1. Introduction
Coronavirus disease 2019 (COVID-19) is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), and is transmitted via respiratory droplets and direct contact [
1,
2] Symptoms, which may include fever, chills, cough, or shortness of breath, appear 2–14 days after exposure to the virus [
3]. The case fatality rate of COVID-19 is approximately 2% to 3%, but it is highly contagious and has developed rapidly worldwide [
2].
The first COVID-19 case in the United States was reported on 21 January 2020 [
4]. The World Health Organization [
5] declared this outbreak a pandemic in March 2020. As of August 2021, the U.S. has the highest number of reported COVID-19 infections and related deaths in the world, accounting for 17.8% of total global confirmed cases. Among 3142 U.S. counties, 247 counties reached the 90th percentile for hospitalization-per-bed, and 136 counties were in the 90th percentile for ICU-per-bed [
6].
Stricter lockdown measures were enforced to combat rising COVID cases, resulting in a global economic crisis. In the U.S., unemployment rates increased to 14.7% in April 2020 [
7]. The pandemic caused economic disruptions and an exceptional increase in uncertainty in the U.S. economy, which will likely drive the U.S. economy into recession [
8]. While following the CDC guidelines, each county and major U.S. city developed its own timing, range, breadth, and depth of actions depending on geographic and demographic differences and political diversity [
9].
As COVID-19 spread throughout communities across the U.S., it became clear that inequities would arise among differing demographics. Several studies suggested that certain racial and ethnic minority groups may have been disproportionately impacted by the spread of COVID-19 [
10,
11]. For instance, the African American population comprises 13% of the total U.S. population [
12], while according to CDC COVID-19 data [
13], it made up 30% of all COVID-19 positive cases in the U.S. as of 15 April 2020. In addition, hospitalization rates due to COVID-19 have a disproportionately higher prevalence among the African American population than among any other race [
14].
In addition, Hispanics are currently the largest ethnic minority in the U.S., with a population of nearly 60 million people [
15]. While Hispanics account for 18% of the total U.S. population, they constitute nearly 28.4% of the total COVID-19 cases nationally [
15]. Nevertheless, the proportions vary strongly in different parts of the country. For instance, a statewide study investigating racial disparities followed 3481 COVID-19 cases in Louisiana and found that non-Hispanic African American individuals represented 77% of hospitalizations and 71% of deaths, despite only making up 31% of the total source population [
10,
11]. In New York City, COVID-19 mortality rates were 220 and 236 per 100,000 for African American and Latinx patients, respectively, whereas White and Asian Americans had mortalities of 110 and 102 per 100,000, respectively [
11].
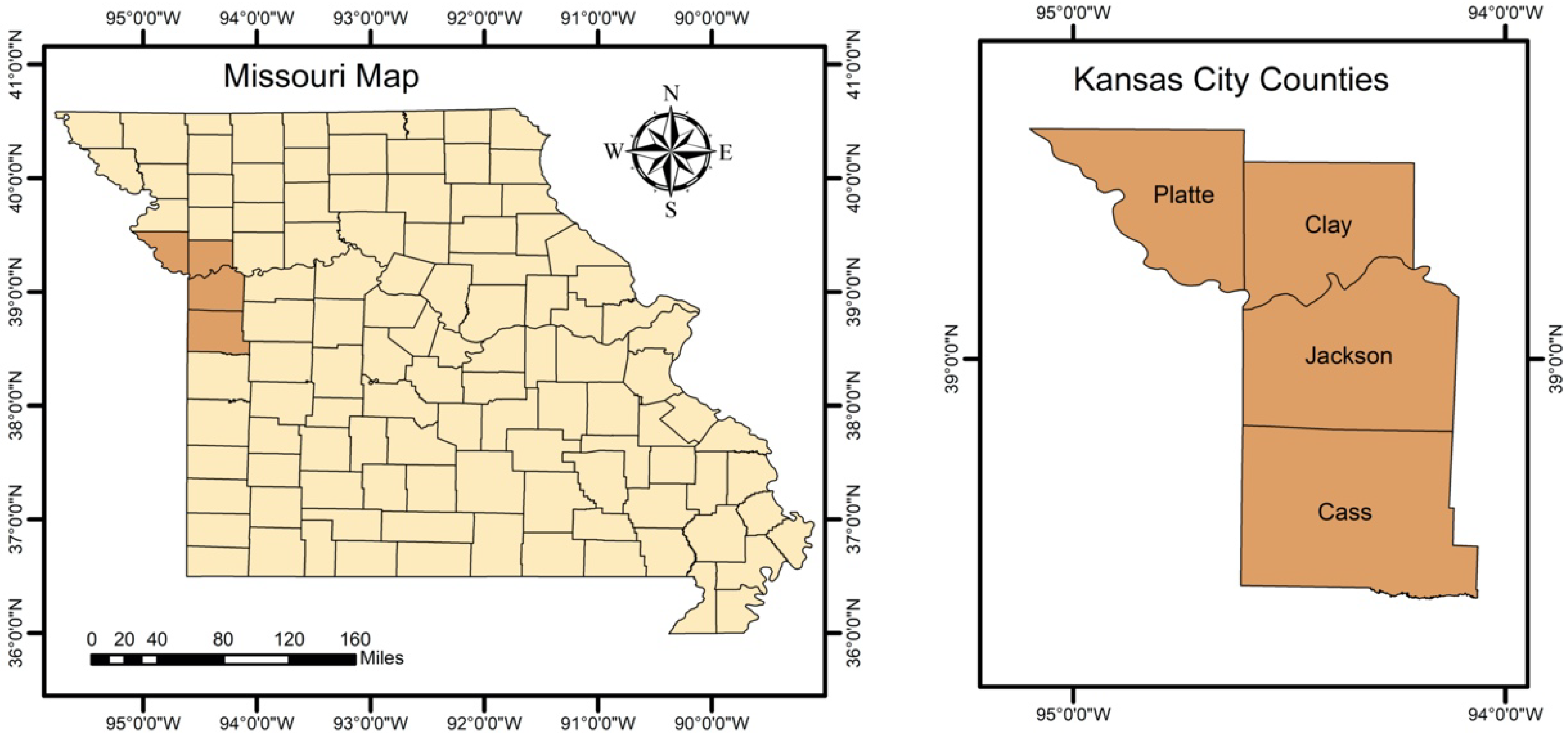
Of particular interest, the City of Kansas City, MO, issued a state of emergency proclamation on 12 March 2020, which effectively placed limits on gatherings and mandated masks [
16]. Like other U.S. cities, social distancing measures were applied throughout Kansas City, MO. Kansas City, MO became one of the U.S.’s COVID-19 hot spots due to a substantial increase in the rate of positive COVID-19 test results in 2020. It also became one of 10 cities across the U.S. that received the attention of the White House coronavirus task force in 2020 [
