
Determinants of Vaccine Acceptance against COVID-19 in China: Perspectives on Knowledge and DrVac-COVID19S Scale

 ,
,
Abstract
:1. Introduction
2. Methodology
2.1. Participants
2.2. Self-Reported Questionnaires
2.3. Data Analysis
3. Results
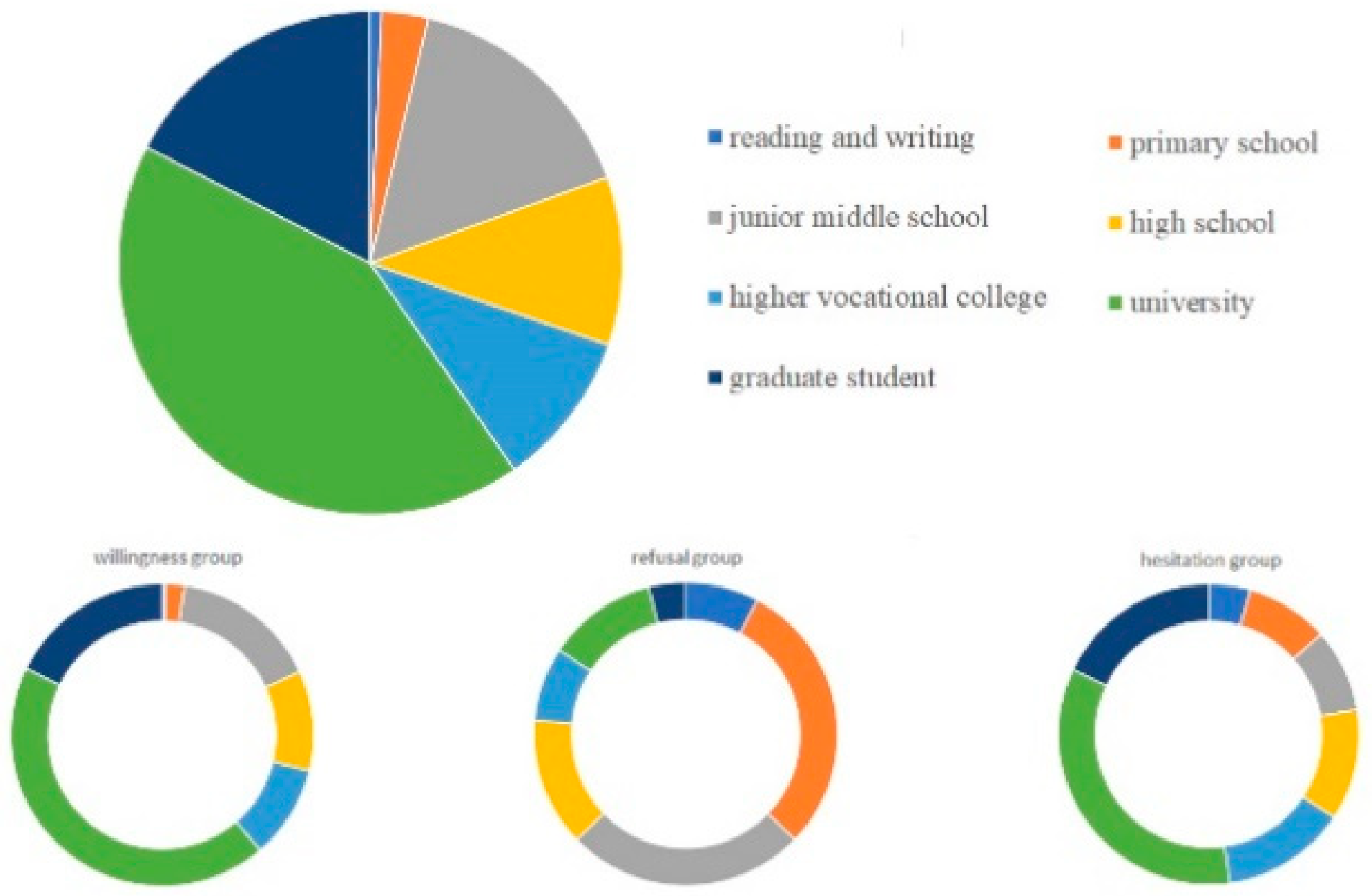
3.1. Participant Characteristics
3.2. Differences between Willing/Unwilling/Hesitant Attitudes in Relation to Socioeconomic Items
3.3. Differences between Willing/Unwilling/Hesitant Attitudes in Relation to Knowledge of COVID-19
3.4. Differences between Willing/Unwilling/Hesitant Attitudes in Relation to Preventive Measures/Behaviors of COVID-19
3.5. Differences between Willing/Unwilling/Hesitant Attitudes in Relation to Knowledge of COVID-19 Vaccination
3.6. Logistic Regression Analysis of Vaccination Attitudes of Willingness and Hesitation (Refusal)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Zeyaullah, M.; AlShahrani, A.M.; Muzammil, K.; Ahmad, I.; Alam, S.; Khan, W.H.; Ahmad, R. COVID-19 and SARS-CoV-2 Variants: Current Challenges and Health Concern. Front. Genet. 2021, 12, 693916. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, S.H.; Mansatta, K.; Mallett, G.; Harris, V.; Emary, K.R.W.; Pollard, A.J. What defines an efficacious COVID-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2. Lancet Infect. Dis. 2021, 21, e26–e35. [Google Scholar] [CrossRef]
- Anderson, R.M.; Vegvari, C.; Truscott, J.; Collyer, B.S. Challenges in creating herd immunity to SARS-CoV-2 infection by mass vaccination. Lancet 2020, 396, 1614–1616. [Google Scholar] [CrossRef]
- Omer, S.B.; Salmon, D.A.; Orenstein, W.A.; de Hart, M.P.; Halsey, N. Vaccine refusal, mandatory immunization, and the risks of vaccine-preventable diseases. N. Engl. J. Med. 2009, 360, 1981–1988. [Google Scholar] [CrossRef]
- Lazarus, J.V.; Ratzan, S.C.; Palayew, A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Kimball, S.; El-Mohandes, A. A global survey of potential acceptance of a COVID-19 vaccine. Nat. Med. 2021, 27, 225–228. [Google Scholar] [CrossRef]
- MacDonald, N.E.; the SAGE Working Group on Vaccine Hesitancy. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Lin, C.; Tu, P.; Beitsch, L.M. Confidence and Receptivity for COVID-19 Vaccines: A Rapid Systematic Review. Vaccines 2020, 9, 16. [Google Scholar] [CrossRef]
- Larson, H.J.; Clarke, R.M.; Jarrett, C.; Eckersberger, E.; Levine, Z.; Schulz, W.S.; Paterson, P. Measuring trust in vaccination: A systematic review. Hum. Vaccines Immunother. 2018, 14, 1599–1609. [Google Scholar] [CrossRef]
- Xiao, X.; Wong, R.M. Vaccine hesitancy and perceived behavioral control: A meta-analysis. Vaccine 2020, 38, 5131–5138. [Google Scholar] [CrossRef]
