
Epidemiological Analysis of SARS-CoV-2 Transmission Dynamics in the State of Odisha, India: A Yearlong Exploratory Data Analysis




Abstract
:1. Introduction
2. Methods
2.1. Study Design and Data Sources
2.2. Analysis
3. Results
3.1. Confirmed Cases, Death Cases, Case Fatality Rates, and Crude Death Rates for 2020 Timeline
3.2. Confirmed Cases, Death Cases, Case Fatality Rates, and Crude Death Rates for 2021 Timeline
3.3. Incidence Rates for 2020 and 2021 Timelines
3.4. Yearlong Temperature Analysis
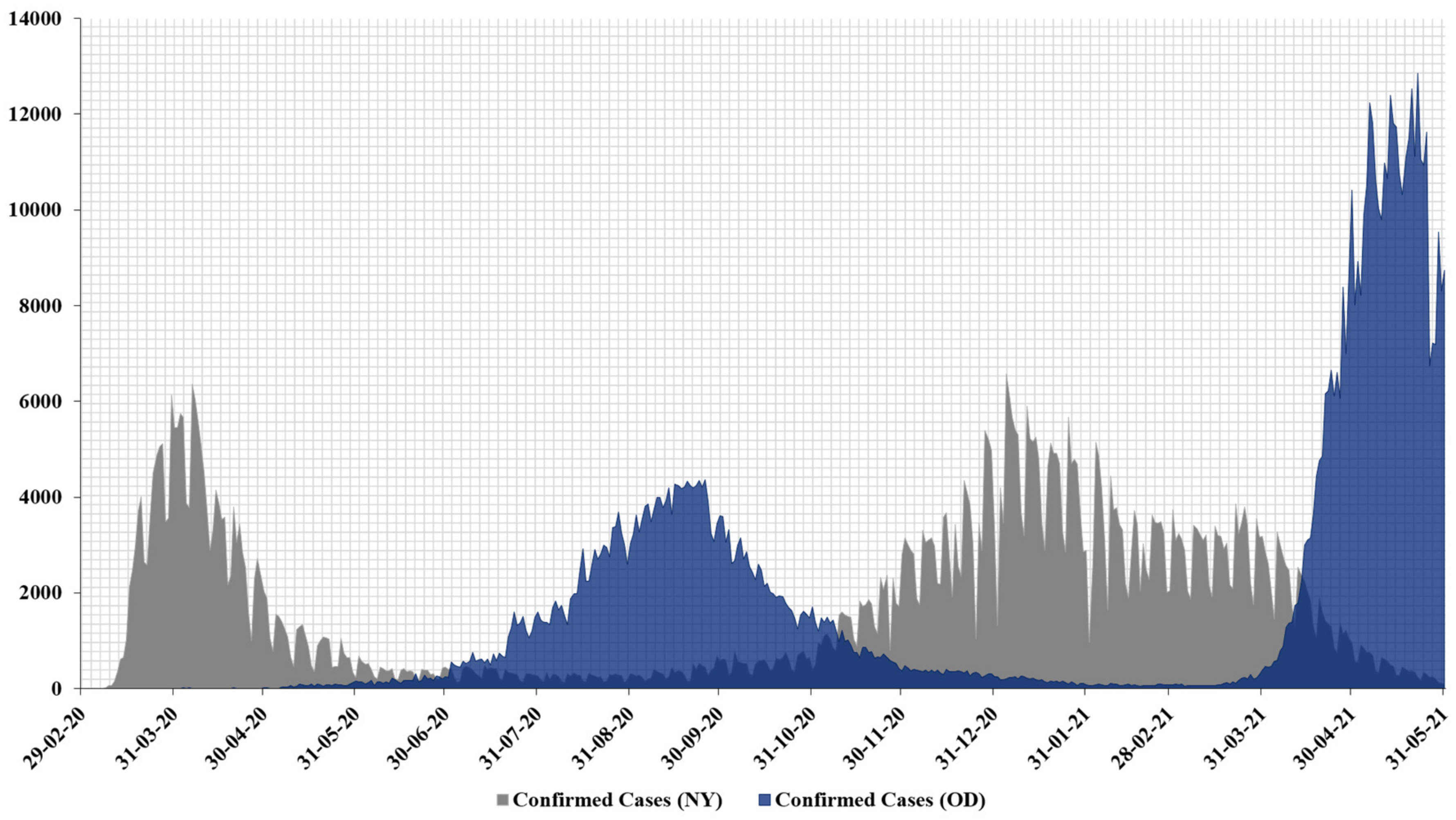
3.5. Yearlong Epidemiological Curve Analysis of COVID-19 Confirmed Cases
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| ACE2 | Angiotensin-converting enzyme 2 |
| CDC | Centers for Disease Control and Prevention |
| CDR | Crude death rate |
| CFR | Case fatality rate |
| COVID-19 | Coronavirus disease 2019 |
| MERS-CoV | Middle East respiratory syndrome coronavirus |
| NCIRD | National Center for Immunization and Respiratory Diseases |
| NY | State of New York |
| OD | State of Odisha |
| SARS-CoV | Severe acute respiratory syndrome coronavirus |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| S-protein | Spike protein |
| USA | United States of America |
| VOC | Variants of concern |
| WHO | World Health Organization |
References
- Cui, J.; Li, F.; Shi, Z.-L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [Green Version]
- Decaro, N.; Lorusso, A. Novel human coronavirus (SARS-CoV-2): A lesson from animal coronaviruses. Vet. Microbiol. 2020, 244, 108693. [Google Scholar] [CrossRef]
- Holshue, M.L.; DeBolt, C.; Lindquist, S.; Lofy, K.H.; Wiesman, J.; Bruce, H.; Spitters, C.; Ericson, K.; Wilkerson, S.; Tural, A. First case of 2019 novel coronavirus in the United States. N. Engl. J. Med. 2020, 382, 929–936. [Google Scholar] [CrossRef] [PubMed]