17]. Despite efforts to reduce the prevalence of infection, 40,486 confirmed cases and 597 deaths had been reported in Kansas City as of 8 July 2021 [
18]. With the increase in COVID-19 vaccinations, and in accordance with CDC guidelines, on 14 May 2021, Kansas City ended its emergency order requiring masking and social distancing. Despite the rise in vaccinations, cases have continued to increase, highlighting the need for a better understanding of how COVID-19 is spreading across the city.
As of 21 October 2021, the World Health Organization (WHO) database shows that out of 310,548 papers related to COVID-19, there are only 37 papers focusing on Kansas City. Most of those papers are associated with medical aspects of COVID-19 in Kansas City, MO [
19,
20,
21,
22,
23]. The other papers relate to factors such as mask mandates [
24,
25], vaccine aspects and patient hospitalization [
24,
26]. One of these papers involved a retrospective study on COVID-19 data examining gender and race [
19]. However, the study focused on the therapeutic factors that influenced COVID-19 patients’ ICU admissions with respect to gender and race. Another study analyzed data from both St. Louis and Kansas City, MO to compare COVID-19 testing rates per diagnosed cases between races [
27]. By studying COVID-19 testing data over time, this study concluded that black populations observed lower COVID-19 testing rates than white populations. Another paper focused on COVID-19 cases in relation to income level by studying specific zip codes in Kansas City, MO [
28]. One main finding was that an increase in median income level was associated with a decrease in the health risk gap. The above-mentioned papers contribute to the existing literature. However, they largely ignore how the geographical distributions of COVID-19 cases may be impacted by demographic factors.
It is crucial to establish spatial monitoring during an evolving pandemic with several strains, such as COVID-19. Spatial statistical clustering can be used as a COVID-19 surveillance tool in communities. Among the global measures of spatial clustering analysis, spatial scan statistics is one of the most popular and powerful techniques applied to perform geographical surveillance of diseases [
29]. Spatial cluster analysis has been used in a wide variety of epidemiological studies to evaluate spatial patterns of infections [
30,
31,
32]. Some examples include identifying birth defects in New York State [
33] and studying spatial patterns of malaria and detecting spatial clusters of tuberculosis in China [
32,
34]. In fact, spatial clusters can be more valuable in identifying regions with an increased risk of COVID-19 in certain racial and ethnic minority groups if we consider the demographic factors. Cluster detection of when and where COVID-19 transmission occurs is critical to preventing another wave, preventing small local outbreaks in certain communities, and eventually controlling the epidemic by establishing testing and vaccination centers in the most impacted regions. To our knowledge, there is no published research article that retrospectively examines COVID-19 spatial clusters with respect to demographic factors in Kansas City, MO. Hence, the main purpose of the present study was to provide an unbiased spatial and temporal analysis of COVID-19 data with respect to demographic factors in Kansas City, MO. Using the COVID-19 data, we analyzed the progression of COVID-19 infection in Kansas City with respect to gender, race, and ethnicity. This study implements a retrospective spatial analysis of COVID-19 in Kansas City, MO, at the zip code level for the period March–November 2020.
