
Health Impact Assessments of Health Sector Proposals: An Audit and Narrative Synthesis



Abstract
:1. Introduction
2. Review Aims
3. Methods
4. Eligibility Criteria
4.1. Inclusion
4.2. Exclusion
5. Data Sources
5.1. Electronic Databases
5.2. HIA Websites
5.3. Study Selection and Data Extraction
6. Analytic Approach
7. Appraisal of HIA Report Quality
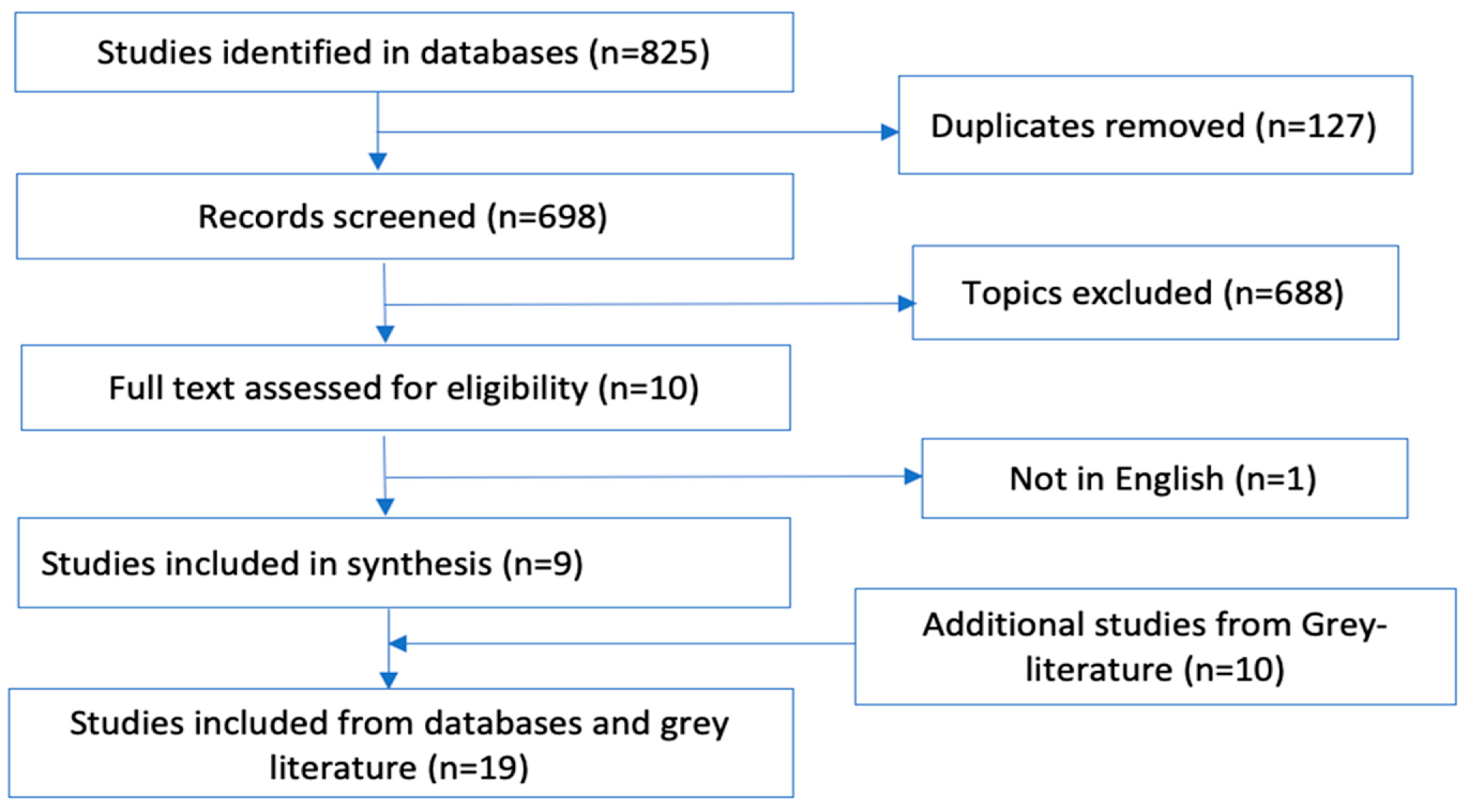
8. Results
8.1. Included HIAs
8.2. Characteristics of Included Health Impact Assessments
8.3. Use of HIA to Assess Health Sector Proposals
8.4. Types of HIAs
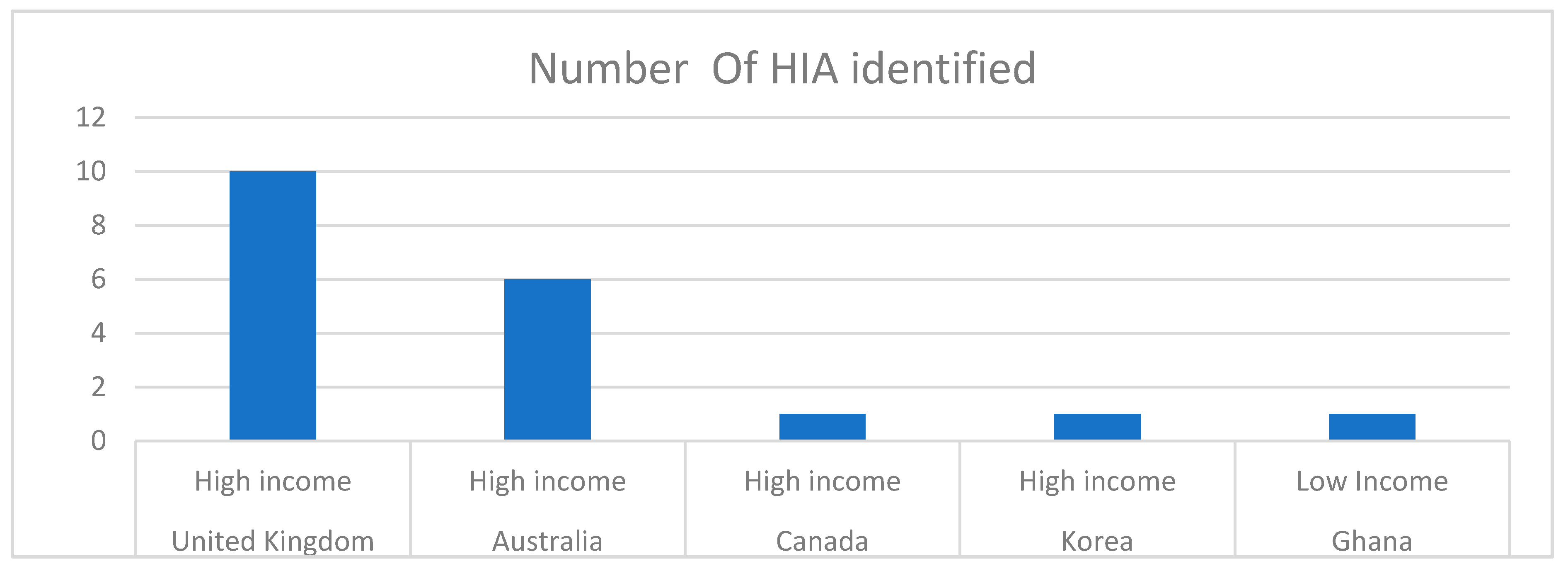
8.5. Setting for HIAs
8.6. Sources of Evidence within HIAs
8.7. The Quality of Health Sector HIA Reports
9. Discussion
10. Implications for Practice and Research
11. Limitations
12. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CASP | Critical appraisal skills program |
| HIA | Health impact assessment |
| PRISMA-P | Preferred Reporting Items for Systematic reviews and Meta-Analysis Protocol |
| WHO | World Health Organization |
References
- McCallum, L.; Souweine, K.; McDaniel, M.; Koppe, B.; McFarland, C.; Butler, K.; Ollson, C. Health impact assessment of an oil drilling project in california. Int. J. Occup. Med. Environ. Health 2016, 29, 229–253. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.J.; Harris-Roxas, B.F.; Harris, E. An overview of the regulatory planning system in New South Wales: Identifying points of intervention for health impact assessment and consideration of health impacts. N. S. W. Public Health Bull. 2007, 18, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Buregeya, J.M.; Loignon, C.; Brousselle, A. Contribution analysis to analyze the effects of the health impact assessment at the local level: A case of urban revitalization. Eval. Program Plan. 2020, 79, 101746. [Google Scholar] [CrossRef] [PubMed]
- Oleribe, O.O.; Ukwedeh, O.; Burstow, N.J.; Gomaa, A.I.; Sonderup, M.W.; Cook, N.; Waked, I.; Spearman, W.; Taylor-Robinson, S.D. Health: Redefined. Pan Afr. Med. J. 2018, 30, 292. [Google Scholar] [CrossRef]
