
Fear of Infection and the Common Good: COVID-19 and the First Italian Lockdown


Abstract
:1. Introduction
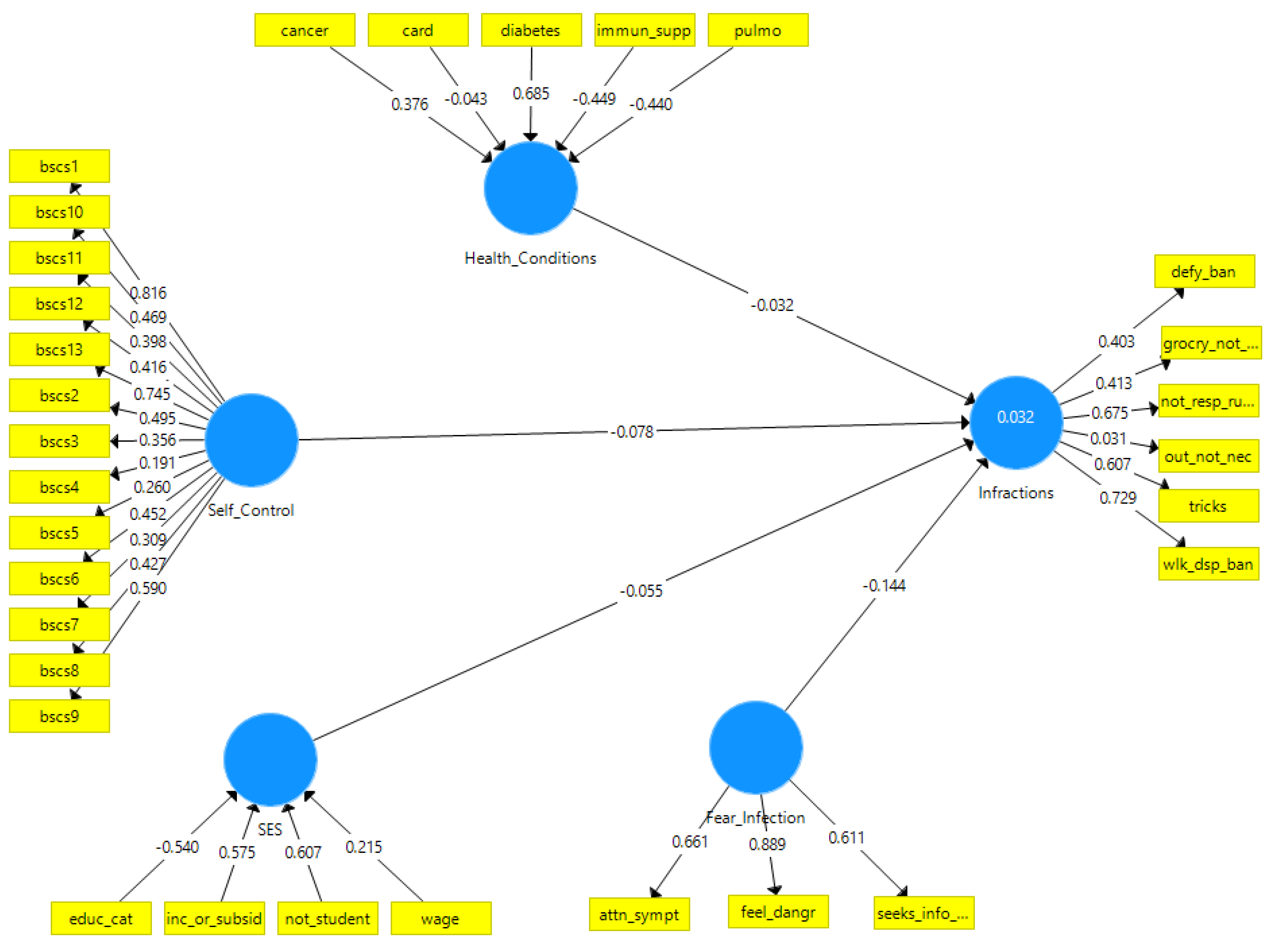
- Higher self-control is inversely related to lockdown violations. Self-control is defined as the ability to restrain impulses, and overall self-discipline [13].