4. Discussion
Spatial cluster analysis is often utilized to identify regions with an increased risk of occurrence of studied phenomena. Studying the cluster patterns of COVID-19 can provide evidence for specific risk factors that influence the spread of this virus, establishing improved prevention and control measures. Understanding the spatial patterns can also enable public health departments and decision-makers to implement more COVID-19 vaccination clinics in high-risk areas, controlling the severity and spread of disease. Thus, the results of this study can assist the KCMO Health Department in developing more effective prevention strategies in future.
The main purpose of the present study was to provide an unbiased spatial and temporal analysis of COVID-19 data in Kansas City, MO. We examined significant differences in COVID-19 clusters with respect to demographic factors of gender, race, and ethnicity. Our research is the first study to utilize retrospective spatial statistics adjusted for demographic factors to monitor COVID-19 in Kansas City, MO.
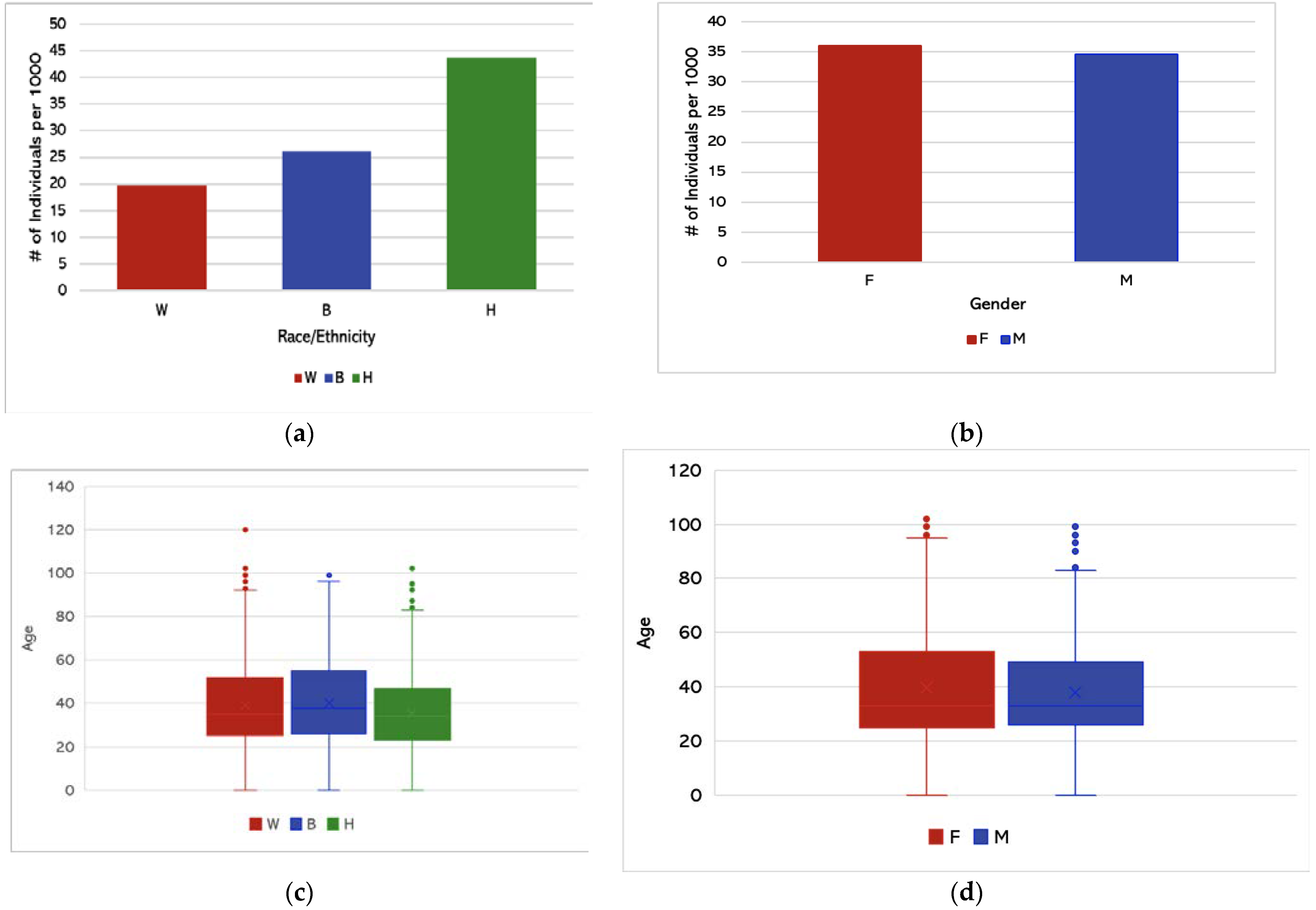
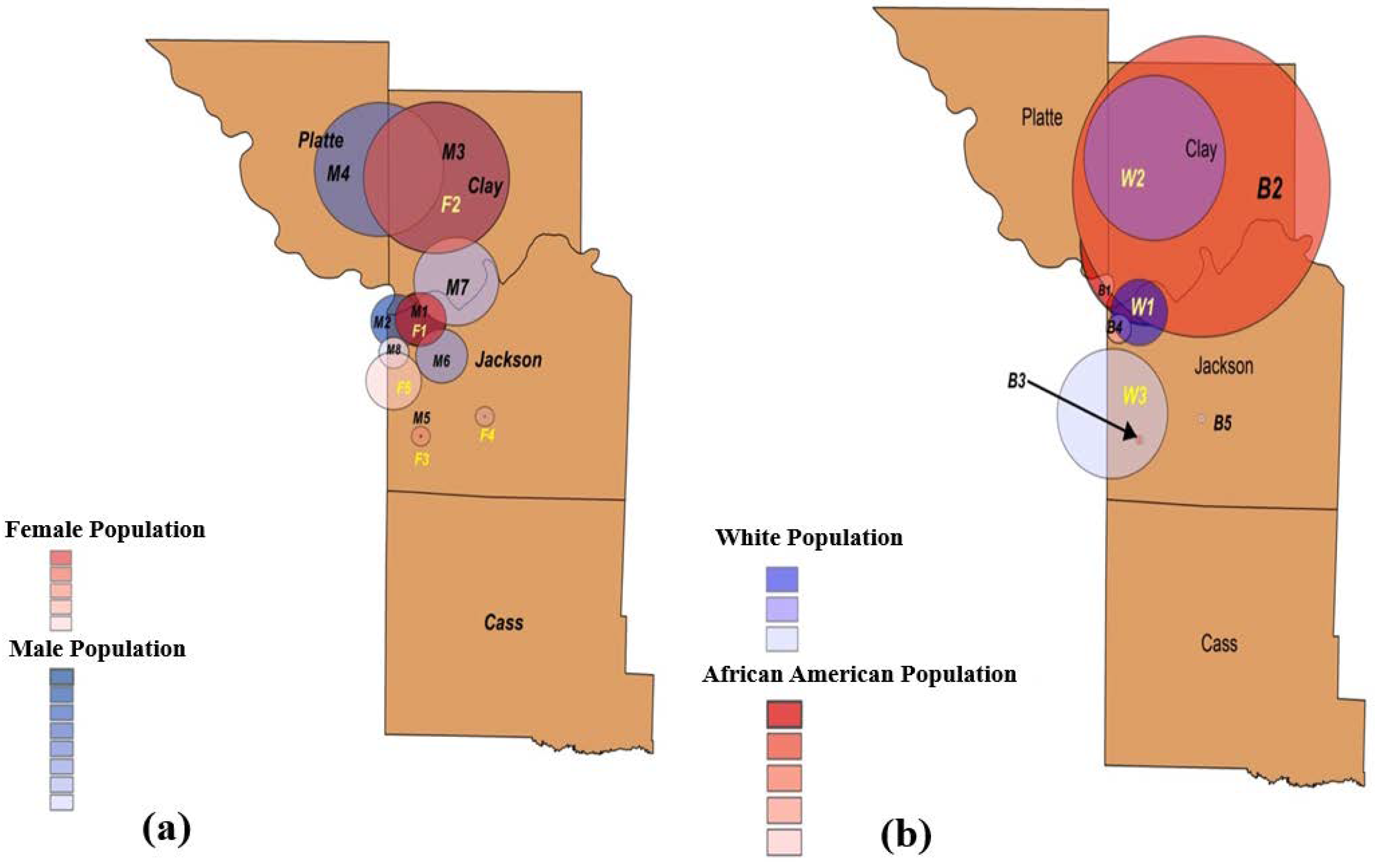
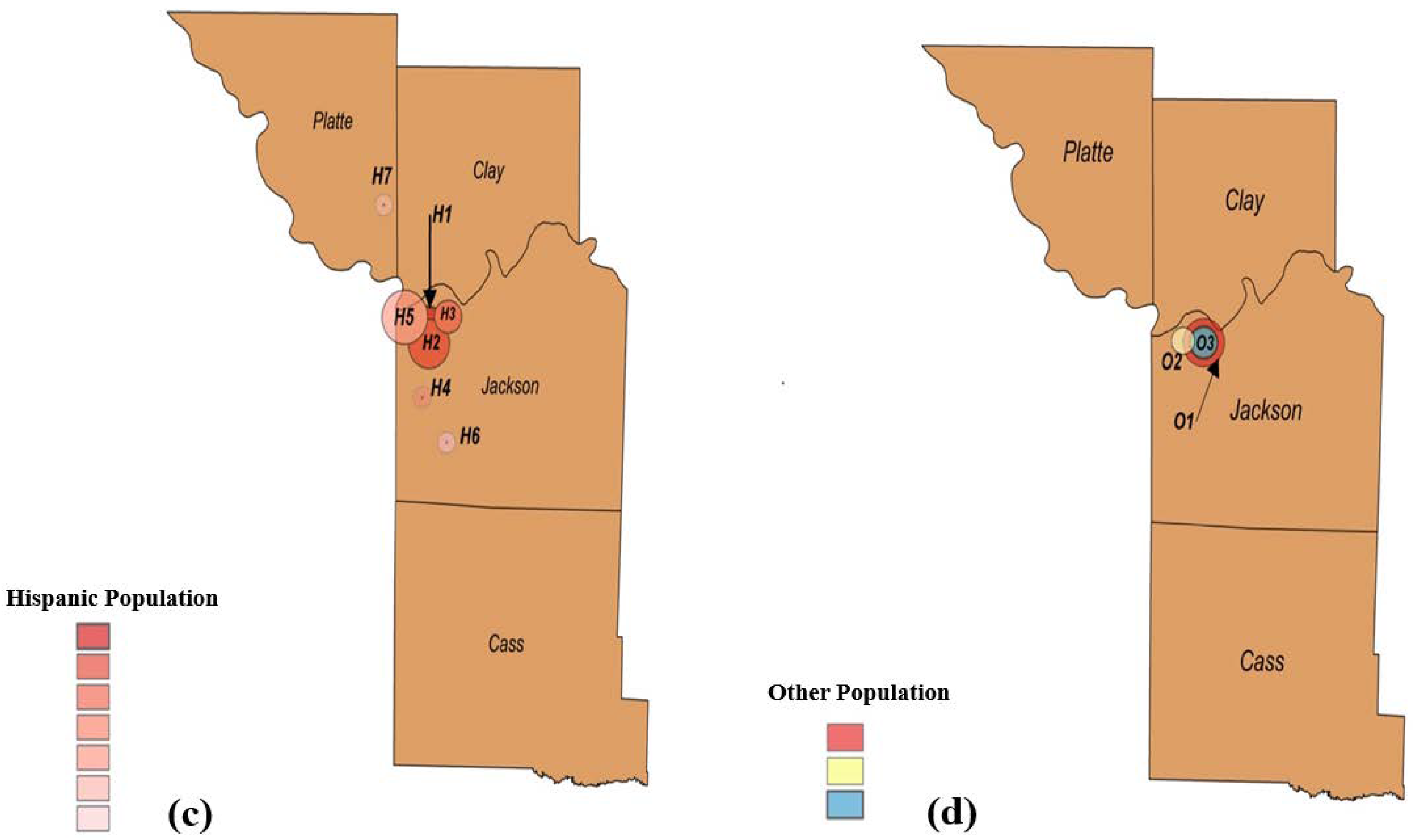
Retrospective spatial analysis was able to identify eight clusters belonging to male populations, five spatial clusters for African American populations, and seven spatial clusters representing Hispanic populations, which had the most scattered clusters and the highest prevalence of COVID-19 cases when compared to those of the African American and White populations. Most of the spatial demographic clusters concentrated in downtown Kansas City, located in Jackson County. In addition, the average age of Hispanic individuals with COVID-19 was significantly lower than that of both African American and White individuals. This finding was identified via ANOVA testing which determined a statistically significant difference between the three groups (Hispanic, Black, and White individuals), followed by a post-hoc test which determined the differences in the means.