- Bourcier, E.; Charbonneau, D.; Cahill, C.; Dannenberg, A.L. An evaluation of health impact assessments in the United States, 2011–2014. Prev. Chronic Dis. 2015, 12, E23. [Google Scholar] [CrossRef] [Green Version]
- Harris, P.; Sainsbury, P.; Kemp, L. The fit between health impact assessment and public policy: Practice meets theory. Soc. Sci. Med. 2014, 108, 46–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkler, M.S.; Furu, P.; Viliani, F.; Cave, B.; Divall, M.; Ramesh, G.; Harris-Roxas, B.; Knoblauch, A.M. Current Global Health Impact Assessment Practice. Int. J. Environ. Res. Public Health 2020, 17, 2988. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.; Parry, J.; Mathers, J. Participation in health impact assessment: Objectives, methods and core values. Bull. World Health Organ. 2005, 83, 58–63. [Google Scholar]
- Veerman, J.L.; Barendregt, J.J.; Mackenbach, J.P. Quantitative health impact assessment: Current practice and future directions. J. Epidemiol. Community Health 2005, 59, 361–370. [Google Scholar] [CrossRef]
- Haigh, F.; Baum, F.; Dannenberg, A.L.; Harris, M.F.; Harris-Roxas, B.; Keleher, H.; Kemp, L.; Morgan, R.; Chok, H.N.; Spickett, J.; et al. The effectiveness of health impact assessment in influencing decision-making in Australia and New Zealand 2005–2009. BMC Public Health 2013, 13, 1188. [Google Scholar] [CrossRef] [Green Version]
- Dannenberg, A.L. Effectiveness of health impact assessments: A synthesis of data from five impact evaluation reports. Prev. Chronic Dis. 2016, 13, E84. [Google Scholar] [CrossRef]
- McCartney, G.; Popham, F.; McMaster, R.; Cumbers, A. Defining health and health inequalities. Public Health 2019, 172, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Mindell, J.; Ison, E.; Joffe, M. A glossary for health impact assessment. J. Epidemiol. Community Health 2003, 57, 647–651. [Google Scholar] [CrossRef] [Green Version]
- Harris, E. Contemporary debates in health impact assessment: What? Why? When? N. S. W. Public Health Bull. 2005, 16, 107–108. [Google Scholar]
