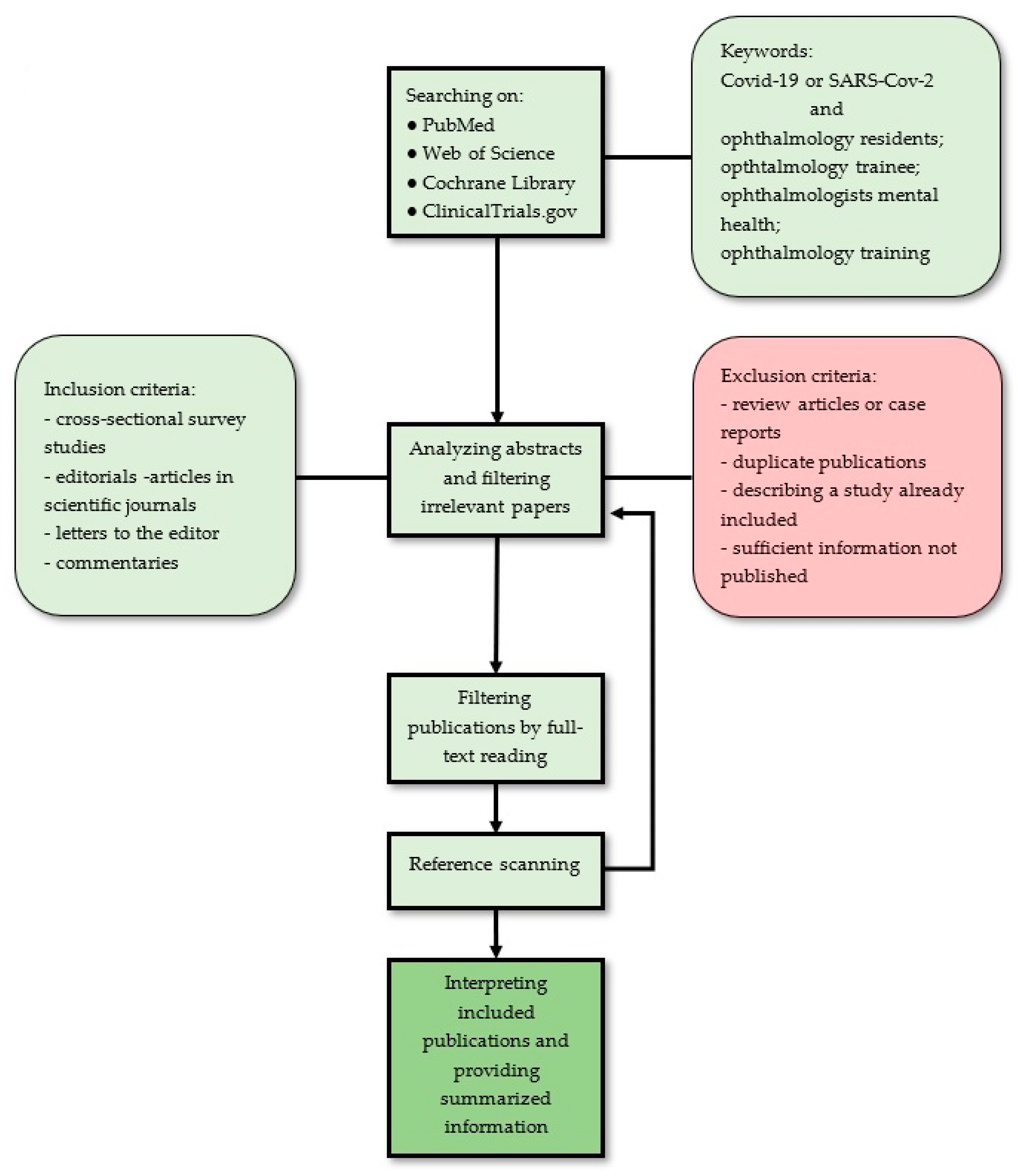
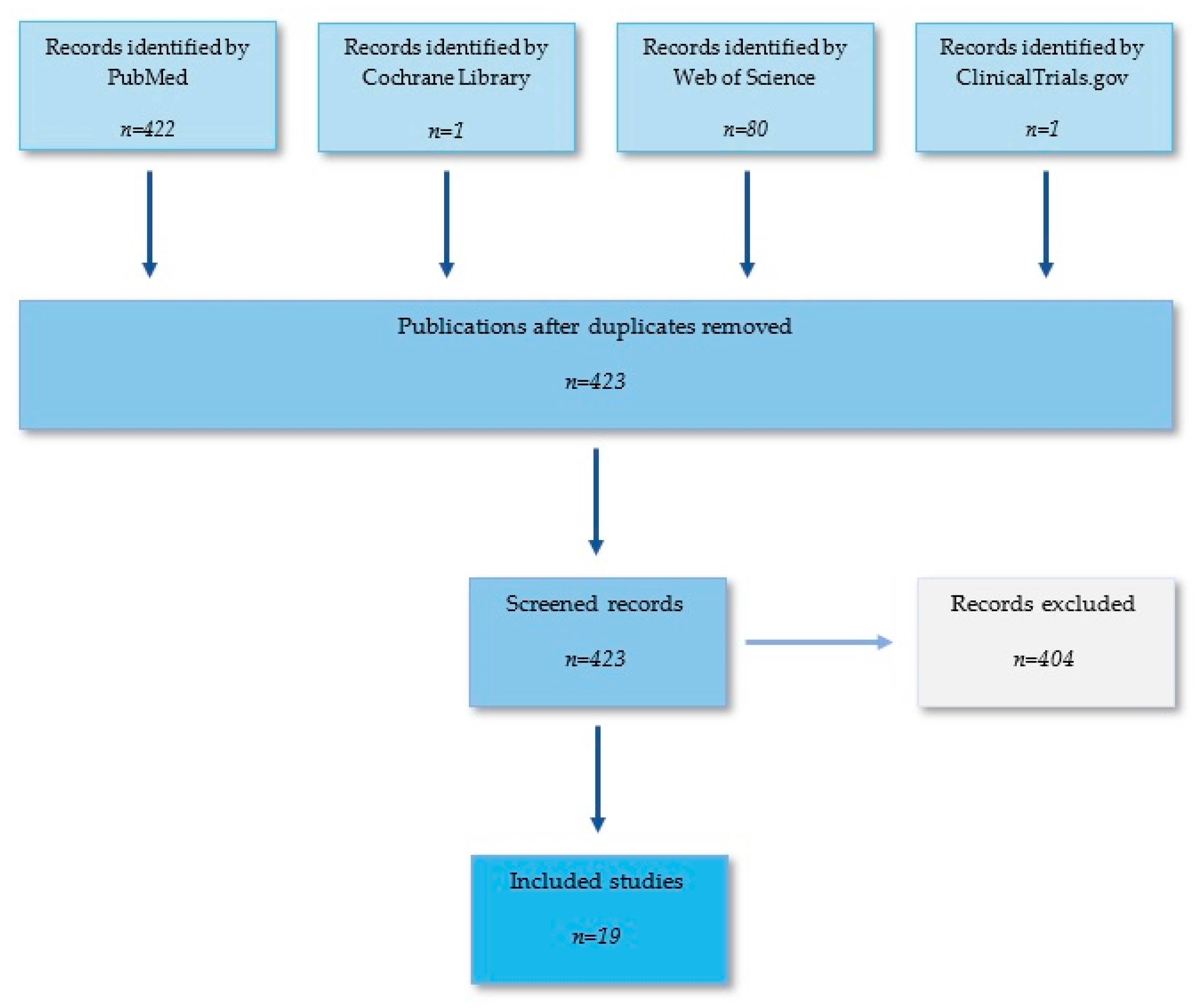
2.1. Literature Search
2.2. Study Selection
2.3. Risk of Bias Assessment
2.4. Data Extraction
3. Results
3.1. Impact on Ophthalmology Trainees’ Mental Health
3.2. Impact on Residency Training Programs
3.2.1. Research Work
3.2.2. Online Teaching Methods
3.2.3. Perspectives
4. Discussion
- Intensifying surgical skills training from the first year of training;
- Introducing virtual surgical simulators (i.e., cataract surgery simulators) to all ophthalmology departments to develop practical skills among trainees;
- Providing additional surgical training for trainees redeployed to COVID-19 units during the pandemic;
- Introducing and improving virtual forms of teaching on a large-scale, including wet labs, virtual simulators, webinars, podcasts, vodcasts, online courses, and symposia.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A novel coronavirus from patients with pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19–11 March 2020. Available online: www.who.int/dg/speeches/detail/who-director-general-s-openingremarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 12 March 2020).
