
Quality of Life, Needs and Fears of Mothers of Children with Disabilities in Saudi Arabia during the COVID-19 Lockdown


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
2.2. Questionnaire
2.2.1. Sociodemographic Characteristics
2.2.2. Quality of Life among Mothers
2.2.3. Mothers’ Needs and Fears
2.3. Ethical Considerations
2.4. Statistical Analysis
3. Results
3.1. Sociodemographic Characteristics
3.2. Quality of Life among Mothers
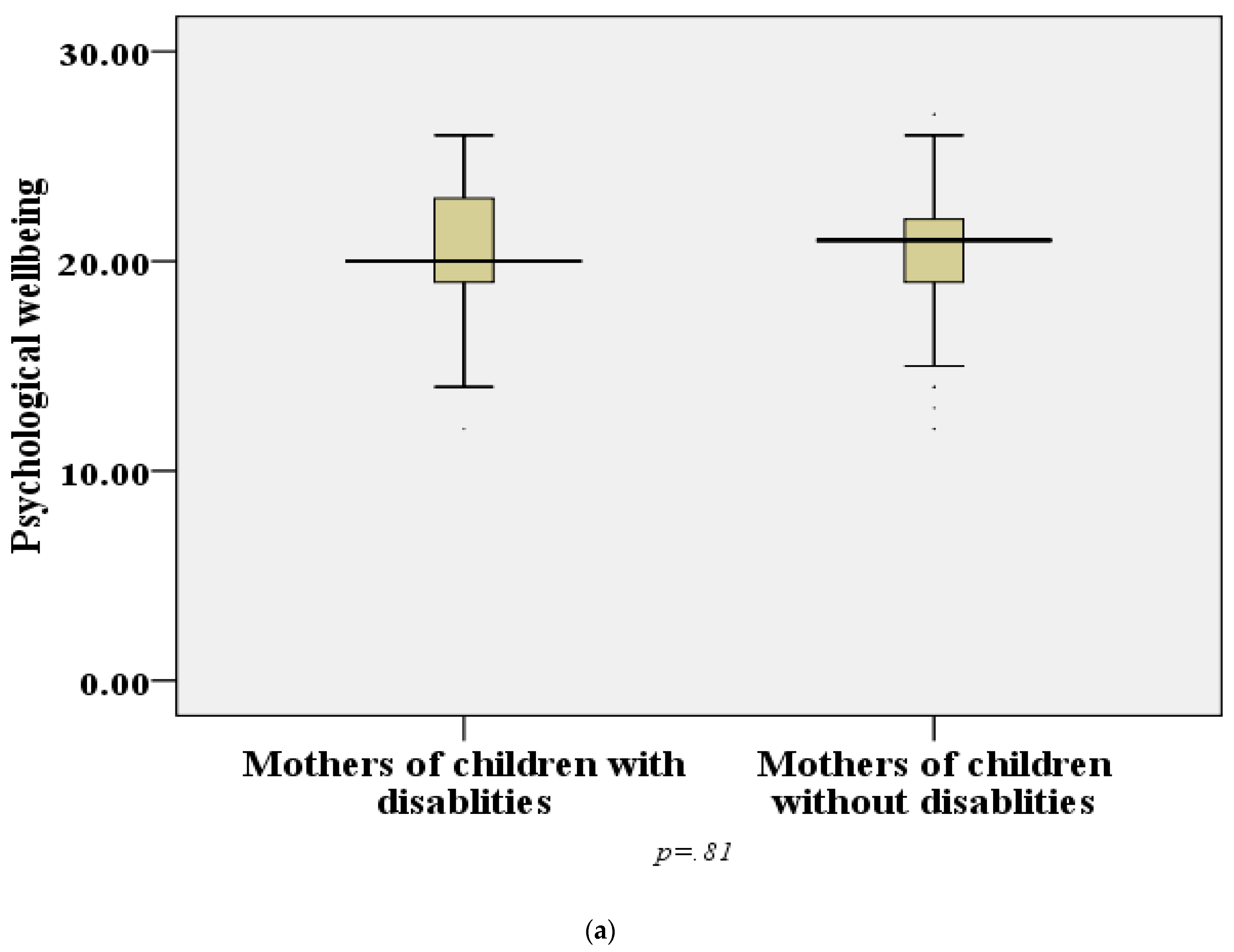
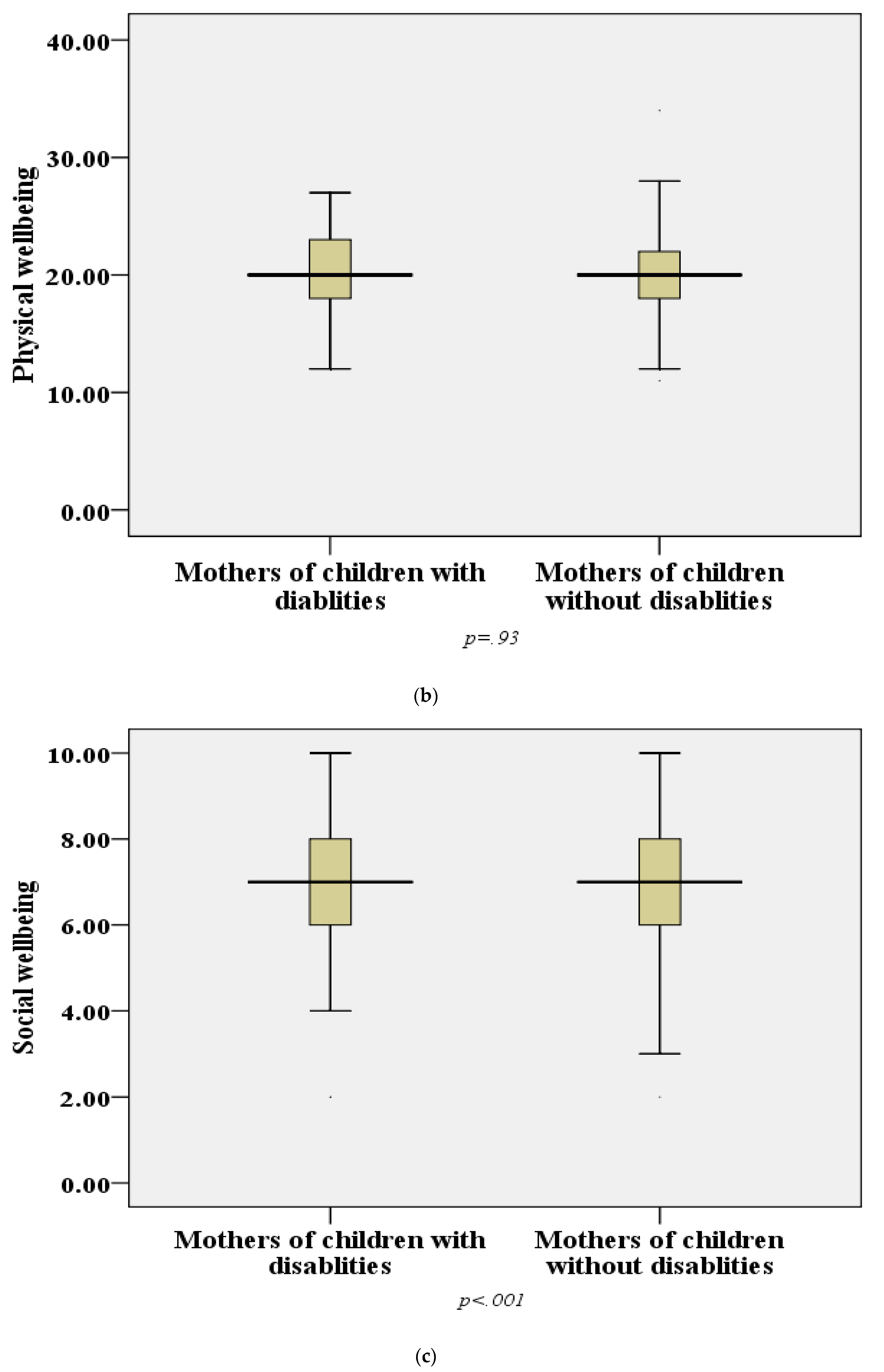
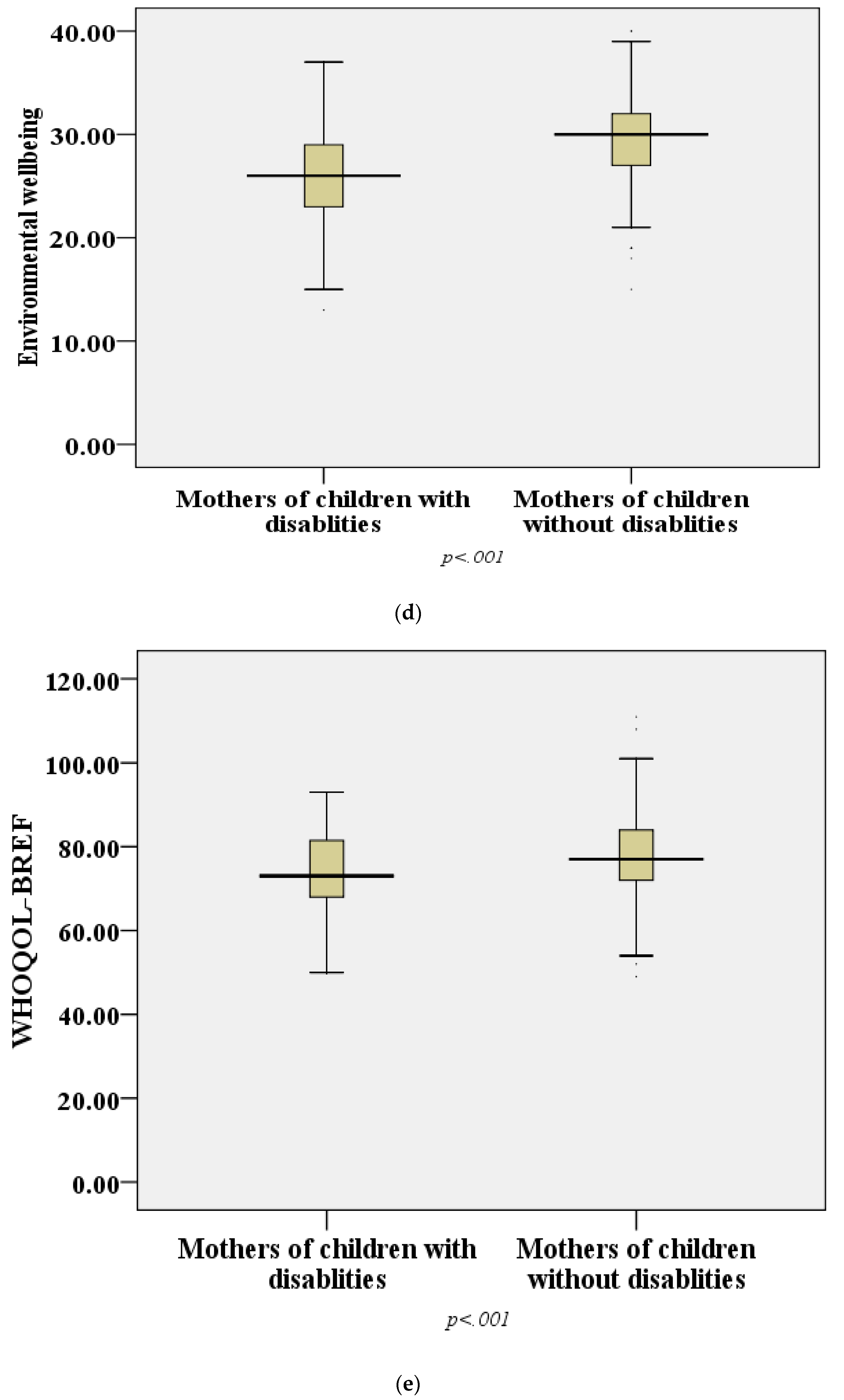
3.2.1. Comparison of Quality of Life between Groups
3.2.2. Predictors of Quality of Life
3.2.3. Mothers’ Needs and Fears
4. Discussion
4.1. Quality of Life
4.2. Required Support for Mothers of Children with Disabilities
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Worcester, J.A.; Nesman, T.M.; Raffaele Mendez, L.M.; Keller, H.R. Giving voice to parents of young children with challenging behavior. Except. Child. 2008, 74, 509–525. [Google Scholar] [CrossRef] [Green Version]
- Gates, B. Responding to Covid-19—A once-in-a-century pandemic? N. Engl. J. Med. 2020, 382, 1677–1679. [Google Scholar] [CrossRef]
- Mortenson, L.Y.; Malani, P.N.; Ernst, R.D. Caring for Someone with COVID-19. JAMA 2020, 324, 2020. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.J.; Bao, Y.; Huang, X.; Shi, J.; Lu, L. Mental health considerations for children quarantined because of COVID-19. Lancet Child Adolesc. Health 2020, 4, 347–349. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Shi, L.; Que, J.; Lu, Q.; Liu, L.; Lu, Z.; Xu, Y.; Liu, J.; Sun, Y.; Meng, S.; et al. The impact of quarantine on mental health status among general population in China during the COVID-19 pandemic. Mol. Psychiatry 2021. [Google Scholar] [CrossRef] [PubMed]
- Manee, F.; Ateya, Y.; Rassafiani, M. A Comparison of the Quality of Life of Arab Mothers of Children with and without Chronic Disabilities. Phys. Occup. Ther. Pediatr. 2016, 36, 260–271. [Google Scholar] [CrossRef] [PubMed]