- Setbon, M.; Raude, J. Factors in vaccination intention against the pandemic influenza A/H1N1. Eur. J. Public Health 2010, 20, 490–494. [Google Scholar] [CrossRef] [Green Version]
- Halpin, C.; Reid, B. Attitudes and beliefs of healthcare workers about influenza vaccination. Nurs. Older People 2019, 31, 32–39. [Google Scholar] [CrossRef]
- Wang, J.; Jing, R.; Lai, X.; Zhang, H.; Lyu, Y.; Knoll, M.D.; Fang, H. Acceptance of COVID-19 Vaccination during the COVID-19 Pandemic in China. Vaccines 2020, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Yeh, Y.C.; Chen, I.H.; Ahorsu, D.K.; Ko, N.-Y.; Chen, K.L.; Li, P.-C.; Yen, C.-F.; Lin, C.-Y.; Griffiths, M.D.; Pakpour, A.H. Measurement Invariance of the Drivers of COVID-19 Vaccination Acceptance Scale: Comparison between Taiwanese and Mainland Chinese-Speaking Populations. Vaccines 2021, 9, 297. [Google Scholar] [CrossRef] [PubMed]
- Abdelhafiz, A.S.; Mohammed, Z.; Ibrahim, M.E.; Ziady, H.H.; Alorabi, M.; Ayyad, M.; Sultan, E.A. Knowledge, Perceptions, and Attitude of Egyptians Towards the Novel Coronavirus Disease (COVID-19). J. Community Health 2020, 45, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Zhong, G.; Zhang, J.; Shuai, L.; Zhang, Z.; Wen, Z.; Wang, B.; Zhao, Z.; Song, X.; Chen, Y. A single dose of an adenovirus-vectored vaccine provides protection against SARS-CoV-2 challenge. Nat. Commun. 2020, 11, 4081. [Google Scholar] [CrossRef]
- Lin, Y.; Hu, Z.; Zhao, Q.; Alias, H.; Danaee, M.; Wong, L.P. Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl. Trop. Dis. 2020, 14, e0008961. [Google Scholar] [CrossRef] [PubMed]
- Prati, G. Intention to receive a vaccine against SARS-CoV-2 in Italy and its association with trust, worry and beliefs about the origin of the virus. Health Educ. Res. 2020, 35, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Detoc, M.; Bruel, S.; Frappe, P.; Tardy, B.; Botelho-Nevers, E.; Gagneux-Brunon, A. Intention to participate in a COVID-19 vaccine clinical trial and to get vaccinated against COVID-19 in France during the pandemic. Vaccine 2020, 38, 7002–7006. [Google Scholar] [CrossRef] [PubMed]
- Wong, L.P.; Alias, H.; Wong, P.F.; Lee, H.Y.; AbuBakar, S. The use of the health belief model to assess predictors of intent to receive the COVID-19 vaccine and willingness to pay. Hum. Vaccines Immunother. 2020, 16, 2204–2214. [Google Scholar] [CrossRef] [PubMed]
- Nzaji, M.K.; Ngombe, L.K.; Mwamba, G.N.; Ndala, D.B.B.; Miema, J.M.; Lungoyo, C.L.; Mwimba, B.L.; Bene, A.C.M.; Musenga, E.M. Acceptability of Vaccination Against COVID-19 Among Healthcare Workers in the Democratic Republic of the Congo. Pragmat. Obs. Res. 2020, 11, 103–109. [Google Scholar] [CrossRef]