- Lai, C.-C.; Shih, T.-P.; Ko, W.-C.; Tang, H.-J.; Hsueh, P.-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and corona virus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef]
- WHO COVID 19 Public Health Emergency of International Concern (PHEIC). Global Research and Innovation Forum: Towards a Research Roadmap. Available online: https://www.who.int/publications/m/item/covid-19-public-health-emergency-of-international-concern- (accessed on 31 May 2021).
- WHO Novel Coronavirus—China. Available online: https://www.who.int/csr/don/12-january-2020-novel-coronavirus-china/en/ (accessed on 31 May 2021).
- Jiang, S.; Shi, Z.; Shu, Y.; Song, J.; Gao, G.F.; Tan, W.; Guo, D. A distinct name is needed for the new coronavirus. Lancet 2020, 395, 949. [Google Scholar] [CrossRef]
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species Severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536. [Google Scholar] [CrossRef] [Green Version]
- WHO. WHO Director-General’s Remarks at the Media Briefing on 2019-nCoV on 11 February 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-remarks-at-the-media-briefing-on-2019-ncov-on-11-february-2020 (accessed on 31 May 2021).
- WHO. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19---11-march-2020 (accessed on 31 May 2021).
- NPR Coronavirus Updates the Coronavirus has Reached Antarctica. Now It’s on Every Continent. Available online: https://www.npr.org/sections/coronavirus-live-updates/2020/12/23/949552848/the-coronavirus-has-reached-every-continent-after-positive-cases-in-antarctica (accessed on 31 May 2021).
