
Caring for Caregivers: Italian Health Care Workers’ Needs during the COVID-19 Pandemic

 ,
,  ,
, 
Abstract
:1. Introduction
1.1. COVID-19 and Mental Distress of Health-Care Workers
1.2. Health-Care Workers and Pandemic: Protective Factors
2. Materials and Methods
2.1. Study Setting and Sample
2.2. Data Analysis
3. Results
- 1.1
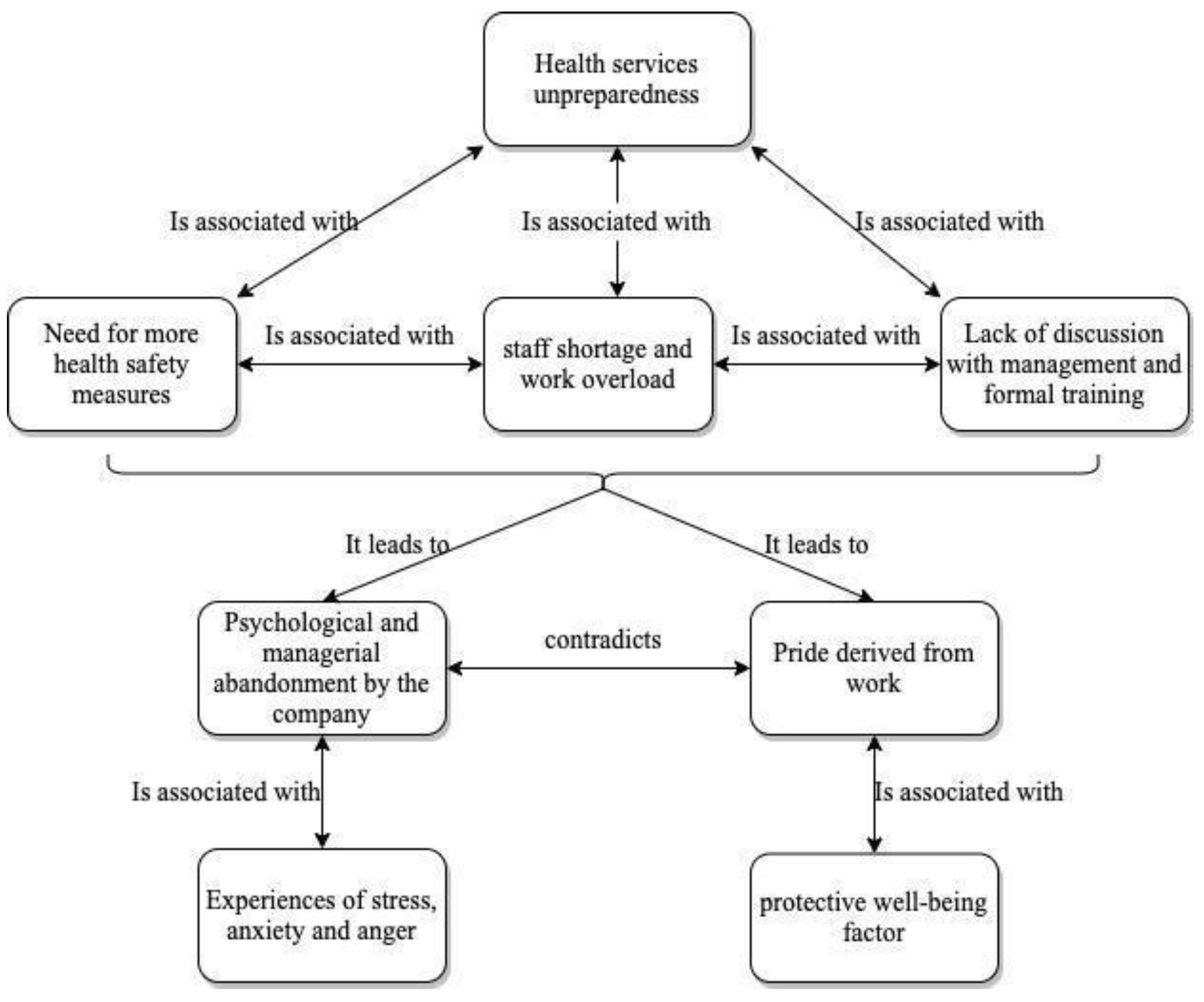
- AUP Unpreparedness
- 1.2
- Lack of Organizational Support
- 1.3