- Reuben, R.C.; Danladi, M.M.A.; Saleh, D.A.; Ejembi, P.E. Knowledge, Attitudes and Practices Towards COVID-19: An Epidemiological Survey in North-Central Nigeria. J. Community Health 2021, 46, 457–470. [Google Scholar] [CrossRef]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef]
- Harapan, H.; Wagner, A.L.; Yufika, A.; Winardi, W.; Anwar, S.; Gan, A.K.; Setiawan, A.M.; Rajamoorthy, Y.; Sofyan, H.; Mudatsir, M. Acceptance of a COVID-19 Vaccine in Southeast Asia: A Cross-Sectional Study in Indonesia. Front. Public Health 2020, 8, 381. [Google Scholar] [CrossRef] [PubMed]
- Bhopal, S.; Nielsen, M. Vaccine hesitancy in low- and middle-income countries: Potential implications for the COVID-19 response. Arch. Dis. Child. 2021, 106, 113–114. [Google Scholar] [CrossRef]
- Bell, S.; Clarke, R.; Mounier-Jack, S.; Walker, J.L.; Paterson, P. Parents’ and guardians’ views on the acceptability of a future COVID-19 vaccine: A multi-methods study in England. Vaccine 2020, 38, 7789–7798. [Google Scholar] [CrossRef]
- Palamenghi, L.; Barello, S.; Boccia, S.; Graffigna, G. Mistrust in biomedical research and vaccine hesitancy: The forefront challenge in the battle against COVID-19 in Italy. Eur. J. Epidemiol. 2020, 35, 785–788. [Google Scholar] [CrossRef] [PubMed]
- Guidry, J.P.D.; Laestadius, L.I.; Vraga, E.K.; Miller, C.A.; Perrin, P.B.; Burton, C.W.; Ryan, M.; Fuemmeler, B.F.; Carlyle, K.E. Willingness to get the COVID-19 vaccine with and without emergency use authorization. Am. J. Infect. Control 2021, 49, 137–142. [Google Scholar] [CrossRef]
- Borriello, A.; Master, D.; Pellegrini, A.; Rose, J.M. Preferences for a COVID-19 vaccine in Australia. Vaccine 2021, 39, 473–479. [Google Scholar] [CrossRef]
- Amanna, I.; Slifka, M.K. Public fear of vaccination: Separating fact from fiction. Viral Immunol. 2005, 18, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Bish, A.; Yardley, L.; Nicoll, A.; Michie, S. Factors associated with uptake of vaccination against pandemic influenza: A systematic review. Vaccine 2011, 29, 6472–6484. [Google Scholar] [CrossRef] [PubMed]
- Smith, L.E.; Amlot, R.; Weinman, J.; Yiend, J.; Rubin, G.J. A systematic review of factors affecting vaccine uptake in young children. Vaccine 2017, 35, 6059–6069. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Items | All | Attitude of Being Vaccinated | p | ||
|---|---|---|---|---|---|
| Willingness | Refusal | Hesitation | |||
| Attitude of vaccination | 1910 (100) | 1792 (93.8) | 51 (2.7) | 67 (3.5) | --- |