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, S.F.; Quadeer, A.A.; McKay, M.R. Preliminary identification of potential vaccine targets for the COVID-19 coronavirus (SARS-CoV-2) based on SARS-CoV immunological studies. Viruses 2020, 12, 254. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walls, A.C.; Park, Y.-J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell 2020, 181, 281–292. [Google Scholar] [CrossRef]
- Cuervo, N.Z.; Grandvaux, N. ACE2: Evidence of role as entry receptor for SARS-CoV-2 and implications in comorbidities. Elife 2020, 9, e61390. [Google Scholar] [CrossRef] [PubMed]
- Poirier, C.; Luo, W.; Majumder, M.S.; Liu, D.; Mandl, K.D.; Mooring, T.A.; Santillana, M. The role of environmental factors on transmission rates of the COVID-19 outbreak: An initial assessment in two spatial scales. Sci. Rep. 2020, 10, 3552677. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Tang, K.; Feng, K.; Li, X.; Lv, W.; Chen, K.; Wang, F. High temperature and high humidity reduce the transmission of COVID-19. arXiv 2020, arXiv:2003.05003. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bherwani, H.; Gupta, A.; Anjum, S.; Anshul, A.; Kumar, R. Exploring dependence of COVID-19 on environmental factors and spread prediction in India. NPJ Clim. Atmos. Sci. 2020, 3, 38. [Google Scholar] [CrossRef]
- Laxminarayan, R.; Wahl, B.; Dudala, S.R.; Gopal, K.; Neelima, S.; Reddy, K.J.; Radhakrishnan, J.; Lewnard, J.A. Epidemiology and transmission dynamics of COVID-19 in two Indian states. Science 2020, 370, 691–697. [Google Scholar] [CrossRef]
- Kumar, S. Effect of meteorological parameters on spread of COVID-19 in India and air quality during lockdown. Sci. Total. Environ. 2020, 745, 141021. [Google Scholar] [CrossRef] [PubMed]
- Byun, W.S.; Heo, S.W.; Jo, G.; Kim, J.W.; Kim, S.; Lee, S.; Park, H.E.; Baek, J.-H. Is coronavirus disease (COVID-19) seasonal? A critical analysis of empirical and epidemiological studies at global and local scales. Environ. Res. 2021, 196, 110972. [Google Scholar] [CrossRef]
- World Health Organization Tracking SARS-CoV-2 Variants. Available online: https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/ (accessed on 31 May 2021).
- Centers for Disease Control & Prevention SARS-CoV-2 Variant Classifications and Definitions. Available online: https://www.cdc.gov/coronavirus/2019-ncov/variants/variant-info.html (accessed on 31 May 2021).
- Zhou, P.; Yang, X.-L.; Wang, X.-G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.-R.; Zhu, Y.; Li, B.; Huang, C.-L. Addendum: A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [Green Version]
- Srivastava, S.; Banu, S.; Singh, P.; Sowpati, D.T.; Mishra, R.K. SARS-CoV-2 genomics: An Indian perspective on sequencing viral variants. J. Biosci. 2021, 46, 22. [Google Scholar] [CrossRef]
- Korber, B.; Fischer, W.M.; Gnanakaran, S.; Yoon, H.; Theiler, J.; Abfalterer, W.; Hengartner, N.; Giorgi, E.E.; Bhattacharya, T.; Foley, B. Tracking changes in SARS-CoV-2 spike: Evidence that D614G increases infectivity of the COVID-19 virus. Cell 2020, 182, 812–827.e19. [Google Scholar] [CrossRef]
- Tegally, H.; Wilkinson, E.; Giovanetti, M.; Iranzadeh, A.; Fonseca, V.; Giandhari, J.; Doolabh, D.; Pillay, S.; San, E.J.; Msomi, N. Emergence and rapid spread of a new severe acute respiratory syndrome-related coronavirus 2 (SARS-CoV-2) lineage with multiple spike mutations in South Africa. MedRxiv 2020. [Google Scholar] [CrossRef]
- Chand, M.; Hopkins, S.; Dabrera, G.; Achison, C.; Barclay, W.; Ferguson, N.; Volz, E.; Loman, N.; Rambaut, A.; Barrett, J. Investigation of novel SARS-CoV-2 variant: Variant of concern 202012/01. In Public Health Engl.; 2020; Version 1, release date 21 December 2020. Available online: https://www.gov.uk/government/publications/investigation-of-novel-sars-cov-2-variant-variant-of-concern-20201201 (accessed on 31 May 2021).
- The New York Times. Available online: https://www.nytimes.com/2021/06/27/opinion/covid-vaccine-variants.html (accessed on 31 May 2021).
- Odisha State Dashboard. Available online: https://statedashboard.odisha.gov.in/ (accessed on 31 May 2021).
- Equator Network the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: Guidelines for Reporting Observational Studies. Available online: https://www.equator-network.org/reporting-guidelines/strobe/ (accessed on 31 May 2021).
