
Diagnostic Accuracy of SARS-CoV-2 Antigen Tests for Community Transmission Screening: A Systematic Review and Meta-Analysis

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
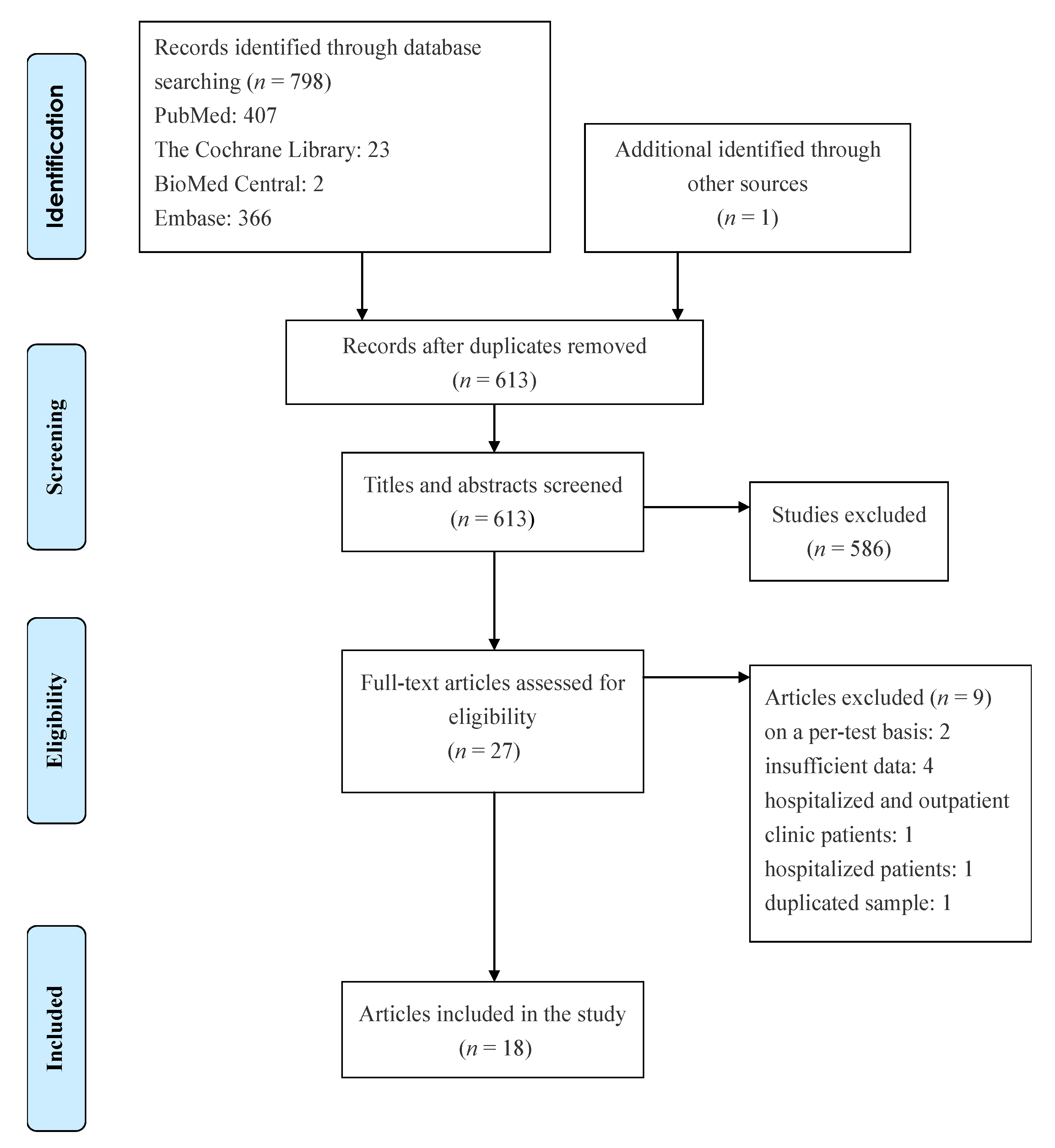
2.1. Literature Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Quality Assessment
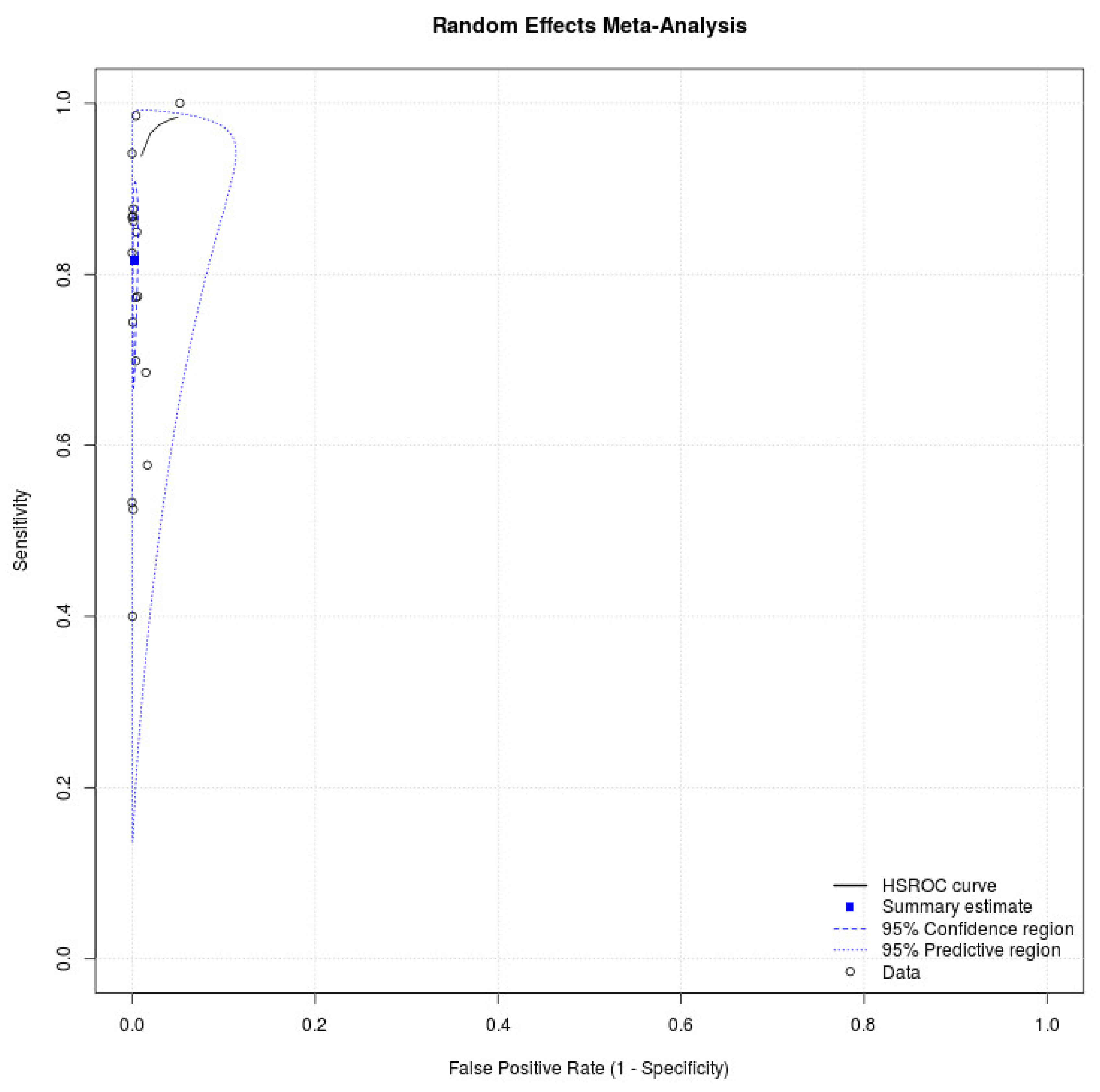
2.4. Statistical Analysis
3. Results
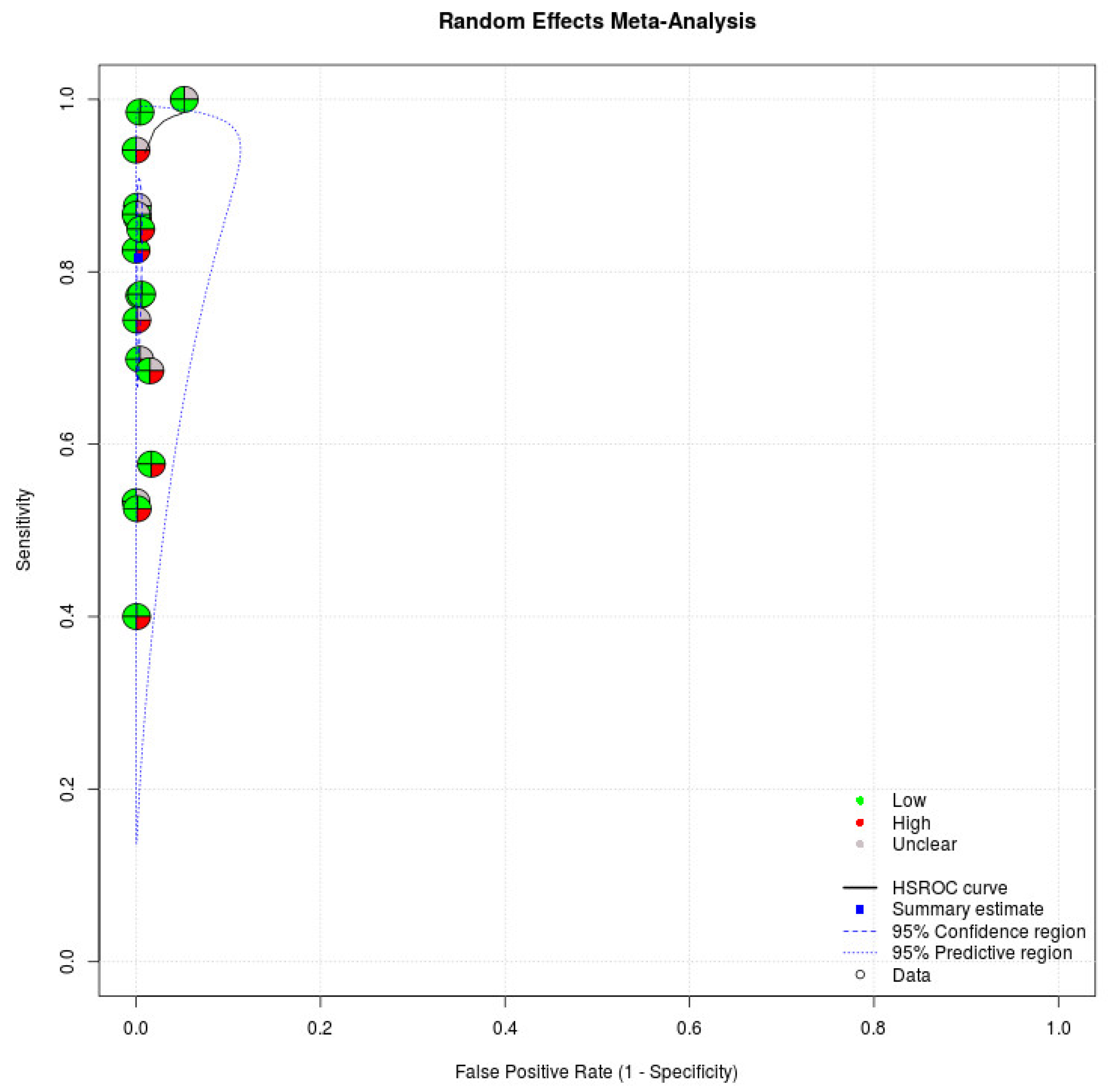
3.1. Quality Assessment
3.2. Investigation of Heterogeneity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johansson, M.A.; Quandelacy, T.M.; Kada, S.; Prasad, P.V.; Steele, M.; Brooks, J.T.; Slayton, R.B.; Biggerstaff, M.; Butler, J.C. SARS-CoV-2 Transmission From People Without COVID-19 Symptoms. JAMA Netw. Open 2021, 4, e2035057. [Google Scholar] [CrossRef]