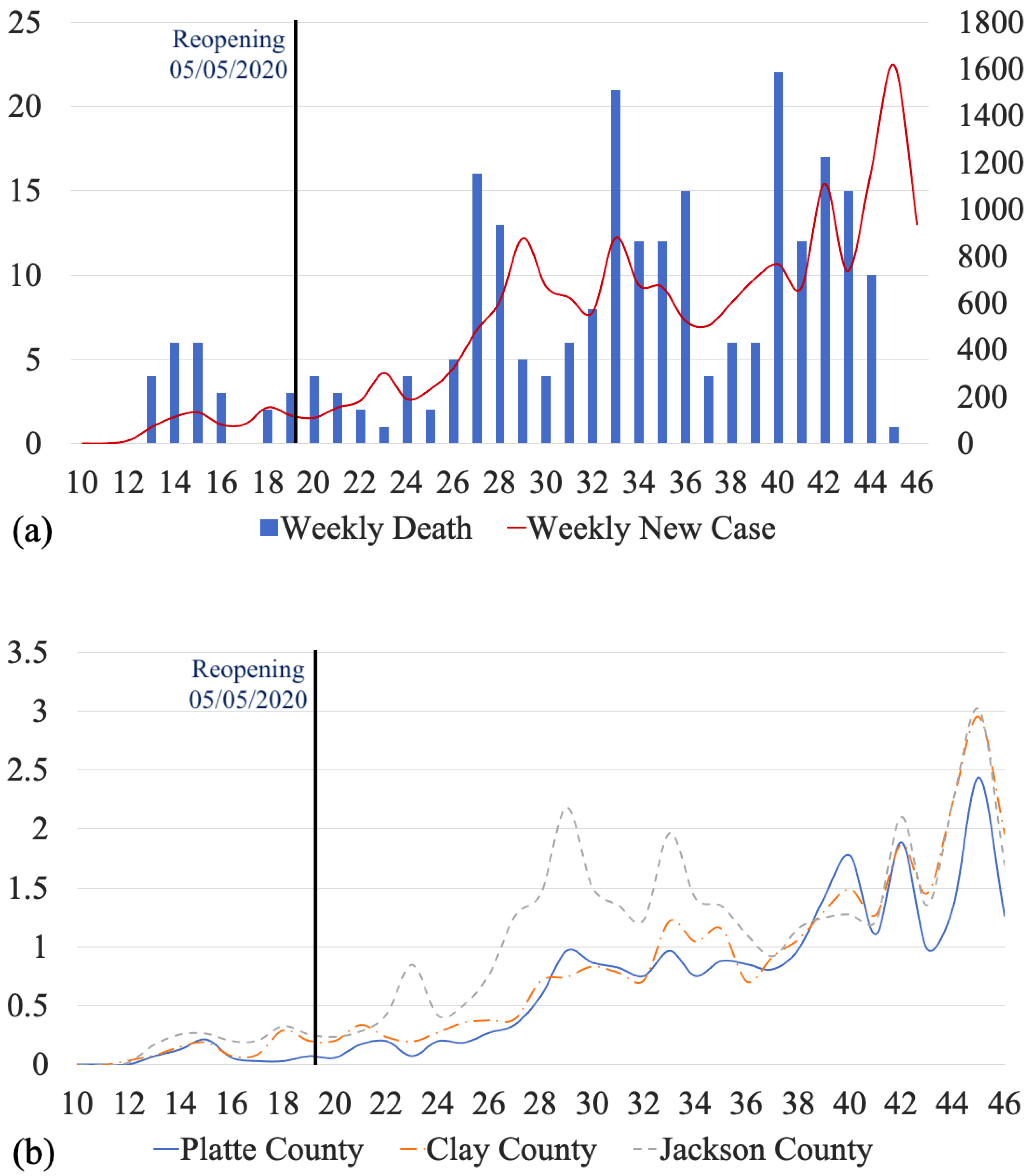
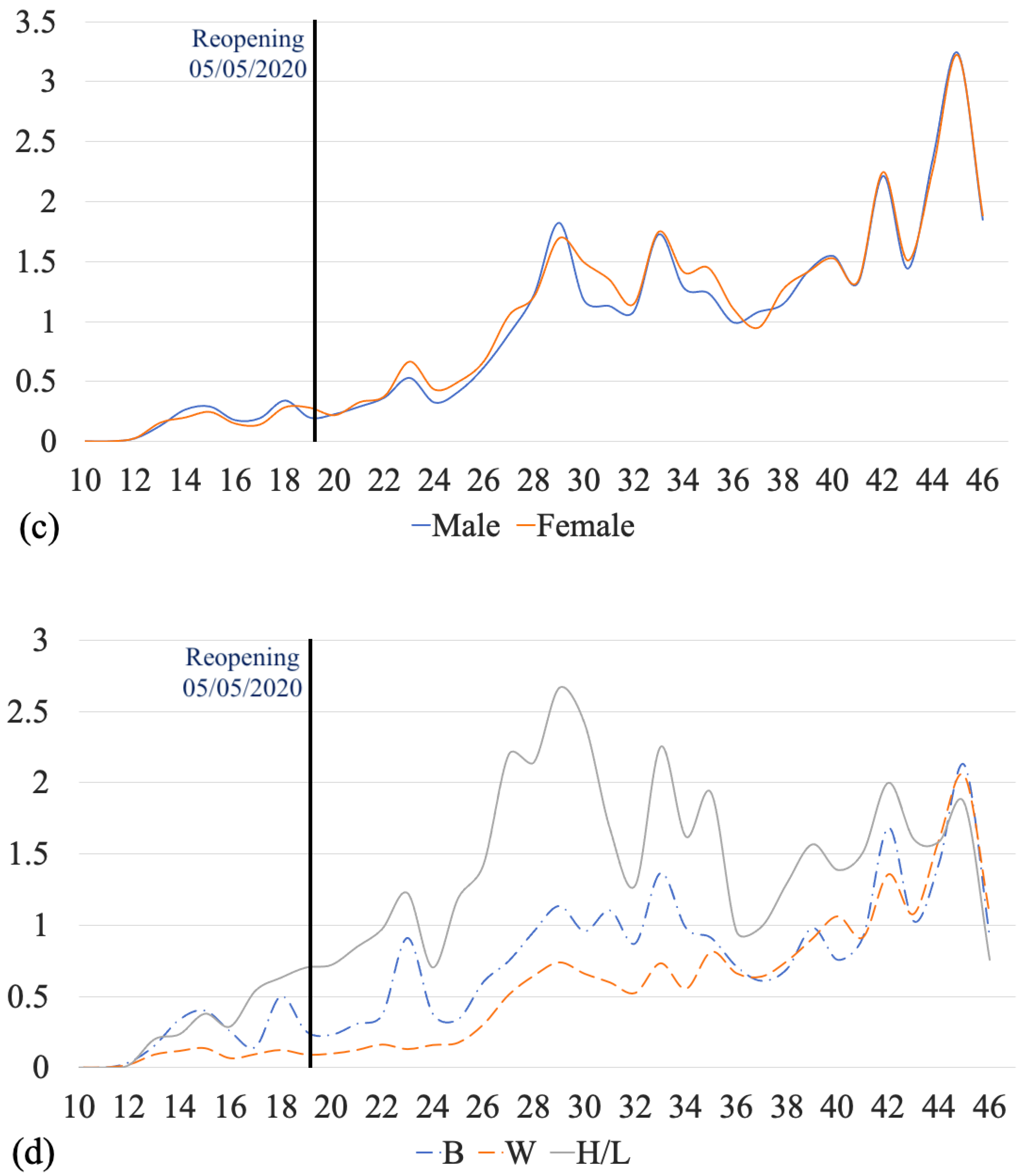
We also monitored the temporal variations in the number of COVID-19 cases between March and November 2020. The time series of the cases had multiple M-shaped (double-top) curves. There were three obvious M-shaped curves that showed the increase in cases occurring with a type of period. Five weeks after reopening, a continuous increase appeared for four weeks, followed by the appearance of an M-shaped curve. Reopening influenced weekly new COVID-19 cases in the short term. In addition, compared to the time series of weekly cases per thousand for Clay County and Platte County, Jackson County had the greatest number of cases per thousand for the first 24 weeks. However, after the 37th week, the COVID-19 outbreak shifted. The trend and number of cases per thousand for the three counties became similar. The time series of Hispanic/Latino cases led the temporal trend until the 44th week.
Despite the contributions of our study, there are several limitations and assumptions. First, to understand why certain communities have been severely impacted by this pandemic, it is important to study the health inequities and social determinants of health that contribute to current conditions. Certain factors such as socioeconomic status, medical conditions, healthcare access, and barriers, such as language and immigration status, may impact the spread of COVID-19 across regions. For instance, cluster H4 of the Hispanic population had an extremely large RR of 4.77. The region of this cluster covered three blocks east of Highway 71 and north of E. 75th Street. Of 361 Hispanic individuals in this region, 61 (16.8%) tested positive for COVID-19. Therefore, it is important to study the factors that impact the spread of COVID-19 in such areas. Being uninsured is another factor that may prevent individuals from seeking proper COVID-19 testing and treatments. In Kansas City, MO, the age-adjusted death rate for Hispanics was 2.7 times higher than for White residents, and the age-adjusted