
Validation of the Korean Version of Impact of Event Scale—Revised (IES-R) in Korean Nurses during the COVID-19 Pandemic



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Variables and Measures
2.2.1. Impact of Event Scale—Revised, IES-R
2.2.2. Perceived Stress Scale, PSS
2.2.3. Generalized Anxiety Disorder Screener, GAD-7
2.2.4. Dimensions of Anger Reactions-5, DAR-5
2.2.5. General Characteristics of Participants
2.3. Statistical Procedures
2.4. Ethical Consideration
3. Results
3.1. Characteristics of Participants of Internet Survey
3.2. Confirmatory Factor Analysis
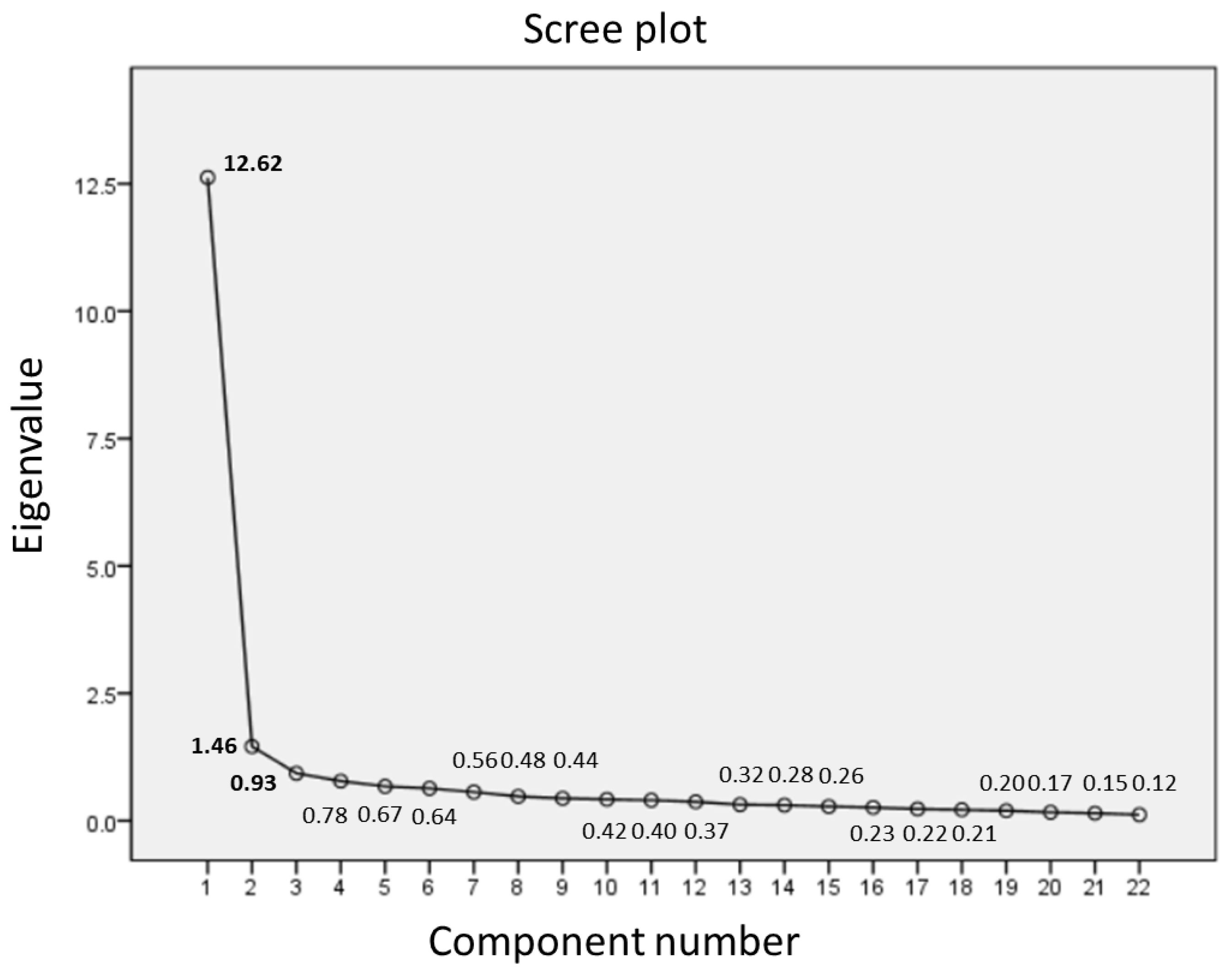
3.3. Exploratory Factor Analysis
3.4. Convergent Validity
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Items | Factor 1 | Factor 2 |
|---|---|---|
| Factor 1. Intrusion and avoidance | ||
| 14. I found myself acting or feeling like I was back at that time. | 0.873 * | −0.187 * |
| 22. I tried not to talk about it. | 0.868 * | 0.137 * |
| 17. I tried to remove it from my memory. | 0.867 * | 0.169 * |
| 8. I stayed away from reminders about it. | 0.861 * | −0.049 |
| 11. I tried not to think about it. | 0.840 * | −0.013 |
| 16. I had waves of strong feelings about it. | 0.828 * | 0.011 |
| 6. I thought about it when I didn’t mean to. | 0.787 * | 0.068 |