- Braccialli, L.M.P.; Bagagi, P.D.S.; Sankako, A.N.; Araújo, R.D.C.T. Quality of life of caregivers of people with special needs. Rev. Bras. Educ. Espec. 2012, 18, 113–126. [Google Scholar] [CrossRef]
- Crehan, C.; Kesler, E.; Nambiar, B.; Dube, Q.; Lufesi, N.; Giaccone, M.; Normand, C.; Azad, K.; Heys, M. The NeoTree application: Developing an integrated mHealth solution to improve quality of newborn care and survival in a district hospital in Malawi. BMJ Glob. Health 2019, 4. [Google Scholar] [CrossRef]
- Alkohaiz, M.A. Educational, Financial, and Social Needs of Families of Children with Multiple Disabilities in Saudi Arabia. 2018. Available online: https://ir.library.louisville.edu/etd/2990/ (accessed on 23 September 2021).
- Sijeeni, A. Understanding the Experiences of Mothers Caring for Children with Down Syndrome in Saudi Arabia. 2016. Available online: https://eprints.qut.edu.au/98052/ (accessed on 23 September 2021).
- Bindawas, S.M.; Vennu, V. The national and regional prevalence rates of disability, type, of disability and severity in Saudi Arabia—Analysis of 2016 demographic survey data. Int. J. Environ. Res. Public Health 2018, 15, 419. [Google Scholar] [CrossRef] [Green Version]
- Abu-basha, E.A.; Al-shunnaq, A.F.; Gehring, R. Original article Ερευνητικό άρθρο. Siriraj Med. J 2012, 63, 159–166. [Google Scholar] [CrossRef]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual. Life Res. 2004, 13, 299–310. [Google Scholar]
- Al-Musharaf, S.; Aljuraiban, G.; Bogis, R.; Alnafisah, R.; Aldhwayan, M.; Tahrani, A. Lifestyle changes associated with COVID-19 quarantine among young Saudi women: A prospective study. PLoS ONE 2021, 16, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Vonneilich, N.; Lüdecke, D.; Kofahl, C. The impact of care on family and health-related quality of life of parents with chronically ill and disabled children. Disabil. Rehabil. 2016, 38, 761–767. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.B.; Sigafoos, J. Does respite care reduce parental stress in families with developmentally disabled children? Child Youth Care Forum 2001, 30, 253–263. [Google Scholar] [CrossRef]