death rate for African Americans was 1.6 times higher than for White residents. Pre-existing medical conditions and access to healthcare may have contributed to the disproportionate impact of COVID-19 on the Hispanic community. Moreover, some researchers suggested that COVID-19 cases in Kansas City, MO were related to income level [
28]. The health risk gap narrows as the median income rises, and being white and having a higher median income offers a significant advantage compared to racial and ethnic minority groups with lower median incomes [
28]. Thus, income level may contribute to the disproportionate impact of COVID-19 on certain communities. Second, only confirmed cases were included in the KCMO Health Department data, and it is vital to note that unconfirmed and probable cases are not evaluated owing to unavailability and uncertainty. As a result, a full perspective on the impact of COVID-19 in Kansas City, MO on certain communities will be impossible to obtain for some time. Third, our results focus on data from March–November of 2020, which was prior to vaccine distribution. Therefore, trends, number of emerging clusters, and relative risks would likely be different if we updated the current data. Lastly, COVID-19 is more severe in the elderly [
40,
41]. Future research can examine spatial clusters with respect to demographic factors that adjust for age and other abovementioned factors (socioeconomic status, income level, and healthcare access).
5. Conclusions
Analyzing the daily confirmed COVID-19 cases in Kansas City, MO, at the zip code level enabled us to study the variations in COVID-19 clusters based on gender, race, and ethnicity. From March to November 2020, we used a retrospective Poisson spatial scan statistic to observe the geographical distribution of COVID-19 cases associated with these demographic variables. Our statistical findings revealed that male population clusters were more widely dispersed than female population clusters. Clusters of the Hispanic population were the most prevalent and the most widely dispersed.