| 5. I avoided letting myself get upset when I thought about it or was reminded of it. | 0.785 * | 0.067 |
| 7. I felt as if it hadn’t happened or wasn’t real. | 0.781 * | −0.125 |
| 9. Pictures about it popped into my mind. | 0.761 * | 0.080 |
| 19. Reminders of it caused me to have physical reactions, such as sweating, trouble breathing, nausea, or a pounding heart. | 0.748 * | −0.245 * |
| 18. I had trouble concentrating. | 0.699 * | 0.154 * |
| 20. I had dreams about it. | 0.682 * | 0.097 |
| 13. My feelings about it were kind of numb. | 0.660 * | 0.048 |
| 1. Any reminder brought back feelings about it. | 0.654 * | 0.092 |
| 12. I was aware that I still had a lot of feelings about it, but I didn’t deal with them. | 0.642 * | 0.197 * |
| 3. Other things kept making me think about it. | 0.634 * | 0.205 * |
| 10. I was jumpy and easily startled. | 0.618 * | 0.163 * |
| 21. I felt watchful and on guard. | 0.583 * | 0.167 * |
| 4. I felt irritable and angry. | 0.430 * | 0.406 * |
| Factor 2. Sleep disturbance | ||
| 2. I had trouble staying asleep. | 0.006 | 0.891 * |
| 15. I had trouble falling asleep. | 0.191 * | 0.732 * |
References
- World Health Organization Emergency Response Team Weekly Epidemiological Update on COVID-19—18 May 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---18-may-2021 (accessed on 19 May 2021).