- Liu, Y.; Morgenstern, C.; Kelly, J.; Lowe, R.; CMMID COVID-19 Working Group; Jit, M. The impact of non-pharmaceutical interventions on SARS-CoV-2 transmission across 130 countries and territories. BMC Med. 2021, 19, 40. [Google Scholar] [CrossRef]
- Oran, D.P.; Topol, E.J. Prevalence of Asymptomatic SARS-CoV-2 Infection: A Narrative Review. Ann. Intern. Med. 2020, 173, 362–367. [Google Scholar] [CrossRef]
- Watson, J.; Whiting, P.F.; Brush, J.E. Interpreting a COVID-19 test result. BMJ 2020, 369, m1808. [Google Scholar] [CrossRef] [PubMed]
- Lieberman, J.A.; Pepper, G.; Naccache, S.N.; Huang, M.L.; Jerome, K.R.; Greninger, A.L. Comparison of Commercially Available and Laboratory-Developed Assays for In Vitro Detection of SARS-CoV-2 in Clinical Laboratories. J. Clin. Microbiol. 2020, 58, e00821-20. [Google Scholar] [CrossRef] [PubMed]
- Toptan, T.; Eckermann, L.; Pfeiffer, A.E.; Hoehl, S.; Ciesek, S.; Drosten, C.; Corman, V.M. Evaluation of a SARS-CoV-2 rapid antigen test: Potential to help reduce community spread? J. Clin. Virol. 2021, 135, 104713. [Google Scholar] [CrossRef] [PubMed]
- Interim Guidance for Antigen Testing for SARS-CoV-2. Available online: https://www.cdc.gov/coronavirus/2019-ncov/lab/resources/antigen-tests-guidelines.html (accessed on 20 June 2021).