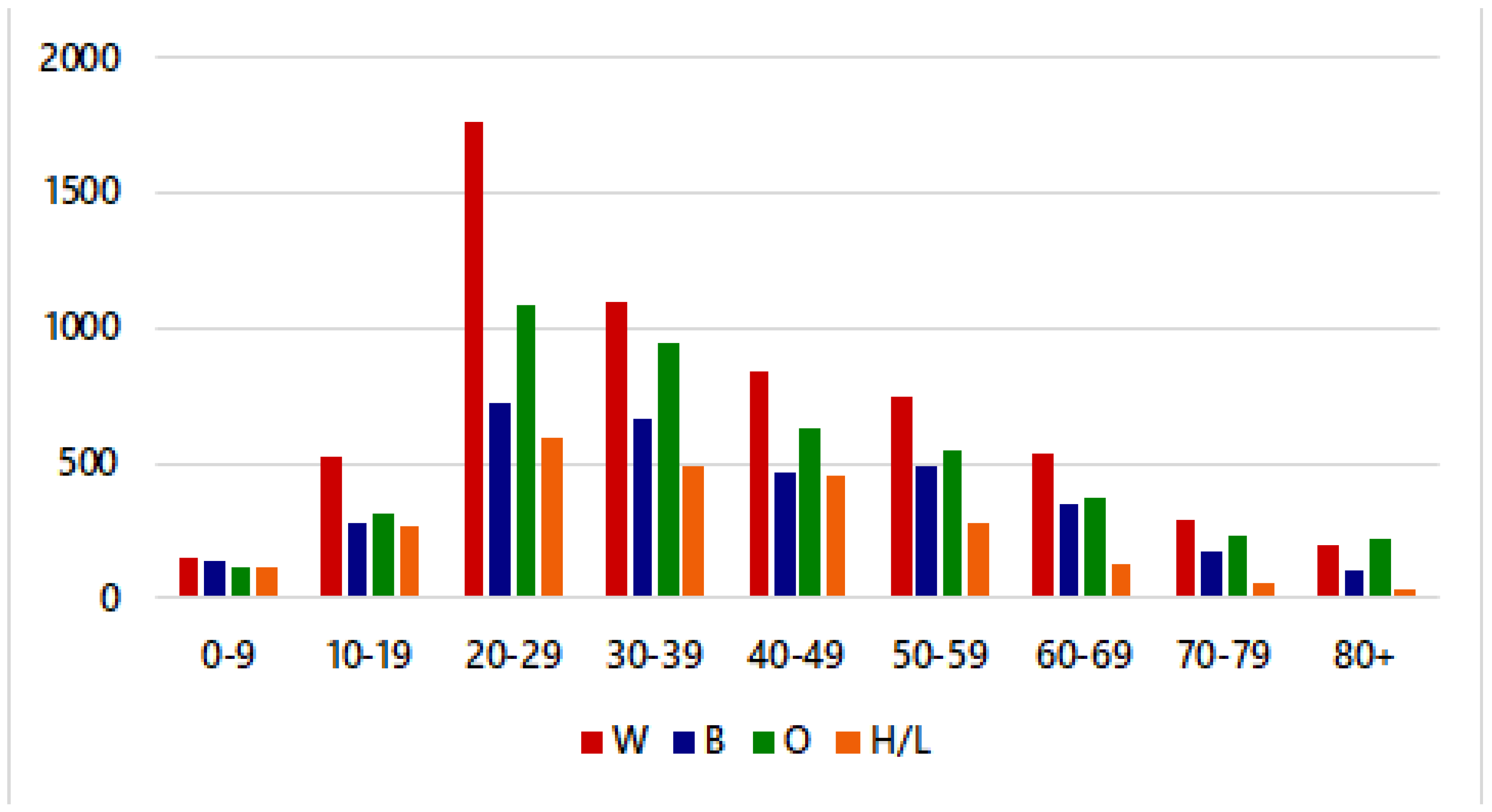
Descriptive analysis showed that Hispanic/Latino individuals had the highest prevalence and led the temporal trend of COVID-19 cases in Kansas City when compared with African American and White individuals. Moreover, the average age of Hispanic individuals with COVID-19 was significantly lower than that of both African American and White individuals. When observing the number of new weekly COVID-19 cases by race/ethnicity, we could see that Hispanic/Latino individuals had a higher rate of cases than African American and White individuals.
A spatial and temporal demographic analysis of COVID-19 data enables local health departments to gain a deeper understanding of the regions of Kansas City with increased incidences of cases, as well as the risk factors that influence the spread of disease. Identifying counties and hotspot areas with the highest incidence of COVID-19 cases can help guide Kansas City, MO in deciding where to increase vaccination distribution efforts and COVID-19 testing sites. It may be beneficial to study the areas with statistically significant clusters to ensure that these regions have adequate testing and triage centers within close proximity. Establishing free COVID-19 testing sites and promoting social distancing guidelines, proper hygiene measures, and distributing masks in these areas could help control the spread of COVID-19, as well.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}