- Higher socio-economic status (SES) is inversely related to lockdown violations. This was based in part on a German study that reported a positive association of higher education and engaging in COVID-19 protective measures [14].
- Having health conditions is inversely related to lockdown violations.
- Greater fear of infection is inversely related to lockdown violations.
2. Materials and Methods
2.1. Participants and Data
2.2. Measures
2.3. Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Latent Variable/Indicator | Description | VIF |
|---|---|---|
| Brief Self-ControlScale | ||
| bscs1 | I am good at resisting temptation | 1.423 |
| bscs2 | I have a hard time breaking bad habits | 1.473 |
| bscs3 | I am lazy | 1.323 |
| bscs4 | I say inappropriate things | 1.299 |
| bscs5 | I do certain things that are bad for me, if they are fun | 1.707 |
| bscs6 | I refuse things that are bad for me | 1.564 |
| bscs7 | I wish I had more discipline | 1.546 |
| bscs8 | People would say that I have iron self-discipline | 1.600 |
| bscs9 | Pleasure and fun sometimes keep me from getting work done | 1.328 |
| bscs10 | I have trouble concentrating | 1.761 |
| bscs11 | I am able to work effectively toward long-term goals | 1.290 |
| bscs12 | Sometimes I can’t stop myself from doing something, even if I know it is wrong | 1.287 |
| bscs13 | I often act without thinking through all the alternatives | 1.697 |
| Health_Conditions | ||
| diabetes | Do you currently suffer from diabetes? | 1.001 |
| cancer | Do you currently suffer from cancer? | 1.003 |
| immun_supp | Do you currently suffer from immunosuppression? | 1.007 |
| pulmo | Do you currently suffer from pulmonary diseases? | 1.009 |
| card | Do you currently suffer from cardiovascular diseases? | 1.013 |
| SES | ||
| not_student | Employment condition: student (reversed) | 1.119 |
| wage | Monthly income of your cohabitation (euros): (<500, 500–1000, 1000–2000, 2000–3000, 3000–4000, >4000) | 1.044 |
| educ_cat | Educational level (elementary school, secondary school, high school, three-year degree, master’s degree, Master/Doctorate/Specialization) | 1.092 |
| inc_or_subsid | Earning income or stopped working but getting paid | 1.145 |
| Fear_Infection | ||
| seeks_info_ascend | Are you actively searching for information on the progress of the epidemic? (number of positive people, number of deaths, containment policies, etc.) | 1.118 |
| feel_dangr | How much do you feel in danger of COVID-19 infection? | 1.258 |
| attn_sympt | In the last period, are you paying more attention than usual to your physical symptoms? | 1.266 |
| Infraction | ||
| out_not_nec | I only go out when necessary (reversed) | 1.005 |
| defy_ban | I go out regularly in defiance of the ban | 1.048 |
| wlk_dsp_ban | I happened to go out for a walk indefiance of the ban | 1.097 |
| grocry_not_nec | I happened to go to the grocery store without real necessity | 1.056 |
| tricks | I am looking for tricks to bypass the ordinances (e.g., I go daily working even if not necessary because I could work from home, I walk around with the dog more times than necessary, I go jogging) | 1.183 |
| not_resp_rules | I respect loyally the rules imposed by ministerial ordinances (reversed) | 1.206 |
Appendix B. Stata Code for Models 1 and 2
| plssem (SC > bscs1-bscs13)/// |
| (HealthConds < immun_supp card pulmo cancer diabetes)/// |
| (SES < wage inc_or_subsid educ_cat not_student)/// |