- Positive Sides of the Work Environment
- 2.1
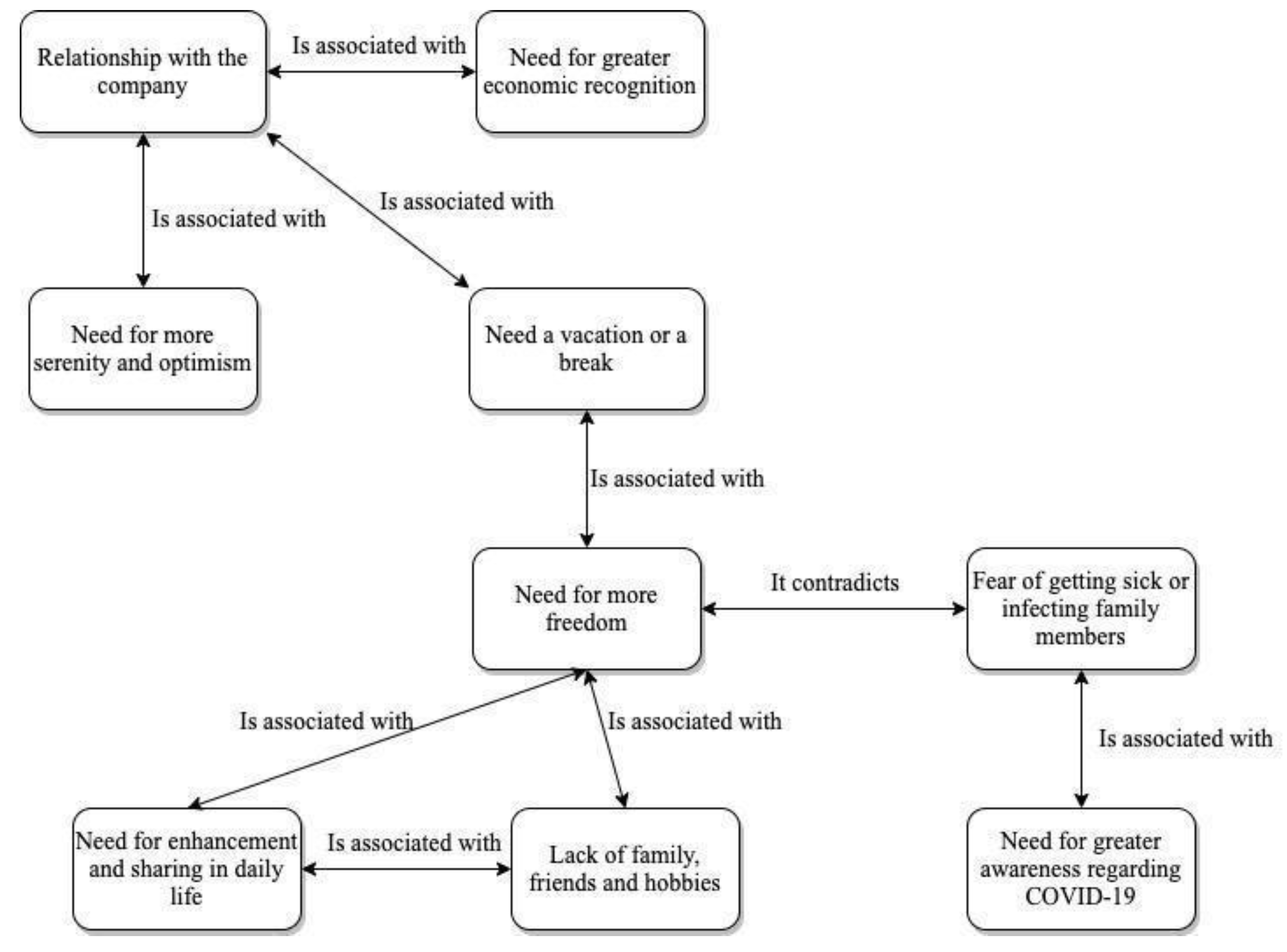
- Psychological, Concrete and Professional Needs
- 2.2
- Perceived deficits
- 3.1
- Uncertainty: Source of Distress or Chance for Growth
- 3.2
- Consequences for Ill People and Their Families
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Weekly Epidemiological Update on COVID-19—13 July 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---13-july-2021 (accessed on 13 July 2021).