- Myers, S.S.; Gaffikin, L.; Golden, C.; Ostfeld, R.; Redford, K.H.; Ricketts, T.H.; Turner, W.R.; Osofsky, S.A. Human health impacts of ecosystem alteration. Proc. Natl. Acad. Sci. USA 2013, 110, 18753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris-Roxas, B.; Viliani, F.; Bond, A.; Cave, B.; Divall, M.; Furu, P.; Harris, P.; Soeberg, M.; Wernham, A.; Winkler, M. Health impact assessment: The state of the art. Impact Assess. Proj. Apprais. 2012, 30, 43–52. [Google Scholar] [CrossRef]
- Lifsey, S.; Cash, A.; Anthony, J.; Mathis, S.; Silva, S. Building the Evidence Base for Population-Level Interventions. Health Educ. Behav. 2015, 42 (Suppl. 1), 133S–140S. [Google Scholar] [CrossRef]
- Bos, R. Health impact assessment and health promotion. Bull. World Health Organ. 2006, 84, 914–915. [Google Scholar] [CrossRef]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; E Brennan, S.; et al. PRISMA 2020 explanation and elaboration: Updated guidance and exemplars for reporting systematic reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. J. Clin. Epidemiol. 2009, 62, e1–e34. [Google Scholar]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dhammi, I.K.; Kumar, S. Medical subject headings (MeSH) terms. Indian J. Orthop. 2014, 48, 443–444. [Google Scholar] [CrossRef] [PubMed]
- McCracken, M.O. Endnote X8. 2006–2013: US; Clarivate: Philadephia, PA, USA, 2017. [Google Scholar]
- Team, T.E. Endnote. 2013, Clarivate: Transparent and Complete Reporting; Clarivate: Philadephia, PA, USA, 2013. [Google Scholar]
- HIA Gateway. Health Impact Assessment Gateway Website I The National Archives. 2017. Available online: http://discovery.nationalarchives.gov.uk/details/r/C16736 (accessed on 21 June 2021).
- HIA Connect. Building Capacity to Undertake Health Impact Assessment. 2017. Available online: http://hiaconnect.edu.au/ (accessed on 21 June 2021).
- The PEW Charitable Trusts. Health Impact Assessment. 2017. Available online: http://www.pewtrusts.org/en/projects/health-impact-project/health-impact-assessment (accessed on 22 June 2021).