- Nguyen, A.X.; Gervasio, K.A.; Wu, A.Y. Differences in SARS-CoV-2 recommendations from major ophthalmology societies worldwide. BMJ Open Ophthalmol. 2020, 5, e000525. [Google Scholar] [CrossRef]
- Dmuchowska, D.A.; Pieklarz, B.; Konopinska, J.; Mariak, Z.; Obuchowska, I. Impact of Three Waves of the COVID-19 Pandemic on the Rate of Elective Cataract Surgeries at a Tertiary Referral Center: A Polish Perspective. Int. J. Environ. Res. Public Health 2021, 18, 8608. [Google Scholar] [CrossRef] [PubMed]
- Dmuchowska, D.A.; Cwalina, I.; Krasnicki, P.; Konopinska, J.; Saeed, E.; Mariak, Z.; Obuchowska, I. The Impact of Three Waves of the COVID-19 Pandemic on the Characteristics of Primary Rhegmatogenous Retinal Detachments at a Tertiary Referral Centre. Clin. Ophthalmol. 2021, 15, 3481–3491. [Google Scholar] [CrossRef] [PubMed]
- Ferrara, M.; Romano, V.; Steel, D.H.; Gupta, R.; Iovino, C.; van Dijk, E.H.; Romano, M.R. Reshaping ophthalmology training after COVID-19 pandemic. Eye 2020, 34, 2089–2097. [Google Scholar] [CrossRef] [PubMed]
- Olivia Li, J.P.; Shantha, J.; Wong, T.Y.; Wong, E.Y.; Mehta, J.; Lin, H.; Lin, X.; Strouthidis, N.G.; Park, K.H.; Fung, A.T.; et al. Preparedness among ophthalmologists: During and beyond the COVID-19 pandemic. Ophthalmology 2020, 127, 569–572. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, S. Impact of COVID-19 pandemic on ophthalmology service provisions and training. J. Cataract. Refract. Surg. 2020, 46, 1455–1456. [Google Scholar] [CrossRef]
- Alahmadi, A.S.; Alhatlan, H.M.; Bin Helayel, H.; Khandekar, R.; Al Habash, A.; Al-Shahwan, S. Residents’ perceived impact of COVID-19 on Saudi ophthalmology training programs-a survey. Clin. Ophthalmol. 2020, 14, 3755–3761. [Google Scholar] [CrossRef] [PubMed]
- Khanna, R.C.; Honavar, S.G.; Metla, A.L.; Bhattacharya, A.; Maulik, P.K. Psychological impact of COVID-19 on ophthalmologists-in-training and practicing ophthalmologists in India. Indian J. Ophthalmol. 2020, 68, 994–998. [Google Scholar] [CrossRef]
- Almater, A.I.; Tobaigy, M.F.; Younis, A.S.; Alaqeel, M.K.; Abouammoh, M.A. Effect of 2019 Coronavirus Pandemic on Ophthalmologists Practicing in Saudi Arabia: A Psychological Health Assessment. Middle East Afr. J. Ophthalmol. 2020, 27, 79–85. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Mishra, D.; Nair, A.; Gandhi, R.; Gogate, P.J.; Mathur, S.; Bhushan, P.; Srivastav, T.; Singh, H.; Sinha, B.P.; Singh, M.K. The impact of COVID-19 related lockdown on ophthalmology training programs in India–outcomes of a survey. Indian J. Ophthalmol. 2020, 68, 999–1004. [Google Scholar] [CrossRef] [PubMed]
- Szigiato, A.A.; Palakkamanil, M.; Aubin, M.J.; Ziai, S. Canadian ophthalmology resident experience during the COVID-19 pandemic. Can. J. Ophthalmol. 2020, 56, e42–e44. [Google Scholar] [CrossRef] [PubMed]
- Kavadarlı, I.; Mutlu, M. Effects of the COVID-19 Pandemic on Turkish Ophthalmologists. Turk. J. Ophthalmol. 2021, 51, 95–101. [Google Scholar] [CrossRef] [PubMed]
- El-Saied, H.M.A.; Salah Eddin Abdelhakim, M.A. Impact of COVID-19 pandemic on young ophthalmologists in Cairo university hospitals. Semin. Ophthalmol. 2020, 35, 296–306. [Google Scholar] [CrossRef]
- Mishra, D.; Nair, A.G.; Verma, L.; Grover, A.K.; Mathur, S.; Srivastav, T. The perceived impact of webinars during the COVID.19 pandemic: A survey of ophthalmology trainees from India. Oman J. Ophthalmol. 2021, 14, 78–84. [Google Scholar] [CrossRef] [PubMed]