- Istat & ISS. Impatto Dell’Epidemia COVID-19 Sulla Mortalità Totale Della Popolazione Residente. Anno 2020 e Gennaio–Aprile 2021. 10 June 2021. Available online: https://www.istat.it/it/archivio/258463 (accessed on 10 August 2021).
- ISS. Caratteristiche Dei Pazienti Deceduti Positivi All’Infezione Da SARS-Cov-2 in Italia. EpiCentro—Portale Di Epidemiologia Per Gli Operatori Sanitari. 28 July 2021. Available online: https://www.epicentro.iss.it/coronavirus/sars-cov-2-decessi-italia#1 (accessed on 10 August 2021).
- Tomaino, S.C.; Cipolletta, S.; Kostova, Z.; Todorova, I. Stories of life during the first wave of the COVID-19 pandemic in Italy: A qualitative study. Int. J. Environ. Res. Public Health 2021, 18, 7630. [Google Scholar] [CrossRef]
- Istat & ISS. Impatto Dell’epidemia COVID-19 Sulla Mortalità Totale Della Popolazione Residente. Periodo Anno 2020. 5 March 2021. Available online: https://www.istat.it/it/archivio/254507 (accessed on 10 August 2021).
- Felice, C.; Di Tanna, G.L.; Zanus, G.; Grossi, U. Impact of COVID-19 outbreak on healthcare workers in Italy: Results from a national E-survey. J. Community Health 2020, 45, 675–683. [Google Scholar] [CrossRef] [PubMed]
- Pisano, G.P.; Sadun, R.; Zanini, M. Lessons from Italy’s Response to Coronavirus. Harvard Business Review. Available online: https://hbr.org/2020/03/lessons-from-italys-response-to-coronavirus (accessed on 27 March 2020).
- Costantini, M.; Sleeman, K.E.; Peruselli, C.; Higginson, I.J. Response and role of palliative care during the COVID-19 pandemic: A national telephone survey of hospices in Italy. Palliat. Med. 2020, 34, 889–895. [Google Scholar] [CrossRef]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Nyashanu, M.; Pfende, F.; Ekpenyong, M. Exploring the challenges faced by frontline workers in health and social care amid the COVID-19 pandemic: Experiences of frontline workers in the English Midlands region, UK. J. Interprof. Care 2020, 34, 655–661. [Google Scholar] [CrossRef]
- Savoia, E.; Argentini, G.; Gori, D.; Neri, E.; Piltch-Loeb, R.; Fantini, M.P. Factors associated with access and use of PPE during COVID-19: A cross-sectional study of Italian physicians. PLoS ONE 2020, 15, e0239024. [Google Scholar] [CrossRef] [PubMed]
- Tabah, A.; Ramanan, M.; Laupland, K.B.; Buetti, N.; Cortegiani, A.; Mellinghoff, J.; Conway Morris, A.; Camporota, L.; Zappella, N.; Elhadi, M.; et al. Personal protective equipment and intensive care unit healthcare worker safety in the COVID-19 era (PPE-SAFE): An international survey. J. Crit. Care 2020, 59, 70–75. [Google Scholar] [CrossRef]
- Cai, H.; Tu, B.; Ma, J.; Chen, L.; Fu, L.; Jiang, Y.; Zhuang, Q. Psychological impacts and coping strategies of front-line medical staff during COVID-19 outbreak in Hunan, China. Med. Sci. Monit. 2020, 26, e924171-1–e924171-16. [Google Scholar] [CrossRef] [Green Version]
- Rapisarda, F.; Vallarino, M.; Cavallini, E.; Barbato, A.; Brousseau-Paradis, C.; De Benedictis, L.; Lesage, A. The early impact of the COVID-19 emergency on mental health workers: A survey in Lombardy, Italy. Int. J. Environ. Res. Public Health 2020, 17, 8615. [Google Scholar] [CrossRef]