- World Health Organisation (WHO). Health Impact Assessment. 2017. Available online: http://www.who.int/hia/en/ (accessed on 22 June 2021).
- IAIA. The Leading Global Network on Impact Assessment. 2017. Available online: http://www.iaia.org/ (accessed on 21 June 2021).
- SOPHIA. HIA Publications. 2017. Available online: https://hiasociety.org/HIA-Publications (accessed on 21 June 2021).
- Davey, S.; Davey, A.; Singh, J. Metanarrative review: Current status and opportunities for public health research. Int. J. Health Syst. Disaster Manag. 2013, 1, 59–63. [Google Scholar] [CrossRef]
- Harris, P.; Harris-Roxas, B.; Harris, E.; Kemp, L. Health Impact Assessment: A Practical Guide; Centre for Health Equity Training, Research and Evaluation (CHETRE). Part of the UNSW Research Centre for Primary Health Care and Equity, UNSW: Sydney, Australia, 2007. [Google Scholar]
- Critical Skills Appraisal Programme (CASP). CASP Checklist. 2006. Available online: http://www.casp-uk.net/casp-tools-checklists (accessed on 25 June 2021).
- Maxwell, M.; Harris, P.; Peters, S.; Thornell, M.; D’Souza, L. A health impact assessment on the construction phase of a major hospital redevelopment. Aust. Health Rev. 2008, 32, 509–519. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.Y.; Jeon, S.Y.; Jeon, M.J.; Lee, K.-H.; Lee, S.G.; Kim, D.; Kang, E.; Bae, S.-G.; Kim, J. Health impact assessment of free immunization program in Jinju City, Korea. J. Prev. Med. Public Health 2012, 45, 267–275. [Google Scholar] [CrossRef] [Green Version]
- Fell, G.; Haroon, S. Learning from a Rapid Health Impact Assessment of a proposed maternity service reconfiguration in the English NHS. BMC Public Health 2008, 8, 138. [Google Scholar] [CrossRef] [Green Version]
- Douglas, C.H.; Higgins, A.; Dabbs, C.; Walbank, M. Health impact assessment for the sustainable futures of Salford. J. Epidemiol. Community Health 2004, 58, 642–648. [Google Scholar] [CrossRef] [Green Version]
- Ali, S.; O’Callaghan, V.; Middleton, J.; Little, R. A prospective mini health impact assessment of the ’Towards 2010’ programme in Sandwell and West Birmingham in the West Midlands. Public Health 2007, 121, 469–481. [Google Scholar] [CrossRef]
- Bendel, N.; Owen-Smith, V. A prospective health impact review of the redevelopment of Central Manchester Hospitals. Environ. Impact Assess. Rev. 2005, 25, 783–790. [Google Scholar] [CrossRef]
- Maxwell, M.L. A health impact assessment of the Liverpool Hospital redevelopment. N. S. W. Public Health Bull. 2007, 18, 172–173. [Google Scholar] [CrossRef] [Green Version]
- Australian Indigenous Doctors’ Association; University of New South Wales Centre for Health Equity Training, Research and Evaluation. Health Impact Assessment of the Northern Territory Emergency Response; Australian Indigenous Doctors’ Association: Canberra, Australia, 2010. [Google Scholar]
- O’Hara, B.; Hughes, J.; Kehoe, P.; Baird, H.; Milham, T.; Hills, S. The Health Impact Assessment Statement on the NSW Integrated Chronic Disease Prevention Campaign; NSW Health: Sydney, Australia, 2004. [Google Scholar]
- Cooke, A.; Benson, K.; Snowden, L.; Bowman, A. West Stockwell Primary Health and Community Resource Centre A Health Impact Assessment; West Stockwell Primary Care and Community Resource Centre: London, UK, 2004. [Google Scholar]
- Ardem, K. Rapid Health Impact Assessment of the Private Finance Initiative Proposal “Modernising Healthcare for a deprived Community”; South Liverpool Primary Care Trust: Liverpool, UK, 2003. [Google Scholar]
- Abrahams, D.; Pennington, A. A Rapid Health Impact Assessment of „Our Health, Our Care, Our Say‟ on Young Carers; University of Liverpool: Liverpool, UK, 2008. [Google Scholar]
- Shepherd, M. Report of the Health Impact Assessment of Proposed Changes to Mental Health Services in Cardiff and the Vale of Glamorgan; Cardiff Institute of Society and Health: Cardiff, UK, 2011. [Google Scholar]