- Hussain, R.; Singh, B.; Shah, N.; Jain, S. Impact of COVID-19 on ophthalmic specialist training in the United Kingdom: The trainees’ perspective. Eye 2020, 34, 2157–2160. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.; De Silva, I.; Moussa, G.; Islam, T.; Osman, L.; Malick, H.; Deol, S.; Youssef, M.; Farrag, A.; Ashraf, R.; et al. Redeployment of ophthalmologists in the United Kingdom during the coronavirus disease pandemic. Eur. J. Ophthalmol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ramirez, D.A.; Dawoud, S.A. Resident perspectives on COVID-19: Three takeaways. Am. J. Ophthalmol. 2020, 220, A2–A4. [Google Scholar] [CrossRef]
- Rakowsky, S.; Flashner, B.M.; Doolin, J.; Reese, Z.; Shpilsky, J.; Yang, S.; Smith, C.C.; Graham, K. Five questions for residency leadership in the time of COVID-19: Reflections of chief medical residents from an internal medicine program. Acad. Med. 2020, 95, 1152–1154. [Google Scholar] [CrossRef]
- Bakshi, S.K.; Ho, A.C.; Chodosh, J.; Fung, A.T.; Chan, R.V.P.; Ting, D.S.W. Training in the year of the eye: The impact of the COVID-19 pandemic on ophthalmic education. Br. J. Ophthalmol. 2020, 104, 1181–1183. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.G.; Gandhi, R.A.; Natarajan, S. Effect of COVID-19 related lockdown on ophthalmic practice and patient care in India: Results of a survey. Indian J. Ophthalmol. 2020, 68, 725–730. [Google Scholar] [CrossRef]
- Wong, T.Y.; Bandello, F. Academic ophthalmology during and after the COVID-19 pandemic. Ophthalmology 2020, 127, e51–e52. [Google Scholar] [CrossRef] [PubMed]
- Silva, N.; Laiginhas, R.; Meireles, A.; Barbosa Breda, J. Impact of the COVID-19 pandemic on ophthalmology residency training in Portugal. Acta Med. Port. 2020, 33, 640–648. [Google Scholar] [CrossRef]
- Konopińska, J.; Obuchowska, I.; Lisowski, Ł.; Dub, N.; Dmuchowska, D.A.; Rękas, M. Impact of the COVID-19 pandemic on ophthalmic specialist training in Poland. PLoS ONE 2021, 16, e0257876. [Google Scholar] [CrossRef] [PubMed]
- Rana, R.; Kumawat, D.; Sahay, P.; Gour, N.; Patel, S.; Samanta, R.; Singh, A.; Mittal, S. Perception among ophthalmologists about webinars as a method of continued medical education during COVID-19 pandemic. Indian J. Ophthalmol. 2021, 69, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, S.; Shakeel, T.; Gupta, P.; Kakkar, A.; Vats, V.; Jain, M.; Rathi, V.; Panwar, J.; Kaur, K.; Gupta, H. Impact of ophthalmic webinars on the resident’s learning experience during COVID-19 pandemic: An insight into its present and future prospects. Indian J. Ophthalmol. 2021, 69, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.; Agarwal, D. Commentary: Restructuring residency training in ophthalmology during COVID-19 era: Challenges and opportunities. Indian J. Ophthalmol. 2020, 68, 1005–1006. [Google Scholar] [CrossRef] [PubMed]
- Naushad, V.; Bierens, J.; Nishan, K.; Firjeeth, C.; Mohammad, O.; Maliyakkal, A.; ChaliHadan, S.; Schreiber, M.D. A systematic review of the impact of disaster on the mental health of medical responders. Prehospital Disaster Med. 2019, 34, 632–643. [Google Scholar] [CrossRef] [PubMed]
- Spoorthy, M.S.; Pratapa, S.K.; Mahant, S. Mental health problems faced by healthcare workers due to the COVID-19 pandemic-a review. Asian J. Psychiatry 2020, 51, 102119. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Chen, M.; Zheng, X.; Liu, J. Screening for Chinese medical staff mental health by SDS and SAS during the outbreak of COVID-19. J. Psychosom. Res. 2020, 133, 110102. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA 2020, 3, e203976. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Li, Y.; Jiang, J.; Feng, Y.; Lu, D.; Zhang, W.; Song, H. COVID-19 outbreak-related psychological distress among healthcare trainees: A cross-sectional study in China. BMJ 2020, 10, e041671. [Google Scholar] [CrossRef]