- Salari, N.; Khazaie, H.; Hosseinian-Far, A.; Khaledi-Paveh, B.; Kazeminia, M.; Mohammadi, M.; Shohaimi, S.; Daneshkhah, A.; Eskandari, S. The prevalence of stress, anxiety and depression within front-line healthcare workers caring for COVID-19 patients: A systematic review and meta-regression. Hum. Resour. Health 2020, 18, 100. [Google Scholar] [CrossRef]
- Carmassi, C.; Foghi, C.; Dell’Oste, V.; Cordone, A.; Bertelloni, C.A.; Bui, E.; Dell’Osso, L. PTSD symptoms in healthcare workers facing the three coronavirus outbreaks: What can we expect after the COVID-19 pandemic. Psychiatry Res. 2020, 292, 113312. [Google Scholar] [CrossRef]
- Kameg, B.N. Psychiatric-mental health nursing leadership during coronavirus disease 2019 (COVID-19). J. Psychiatr. Ment. Health Nurs. 2020, 28, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Khanlou, N.; Orazietti, B.E. Nurses respond to COVID-19 pandemic: Mental health support for frontline nurses. Int. N. Y. Integr. 2020, 10, 27–28. [Google Scholar]
- Eun, H.; Kwon, T.; Lee, S.; Kim, T.; Choi, M.; Cho, S. A Study on reliability and validity of the Korean version of Impact of Event Scale-Revised. J. Korean Neuropsychiatr. Assoc. 2005, 44, 303–310. [Google Scholar]
- Horowitz, M.; Wilner, N.; Alvarez, W. Impact of Event Scale: A measure of subjective stress. Psychosom. Med. 1979, 41, 209–218. [Google Scholar] [CrossRef] [Green Version]
- Weiss, D.S.; Marmar, C.R. The impact of event scale-revised. In Assessing Psychological Trauma and PTSD; Wilson, J.P., Keane, T.M., Eds.; Guilford Press: New York, NY, USA, 1997; pp. 399–411. [Google Scholar]
- Lim, H.K.; Woo, J.M.; Kim, T.S.; Kim, T.H.; Choi, K.S.; Chung, S.K.; Chee, I.S.; Lee, K.U.; Paik, K.C.; Seo, H.J.; et al. Reliability and validity of the Korean version of the Impact of Event Scale-Revised. Compr. Psychiatry 2009, 50, 385–390. [Google Scholar] [CrossRef]
- Wu, K.K.; Chan, K.S. The development of the Chinese version of Impact of Event Scale—Revised (CIES-R). Soc. Psychiatry Psychiatr. Epidemiol. 2003, 38, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Sveen, J.; Low, A.; Dyster-Aas, J.; Ekselius, L.; Willebrand, M.; Gerdin, B. Validation of a Swedish version of the Impact of Event Scale-Revised (IES-R) in patients with burns. J. Anxiety Disord. 2010, 24, 618–622. [Google Scholar] [CrossRef]
- Brunet, A.; St-Hilaire, A.; Jehel, L.; King, S. Validation of a French version of the impact of event scale-revised. Can. J. Psychiatry 2003, 48, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.; Zhang, J.; Shi, Z.; Zhou, M.; Huang, D.; Liu, P. Confirmatory factor analysis of posttraumatic stress symptoms assessed by the Impact of Event Scale-Revised in Chinese earthquake victims: Examining factor structure and its stability across sex. J. Anxiety Disord. 2011, 25, 369–375. [Google Scholar] [CrossRef] [PubMed]
- Morina, N.; Böhme, H.F.; Ajdukovic, D.; Bogic, M.; Franciskovic, T.; Galeazzi, G.M.; Kucukalic, A.; Lecic-Tosevski, D.; Popovski, M.; Schützwohl, M.; et al. The structure of post-traumatic stress symptoms in survivors of war: Confirmatory factor analyses of the Impact of Event Scale--revised. J. Anxiety Disord. 2010, 24, 606–611. [Google Scholar] [CrossRef] [PubMed]