- NSW Health. Future Directions for Health Promotion; Mid Western Health Service: Melbourne, Australia, 2008. [Google Scholar]
- Critchley, S. Report on Rapid Health Impact Assessment of CADMHAS; Cardiff Institute of Society Health and Ethics: Cardiff, UK, 2007. [Google Scholar]
- Neumayer, B.; Chapman, J.; Haberecht, R. Reviewing a Rural Health Service Redesign Proposal Using the Health Impact Assessment (HIA) Process; Greater Southern Area Health Service: Cooma, Australia, 2004. [Google Scholar]
- Atkinson, P.; Cooke, A.; Benson, B. The Dulwich WellBeing Centre: A Health Impact Assessment; Dulwich Wellbeing Centre: London, UK, 2003. [Google Scholar]
- Rattle, R. Health Impact Assessment, Municipal Development Practices and Children’s Health. Int. J. Child Youth Fam. Stud. 2015, 6, 308–327. [Google Scholar] [CrossRef] [Green Version]
- Aboagye, D.-C.; Akuffo, K.; Khan, H. Community Health Impact Assessment in Ghana: Contemporary Concepts and Practical Methods. Inq. J. Med. Care Organ. Provis. Financ. 2019, 56, 46958019845292. [Google Scholar] [CrossRef]
- Critical Appraisal Skills Programme. Qualitative Research Checklist, in Critical Appraisal Skills Programme (CASP); Critical Appraisal Skills Programme: Oxford, UK, 2012. [Google Scholar]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Woolf, S.; Schünemann, H.J.; Eccles, M.P.; Grimshaw, J.M.; Shekelle, P. Developing clinical practice guidelines: Types of evidence and outcomes; values and economics, synthesis, grading, and presentation and deriving recommendations. Implement. Sci. 2012, 7, 61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Titler, M.G. Nursing Science and Evidence-Based Practice. West. J. Nurs. Res. 2011, 33, 291–295. [Google Scholar] [CrossRef]
- Harris-Roxas, B.F.; Harris, P.J. Learning by doing: The value of case studies of health impact assessment. N. S. W. Public Health Bull. 2007, 18, 161–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Erlanger, T.E.; Krieger, G.R.; Singer, B.H.; Utzinger, J. The 6/94 gap in health impact assessment. Environ. Impact Assess. Rev. 2008, 28, 349–358. [Google Scholar] [CrossRef]
- Hirani, V.; Tull, K.; Ali, A.; Mindell, J. Urgent action needed to improve vitamin D status among older people in England! Age Ageing 2010, 39, 62–68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dwyer, J.M. Australian health system restructuring—What problem is being solved? Aust. N. Z. Health Policy 2004, 1, 6. [Google Scholar] [CrossRef] [Green Version]
- Elwyn, G.; Frosch, D.; Thomson, R.; Joseph-Williams, N.; Lloyd, A.; Kinnersley, P.; Cording, E.; Tomson, D.; Dodd, C.; Rollnick, S.; et al. Shared Decision Making: A Model for Clinical Practice. J. Gen. Intern. Med. 2012, 27, 1361–1367. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; E McKenzie, J.; Kirkham, J.; Dwan, K.; Kramer, S.; Green, S.; Forbes, A. Bias due to selective inclusion and reporting of outcomes and analyses in systematic reviews of randomised trials of healthcare interventions. Cochrane Database Syst. Rev. 2014, 2015, MR000035. [Google Scholar] [CrossRef] [PubMed]
- Public Health Agency of Canada. Promote and Protect the Health of Canadians through Leadership, Partnership, Innovation and Action in Public Health. In Toward Health Equity: Canadian Approaches to the Health Sector Role; Public Health Agency of Canada: Ottawa, ON, Canada, 2014. [Google Scholar]
- Bhatia, R.; Farhang, L.; Heller, J.; Lee, M.; Orenstein, M.; Richardson, M.; Wernham, A. Minimum Elements and Practice Standards for Health Impact Assessment; Version 3. 2014. Available online: https://www.tn.gov/content/dam/tn/health/documents/learningopportunities/HIA_Best_Practice_Standards_2014.pdf (accessed on 25 October 2021).