| (Fearinfect > feel_dangr attn_sympt seeks_info_ascend)/// |
| (Infrac > not_resp_rules defy_ban out_not_nec wlk_dsp_ban grocry_not_nec tricks),/// |
| structural(Infrac SC Fearinfect SES HealthConds)/// |
| boot(5000) seed(919) stats maxiter(100) |
| estat total |
| plssem (SC > bscs1-bscs13)/// |
| (HealthConds < immun_supp card pulmo cancer diabetes)/// |
| (SES < wage inc_or_subsid educ_cat not_student)/// |
| (Fearinfect > feel_dangr attn_sympt seeks_info_ascend)/// |
| (Infrac > not_resp_rules defy_ban out_not_nec wlk_dsp_ban grocry_not_nec tricks),/// |
| structural(Infrac SC Fearinfect SES HealthConds,/// |
| Fearinfect HealthConds)/// |
| boot(5000) seed(919) stats maxiter(100) |
| estat indirect, effects(Infrac Fearinfect HealthConds)/// |
| boot(500) seed(919) |
References
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Flesia, L.; Monaro, M.; Mazza, C.; Fietta, V.; Colicino, E.; Segatto, B.; Roma, P. Predicting Perceived Stress Related to the Covid-19 Outbreak through Stable Psychological Traits and Machine Learning Models. J. Clin. Med. 2020, 9, 3350. [Google Scholar] [CrossRef] [PubMed]
- BBC News. Coronavirus: Italy Takes ‘Calculated Risk’ in Easing Restrictions—PM: BBC. 2020. Available online: https://www.bbc.com/news/world-europe-52687448 (accessed on 11 June 2020).
- Flaxman, S.; Mishra, S.; Gandy, A.; Unwin, H.J.T.; Mellan, T.A.; Coupland, H.; Whittaker, C.; Zhu, H.; Berah, T.; Eaton, J.W.; et al. Estimating the effects of non-pharmaceutical interventions on COVID-19 in Europe. Nature 2020, 584, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.; Bloom, N.; Davis, S.; Terry, S. COVID-Induced Economic Uncertainty; Working Paper 26983; National Bureau of Economic Research: Cambridge, MA, USA, 2020.
- Killgore, W.D.S.; Cloonan, S.A.; Taylor, E.C.; Dailey, N.S. Loneliness: A signature mental health concern in the era of COVID-19. Psychiatry Res. 2020, 290, 113117. [Google Scholar] [CrossRef] [PubMed]
- Killgore, W.D.S.; Cloonan, S.A.; Taylor, E.C.; Fernandez, F.; Grandner, M.A.; Dailey, N.S. Suicidal ideation during the COVID-19 pandemic: The role of insomnia. Psychiatry Res. 2020, 290, 113134. [Google Scholar] [CrossRef] [PubMed]
- Odriozola-Gonzalez, P.; Planchuelo-Gomez, A.; Irurtia, M.J.; de Luis-Garcia, R. Psychological effects of the COVID-19 outbreak and lockdown among students and workers of a Spanish university. Psychiatry Res. 2020, 290, 113108. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Lowenberg, A.D. Neoclassical Economics as a Theory of Politics and Institutions. Cato J. 1990, 9, 619–639. [Google Scholar]
- Hardin, G. The tragedy of the commons. The population problem has no technical solution; it requires a fundamental extension in morality. Science 1968, 162, 1243–1248. [Google Scholar] [CrossRef] [Green Version]
- Ferrari, J.R.; Stevens, E.B.; Jason, L.A. The Relationship of Self-Control and Abstinence Maintenance: An Exploratory Analysis of Self-Regulation. J. Groups Addict. Recover. 2009, 4, 32–41. [Google Scholar] [CrossRef] [Green Version]
- Lüdecke, D.; von dem Knesebeck, O. Protective behavior in course of the COVID-19 outbreak--survey results from Germany. Front Public Health. 2020, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kock, N.; Hadaya, P. Minimum sample size estimation in PLS-SEM: The inverse square root and gamma-exponential methods. Inform. Syst. J. 2018, 28, 227–261. [Google Scholar] [CrossRef]