- Vallée, M.; Kutchukian, S.; Pradère, B.; Verdier, E.; Durbant, È.; Ramlugun, D.; Weizman, I.; Kassir, R.; Cayeux, A.; Pécheux, O.; et al. Prospective and observational study of COVID-19’s impact on mental health and training of young surgeons in France. Br. J. Surg. 2020, 107, e486–e488. [Google Scholar] [CrossRef] [PubMed]
- Lyson, T.; Kisluk, J.; Alifier, M.; Politynska-Lewko, B.; Sieskiewicz, A.; Kochanowicz, J.; Reszec, J.; Niklinski, J.; Rogowski, M.; Konopinska, J.; et al. Transnasal endoscopic skull base surgery in the COVID-19 era: Recommendations for increasing the safety of the method. Adv. Med. Sci. 2021, 66, 221–230. [Google Scholar] [CrossRef]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Ho, C.S.; Ho, R.C. Immediate psychological responses and associated factors during the initial stage of the 2019 coronavirus disease (COVID-19) epidemic among the general population in China. Int. J. Environ. Res. Public Health 2020, 17, 1729. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Konopińska, J.; Obuchowska, I.; Lisowski, Ł.; Dub, N.; Kozera, M.; Rękas, M. Intention to get COVID-19 vaccinations among ophthalmology residents in Poland: A cross-sectional survey. Vaccines 2021, 9, 371. [Google Scholar] [CrossRef]
- Mehrotra, A.; Chernew, M.; Linetsky, D.; Hatch, H.; Cutler, D. The Impact of the COVID-19 Pandemic on Outpatient Visits: A Rebound Emerges; To the Point (Blog); Commonwealth Fund: New York, NY, USA, 2020. [Google Scholar] [CrossRef]
- American Academy of Ophthalmology. Recommendations for Urgent and Nonurgent Patient Care 2020. Available online: https://www.aao.org/headline/new-recommendations-urgent-nonurgent-patient-care (accessed on 1 May 2021).
- Moazzami, B.; Razavi-Khorasani, N.; Dooghaie Moghadam, A.; Farokhi, E.; Rezaei, N. COVID-19 and telemedicine: Immediate action required for maintaining healthcare providers well-being. J. Clin. Virol. 2020, 126, 104345. [Google Scholar] [CrossRef] [PubMed]
- Saleem, S.M.; Pasquale, L.R.; Sidoti, P.A.; Tsai, J.C. Virtual ophthalmology: Telemedicine in a COVID-19 era. Am. J. Ophthalmol. 2020, 216, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Jaud, C.; Salleron, J.; Cisse, C.; Angioi-Duprez, K.; Berrod, J.P.; Conart, J.B. EyeSi Surgical Simulator: Validation of a proficiency-based test for assessment of vitreoretinal surgical skills. Acta Ophthalmol. 2020, 99, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Staropoli, P.C.; Gregori, N.Z.; Junk, A.K.; Galor, A.; Goldhardt, R.; Goldhagen, B.E.; Shi, W.; Feuer, W. Surgical simulation training reduces intraoperative cataract surgery complications among residents. Simul. Healthc. J. Soc. Simul. Healthc. 2018, 13, 11–15. [Google Scholar] [CrossRef] [PubMed]
- Chatziralli, I.; Ventura, C.V.; Touhami, S.; Reynolds, R.; Nassisi, M.; Weinberg, T.; Pakzad-Vaezi, K.; Anaya, D.; Mustapha, M.; Plant, A.; et al. Transforming ophthalmic education into virtual learning during COVID-19 pandemic: A global perspective. Eye 2020, 35, 1459–1466. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Participants | Respondents | Psychiatric Symptoms | Main Findings |
|---|---|---|---|---|