- Fredsgaard, M.W.; Cave, B.; Bond, A. A Review Package for Health Impact Assessment Reports of Development Projects; Ben Cave Associates Ltd.: Leeds, UK, 2009. [Google Scholar]
- Harris, E.; Sainsbury, P.; Simpson, S.; Harris-Roxas, B. Addressing The Societal Determinants of Health: Investing in a Sustainable Health System; Centre for Health Equity Training Research and Evaluation: Sydney, Australia, 2013. [Google Scholar]
- Kumar, S.; Kumar, N.; Vivekadhish, S. Millennium Development Goals (MDGs) to Sustainable Development Goals (SDGs): Addressing Unfinished Agenda and Strengthening Sustainable Development and Partnership. Indian J. Community Med. 2016, 41, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Gilson, L.; Doherty, J.; Lowenson, R.; Francis, V. Challenging inequity through health systems: Final report of the Knowledge Network on health systems. In WHO Commission on the Social Determinants of Health; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Winkler, M.S.; Krieger, G.R.; Divall, M.J.; Cissé, G.; Wielga, M.; Singer, B.H.; Tanner, M.; Utzinger, J. Untapped potential of health impact assessment. Bull. World Health Organ. 2013, 91, 298–305. [Google Scholar] [CrossRef]
- Byambaa, T.; Jones, C.; Davison, C. Challenges of Building Health Impact Assessment Capacity in Developing Countries: A Review. Columbia Univ. J. Glob. Health 2014, 2, 5–8. [Google Scholar]



{kind=link}
{kind=link}
| Author and Title | Year | Country | Nature | Levels of HIA | Method | Objective | Outcome | Source |
|---|---|---|---|---|---|---|---|---|
| A health impact assessment on the construction phase of a major hospital redevelopment [35] (Maxwell et al.) | 2008 | Australia | Project- | Intermediate | -Literature Review -Consultation -Interviews | To provide a recommendation to hospital planners on how to minimize potential negative impacts and increase the positive impacts | Suggested creation of an asbestos removal strategy Recommended creation of a position that could facilitate the transition of the redevelopment process and management of certain requirements for the contractors’ contract. Example use of effective safety barrier | Database |
| Health impact assessment of free immunization program in Jinju City, Korea [36] (Kim et al.) | 2012 | Korea | Program- | Rapid | -Literature Review -Case Studies -Geographical information systems analysis -Questionnaire -Expert consultations | To evaluate the potential health impacts and identify the best way to improve the quality of the free immunizations by increasing gains and decreasing the risk | Separate recommendations were provided for both the private clinics and public health centres on reorientation of roles, management, development of better strategies, training, collaboration, and establishment of monitoring systems | Database |
| Learning from a Rapid Health Impact Assessment of a proposed maternity service reconfiguration in the English NHS [37] (Fell and Haroon.) | 2008 | United Kingdom | Proposal- | Rapid Desktop | -Published literature review -Cohort study of hospital study | To enable PCT and the Hospital Trust Board to evaluate the potential consequences of reconfigurations to access to maternal services, maternal and infant health amongst different socio-economic groups | The proposal showed the ability to reduce inequalities, which would be influenced by the saving attained through reconfiguration. Recommendations also ensured that the proposal went hand in hand with the government requirements with the implementation of a few strategies | Database |
| Health impact assessment for the sustainable futures of Salford [38] (Douglas et al.) | 2004 | United Kingdom | Project- | Comprehensive | -Interviews -Meetings -Published secondary sources | To provide quality services to patients and promote easy access to care and ensure personalized 24 h integrated health and social care. | Recommendations were made to the partnership between LIFT and SHIFT to explore and expand their operational definition of health. The community definition of health was wider than the medical and clinical perspective and was mainly based on healthy living and wellbeing | Database |
| A prospective mini health impact assessment of the ‘Towards 2010’ program in Sandwell and West Birmingham in the West Midlands [39] (Ali et al.) | 2007 | United Kingdom | Program- | Desktop Rapid | -Published literature -Professional knowledge | To identify and inform the Board on the most beneficial options of the program for the local population | Of the four evaluated options, two of them showed potential for maximum health benefits in health and wellbeing improvement Option A would improve existing facilities though has limited potential for a whole system approach Option B would improve both existing facilities and bring services closer to the community Options C and D had the highest potential for a whole system change with a broader linkage to regeneration initiatives | Database |
| A prospective health impact review of the redevelopment of Central Manchester Hospitals [40] (Bendel and Owen-Smith.) | 2005 | United Kingdom | Project- | Rapid | -In-depth discussions with key individuals | To ensure the social determinants of health had been considered. To identity and give recommendations for areas that needed to be improved to promote overall health impact To provide a pilot study that would be utilized across the Greater Manchester | Recommendations were made regarding the construction and design of the building, issues on the design and construction phase, and general issues that impact the wider community. Example of these issues included parks, riding facilities, housing, crime, and extreme weather conditions | Database |