- Tangney, J.P.; Baumeister, R.F.; Boone, A.L. High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. J. Personal. 2004, 72, 271–324. [Google Scholar] [CrossRef] [PubMed]
- Lindner, C.; Nagy, G.; Retelsdorf, J. The dimensionality of the Brief Self-Control Scale-An evaluation of unidimensional and multidimensional applications. Pers. Indiv. Differ. 2015, 86, 465–473. [Google Scholar] [CrossRef]
- Green, L.W. Manual for Scoring Socioeconomic Status for Research on Health Behavior. Public Health Rep. 1970, 85, 815–827. [Google Scholar] [CrossRef] [Green Version]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Bollen, K.A. Latent variables in psychology and the social sciences. Annu. Rev. Psychol. 2002, 53, 605–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hair, J.F.; Howard, M.C.; Nitzl, C. Assessing measurement model quality in PLS-SEM using confirmatory composite analysis. J. Bus. Res. 2020, 109, 101–110. [Google Scholar] [CrossRef]
- Bollen, K.A. Structural Equations with Latent Variables; Wiley: New York, NY, USA, 1989; Volume XIV, 514p. [Google Scholar]
- Rhemtulla, M.; Brosseau-Liard, P.E.; Savalei, V. When Can Categorical Variables Be Treated as Continuous? A Comparison of Robust Continuous and Categorical SEM Estimation Methods Under Suboptimal Conditions. Psychol. Methods. 2012, 17, 354–373. [Google Scholar] [CrossRef] [Green Version]
- Foldnes, N.; Gronneberg, S. Pernicious Polychorics: The Impact and Detection of Underlying Non-normality. Struct. Equ. Modeling 2020, 27, 525–543. [Google Scholar] [CrossRef]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM), 3rd ed.; SAGE: Los Angeles, CA, USA, 2014. [Google Scholar]
- Henseler, J., Jr.; Dijkstra, T. ADANCO 2.0.; Composite Modeling: Kleve, Germany, 2015. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Fit indices in covariance structure modeling: Sensitivity to underparameterized model misspecification. Psychol. Methods 1998, 3, 424–453. [Google Scholar] [CrossRef]
- Henseler, J., Jr. Composite-Based Structural Equation Modeling: Analyzing Latent and Emergent Variables; The Guilford Press: New York, NY, USA, 2021. [Google Scholar]
- Hu, L.T.; Bentler, P.M. Cutoff Criteria for Fit Indexes in Covariance Structure Analysis: Conventional Criteria Versus New Alternatives. Struct. Equ. Modeling 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Marks, I.M.; Nesse, R.M. Fear and Fitness—An Evolutionary Analysis of Anxiety Disorders. Ethol. Sociobiol. 1994, 15, 247–261. [Google Scholar] [CrossRef] [Green Version]
- Ackerman, J.M.; Tybur, J.M.; Blackwell, A.D. What Role Does Pathogen-Avoidance Psychology Play in Pandemics? Trends Cogn. Sci. 2021, 25, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Headland, T.N.; Greene, H.W. Hunter-gatherers and other primates as prey, predators, and competitors of snakes. Proc. Natl. Acad. Sci. USA 2011, 108, E1470–E1474. [Google Scholar] [CrossRef] [Green Version]
- Ebrahim, S.H.; Memish, Z.A. COVID-19—the role of mass gatherings. Travel Med. Infect. Dis. 2020, 34, 101617. [Google Scholar] [CrossRef]
- Sit, S.M.; Lam, T.H.; Lai, A.Y.; Wong, B.Y.; Wang, M.P.; Ho, S.Y. Fear of COVID-19 and its associations with perceived personal and family benefits and harms in Hong Kong. Transl. Behav. Med. 2021, 11, 793–801. [Google Scholar] [CrossRef]
- Petersen, M.B. COVID lesson: Trust the public with hard truths. Nature 2021, 598, 237. [Google Scholar] [CrossRef] [PubMed]