- Aaron Resch, J.; Benz, M.R.; Elliott, T.R. Evaluating a dynamic process model of wellbeing for parents of children with disabilities: A multi-method analysis. Rehabil. Psychol. 2012, 57, 61–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Green, S.E. “We’re tired, not sad”: Benefits and burdens of mothering a child with a disability. Soc. Sci. Med. 2007, 64, 150–163. [Google Scholar] [CrossRef]
- Lederberg, A.R. Parenting Stress and Social Support in Hearing Mothers of Deaf and Hearing Children: A Longitudinal Study. J. Deaf Stud. Deaf Educ. 2002, 7, 330–345. [Google Scholar] [CrossRef] [Green Version]
- Götz, I.; Götz, M. Cystic fibrosis: Psychological issues. Paediatr. Respir. Rev. 2000, 1, 121–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, T.B.; Innocenti, M.S.; Boyce, G.C.; Smith, C.S. Depressive symptomatology and interaction behaviors of mothers having a child with disabilities. Psychol. Rep. 1993, 73, 1184–1186. [Google Scholar] [CrossRef] [PubMed]
- Alwhaibi, R.M.; Zaidi, U.; Alzeiby, I.; Alhusaini, A. Quality of Life and Socioeconomic Status: A Comparative Study among Mothers of Children with and without Disabilities in Saudi Arabia. Child Care Pract. 2020, 26, 62–80. [Google Scholar] [CrossRef]
- Haimour, A.I.; Abu-Hawwash, R.M. Evaluating Quality of life of parents having a child with disability. Int. Interdiscip. J. Educ. 2012, 1, 37–43. [Google Scholar]
- Asi, K.Y. Quality of Life among Parents of Children with Autism Spectrum Disorder in Riyadh. Int. Res. Educ. 2016, 4, 76. [Google Scholar] [CrossRef] [Green Version]
- Sulaimani, M.F. A Phenomenological Study of Mothers’ Experiences Navigating Issues of Stigma Related to Autism in the Context of Saudi Arabia; Ohio University: Athens County, OH, USA, 2018. [Google Scholar]
- Ministry of Labor and Social Development Implementing Regulations of the Social Security System. 2015.