| A health impact assessment of the Liverpool Hospital redevelopment [41] (Maxwell.) | 2007 | Australia | Project- | Intermediate | -Literature Review -Key Interviews -Population Profile | To evaluate the health impacts of the project on the community, patients, and their families | The recommendations were made in terms of the priority of the health impacts. The issues were prioritized as follows: reduced parking, health and wellbeing, community and patient safety and increased traffic, | Database/Grey literature |
| Health Impact Assessment of the Northern Territory Emergency Response [42] (Australian Indigenous Doctor’s Association and Centre for Health Equity Training) | 2010 | Australia | Project- | Comprehensive | -Legislative analysis -Community consultations -Community profile -Expert review | To identify potential positive, negative, and unpredicted health impacts of the Northern Territory Emergency Response | The issues identified to have potential health impacts included: external leadership, Education, governance and control, housing, prohibited materials, children health, and income and alcohol restrictions Recommendations were made to either be stopped, unlikely potential to be effective in the long run, or the option to proceed with caution | Grey literature |
| The Health Impact Assessment Statement on the NSW Integrated Chronic Disease Prevention Campaign [43] (O’Hara B.) | 2004 | Australia | Proposal- | Intermediate | -Community profile -Literature review and Exploration of themes -Expert opinion and key informant interviews -Focus group discussions | To provide information that could be utilized to better the proposal and enhance the positive impacts while at the same time decreasing the negative impacts | Recommendations were made relating to various components of the campaign: mass media communication, branding, public relations, community support, promotion of appropriate referral point and appropriate, accessible information and merchandise | Grey literature |
| West-Stockwell Primary Health and Community Resource Centre A Health Impact Assessment [44] (Cooke and Bowman.) | 2004 | United Kingdom | Project- | Rapid | -Community-based sessions -Interviews -Published literature | To provide recommendations on how to mitigate short term negative impacts on health and assist West Stockwell Partners Board in decision making | The recommendations were made in terms of service provision, safety, communication, communication development, community space provision, and means of easily manoeuvring around | Grey literature |
| Rapid Health Impact Assessment of the Private Finance Initiative Proposal “Modernising Healthcare for a deprived Community” [45] (Ardem.) | 2003 | United Kingdom | Proposal- | Rapid | Unclear | To measure potential health outcomes of the proposal against social gains and sustainable financial support | Recommendations were made for readjustment and modification in the development phases to improve the potential health outcome | Grey literature |
| A Rapid Health Impact Assessment of “Our Health, Our Care, Our Say” on Young Carers [46] (Abrahams and Pennington.) | 2008 | United Kingdom | Policy- | Rapid | -Secondary sources -Published literature -Interviews -Focus groups | To inform decision making during the policy planning process by illustrating the health implications of the policy | The policy illustrated potential opportunities to promote systems improvements, increase available resources and support the younger population and their families. On the other hand, it opened a chance for the introduction of drivers promoting the status of young carers and opportunities to increase their visibility across health and social care services through various recommendations made | Grey literature |
| Report of the Health Impact Assessment of Proposed Changes to Mental Health Services [47] (Shepherd.) | 2011 | United Kingdom | Proposal- | Rapid | -Consultations -Literature review -Workshops | To inform the Board on the strengths and weaknesses of their proposal to make reforms and aid in decision making | Results showed the presence of an opportunity for the Board to develop a good relationship between itself and the community to address the various concerns presented and those that may emerge such as stigmatization and assumptions made to maximize health benefits. | Grey literature |
| Future Directions for Health Promotion. 2008, Mid-Western Health Service [48] (NSW Health) | 2008 | Australia | Proposal- | Rapid | -Literature review -Geographic patches -Surveys -Interviews | To identify whether the changes would have any positive impact or unpredictable consequences to the communities in MWAHS and offer recommendations for improvement. | Strategic approach recommendations were made focusing on the development of the workforce, prioritizing plans and policy on equity issues, targeting the vulnerable communities, and ensuring a supportive infrastructure at the local level | Grey literature |
| Report on Rapid Health Impact Assessment of CADMHAS [49] (Critchley et al.) | 2007 | United Kingdom | Program- | Rapid | -Participatory workshop | To ensure that the positive health benefits were maximized, and the negative impacts are highly decreased for the health and wellbeing of the population | Recommendations to improve health and wellbeing and reduce the inequalities within the community through CADMHAS were made through service delivery.The implementation was highly dependent on the amount of funding the proposal received. | Grey literature |