- Lu, W.; Wang, H.; Lin, Y.; Li, L. Psychological status of medical workforce during the COVID-19 pandemic: A cross-sectional study. Psychiatry Res. 2020, 288, 112936. [Google Scholar] [CrossRef]
- Fawaz, M.; Samaha, A. The psychosocial effects of being quarantined following exposure to COVID-19: A qualitative study of lebanese health care workers. Int. J. Soc. Psychiatry 2020, 66, 560–565. [Google Scholar] [CrossRef] [PubMed]
- Sun, N.; Wei, L.; Shi, S.; Jiao, D.; Song, R.; Ma, L.; Wang, H.; Wang, C.; Wang, Z.; You, Y.; et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am. J. Infect. Control 2020, 48, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Puci, M.V.; Nosari, G.; Loi, F.; Puci, G.V.; Montomoli, C.; Ferraro, O.E. Risk Perception and Worries among Health Care Workers in the COVID-19 Pandemic: Findings from an Italian Survey. Healthcare 2020, 8, 535. [Google Scholar] [CrossRef]
- Simione, L.; Gnagnarella, C. Differences between health workers and general population in risk perception, behaviors, and psychological distress related to COVID-19 spread in Italy. Front. Psychol. 2020, 11, 2166. [Google Scholar] [CrossRef] [PubMed]
- Luquiens, A.; Morales, J.; Bonneville, M.; Potier, H.; Perney, P.; Faure, G.; Canaguier, A. Mental burden of hospital workers during the COVID-19 crisis: A quanti-qualitative analysis. Front. Psychiatry 2021, 12, 510. [Google Scholar] [CrossRef] [PubMed]
- Serrano-Ripoll, M.J.; Meneses-Echavez, J.F.; Ricci-Cabello, I.; Fraile-Navarro, D.; Fiol-deRoque, M.A.; Pastor-Moreno, G.; Castro, A.; Ruiz-Pérez, I.; Zamanillo Campos, R.; Gonçalves-Bradley, D.C. Impact of viral epidemic outbreaks on mental health of healthcare workers: A rapid systematic review and meta-analysis. J. Affect. Disord. 2020, 277, 347–357. [Google Scholar] [CrossRef]
- Moitra, M.; Rahman, M.; Collins, P.Y.; Gohar, F.; Weaver, M.; Kinuthia, J.; Rössler, W.; Petersen, S.; Unutzer, J.; Saxena, S.; et al. Mental health consequences for healthcare workers during the COVID-19 pandemic: A scoping review to draw lessons for LMICs. Front. Psychiatry 2021, 12, 22. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Vizheh, M.; Qorbani, M.; Arzaghi, S.M.; Muhidin, S.; Javanmard, Z.; Esmaeili, M. The mental health of healthcare workers in the COVID-19 pandemic: A systematic review. J. Diabetes Metab. Disord. 2020, 19, 1967–1978. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.; Ma, S.; Wang, Y.; Cai, Z.; Hu, J.; Wei, N.; Wu, J.; Du, H.; Chen, T.; Li, R.; et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw. Open 2020, 3, e203976. [Google Scholar] [CrossRef]
- Zhang, J.; Deng, X.; Liu, H.; Xu, X.; Fang, R. Evaluation of the mental health status of community healthcare workers during the COVID-19 outbreak. Medicine 2021, 100, e24739. [Google Scholar] [CrossRef] [PubMed]
- Morgantini, L.A.; Naha, U.; Wang, H.; Francavilla, S.; Acar, Ö.; Flores, J.M.; Crivellaro, S.; Moreira, D.; Abern, M.; Eklund, M.; et al. Factors contributing to healthcare professional burnout during the COVID-19 pandemic: A rapid turnaround global survey. PLoS ONE 2020, 15, e0238217. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental health outcomes among frontline and second-line health care workers during the coronavirus disease 2019 (COVID-19) pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef]