- Vanaken, L.; Scheveneels, S.; Belmans, E.; Hermans, D. Validation of the Impact of Event Scale With Modifications for COVID-19 (IES-COVID19). Front. Psychiatry 2020, 11, 738. [Google Scholar] [CrossRef]
- Grassi, M.; Pellizzoni, S.; Vuch, M.; Apuzzo, G.M.; Agostini, T.; Murgia, M. Psychometric Properties of the Syrian Arabic Version of the Impact of Event Scale-Revised in the Context of the Syrian Refugee Crisis. J. Trauma. Stress 2021. [Google Scholar] [CrossRef]
- Tabachnick, B.G.; Fidell, L.S. Using Multivariate Statistics, 4th ed.; Ally and Bacon: Boston, MA, USA, 2001. [Google Scholar]
- Park, J.E.; Kim, W.H.; Roh, D.; Won, S.D.; Kim, H.K.; Kang, S.H.; Hong, N.; Park, S.Y.; Kim, D.; Chae, J.H. Workbook for Assessment in Disaster Behavioral Health; Korean Academy of Anxiety and Mood, Korea Mental Health Technology R&D Project: Uiwang, Korea, 2016. [Google Scholar]
- Brandes, D.; Ben-Schachar, G.; Gilboa, A.; Bonne, O.; Freedman, S.; Shalev, A.Y. PTSD symptoms and cognitive performance in recent trauma survivors. Psychiatry Res. 2002, 110, 231–238. [Google Scholar] [CrossRef]
- Regehr, C.; LeBlanc, V.R. PTSD, acute stress, performance and decision-making in emergency service workers. J. Am. Acad. Psychiatry Law 2017, 45, 184–192. [Google Scholar]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Lee, J.; Shin, C.; Ko, Y.-H.; Lim, J.; Joe, S.-H.; Kim, S.; Jung, I.-K.; Han, C. The Reliability and validity studies of the Korean version of the perceived stress scale. Korean J. Psychosom. Med. 2012, 20, 127–134. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.W.; Löwe, B. A Brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [Green Version]
- Seo, J.-G.; Cho, Y.W.; Lee, S.-J.; Lee, J.-J.; Kim, J.-E.; Moon, H.-J.; Park, S.-P. Validation of the generalized anxiety disorder-7 in people with epilepsy: A MEPSY study. Epilepsy Behav. 2014, 35, 59–63. [Google Scholar] [CrossRef]
- Forbes, D.; Hawthorne, G.; Elliott, P.; McHugh, T.; Biddle, D.; Creamer, M.; Novaco, R.W. A concise measure of anger in combat-related posttraumatic stress disorder. J. Trauma. Stress 2004, 17, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Steiger, J.H. Aspects of person-machine communication in structural modeling of correlations and covariances. Multivar. Behav. Res. 1988, 23, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 2nd ed.; Guilford Press: New York, NY, USA, 2005. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Education: Harlow, UK, 2013. [Google Scholar]
- DeVon, H.A.; Block, M.E.; Moyle-Wright, P.; Ernst, D.M.; Hayden, S.J.; Lazzara, D.J.; Savoy, S.M.; Kostas-Polston, E. A psychometric toolbox for testing validity and reliability. J. Nurs. Scholarsh. 2007, 39, 155–164. [Google Scholar] [CrossRef]
- Marvaldi, M.; Mallet, J.; Dubertret, C.; Moro, M.R.; Guessoum, S.B. Anxiety, depression, trauma-related, and sleep disorders among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2021, 126, 252–264. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Lee, D.-H.; Jung, H.-y.; Lee, D.-H. A Latent Profile Analysis: Patterns of PTSD symptom severity in South Korean Adults exposed to traumatic events. Korean J. Couns. 2020, 21, 125–147. [Google Scholar]

| Variables | Categories | Frequency (%) | Mean (SD) |
|---|---|---|---|
| Socio-demographic characteristics | |||
| Gender | Male | 24 (9.6) | |
| Female | 225 (90.4) | ||