- Smith, L.E.; Greenberg, J.S.; Seltzer, M.M. Social support and well-being at mid-life among mothers of adolescents and adults with autism spectrum disorders. J. Autism Dev. Disord. 2012, 42, 1818–1826. [Google Scholar] [CrossRef]
- Ha, J.H.; Greenberg, J.S.; Seltzer, M.M. Parenting a child with a disability: The role of social support for African American parents. Fam. Soc. 2011, 92, 405–411. [Google Scholar] [CrossRef] [Green Version]
- Cramm, J.M.; Nieboer, A.P. Psychological well-being of caregivers of children with intellectual disabilities: Using parental stress as a mediating factor. J. Intellect. Disabil. 2011, 15, 101–113. [Google Scholar] [CrossRef]
- Rovers, M.; Kocum, L. Development of a holistic model of spirituality. J. Spiritual. Ment. Health 2010, 12, 2–24. [Google Scholar] [CrossRef]
- Bousso, R.S.; Poles, K.; de Souza Serafim, T.; de Miranda, M.G. Religious beliefs, illness and death: Family’s perspectives in illness experience. Rev. Da Esc. Enferm. 2011, 45, 391–397. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | Study Group | Total n (%) | p-Value | ||
|---|---|---|---|---|---|
| MCD n (%) | CON n (%) | ||||
| Age groups (y) | 18–25 | 2(2.2) | 8(3.2) | 10(2.9) | 0.05 * |
| 26–35 | 25(26.9) | 76(30.8) | 101(29.7) | ||
| 36–45 | 49(52.7) | 91(36.8) | 140(41.2) | ||
| ≥46 | 17(18.3) | 72(29.1) | 67(19.7) | ||
| Nationality | Saudi | 86(92.5) | 212(85.8) | 298(87.6) | 0.09 |
| Non-Saudi | 7(7.5) | 35(14.2) | 42(12.4) | ||
| Education | ≤Primary | 16(17.2) | 4(1.6) | 20(5.9) | <0.001 * |
| Secondary | 30(32.3) | 31(12.6) | 61(17.9) | ||
| College | 41(44.1) | 155(62.8) | 196(57.6) | ||
| Higher | 6(6.5) | 57(23.1) | 63(18.5) | ||
| Occupation | Housewife | 65(69.9) | 109(44.1) | 174(51.2) | <0.001 * |
| Working mother | 28(30.1) | 138(55.9) | 166(48.8) | ||
| Marital state | Married | 79(84.9) | 228(92.3) | 307(90.3) | 0.04 * |
| Single mother | 14(15.1) | 19(7.7) | 33(9.7) | ||
| Income | Low | 35(37.6) | 22(8.9) | 57(16.8) | <0.001 * |
| Moderate | 55(59.1) | 197(79.8) | 252(74.1) | ||
| High | 3(3.2) | 28(11.3) | 31(9.1) | ||