- New York State Department of Health NYSDOH COVID-19 Tracker. Available online: https://covid19tracker.health.ny.gov/views/NYS-COVID19-Tracker/NYSDOHCOVID-19Tracker-Map?%3Aembed=yes&%3Atoolbar=no&%3Atabs=n,%20https://www1.nyc.gov/site/doh/covid/covid-19-data.page (accessed on 31 May 2021).
- GitHub Coronavirus Data. Available online: https://github.com/nychealth/coronavirus-data.git (accessed on 31 May 2021).
- United State Census Bureau. 2020. Available online: https://www.census.gov/ (accessed on 31 May 2021).
- Office of the Registrar General & Census Commissioner. 2020. Available online: https://censusindia.gov.in/ (accessed on 31 May 2021).
- CDC The Flu Season. Available online: https://www.cdc.gov/flu/about/season/flu-season.htm (accessed on 31 May 2021).
- Koul, P.A.; Broor, S.; Saha, S.; Barnes, J.; Smith, C.; Shaw, M.; Chadha, M.; Lal, R.B. Differences in influenza seasonality by latitude, northern India. Emerg. Infect. Dis. 2014, 20, 1723. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Gagliardi, M.C.; Tieri, P.; Ortona, E.; Ruggieri, A. ACE2 expression and sex disparity in COVID-19. Cell Death Discov. 2020, 6, 1–2. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.I.; Nikitara, K. COVID-19 and smoking: A systematic review of the evidence. Tob. Induc. Dis. 2020, 18, 20. [Google Scholar] [CrossRef]
- Ghosh, S.; Klein, R.S. Sex drives dimorphic immune responses to viral infections. J. Immunol. 2017, 198, 1782–1790. [Google Scholar] [CrossRef] [Green Version]
- Devaux, C.A.; Rolain, J.-M.; Raoult, D. ACE2 receptor polymorphism: Susceptibility to SARS-CoV-2, hypertension, multi-organ failure, and COVID-19 disease outcome. J. Microbiol. Immunol. Infect. 2020, 53, 425–435. [Google Scholar] [CrossRef]
- Kuba, K.; Imai, Y.; Rao, S.; Gao, H.; Guo, F.; Guan, B.; Huan, Y.; Yang, P.; Zhang, Y.; Deng, W. A crucial role of angiotensin converting enzyme 2 (ACE2) in SARS coronavirus–induced lung injury. Nat. Med. 2005, 11, 875–879. [Google Scholar] [CrossRef]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor recognition by the novel coronavirus from Wuhan: An analysis based on decade-long structural studies of SARS coronavirus. J. Virol. 2020, 94, e00127-20. [Google Scholar] [CrossRef] [Green Version]
- Zoufaly, A.; Poglitsch, M.; Aberle, J.H.; Hoepler, W.; Seitz, T.; Traugott, M.; Grieb, A.; Pawelka, E.; Laferl, H.; Wenisch, C. Human recombinant soluble ACE2 in severe COVID-19. Lancet Respir. Med. 2020, 8, 1154–1158. [Google Scholar] [CrossRef]
- Hanff, T.C.; Harhay, M.O.; Brown, T.S.; Cohen, J.B.; Mohareb, A.M. Is there an association between COVID-19 mortality and the renin-angiotensin system—A call for epidemiologic investigations. Clin. Infect. Dis. 2020, 71, 870–874. [Google Scholar] [CrossRef] [Green Version]
- Sama, I.E.; Ravera, A.; Santema, B.T.; van Goor, H.; Ter Maaten, J.M.; Cleland, J.G.; Rienstra, M.; Friedrich, A.W.; Samani, N.J.; Ng, L.L. Circulating plasma concentrations of angiotensin-converting enzyme 2 in men and women with heart failure and effects of renin–angiotensin–aldosterone inhibitors. Eur. Heart J. 2020, 41, 1810–1817. [Google Scholar] [CrossRef]
- Bukowska, A.; Spiller, L.; Wolke, C.; Lendeckel, U.; Weinert, S.; Hoffmann, J.; Bornfleth, P.; Kutschka, I.; Gardemann, A.; Isermann, B. Protective regulation of the ACE2/ACE gene expression by estrogen in human atrial tissue from elderly men. Exp. Biol. Med. 2017, 242, 1412–1423. [Google Scholar] [CrossRef]