- Pray, I.W.; Ford, L.; Cole, D.; Lee, C.; Bigouette, J.P.; Abedi, G.R.; Bushman, D.; Delahoy, M.J.; Currie, D.; Cherney, B.; et al. Performance of an Antigen-Based Test for Asymptomatic and Symptomatic SARS-CoV-2 Testing at Two University Campuses—Wisconsin, September–October 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 69, 1642–1647. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Olliaro, P.L.; Boeras, D.I.; Fongwen, N. Scaling up COVID-19 rapid antigen tests: Promises and challenges. Lancet Infect. Dis. 2021, 21, e290–e295. [Google Scholar] [CrossRef]
- McInnes, M.D.F.; Moher, D.; Thombs, B.D.; McGrath, T.A.; Bossuyt, P.M.; the PRISMA-DTA Group; Clifford, T.; Cohen, J.F.; Deeks, J.J.; Gatsonis, C.; et al. Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: The PRISMA-DTA Statement. JAMA 2018, 319, 388–396. [Google Scholar] [CrossRef]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef]
- Takwoingi, Y.; Riley, R.D.; Deeks, J.J. Meta-analysis of diagnostic accuracy studies in mental health. Evid. Based Ment. Health 2015, 18, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Chartrand, C.; Leeflang, M.M.; Minion, J.; Brewer, T.; Pai, M. Accuracy of rapid influenza diagnostic tests: A meta-analysis. Ann. Intern. Med. 2012, 156, 500–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zamora, J.; Abraira, V.; Muriel, A.; Khan, K.; Coomarasamy, A. Meta-DiSc: A software for meta-analysis of test accuracy data. BMC Med. Res. Methodol. 2006, 6, 31. [Google Scholar] [CrossRef]
- Freeman, S.C.; Kerby, C.R.; Patel, A.; Cooper, N.J.; Quinn, T.; Sutton, A.J. Development of an interactive web-based tool to conduct and interrogate meta-analysis of diagnostic test accuracy studies: MetaDTA. BMC Med. Res. Methodol. 2019, 19, 81. [Google Scholar] [CrossRef] [PubMed]
- Pollock, N.R.; Tran, K.; Jacobs, J.R.; Cranston, A.E.; Smith, S.; O’Kane, C.Y.; Roady, T.J.; Moran, A.; Scarry, A.; Carroll, M.; et al. Performance and Operational Evaluation of the Access Bio CareStart Rapid Antigen Test in a High-Throughput Drive-Through Community Testing Site in Massachusetts. Open Forum. Infect. Dis. 2021, 8, ofab243. [Google Scholar] [CrossRef]
- García-Fiñana, M.; Hughes, D.M.; Cheyne, C.P.; Burnside, G.; Stockbridge, M.; Fowler, T.A.; Fowler, V.L.; Wilcox, M.H.; Semple, M.G.; Buchan, I. Performance of the Innova SARS-CoV-2 antigen rapid lateral flow test in the Liverpool asymptomatic testing pilot: Population based cohort study. BMJ 2021, 374, n1637. [Google Scholar] [CrossRef]
- Lindner, A.K.; Nikolai, O.; Rohardt, C.; Kausch, F.; Wintel, M.; Gertler, M.; Burock, S.; Hörig, M.; Bernhard, J.; Tobian, F.; et al. Diagnostic accuracy and feasibility of patient self-testing with a SARS-CoV-2 antigen-detecting rapid test. J. Clin. Virol. 2021, 141, 104874. [Google Scholar] [CrossRef]
- Krüger, L.J.; Gaeddert, M.; Tobian, F.; Lainati, F.; Gottschalk, C.; Klein, J.A.F.; Schnitzler, P.; Kräusslich, H.G.; Nikolai, O.; Lindner, A.K.; et al. The Abbott PanBio WHO emergency use listed, rapid, antigen-detecting point-of-care diagnostic test for SARS-CoV-2-Evaluation of the accuracy and ease-of-use. PLoS ONE 2021, 16, e0247918. [Google Scholar] [CrossRef]
- Van der Moeren, N.; Zwart, V.F.; Lodder, E.B.; Van den Bijllaardt, W.; Van Esch, H.R.J.M.; Stohr, J.J.J.M.; Pot, J.; Welschen, I.; Van Mechelen, P.M.F.; Pas, S.D.; et al. Evaluation of the test accuracy of a SARS-CoV-2 rapid antigen test in symptomatic community dwelling individuals in the Netherlands. PLoS ONE 2021, 16, e0250886. [Google Scholar]
- Peña, M.; Ampuero, M.; Garcés, C.; Gaggero, A.; García, P.; Velasquez, M.S.; Luza, R.; Alvarez, P.; Paredes, F.; Acevedo, J.; et al. Performance of SARS-CoV-2 rapid antigen test compared with real-time RT-PCR in asymptomatic individuals. Int. J. Infect. Dis. 2021, 107, 201–204. [Google Scholar] [CrossRef]