| Physical health problems | Yes | 21(22.6) | 60(24.3) | 81(23.8) | 0.77 |
| DM | 3(14.3) | 17(28.3) | |||
| HTN | 2(9.5) | 13(21.7) | |||
| Bronchial asthma | 3(14.3) | 7(11.7) | |||
| Others ** | 10(47.6) | 14(23.3) | |||
| Cholesterol | 3(14.3) | 9(15.0) | |||
| No | 72 (77.4) | 187(75.7) | 259(76.2) | ||
| Mental problems | Yes | 5(5.4) | 6(2.4) | 11(3.2) | 14.29 |
| No | 88(94.6) | 241(97.6) | 329(96.8) | ||
| Characteristics | Mothers’ Responses | Mothers with Disabled Child No (%) | Mothers without Disabled Child No (%) | Total No (%) | p Value |
|---|---|---|---|---|---|
| How would you rate your quality of life? a | Very poor | 0(0.0) | 1(0.4) | 1(0.3) | <0.001 * |
| Poor | 15(16.1) | 7(2.8) | 22(6.5) | ||
| Neither good nor poor | 22(23.7) | 32(13.0) | 54(15.9) | ||
| Good | 36(38.7) | 111(44.9) | 147(43.2) | ||
| Very good | 20(21.5) | 96(38.9) | 116(34.1) | ||
| How satisfied are you with your health? | Very dissatisfied | 1(1.1) | 2(0.8) | 3(0.9) | 0.29 |
| Dissatisfied | 6(6.5) | 11(4.5) | 17(5.0) | ||
| Neither dissatisfied nor satisfied | 25(26.9) | 48(19.4) | 73(21.5) | ||
| Satisfied | 35(37.6) | 113(45.7) | 148(43.5) | ||
| Very satisfied | 26(28.0) | 73(29.6) | 99(29.1) | ||
| Total | 93(27.4) | 247(72.64) | 340(100.0) |
| Characteristics | Mothers’ Responses | Mothers with Disabled Child No (%) | Mothers without Disabled Child No (%) | Total No (%) | p Value |
|---|---|---|---|---|---|
| How safe do you feel in your daily life? | Not at all | 2(2.2) | 6(2.4) | 8(2.4) | 0.08 |
| A little | 15(16.1) | 17(6.9) | 32(9.4) | ||
| A moderate amount | 28(30.1) | 71(28.7) | 99(29.1) | ||
| Very much | 31(33.3) | 110(44.5) | 141(41.5) | ||
| Extremely | 17(18.3) | 43(17.4) | 60(17.6) | ||
| How healthy is your physical environment? | Not at all | 1(1.1) | 6(2.4) | 7(2.1) | 0.22 |
| A little | 11(11.8) | 16(6.5) | 27(7.9) | ||
| A moderate amount | 46(49.5) | 104(42.1) | 150(44.1) | ||
| Very much | 31(33.3) | 106(42.9) | 137(40.3) | ||
| Extremely | 4(4.3) | 15(6.1) | 19(5.6) | ||