- Chae, S.H.; Park, H.J. Effectiveness of Penalties for Lockdown Violations During the COVID-19 Pandemic in Germany. Am. J. Public Health 2020, 110, 1844–1849. [Google Scholar] [CrossRef]
- Gottfredson, M.R.; Hirschi, T. A General Theory of Crime; Stanford University Press: Stanford, CA, USA, 1990; Volume XVI, 297p. [Google Scholar]
- Moffitt, T.E.; Arseneault, L.; Belsky, D.; Dickson, N.; Hancox, R.J.; Harrington, H.; Houts, R.; Poulton, R.; Roberts, B.W.; Ross, S.; et al. A gradient of childhood self-control predicts health, wealth, and public safety. Proc. Natl. Acad. Sci. USA 2011, 108, 2693–2698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fritz, C.E.; Williams, H.B. The Human Being in Disasters—A Research Perspective. Ann. Am. Acad. Polit. Soc. Sci. 1957, 309, 42–51. [Google Scholar] [CrossRef]
- Gabbiadini, A.; Baldissarri, C.; Durante, F.; Valtorta, R.R.; De Rosa, M.; Gallucci, M. Together Apart: The Mitigating Role of Digital Communication Technologies on Negative Affect During the COVID-19 Outbreak in Italy. Front. Psychol. 2020, 11, 2763. [Google Scholar] [CrossRef] [PubMed]
- Srol, J.; Mikuskova, E.B.; Cavojova, V. When we are worried, what are we thinking? Anxiety, lack of control, and conspiracy beliefs amidst the COVID-19 pandemic. Appl. Cogn. Psych. 2021, 35, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Earnshaw, V.A.; Eaton, L.A.; Kalichman, S.C.; Brousseau, N.M.; Hill, E.C.; Fox, A.B. COVID-19 conspiracy beliefs, health behaviors, and policy support. Transl. Behav. Med. 2020, 10, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Yaseen, A.; Al-Haidar, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. Conspiracy Beliefs Are Associated with Lower Knowledge and Higher Anxiety Levels Regarding COVID-19 among Students at the University of Jordan. Int. J. Environ. Res. Public Health 2020, 17, 4915. [Google Scholar] [CrossRef] [PubMed]


| Variable | Beta | Bootstrapped 95% CI | t | p |
|---|---|---|---|---|
| Fear of Infection | −0.14 | −0.19–−0.11 | −6.88 | <0.001 |
| Health Conditions | −0.03 | −0.07–0.09 | −0.60 | 0.54 |
| SES | −0.06 | −0.12–0.09 | −0.80 | 0.43 |
| Self-Control | −0.08 | −0.15–0.12 | −1.16 | 0.25 |
| Variable | Beta | Bootstrapped 95% CI | t | p |
|---|---|---|---|---|
| Direct Effects on Infractions | ||||
| Fear of Infection | −0.14 | −0.19–−0.10 | −6.63 | <0.001 |
| Health Conditions | −0.03 | −0.06–0.09 | −0.65 | 0.51 |
| SES | −0.06 | −0.12–0.09 | −0.79 | 0.43 |
| Self-Control | −0.08 | −0.15–0.12 | −1.17 | 0.24 |
| Indirect Effect through Fear of Infection | ||||
| Health Conditions | −0.01 | −0.01–0.00 | −0.57 | 0.57 |
| Variable | Composite Reliability | Average Variance Extracted (AVE) |
|---|---|---|
| Fear of Infection | 0.77 | 0.54 |
| Self-Control | 0.78 | 0.24 |
| Infractions | 0.66 | 0.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balbuena, L.; Monaro, M. Fear of Infection and the Common Good: COVID-19 and the First Italian Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 11341. https://doi.org/10.3390/ijerph182111341
Balbuena L, Monaro M. Fear of Infection and the Common Good: COVID-19 and the First Italian Lockdown. International Journal of Environmental Research and Public Health. 2021; 18(21):11341. https://doi.org/10.3390/ijerph182111341
Chicago/Turabian StyleBalbuena, Lloyd, and Merylin Monaro. 2021. "Fear of Infection and the Common Good: COVID-19 and the First Italian Lockdown" International Journal of Environmental Research and Public Health 18, no. 21: 11341. https://doi.org/10.3390/ijerph182111341