- Shah, M.M.; Salvatore, P.P.; Ford, L.; Kamitani, E.; Whaley, M.J.; Mitchell, K.; Currie, D.W.; Morgan, C.N.; Segaloff, H.E.; Lecher, S.; et al. Performance of Repeat BinaxNOW Severe Acute Respiratory Syndrome Coronavirus 2 Antigen Testing in a Community Setting, Wisconsin, November 2020–December 2020. Clin. Infect. Dis. 2021, 73, S54–S57. [Google Scholar] [CrossRef] [PubMed]
- Ford, L.; Lee, C.; Pray, I.W.; Cole, D.; Bigouette, J.P.; Abedi, G.R.; Bushman, D.; Delahoy, M.J.; Currie, D.W.; Cherney, B.; et al. Epidemiologic characteristics associated with SARS-CoV-2 antigen-based test results, rRT-PCR cycle threshold values, subgenomic RNA, and viral culture results from university testing. Clin. Infect. Dis. 2021, 73, e1348–e1355. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.; Nsoga, M.T.N.; Perez-Rodriguez, F.J.; Aad, Y.A.; Sattonnet-Roche, P.; Gayet-Ageron, A.; Jaksic, C.; Torriani, G.; Boehm, E.; Kronig, I.; et al. Diagnostic accuracy of two commercial SARS-CoV-2 antigen-detecting rapid tests at the point of care in community-based testing centers. PLoS ONE 2021, 16, e0248921. [Google Scholar] [CrossRef] [PubMed]
- Stokes, W.; Berenger, B.M.; Portnoy, D.; Scott, B.; Szelewicki, J.; Singh, T.; Venner, A.A.; Turnbull, L.; Pabbaraju, K.; Shokoples, S.; et al. Clinical performance of the Abbott Panbio with nasopharyngeal, throat, and saliva swabs among symptomatic individuals with COVID-19. Eur. J. Clin. Microbiol. Infect. Dis. 2021, 40, 1721–1726. [Google Scholar] [CrossRef] [PubMed]
- Takeuchi, Y.; Akashi, Y.; Kato, D.; Kuwahara, M.; Muramatsu, S.; Ueda, A.; Notake, S.; Nakamura, K.; Ishikawa, H.; Suzuki, H. The evaluation of a newly developed antigen test (QuickNavi™-COVID19 Ag) for SARS-CoV-2: A prospective observational study in Japan. J. Infect. Chemother. 2021, 27, 890–894. [Google Scholar] [CrossRef]
- Gili, A.; Paggi, R.; Russo, C.; Cenci, E.; Pietrella, D.; Graziani, A.; Stracci, F.; Mencacci, A. Evaluation of Lumipulse® G SARS-CoV-2 antigen assay automated test for detecting SARS-CoV-2 nucleocapsid protein (NP) in nasopharyngeal swabs for community and population screening. Int. J. Infect. Dis. 2021, 105, 391–396. [Google Scholar] [CrossRef]
- Pollock, N.R.; Jacobs, J.R.; Tran, K.; Cranston, A.E.; Smith, S.; O’Kane, C.Y.; Roady, T.J.; Moran, A.; Scarry, A.; Carroll, M.; et al. Performance and Implementation Evaluation of the Abbott BinaxNOW Rapid Antigen Test in a High-Throughput Drive-Through Community Testing Site in Massachusetts. J. Clin. Microbiol. 2021, 59, e00083-21. [Google Scholar] [CrossRef] [PubMed]
- Okoye, N.C.; Barker, A.P.; Curtis, K.; Orlandi, R.R.; Snavely, E.A.; Wright, C.; Hanson, K.E.; Pearson, L.N. Performance Characteristics of BinaxNOW COVID-19 Antigen Card for Screening Asymptomatic Individuals in a University Setting. J. Clin. Microbiol. 2021, 59, e03282-20. [Google Scholar] [CrossRef]
- Prince-Guerra, J.L.; Almendares, O.; Nolen, L.D.; Gunn, J.K.L.; Dale, A.P.; Buono, S.A.; Deutsch-Feldman, M.; Suppiah, S.; Hao, L.; Zeng, Y.; et al. Evaluation of Abbott BinaxNOW Rapid Antigen Test for SARS-CoV-2 Infection at Two Community-Based Testing Sites—Pima County, Arizona, 3–17 November 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Igloi, Z.; Velzing, J.; van Beek, J.; van de Vijver, D.; Aron, G.; Ensing, R.; Benschop, K.; Han, W.; Boelsums, T.; Koopmans, M.; et al. Clinical Evaluation of Roche SD Biosensor Rapid Antigen Test for SARS-CoV-2 in Municipal Health Service Testing Site, the Netherlands. Emerg. Infect. Dis. 2021, 27, 1323–1329. [Google Scholar] [CrossRef]
- Landaas, E.T.; Storm, M.L.; Tollånes, M.C.; Barlinn, R.; Kran, A.B.; Bragstad, K.; Christensen, A.; Andreassen, T. Diagnostic performance of a SARS-CoV-2 rapid antigen test in a large, Norwegian cohort. J. Clin. Virol. 2021, 137, 104789. [Google Scholar] [CrossRef] [PubMed]