| Have you enough money to meet your needs? | Not at all | 11(11.8) | 0(0.0) | 11(3.2) | <0.001 * |
| A little | 28(30.1) | 15(6.1) | 43(12.6) | ||
| Moderately | 30(32.3) | 106(42.9) | 136(40.0) | ||
| Mostly | 21(22.6) | 91(36.8) | 112(32.9) | ||
| Completely | 3(3.2) | 35(14.2) | 38(11.2) | ||
| How available to you is the information about COVID 19 in your day-to-day life? | Not at all | 1(1.1) | 0(0.0) | 1(0.3) | 0.002 * |
| A little | 8(8.6) | 7(2.8) | 15(4.4) | ||
| Moderately | 18(19.4) | 34(13.8) | 52(15.3) | ||
| Mostly | 53(57.0) | 129(52.2) | 182(53.5) | ||
| Completely | 13(14.0) | 77(31.2) | 90(26.5) | ||
| To what extent do you have the opportunity for leisure activities during COVID 19 period? | Not at all | 17(18.3) | 14(5.7) | 31(9.1) | 0.001 * |
| A little | 30(32.3) | 64(25.9) | 94(27.6) | ||
| Moderately | 36(38.7) | 107(43.3) | 143(42.1) | ||
| Mostly | 9(9.7) | 58(23.5) | 67(19.7) | ||
| Completely | 1(1.1) | 4(1.6) | 5(1.5) | ||
| How satisfied are you with the conditions of your living place? | Very dissatisfied | 13(14.0) | 5(2.0) | 18(5.3) | <0.001 * |
| Dissatisfied | 10(10.8) | 18(7.3) | 28(8.2) | ||
| Neither satisfied nor dissatisfied | 22(23.7) | 56(22.7) | 78(22.9) | ||
| Satisfied | 34(36.6) | 104(42.1) | 138(40.6) | ||
| Very satisfied | 14(15.1) | 64(25.9) | 78(22.9) | ||
| How satisfied are you with your access to health services? | Very dissatisfied | 9(9.7) | 1(0.4) | 10(2.9) | <0.001 * |
| Dissatisfied | 1(1.1) | 11(4.5) | 12(3.5) | ||
| Neither satisfied nor dissatisfied | 37(39.8) | 57(23.1) | 94(27.6) | ||
| Satisfied | 30(32.3) | 106(42.9) | 136(40.0) | ||
| Very satisfied | 16(17.2) | 72(29.1) | 88(25.9) | ||
| How satisfied are you with your transport? | Very dissatisfied | 8(8.6) | 1(0.4) | 9(2.6) | 0.002 * |
| Dissatisfied | 5(5.4) | 10(4.0) | 15(4.4) | ||
| Neither satisfied nor dissatisfied | 26(28.0) | 55(22.3) | 81(23.8) | ||
| Satisfied | 38(40.9) | 110(44.5) | 148(43.5) | ||
| Very satisfied | 16(17.2) | 71(28.7) | 87(25.6) |
| Dependent Variables | Independent Predictors | Coefficients | Model Statistics | |||||