- Channappanavar, R.; Fett, C.; Mack, M.; Ten Eyck, P.P.; Meyerholz, D.K.; Perlman, S. Sex-based differences in susceptibility to severe acute respiratory syndrome coronavirus infection. J. Immunol. 2017, 198, 4046–4053. [Google Scholar] [CrossRef]
- Shabbir, S.; Hafeez, A.; Rafiq, M.A.; Khan, M.J. Estrogen shields women from COVID-19 complications by reducing ER stress. Med. Hypotheses 2020, 143, 110148. [Google Scholar] [CrossRef] [PubMed]
- Eslami, H.; Jalili, M. The role of environmental factors to transmission of SARS-CoV-2 (COVID-19). AMB Express 2020, 10, 92. [Google Scholar] [CrossRef]
- Ma, Y.; Zhao, Y.; Liu, J.; He, X.; Wang, B.; Fu, S.; Yan, J.; Niu, J.; Zhou, J.; Luo, B. Effects of temperature variation and humidity on the death of COVID-19 in Wuhan, China. Sci. Total Environ. 2020, 724, 138226. [Google Scholar] [CrossRef] [PubMed]
- Bashir, M.F.; Ma, B.; Komal, B.; Bashir, M.A.; Tan, D.; Bashir, M. Correlation between climate indicators and COVID-19 pandemic in New York, USA. Sci. Total Environ. 2020, 728, 138835. [Google Scholar] [CrossRef] [PubMed]
- Oliveiros, B.; Caramelo, L.; Ferreira, N.C.; Caramelo, F. Role of temperature and humidity in the modulation of the doubling time of COVID-19 cases. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Lian, X.; Huang, J.; Zhang, L.; Liu, C.; Liu, X.; Wang, L. Environmental indicator for effective control of COVID-19 spreading. MedRxiv 2020. [Google Scholar] [CrossRef]
- Kudo, E.; Song, E.; Yockey, L.J.; Rakib, T.; Wong, P.W.; Homer, R.J.; Iwasaki, A. Low ambient humidity impairs barrier function and innate resistance against influenza infection. Proc. Natl. Acad. Sci. USA 2019, 116, 10905–10910. [Google Scholar] [CrossRef] [Green Version]
- Casanova, L.M.; Jeon, S.; Rutala, W.A.; Weber, D.J.; Sobsey, M.D. Effects of air temperature and relative humidity on coronavirus survival on surfaces. Appl. Environ. Microbiol. 2010, 76, 2712–2717. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Wilde, A.H.; Snijder, E.J.; Kikkert, M.; van Hemert, M.J. Host factors in coronavirus replication. Roles Host Gene Non-Coding RNA Expr. Virus Infect. 2017, 419, 1–42. [Google Scholar]
- Rath, S.L.; Kumar, K. Investigation of the effect of temperature on the structure of SARS-Cov-2 Spike Protein by Molecular Dynamics Simulations. Front. Mol. Biosci. 2020, 7, 583523. [Google Scholar] [CrossRef]
- Singh, J.; Rahman, S.A.; Ehtesham, N.Z.; Hira, S.; Hasnain, S.E. SARS-CoV-2 variants of concern are emerging in India. Nat. Med. 2021, 27, 1131–1133. [Google Scholar] [CrossRef] [PubMed]
- Mint Covid-19: Odisha Reports First Case of Delta Plus Variant. Available online: https://www.livemint.com/news/india/covid19-odisha-reports-first-case-of-delta-plus-variant-11624630506671.html (accessed on 31 May 2021).
- BBC News Delta Plus India: Scientists Say Too Early to Tell Risk of COVID-19 Variant. Available online: https://www.bbc.com/news/world-asia-india-57564560 (accessed on 14 October 2021).
- The New Indian Express COVID-19: Delta Variant Dominates Odisha, Accounts for 98 Percent of Sequenced Samples. Available online: https://www.newindianexpress.com/states/odisha/2021/jul/15/covid-19-delta-variant-dominates-odisha-accounts-for-98-per-cent-of-sequenced-samples-2330378.html (accessed on 14 October 2021).