- Pilarowski, G.; Marquez, C.; Rubio, L.; Peng, J.; Martinez, J.; Black, D.; Chamie, G.; Jones, D.; Jacobo, J.; Tulier-Laiwa, V.; et al. Field performance and public health response using the BinaxNOW TM Rapid SARS-CoV-2 antigen detection assay during community-based testing. Clin. Infect. Dis. 2020. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.; Thompson, S.G.; Deeks, J.J.; Altman, D.G. Measuring inconsistency in meta-analyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [Green Version]
- Baeyens, J.P.; Serrien, B.; Goossens, M.; Clijsen, R. Questioning the “SPIN and SNOUT” rule in clinical testing. Arch. Physiother. 2019, 9, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sethuraman, N.; Jeremiah, S.S.; Ryo, A. Interpreting Diagnostic Tests for SARS-CoV-2. JAMA 2020, 323, 2249–2251. [Google Scholar] [CrossRef] [PubMed]
- Mina, M.J.; Parker, R.; Larremore, D.B. Rethinking COVID-19 Test Sensitivity—A Strategy for Containment. N. Engl. J. Med. 2020, 383, e120. [Google Scholar] [CrossRef]
- Van der Toorn, W.; Oh, D.Y.; Bourquain, D.; Michel, J.; Krause, E.; Nitsche, A.; von Kleist, M.; Working Group on SARS-CoV-2 Diagnostics at RKI. An intra-host SARS-CoV-2 dynamics model to assess testing and quarantine strategies for incoming travelers, contact management, and de-isolation. Patterns 2021, 2, 100262. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.; Hill, E.M.; Tildesley, M.J.; Dyson, L.; Keeling, M.J. Vaccination and non-pharmaceutical interventions for COVID-19: A mathematical modelling study. Lancet Infect. Dis. 2021, 21, 793–802. [Google Scholar] [CrossRef]
- Bhopal, R.S. COVID-19 zugzwang: Potential public health moves towards population (herd) immunity. Public Health Pract. 2020, 1, 100031. [Google Scholar] [CrossRef]
- Vandenberg, O.; Martiny, D.; Rochas, O.; van Belkum, A.; Kozlakidis, Z. Considerations for diagnostic COVID-19 tests. Nat. Rev. Microbiol. 2021, 19, 171–183. [Google Scholar] [CrossRef]
- Options for the Use of Rapid Antigen Tests for COVID-19 in the EU/EEA and the UK. Available online: https://www.ecdc.europa.eu/en/publications-data/options-use-rapid-antigen-tests-COVID-19-eueea-and-uk (accessed on 20 June 2021).
- WHO. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection Using Rapid Immunoassays: Interim Guidance. Available online: https://www.who.int/publications/i/item/antigen-detection-in-the-diagnosis-of-SARS-CoV-2infection-using-rapid-immunoassays (accessed on 20 June 2021).
- Quilty, B.J.; Clifford, S.; Hellewell, J.; Russell, T.W.; Kucharski, A.J.; Flasche, S.; Edmunds, W.J.; Centre for the Mathematical Modelling of Infectious Diseases COVID-19 Working Group. Quarantine and testing strategies in contact tracing for SARS-CoV-2: A modelling study. Lancet Public Health 2021, 6, e175–e183. [Google Scholar] [CrossRef]
- Chow, A.; Htun, H.L.; Kyaw, W.M.; Lee, L.T.; Ang, B. Asymptomatic health-care worker screening during the COVID-19 pandemic. Lancet 2020, 396, 1393–1394. [Google Scholar] [CrossRef]
- Crozier, A.; Rajan, S.; Buchan, I.; McKee, M. Put to the test: Use of rapid testing technologies for COVID-19. BMJ 2021, 372, n208. [Google Scholar] [CrossRef] [PubMed]
- Mercer, T.R.; Salit, M. Testing at scale during the COVID-19 pandemic. Nat. Rev. Genet. 2021, 22, 415–426. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, G.; Mancini, P.; Bonanno Ferraro, G.; Veneri, C.; Iaconelli, M.; Lucentini, L.; Bonadonna, L.; Brusaferro, S.; Brandtner, D.; Fasanella, A.; et al. Rapid screening for SARS-CoV-2 variants of concern in clinical and environmental samples using nested RT-PCR assays targeting key mutations of the spike protein. Water Res. 2021, 197, 117104. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Study Design | Testing Site | Patient Population | Prevalence (%) | Participants (Total/Data Extraction) | Age Median (Range) | Days After Symptom Onset Median (Range) | Specimen Type | Index Tests | Reference Standard | Ct Value of Positive RT-PCR Median (Range) | Threshold Value (Ct) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pollock NR [16] 2021 | Prospective | Drive-through testing site | Asymptomatic and symptomatic | 15.6 | (1063/1498) | NA | adult: 3 (0–44) children: 3 (1–20) | Anterior nasal swab | Access Bio CareStart COVID-19 Antigen test | RT-PCR | NA | ≤25, ≤30, ≤35 |