|---|---|---|---|---|---|---|---|---|
| B | β | T | p-Value | 95% CI | ||||
| Lower | Upper | |||||||
| WHOQOL-BREF | (Constant) | 49.21 | 5.42 | 0.001 | 31.36 | 67.06 | R2 = 0.103 F = 4.2<0.005 | |
| Age | 1.69 | 0.10 | 2.00 | 0.04 | 0.03 | 3.36 | ||
| Nationality | −0.50 | −0.01 | −0.24 | 0.80 | −4.50 | 3.50 | ||
| Education | 0.84 | 0.05 | 0.76 | 0.44 | −1.33 | 3.01 | ||
| Occupation | 2.11 | 0.08 | 1.34 | 0.17 | −0.97 | 5.21 | ||
| Income | 2.03 | 0.08 | 1.31 | 0.18 | −1.00 | 5.06 | ||
| Marital status | 1.32 | 0.06 | 1.21 | 0.22 | −0.81 | 3.45 | ||
| Children existence of disability (Yes/no) | 4.80 | 0.17 | 2.94 | 0.003 | 1.59 | 8.01 | ||
| Health problems | 1.37 | 0.04 | 0.84 | 0.39 | −1.81 | 4.56 | ||
| Mental problems | 6.79 | 0.09 | 1.78 | 0.07 | −0.69 | 4.28 | ||
| |||||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| WHOQOL-BREF scale | 1 | ||||||
| Age | −0.05 | 1 | |||||
| Marital status | 0.04 | 0.07 | 1 | ||||
| Nationality | −0.03 | −0.18 | −0.01 | 1 | |||
| Education | −0.08 | 0.004 | −0.11 | −0.03 | 1 | ||
| Occupation | 0.05 | 0.21 * | 0.05 | −0.19 | 0.35 ** | 1 | |
| Income | −0.02 | −0.03 | −0.24 * | 0.12 | 0.42 ** | 0.36 ** | 1 |
| |||||||
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | |
| WHOQOL-BREF scale | 1 | ||||||
| Age | 0.13 * | 1 | |||||
| Marital status | 0.07 | 0.047 | 1 | ||||
| Nationality | −0.04 | 0.022 | −0.12 | 1 | |||
| Education | 0.03 | −0.261 ** | −0.09 | −0.02 | 1 | ||
| Occupation | 0.13 * | −0.018 | 0.01 | −0.06 | 0.35 ** | 1 | |
| Income | 0.15 * | 0.33 ** | −0.12 | −0.01 | 0.29 ** | 0.27 ** | 1 |
| ||||||
|---|---|---|---|---|---|---|
| Characteristic | Study Group | Total n (%) | Test | p-Value | OR (95%CI) | |
| MCD n (%) | CON n (%) | |||||
| Infection of child with COVID-19 | 30 (32.3) | 108 (43.7) | 138 (40.6) | 17.5 | 0.004 * | 1 |
| Exposure of child to home accidents and emergencies | 7 (7.5) | 36 (14.6) | 43 (12.6) | 1.43 (0.54–3.92) | ||
| Lack of access to medical care in timely manner due to lockdown | 12 (12.9) | 38 (15.9) | 50 (14.8) | 0.88 (0.39–2.03) | ||