| Age (years) | 31.42 (8.47) | ||
| 20–29 | 145 (58.2) | ||
| 30–39 | 65 (26.2) | ||
| 40≤ | 39 (15.6) | ||
| Marital Status | Single | 177 (71.1) | |
| Married | 72 (28.9) | ||
| Highest education level | Associate degree | 51 (20.5) | |
| Bachelor’s degree | 172 (69.1) | ||
| Postgraduate student | 11 (4.4) | ||
| Master’s or doctoral degree | 15 (6.0) | ||
| Job characteristics | |||
| COVID-19 -related task period (months) | 6.47 (3.77) | ||
| <6 | 88 (35.4) | ||
| 6≤, <12 | 84 (33.7) | ||
| 12≤ | 77 (30.9) | ||
| Years of Experience | 7.32 (7.60) | ||
| <1 | 21 (8.4) | ||
| 1≤, <3 | 54 (21.7) | ||
| 3≤, <5 | 41 (16.4) | ||
| 5≤, <10 | 37 (14.9) | ||
| 10 ≤ | 96 (38.6) | ||
| Position | Staff | 228 (91.6) | |
| Manager | 5 (2.0) | ||
| Others | 16 (6.4) | ||
| Institution 1 | Tertiary general hospital | 93 (31.2) | |
| General hospital | 110 (36.9) | ||
| Public health center | 38 (12.8) | ||
| Temporary screening clinic | 37 (12.4) | ||
| Long-term care hospital | 7 (2.3) | ||
| Others | 13 (4.4) | ||
| Mental health characteristics | |||
| IES-R | 17.66 (15.98) | ||
| <18 | 149 (59.8) | ||
| 18≤ | 100 (40.2) | ||
| PSS | 21.39 (6.08) | ||
| GAD-7 | 6.08 (5.44) | ||
| <10 | 195 (78.3) | ||
| 10≤ | 54 (21.7) | ||
| DAR-5 | 9.56 (4.37) | ||
| <12 | 177 (71.1) | ||
| 12≤ | 72 (28.9) | ||
| Items | Weiss et al. [8] | Lim et al. [9] | Eun et al. [6] |
|---|---|---|---|
| 1. Any reminder brought back feelings about it. | I | I | I |
| 2. I had trouble staying asleep. | I | H | S/N |
| 3. Other things kept making me think about it. | I | I | I |
| 4. I felt irritable and angry. | H | I | H |
| 5. I avoided letting myself get upset when I thought about it or was reminded of it. | A | A | A |
| 6. I thought about it when I didn’t mean to. | I | I | I |
| 7. I felt as if it hadn’t happened or wasn’t real. | A | N/D | S/N |
| 8. I stayed away from reminders about it. | A | I | A |
| 9. Pictures about it popped into my mind. | I | I | I |
| 10. I was jumpy and easily startled. | H | H | H |
| 11. I tried not to think about it. | A | A | A |
| 12. I was aware that I still had a lot of feelings about it, but I didn’t deal with them. | A | A | A |
| 13. My feelings about it were kind of numb. | A | N/D | S/N |
| 14. I found myself acting or feeling like I was back at that time. | I | N/D | H |
| 15. I had trouble falling asleep. | H | H | S/N |
| 16. I had waves of strong feelings about it. | I | I | I |
| 17. I tried to remove it from my memory. | A | A | A |
| 18. I had trouble concentrating. | H | H | H |
| 19. Reminders of it caused me to have physical reactions, such as sweating, trouble breathing, nausea, or a pounding heart. | H | I | H |
| 20. I had dreams about it. | I | H | S/N |
| 21. I felt watchful and on guard. | H | H | H |
| 22. I tried not to talk about it. | A | A | A |
| Items | Mean (SD) | Correlation with Total | α If Item Deleted | Factor 1 | Factor 2 | Factor 3 |
|---|---|---|---|---|---|---|
| Intrusion (Cronbach’s alpha = 0.933) | ||||||
| 1. Any reminder brought back feelings about it. | 0.98 (0.90) | 0.700 | 0.961 | 0.76 * | 0.00 | −0.02 |
| 3. Other things kept making me think about it. | 0.87 (0.91) | 0.756 | 0.961 | 0.74 * | 0.01 | 0.09 |
| 4. I felt irritable and angry. | 1.45 (1.19) | 0.691 | 0.962 | 0.70 * | −0.13 | 0.26 * |