| García-Fiñana M [17] 2021 | Prospective, cross sectional, consecutive | Community testing sites | Asymptomatic | 1.3 | (5869/5504) | 50 (mean) (±18, SD) | NA | Self-administered swabs (combined throat and nose) | Innova lateral flow test | RT-PCR | NA | NA |
| Lindner AK [18] 2021 | Prospective, consecutive | Ambulatory SARS-CoV-2 testing facility | Symptomatic | NA | (168/144) | 35 (mean) (±11.5, SD) | 3.4 (mean) (±2.0, SD) | Nasal swab (self-sampling) | STANDARD Q COVID-19 Ag Test | RT-PCR | NA | NA |
| Krüger LJ [19] 2021 | Prospective | Drive-in testing site, clinical ambulatory testing facility | Asymptomatic and symptomatic | NA | (1261/1108) | 39.4 (mean) (±14.1, SD) | 4.01 (mean) (±3.1, SD) | Nasopharyngeal swab, oropharyngeal swab | Panbio COVID-19 Ag Rapid Test Device, immunochro-matography | RT-PCR | NA | NA |
| Van der Moeren N [20] 2021 | Prospective | COVID-19 test center | Symptomatic | 4.8 | (354/351) | NA | NA | Nose/throat swabs | BD Veritor System for Rapid Detection of SARS-CoV-2 | RT-PCR | NA | NA |
| Peña M [21] 2021 | Prospective | Public testing sites | Asymptomatic | 11 | (854/842) | 36.7 (mean) (±16.5, SD) | NA | Nasopharyngeal swab | STANDARD Q COVID-19 Ag Test | RT-PCR | NA | 40 |
| Shah MM [22] 2021 | Prospective | Community testing site | Asymptomatic and symptomatic | 15.8 | (2127/2110) the initial BinaxNOW test | NA | ≤7 | Nasal swab (self-sampling) | BinaxNOW COVID-19 Ag card | RT-PCR | NA | 37 |
| Ford L [23] 2021 | Prospective | Two universities | Asymptomatic and symptomatic | NA | (1058/1051) symptomatic: 219 asymptomatic: 832 | 15–24 (87.9%) ≥25 (12.1%) | NA | Nasal swabs | Sofia SARS Antigen, fluorescent immunoassay | RT-PCR | NA | 40 |
| Berger A [24] 2021 | Prospective | Community-based testing centers | Asymptomatic and symptomatic | NA | (1064/1064) | 34 (±12.5, SD) | NA | Nasopharyngeal swab | Panbio COVID-19 Ag Rapid Test Device, Standard Q COVID-19 Ag kit, | RT-PCR | 21.5 (14.2–34.2) | NA |
| Stokes W [25] 2021 | Prospective | Community COVID-19 assessment centers | Symptomatic | NA | (1641/1641) | 39 (5–90) | NA | Nasopharyngeal swab | Panbio COVID-19 Ag Rapid Test Device, immunochro-matography | RT-PCR | 22.1 (13.2–33.9), (E-gene) | 35 |
| Takeuchi Y [26] 2021 | Prospective | Drive-through-type at a PCR center | Asymptomatic and symptomatic | NA | (1186/1186) | 23 | 2 | Nasopharyngeal swab | QuickNavi™-COVID19 Ag | RT-PCR | NA | NA |
| Gili A [27] 2021 | Prospective | Schools, prisons, elderly care homes, and from hospital healthcare worker surveillance programs | NA | 5.2 | (1738/1738) | NA | NA | Nasopharyngeal swab | Lumipulse® SARS-CoV-2 antigen assay | RT-PCR | NA | 35 |
| Pollock NR [28] 2021 | Prospective | Drive-through testing site | Asymptomatic and symptomatic | 12.7 | (2308/2308) | all ages | 7 | Anterior nasal swab | BinaxNOW COVID-19 Ag card | RT-PCR | 26.9 (for adults, asymptomatic) 20.5 (for adults, symptomatic for ≤7 days) | 40 |
| Okoye NC [29] 2021 | Prospective | A university setting | Asymptomatic | 1.7 | (2645/2638) | 24 (mean) (15–86) | NA | Nasal swab | BinaxNOW COVID-19 Ag card | RT-PCR | 17.6 | NA |
| Prince-Guerra JL [30] 2021 | Prospective | Two community-based testing sites | Asymptomatic and symptomatic | 8.7 | (3419/3419) | 41 (10–95) | 4 (0–210) | Anterior nasal swab | BinaxNOW COVID-19 Ag card | RT-PCR | 22 (symptomatic) 22.5 (asymptomatic) | NA |