| Deterioration of child’s medical condition | 17 (18.3) | 16 (6.5) | 33 (9.7) | 0.26 (0.11–0.62) | ||
| Shortage of medical supplies | 17 (18.3) | 29 (11.7) | 46 (13.5) | 0.47 (0.22–1.04) | ||
| Media addiction | 10 (10.8) | 20 (8.0) | 30 (8.8) | 0.56 (0.22–1.43) | ||
| ||||||
| Characteristic | Study Group | Total n (%) | Test | p-value | OR (95% CI) | |
| MCD n (%) | CON n (%) | |||||
| Emotional and psycho-logical support | 24 (25.8) | 45 (18.2) | 69 (20.3) | 18.4 | 0.010 * | 1 |
| Family support | 20 (21.5) | 48 (19.4) | 68 (20.0) | 1.28 (0.59–2.80) | ||
| Spiritual support | 16 (17.2) | 23 (9.3) | 39 (11.5) | 0.77 (0.32–1.86) | ||
| Medical services | 12 (12.9) | 44 (17.8) | 56 (16.5) | 1.76 (0.74–4.22) | ||
| Entertainment | 6 (6.5) | 44 (17.8) | 50 (14.7) | 3.91 (1.35–11.89) | ||
| Availability of supplies | 7 (7.5) | 13 (5.3) | 20 (5.9) | 0.99 (0.31–3.20) | ||
| Financial support | 3 (3.2) | 2 (0.8) | 5 (1.5) | 0.36 (0.04–2.88) | ||
| Educational campaigns and media guidance | 5 (5.4) | 28 (11.3) | 33 (9.7) | 2.99 (1.13–10.14) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al Awaji, N.; Aldhahi, M.; Akil, S.; Awad, S.; Mortada, E. Quality of Life, Needs and Fears of Mothers of Children with Disabilities in Saudi Arabia during the COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 11442. https://doi.org/10.3390/ijerph182111442
Al Awaji N, Aldhahi M, Akil S, Awad S, Mortada E. Quality of Life, Needs and Fears of Mothers of Children with Disabilities in Saudi Arabia during the COVID-19 Lockdown. International Journal of Environmental Research and Public Health. 2021; 18(21):11442. https://doi.org/10.3390/ijerph182111442
Chicago/Turabian StyleAl Awaji, Nisreen, Monira Aldhahi, Shahnaz Akil, Salwa Awad, and Eman Mortada. 2021. "Quality of Life, Needs and Fears of Mothers of Children with Disabilities in Saudi Arabia during the COVID-19 Lockdown" International Journal of Environmental Research and Public Health 18, no. 21: 11442. https://doi.org/10.3390/ijerph182111442