- Etkind, S.N.; Bone, A.E.; Lovell, N.; Cripps, R.L.; Harding, R.; Higginson, I.J.; Sleeman, K.E. The role and response of Palliative Care and Hospice services in epidemics and pandemics: A rapid review to inform practice during the COVID-19 pandemic. J. Pain Symptom Manag. 2020, 60, e31–e40. [Google Scholar] [CrossRef]
- Muhr, T. ATLAS/ti—A prototype for the support of text interpretation. Qual. Sociol. 1991, 14, 349–371. [Google Scholar] [CrossRef]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Corbin, J.M.; Strauss, A. Grounded theory research: Procedures, canons, and evaluative criteria. Qual. Sociol. 1990, 13, 3–21. [Google Scholar] [CrossRef]
- Lasalvia, A.; Bonetto, C.; Bertani, M.; Bissoli, S.; Cristofalo, D.; Marrella, G.; Ceccato, E.; Cremonese, C.; De Rossi, M.; Lazzarotto, L.; et al. Influence of perceived organisational factors on job burnout: Survey of community mental health staff. Br. J. Psychiatry 2009, 195, 537–544. [Google Scholar] [CrossRef] [PubMed]
- Cipolletta, S.; Ortu, M.C. COVID-19: Common constructions of the pandemic and their implications. J. Constr. Psychol. 2020, 34, 278–294. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | No. | % |
|---|---|---|
| Date of completion | ||
| Post-vaccine | 500 | 98.23 |
| Pre-vaccine | 9 | 1.77 |
| Sex | ||
| Men | 130 | 25.54 |
| Woman | 379 | 74.46 |
| Age | ||
| 19–29 | 36 | 7.07 |
| 30–39 | 68 | 13.36 |
| 40–49 | 112 | 22.00 |
| 50–59 | 224 | 44.01 |
| 60–69 | 66 | 12.97 |
| >69 | 1 | 0.20 |
| Working position | ||
| General ward | 170 | 33.40 |
| Territorial services | 178 | 34.97 |
| COVID-19 ward | 81 | 15.91 |
| Administrative services | 73 | 14.37 |
| Not working in AUP | 6 | 1.18 |
| Educational level | ||
| PhD | 7 | 1.38 |
| Post-lauream master | 68 | 13.36 |
| University | 242 | 47.54 |
| High School | 170 | 33.40 |
| Middle School | 21 | 4.13 |
| Children | ||
| Yes | 330 | 64.83 |
| No | 178 | 34.97 |
| Social status | ||
| Married | 293 | 57.56 |
| Involved with someone | 84 | 16.50 |
| Single | 60 | 11.79 |
| Divorced | 60 | 11.79 |
| Widowed | 11 | 2.16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Leo, D.; Martucci, M.M.; Grossi, A.; Siviero, F.; Vicentini, S.; Romascu, C.; Mercurio, A.; Battaglia, M.; Tribbia, N. Caring for Caregivers: Italian Health Care Workers’ Needs during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11386. https://doi.org/10.3390/ijerph182111386
De Leo D, Martucci MM, Grossi A, Siviero F, Vicentini S, Romascu C, Mercurio A, Battaglia M, Tribbia N. Caring for Caregivers: Italian Health Care Workers’ Needs during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(21):11386. https://doi.org/10.3390/ijerph182111386
Chicago/Turabian StyleDe Leo, Diego, Maria Maddalena Martucci, Antonello Grossi, Francesca Siviero, Silvia Vicentini, Carolina Romascu, Arianna Mercurio, Martina Battaglia, and Noemi Tribbia. 2021. "Caring for Caregivers: Italian Health Care Workers’ Needs during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 21: 11386. https://doi.org/10.3390/ijerph182111386