| 5. I avoided letting myself get upset when I thought about it or was reminded of it. | 0.86 (1.03) | 0.803 | 0.960 | 0.87 * | 0.03 | −0.06 |
| 6. I thought about it when I didn’t mean to. | 0.93 (1.04) | 0.813 | 0.960 | 0.87 * | 0.03 | −0.06 |
| 9. Pictures about it popped into my mind. | 0.92 (1.01) | 0.791 | 0.960 | 0.88 * | 0.02 | −0.06 |
| 16. I had waves of strong feelings about it. | 0.73 (0.94) | 0.813 | 0.960 | 0.69 * | 0.16 | 0.01 |
| 20. I had dreams about it. | 0.73 (0.97) | 0.733 | 0.961 | 0.43 * | 0.30 | 0.09 |
| 21. I felt watchful and on guard. | 0.85 (1.01) | 0.683 | 0.961 | 0.34 * | 0.29 | 0.16 |
| Avoidance (Cronbach’s alpha = 0.937) | ||||||
| 7. I felt as if it hadn’t happened or wasn’t real. | 0.59 (0.89) | 0.673 | 0.961 | 0.07 | 0.68 * | −0.01 |
| 8. I stayed away from reminders about it. | 0.70 (0.99) | 0.795 | 0.960 | 0.32 * | 0.55 * | 0.00 |
| 10. I was jumpy and easily startled. | 0.66 (0.95) | 0.722 | 0.961 | 0.31 * | 0.36 * | 0.17 * |
| 11. I tried not to think about it. | 0.81 (0.99) | 0.801 | 0.960 | 0.40 * | 0.47 * | 0.01 |
| 12. I was aware that I still had a lot of feelings about it, but I didn’t deal with them. | 0.73 (0.97) | 0.758 | 0.961 | 0.33 * | 0.37 * | 0.19 * |
| 13. My feelings about it were kind of numb. | 0.62 (0.92) | 0.678 | 0.961 | −0.25 | 0.87 * | 0.23 |
| 14. I found myself acting or feeling like I was back at that time. | 0.55 (0.88) | 0.722 | 0.961 | 0.05 | 0.78 * | −0.05 |
| 17. I tried to remove it from my memory. | 0.49 (0.75) | 0.717 | 0.961 | 0.12 | 0.72 * | −0.05 |
| 18. I had trouble concentrating. | 0.85 (0.96) | 0.788 | 0.960 | 0.02 | 0.68 * | 0.26 * |
| 19. Reminders of it caused me to have physical reactions, such as sweating, trouble breathing, nausea, or a pounding heart. | 0.31 (0.63) | 0.559 | 0.963 | −0.02 | 0.71 * | -0.11 |
| 22. I tried not to talk about it. | 0.55 (0.85) | 0.741 | 0.961 | 0.13 | 0.71 * | -0.02 |
| Sleep disturbance (Cronbach’s alpha = 0.876) | ||||||
| 2. I had trouble staying asleep. | 1.26 (1.15) | 0.580 | 0.963 | 0.15 | 0.01 | 0.80 * |
| 15. I had trouble falling asleep. | 1.22 (1.23) | 0.664 | 0.962 | 0.00 | 0.27 * | 0.75 * |
| Factors | No. of Items | r (p) | ||
|---|---|---|---|---|
| PSS | GAD-7 | DAR-5 | ||
| Total score | 22 | 0.58 (<0.001) | 0.72 (<0.001) | 0.67 (<0.001) |
| Intrusion | 9 | 0.61 (<0.001) | 0.72 (<0.001) | 0.67 (<0.001) |
| Avoidance | 11 | 0.49 (<0.001) | 0.67 (<0.001) | 0.61 (<0.001) |
| Sleep disturbance | 2 | 0.48 (<0.001) | 0.51 (<0.001) | 0.48 (<0.001) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, Y.S.; Park, K.-H.; Lee, J. Validation of the Korean Version of Impact of Event Scale—Revised (IES-R) in Korean Nurses during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11311. https://doi.org/10.3390/ijerph182111311
Park YS, Park K-H, Lee J. Validation of the Korean Version of Impact of Event Scale—Revised (IES-R) in Korean Nurses during the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(21):11311. https://doi.org/10.3390/ijerph182111311
Chicago/Turabian StylePark, Young Suk, Kwang-Hi Park, and Juna Lee. 2021. "Validation of the Korean Version of Impact of Event Scale—Revised (IES-R) in Korean Nurses during the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 21: 11311. https://doi.org/10.3390/ijerph182111311