| Reviewing a Rural Health service Redesign Proposal Using the Health Impact Assessment (HIA) Process [50] (Neumayer.) | 2004 | Australia | Proposal- | Rapid | -Community profile -Literature review -Scenario Approach -Cost–benefit analysis | To identify the consequences of the proposal in terms of quality of service, access, availability, and the workforce | Recommendations were made to support the reconfiguration of the existing services against the model of no change to current existing services | Grey literature |
| The Dulwich WellBeing Centre… a Health Impact Assessment [51] (Atkinson et al.) | 2003 | United Kingdom | Project- | Rapid | -Literature review -Community profile -Community-based discussions -Workshops -Previous research conducted as preliminary thinking of the project -Mapping of older people’s services | To provide information that could be utilized to strengthen and improve health opportunities and capture the views of the community and their support | Both short term and long-term recommendations were identified since the results indicated the need for a more holistic model which embraces the concept of wellbeing. The centre would provide a sense of ownership and identity for the community other than just delivery of services or a physical space | Grey literature |
| Health Impact Assessment, Municipal Development Practices, And Children’s Health [52] (Rattle.) | 2015 | Canada | Project- | Rapid Desk-based | -Limited discussion | To identify and evaluate the impacts of the project, to recommend ways to mitigate the impacts, and to inform future policies makers and program development of any similar nature that may be undertaken | Different populations were affected differently. The immediate community was advantaged from easy access to health services thus improved health. On the other hand, residents, those attending school and work around the area would be faced with increased traffic, air pollution, noise, decreased green space as well as stress. | Database |
| Community Health Impact Assessment in Ghana: Contemporary Concepts and practical methods [53] | 2019 | Ghana | Policy | Desktop | -Focus group discussion, -Key informant interviews -literature review. | To identify the impact and influence of the NHIS policy on health and the type of influence on the population. | Not discussed. Article focused and discussed processes and methods utilized in the HIA. | Database |
| Setting for HIAs | Number of HIAs | Definition of Terms and Examples |
|---|---|---|
| Projects | 8 | Project in the HIAs was used to refer to a specific activity that was undertaken in a specified location. Projects included focused on issues such as a construction phase of Manchester hospital in the United Kingdom [40], redevelopment of Liverpool Hospital in Australia [41] and assessment of the Northern Territory Emergency [42]. |
| Proposals | 6 | Proposals referred to all formal plans that were put forward for consideration for future implementation [13]. Proposals focused on redesigning rural health services, health promotions [48] and changes to mental health services [47] amongst others. |
| Programs | 3 | A program was described as a set of related activities that eventually give effect to the policy [13]. The programs reviewed addressed issues such as free immunization in Korea and chronic disease prevention campaign in Australia [36,43]. |
| Policies | 2 | Policy, contrary to proposals and projects referred to how an organization or the government aims to achieve a set of objectives. The policy subject to HIA conducted in the United Kingdom dealt with the health of the young populations and opportunities available for improvements of their health and that of their families [46] while the one in Ghana focused on Ghana’s National Health Insurance Scheme [53]. |
| Number of HIAs | Focus of HIAs | Examples |
|---|---|---|
| 12 | Service and service reconfiguration | The services and service reconfiguration aspects included: free immunization, maternity service, chronic disease prevention, primary health care, health care for vulnerable communities, youth and young carers service, mental health, mental health advocacy, national health insurance scheme, and rural health service reconfiguration of the HIAs [36,37,39,42,43,46,47,48,49,50,52,53]. |
| 7 | Physical | The HIAs that assessed proposed physical changes to the health system focused on reconstruction, redevelopment, and development of hospitals about the HIAs [35,38,40,41,44,45,51]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wanjohi, N.W.; Harrison, R.; Harris-Roxas, B. Health Impact Assessments of Health Sector Proposals: An Audit and Narrative Synthesis. Int. J. Environ. Res. Public Health 2021, 18, 11466. https://doi.org/10.3390/ijerph182111466
Wanjohi NW, Harrison R, Harris-Roxas B. Health Impact Assessments of Health Sector Proposals: An Audit and Narrative Synthesis. International Journal of Environmental Research and Public Health. 2021; 18(21):11466. https://doi.org/10.3390/ijerph182111466
Chicago/Turabian StyleWanjohi, Nelius Wanjiku, Reema Harrison, and Ben Harris-Roxas. 2021. "Health Impact Assessments of Health Sector Proposals: An Audit and Narrative Synthesis" International Journal of Environmental Research and Public Health 18, no. 21: 11466. https://doi.org/10.3390/ijerph182111466