- Lauring, A.S.; Hodcroft, E.B. Genetic variants of SARS-CoV-2—What do they mean? JAMA 2021, 325, 529–531. [Google Scholar] [CrossRef]
- Harvey, W.T.; Carabelli, A.M.; Jackson, B.; Gupta, R.K.; Thomson, E.C.; Harrison, E.M.; Ludden, C.; Reeve, R.; Rambaut, A.; Peacock, S.J. SARS-CoV-2 variants, spike mutations and immune escape. Nat. Rev. Microbiol. 2021, 19, 409–424. [Google Scholar] [CrossRef]
- Bakhshandeh, B.; Jahanafrooz, Z.; Abbasi, A.; Goli, M.B.; Sadeghi, M.; Mottaqi, M.S.; Zamani, M. Mutations in SARS-CoV-2; Consequences in structure, function, and pathogenicity of the virus. Microb. Pathog. 2021, 154, 104831. [Google Scholar] [CrossRef]
- Krause, P.R.; Fleming, T.R.; Longini, I.M.; Peto, R.; Briand, S.; Heymann, D.L.; Beral, V.; Snape, M.D.; Rees, H.; Ropero, A.-M. SARS-CoV-2 Variants and Vaccines. N. Engl. J. Med. 2021, 385, 179–186. [Google Scholar] [CrossRef]
- Abdool Karim, S.S.; de Oliveira, T. New SARS-CoV-2 variants—Clinical, public health, and vaccine implications. N. Engl. J. Med. 2021, 384, 1866–1868. [Google Scholar] [CrossRef]
- Pattabiraman, C. Tracking SARS-COV-2 Variants of Concern. Available online: https://www.orfonline.org/research/tracking-sars-cov-2-variants-of-concern/ (accessed on 31 May 2021).
- Altmann, D.M.; Boyton, R.J.; Beale, R. Immunity to SARS-CoV-2 variants of concern. Science 2021, 371, 1103–1104. [Google Scholar] [CrossRef]
- Rashed, E.A.; Kodera, S.; Gomez-Tames, J.; Hirata, A. Influence of absolute humidity, temperature and population density on COVID-19 spread and decay durations: Multi-prefecture study in Japan. Int. J. Environ. Res. Public Health 2020, 17, 5354. [Google Scholar] [CrossRef] [PubMed]
- Diao, Y.; Kodera, S.; Anzai, D.; Gomez-Tames, J.; Rashed, E.A.; Hirata, A. Influence of population density, temperature, and absolute humidity on spread and decay durations of COVID-19: A comparative study of scenarios in China, England, Germany, and Japan. One Health 2021, 12, 100203. [Google Scholar] [CrossRef] [PubMed]
- Ganasegeran, K.; Jamil, M.F.A.; Ch’ng, A.S.H.; Looi, I.; Peariasamy, K.M. Influence of Population Density for COVID-19 Spread in Malaysia: An Ecological Study. Int. J. Environ. Res. Public Health 2021, 18, 9866. [Google Scholar] [CrossRef] [PubMed]
- Deccan Herald Odisha Extends Lockdown to Entire State from March 24 Midnight. Available online: https://www.deccanherald.com/national/east-and-northeast/odisha-extends-lockdown-to-entire-state-from-march-24-midnight-817162.html (accessed on 31 May 2020).