| Iglὁi Z 2021 [31] | Prospective | Drive-through testing location | Asymptomatic and symptomatic | 19.2 | (3615/970) symptomatic: 886 | 42 (18–86) | 4 | Nasopharyngeal swab | STANDARD Q COVID-19 Ag Test | RT-PCR | 23.6 (15.6–37.4), (E-gene) | NA |
| Landaas ET [32] 2021 | Prospective | test station | Asymptomatic and symptomatic | 6.3 | (4025/3991) | ≥10 | NA | Throat/nasopharyngeal swabs | Panbio COVID-19 Ag Rapid Test Device, immunochro-matography | RT-PCR | 24.5 (symptomatic) 28.2 (asymptomatic) | NA |
| Pilarowski G [33] 2020 | Prospective | at a plaza | Participants in an urban commercial transport hub | 7.2 | (3302/3302) | <13, 13–18, >18 | NA | Nasal swab | BinaxNOW™ COVID-19 Ag Card | RT-PCR | NA | 35 |
| Study | True Positive | False Positive | False Negative | True Negative |
|---|---|---|---|---|
| Pollock NR [16] 2021 | 135 | 21 | 99 | 1243 |
| García-Fiñana M [17] 2021 | 28 | 3 | 42 | 5431 |
| Lindner AK [18] 2021 | 33 | 0 | 7 | 104 |
| Krüger LJ [19] 2021 | 92 | 1 | 14 | 1001 |
| Van der Moeren N [20] 2021 | 16 | 0 | 1 | 334 |
| Peña M [21] 2021 | 51 | 3 | 22 | 766 |
| Shah MM [22] 2021 | 258 | 7 | 76 | 1769 |
| Ford L [23] 2021 | 37 | 15 | 17 | 982 |
| Berger A [24] 2021 | 276 | 1 | 39 | 748 |
| Stokes W [25] 2021 | 231 | 2 | 37 | 1371 |
| Takeuchi Y [26] 2021 | 91 | 0 | 14 | 1081 |
| Gili A [27] 2021 | 90 | 86 | 0 | 1562 |
| Pollock NR [28] 2021 | 226 | 12 | 66 | 2004 |
| Okoye NC [29] 2021 | 24 | 0 | 21 | 2593 |
| Prince-Guerra JL [30] 2021 | 157 | 4 | 142 | 3116 |
| Iglὁi Z [31] 2021 | 158 | 4 | 28 | 780 |
| Landaas ET [32] 2021 | 186 | 3 | 64 | 3738 |
| Pilarowski G [33] 2020 | 201 | 13 | 3 | 3085 |
| Study | Risk of Bias | Applicability Concerns | |||||
|---|---|---|---|---|---|---|---|
| Patient Selection | Index Test | Reference Standard | Flow and Timing | Patient Selection | Index Test | Reference Standard | |
| Pollock NR [16] 2021 | L | L | L | H | L | L | L |
| García-Fiñana M [17] 2021 | L | L | L | H | L | L | L |
| Lindner AK [18] 2021 | L | L | L | H | L | L | L |
| Krüger LJ [19] 2021 | L | L | L | H | L | L | L |
| Van der Moeren N [20] 2021 | U | L | L | H | L | L | L |
| Peña M [21] 2021 | U | L | L | H | L | L | L |
| Shah MM [22] 2021 | U | L | L | H | L | L | L |
| Ford L [23] 2021 | U | L | L | H | L | L | L |
| Berger A [24] 2021 | U | L | L | L | L | L | L |
| Stokes W [25] 2021 | U | L | L | H | L | L | L |
| Takeuchi Y [26] 2021 | U | L | L | L | H | L | L |
| Gili A [27] 2021 | U | L | L | L | L | L | L |
| Pollock NR [28] 2021 | L | L | L | L | L | L | L |
| Okoye NC [29] 2021 | U | L | L | H | L | L | L |
| Prince-Guerra JL [30] 2021 | L | L | L | H | L | L | L |
| Iglὁi Z [31] 2021 | L | L | L | H | L | L | L |
| Landaas ET [32] 2021 | U | L | L | H | L | L | L |
| Pilarowski G [33] 2020 | L | L | L | L | L | L | L |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-C.; Lu, S.-C.; Bai, C.-H.; Wang, P.-Y.; Lee, K.-Y.; Wang, Y.-H. Diagnostic Accuracy of SARS-CoV-2 Antigen Tests for Community Transmission Screening: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11451. https://doi.org/10.3390/ijerph182111451
Chen C-C, Lu S-C, Bai C-H, Wang P-Y, Lee K-Y, Wang Y-H. Diagnostic Accuracy of SARS-CoV-2 Antigen Tests for Community Transmission Screening: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2021; 18(21):11451. https://doi.org/10.3390/ijerph182111451
Chicago/Turabian StyleChen, Cheng-Chieh, Shou-Cheng Lu, Chyi-Huey Bai, Pei-Yu Wang, Kang-Yun Lee, and Yuan-Hung Wang. 2021. "Diagnostic Accuracy of SARS-CoV-2 Antigen Tests for Community Transmission Screening: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 18, no. 21: 11451. https://doi.org/10.3390/ijerph182111451