| El-Saied et al., 2020 [16] | 79 | Trainees and young ophthalmologists (practicing for <1 to 9 years) | Negative feelings | There were 55.8% who felt unlucky starting ophthalmic practice during the COVID era; 11.4% regret being ophthalmologists; 19% regret being physicians; 30.4% think about a career shift; 21.8% think they might need a psychological assessment and help after the pandemic. |
| Alahmadi et al., 2020 [9] | 142 | Residents | Depression | Mild depression: 33.1%; moderate depression: 26.1%; severe depression: 11.3%. |
| Khanna et al., 2020 [10] | 2355 | Ophthalmologists, ophthalmology trainees; 358 (15.2%) were residents or fellows under training | Depression | Mild depression: 21.4%; moderate depression: 6.9%; severe depression: 4.3%. Depression significantly higher in younger individuals, females, those not in practice, ophthalmologists-in-training, and those who were single. |
| Szigiato et al., 2020 [14] | 102 | Trainee | Anxiety | Higher level of anxiety than before pandemic: 70%; |
| Mishra et al., 2020 [13] | 716 | Trainee | Stress | increased stress levels: 54.8%; generally unhappy state of mind during lockdown period: 46.5%. |
| Kavadarli et al., 2021 [15] | 161 | Actively working ophthalmologists with 28.4% ophthalmologists at the age of 25–34 years | Anxiety | Ninety-one percent of the participants stated that their anxiety level increased during the pandemic, most commonly due to the risk of transmitting the disease to their family (83%). |
| Almater et al., 2020 [11] | 118 | Ophthalmologists with varying practical experience, and the majority are residents (61.7%) | Depression Anxiety Insomnia Stress | Depression in 50.5% of respondents (21.4% reported severe and moderately severe symptoms; 17.8% with moderate symptoms and 21.5% with mild symptoms). Depression significantly higher among females, participants living with the elderly. Anxiety in 46.7% of participants (25.2% with mild symptoms, 15.9% with moderate, and 5.6% with severe symptoms). Anxiety significantly more common among females, frontline healthcare providers, and those living with elderly. Insomnia in 44.9% of respondents (29.9 with mild symptoms, 13.1% with moderate and 1.9/5 with severe symptoms), more commonly in front-line healthcare providers. Higher level of stress in 22% of respondents (28% with low level, 68% moderate level and 3.7% with severe); more common in females. |
| Reference | Country/Region | Redeployment (%) |
|---|---|---|
| Silva et al., 2020 [25] | Portugal | 25% |
| Szigiato et al., 2020 [14] | Canada | 4.9% |
| Mishra et al., 2020 [13] | India | 24.6% |
| Ferrara et al., 2020 [6] | 32 different countries | 27–28% |
| Alahmadi et al., 2020 [9] | Saudi Arabia | 18.3% |
| Hussain et al., 2020 [18] | United Kingdom | 39% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dub, N.; Konopińska, J.; Obuchowska, I.; Lisowski, Ł.; Dmuchowska, D.A.; Rękas, M. The Impact of the COVID-19 Pandemic on Ophthalmology Residents: A Narrative Review. Int. J. Environ. Res. Public Health 2021, 18, 11567. https://doi.org/10.3390/ijerph182111567
Dub N, Konopińska J, Obuchowska I, Lisowski Ł, Dmuchowska DA, Rękas M. The Impact of the COVID-19 Pandemic on Ophthalmology Residents: A Narrative Review. International Journal of Environmental Research and Public Health. 2021; 18(21):11567. https://doi.org/10.3390/ijerph182111567
Chicago/Turabian StyleDub, Natalia, Joanna Konopińska, Iwona Obuchowska, Łukasz Lisowski, Diana Anna Dmuchowska, and Marek Rękas. 2021. "The Impact of the COVID-19 Pandemic on Ophthalmology Residents: A Narrative Review" International Journal of Environmental Research and Public Health 18, no. 21: 11567. https://doi.org/10.3390/ijerph182111567