- Kumar, V.M.; Pandi-Perumal, S.R.; Trakht, I.; Thyagarajan, S.P. Strategy for COVID-19 vaccination in India: The country with the second highest population and number of cases. NPJ Vaccines 2021, 6, 60. [Google Scholar] [CrossRef] [PubMed]
- New 18 Odisha Targets to Complete Vaccination Drive by December 2021. Available online: https://www.news18.com/news/india/odisha-targets-to-complete-vaccination-drive-by-december-2021-4150097.html (accessed on 14 October 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Baseline Characteristics | Confirmed Cases n (%) | Death Cases n (%) | Case Fatality Rates (%) | Crude Death Rates per 100,000 of the Population (%) | ||||
|---|---|---|---|---|---|---|---|---|
| OD | NY | OD | NY | OD | NY | OD | NY | |
| Overall/Total | 2223 | 203,006 | 7 | 17,766 | 0.3 | 8.8 | 0.015 | 91.175 |
| Age group, years 0–14 15–40 41–60 60+ Missing | ||||||||
57 (2.6) 1317 (59.2) 492 (22.1) 82 (3.7) 275 (12.4) | 4955 (2.4) 69,610 (34.3) 69,402 (34.2) 46,021 (22.7) 13,018 (6.4) | 0 (0) 2 (0.15) 0 (0) 5 (6.09) 0 (0) | 10 (0.2) 625 (0.8) 3556 (5.1) 11,694 (25.4) 1881 (14.4) | 0.0 0.2 0.0 6.1 0.0 | 0.2 0.9 5.1 25.4 14.4 | 0.0 0.004 0.0 0.011 0.0 | 0.051 3.208 18.249 60.014 9.653 | |
| Gender-wise Male Female Unknown | ||||||||
1702 (76.6) 246 (11.1) 275 (12.4) | 98,038 (48.3) 92,228 (45.4) 12,740 (6.3) | 7 (0.4) 0 (0) 0 (0) | 9634 (9.8) 6223 (6.7) 1909 (14.9) | 0.4 0.0 0.0 | 9.8 6.7 15 | 0.030 0.0 0.0 | 101.841 62.088 9.798 | |
| Period (date of onset) Before March 2020 1–31 March 2020 1–30 April 2020 1–31 May 2020 | ||||||||
0 (0.0) 5 (0.2) 148 (6.7) 2070 (93.1) | 1 (0.0) 65,203 (32.1) 109,342 (53.9) 28,460 (14) | 0 (0.0) 0 (0.0) 1 (14.3) 6 (85.7) | 0 (0.0) 2193 (12.3) 12,742 (71.7) 2831 (15.9) | - 0.0 0.7 0.3 | 0.0 3.4 11.7 9.9 | 0.0 0.0 0.002 0.013 | 0.0 11.255 65.392 14.529 | |
| Baseline Characteristics | Confirmed Cases n (%) | Death Cases n (%) | Case Fatality Rates (%) | Crude Death Rates per 100,000 of the Population (%) | ||||
|---|---|---|---|---|---|---|---|---|
| OD | NY | OD | NY | OD | NY | OD | NY | |
| Overall/Total (1 March–31 May 2021) | 436,455 | 159,364 | 875 | 3570 | 0.2 | 2.2 | 1.84 | 17.50 |
| Age group and gender distribution | *** Case data could not be retrieved *** | |||||||
| Period (date of onset) Before March 2021 1–31 March 2021 1–30 April 2021 1–31 May 2021 | ||||||||
7411 4034 113,296 319,125 | 223,871 91,966 54,294 13,104 | 40 5 133 737 | 4192 1782 1232 556 | 0.5 0.1 0.1 0.2 | 1.9 1.9 2.3 4.2 | 0.08 0.01 0.28 1.55 | 20.55 8.74 6.04 2.73 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nasker, S.S.; Nanda, A.; Ramadass, B.; Nayak, S. Epidemiological Analysis of SARS-CoV-2 Transmission Dynamics in the State of Odisha, India: A Yearlong Exploratory Data Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11203. https://doi.org/10.3390/ijerph182111203
Nasker SS, Nanda A, Ramadass B, Nayak S. Epidemiological Analysis of SARS-CoV-2 Transmission Dynamics in the State of Odisha, India: A Yearlong Exploratory Data Analysis. International Journal of Environmental Research and Public Health. 2021; 18(21):11203. https://doi.org/10.3390/ijerph182111203
Chicago/Turabian StyleNasker, Sourya Subhra, Ananya Nanda, Balamurugan Ramadass, and Sasmita Nayak. 2021. "Epidemiological Analysis of SARS-CoV-2 Transmission Dynamics in the State of Odisha, India: A Yearlong Exploratory Data Analysis" International Journal of Environmental Research and Public Health 18, no. 21: 11203. https://doi.org/10.3390/ijerph182111203