| Age, years | <0.001 | ||||
| 18–<30 | 423 (22.1) | 407 (22.7) | 6 (11.8) | 10 (14.9) | |
| 30–<40 | 598 (31.3) | 576 (32.1) | 6 (11.8) | 16 (23.9) | |
| 40–<50 | 535 (28) | 510 (28.5) | 8 (15.7) | 17 (25.4) | |
| 50–<60 | 271 (14.2) | 249 (13.9) | 10 (19.6) | 12 (17.9) | |
| ≥60 | 83 (4.3) | 50 (2.8) | 21 (41.2) | 12 (17.9) | |
| Gender | 0.955 | ||||
| male | 713 (37.3) | 670 (37.4) | 18 (35.3) | 25 (37.3) | |
| female | 1199 (62.7) | 1122 (62.6) | 33 (64.7) | 42 (62.7) | |
| Place of residence | <0.001 | ||||
| urban | 1503 (78.7) | 1423 (79.4) | 27 (52.9) | 53 (79.1) | |
| Rural | 407 (21.3) | 369 (20.6) | 24 (47.1) | 14 (20.9) | |
| Marital status | 0.026 | ||||
| married | 1550 (81.2) | 1444 (80.6) | 48 (94.1) | 58 (86.6) | |
| others | 360 (18.8) | 348 (19.4) | 3 (5.9) | 9 (13.4) | |
| Educational level | <0.001 | ||||
| reading and writing | 14 (0.7) | 7 (0.4) | 4 (7.8) | 3 (4.5) | |
| primary school | 57 (3) | 36 (2) | 15 (29.4) | 6 (9) | |
| junior middle school | 301 (15.8) | 282 (15.7) | 13 (25.5) | 6 (9) | |
| high school | 206 (10.8) | 191 (10.7) | 7 (13.7) | 8 (11.9) | |
| higher vocational college | 192 (10) | 179 (10) | 4 (7.8) | 9 (13.4) | |
| university | 808 (42.3) | 779 (43.5) | 6 (11.8) | 23 (34.3) | |
| graduate student | 332 (17.4) | 318 (17.7) | 2 (3.9) | 12 (17.9) | |
| Yearly per capita income, RMB | <0.001 | ||||
| <50,000 | 468 (24.5) | 413 (23.1) | 34 (66.7) | 21 (31.3) | |
| 50,000–100,000 | 658 (34.5) | 624 (34.8) | 12 (23.5) | 22 (32.8) | |
| >100,000 | 784 (41) | 755 (42.1) | 5 (9.8) | 24 (35.8) | |
| Tobacco use | 0.940 | ||||
| yes | 208 (10.9) | 194 (10.8) | 6 (11.8) | 8 (11.9) | |
| no | 1702 (89.1) | 1598 (89.2) | 45 (88.2) | 59 (88.1) | |
| Alcohol use | 0.532 | ||||
| yes | 104 (5.4) | 99 (5.5) | 1 (2) | 4 (6) | |
| no | 1806 (94.6) | 1693 (94.5) | 50 (98) | 63 (94) | |
| Health status | <0.001 | ||||
| health | 1647 (86.2) | 1596 (89.1) | 11 (21.6) | 40 (59.7) | |
| chronic disease | 263 (13.8) | 196 (10.9) | 40 (78.4) | 27 (40.3) | |
| Living alone | 0.756 | ||||
| yes | 126 (6.6) | 120 (6.7) | 3 (5.9) | 3 (4.5) | |
| no | 1784 (93.4) | 1672 (93.3) | 48 (94.1) | 64 (95.5) | |
| Have children at home | 0.324 | ||||
| yes | 1573 (82.4) | 1476 (82.4) | 45 (88.2) | 52 (77.6) | |
| no | 337 (17.6) | 316 (17.6) | 6 (11.8) | 15 (22.4) | |
| Items | All | Attitude of Being Vaccinated | p | ||
|---|---|---|---|---|---|
| Willingness | Refusal | Hesitation | |||
| COVID-19 spreads by | |||||
| 1. Droplets of affected person (with cough or expiration) | <0.001 | ||||
| yes | 1802 (94.3) | 1711 (95.5) | 32 (62.7) | 59 (88.1) | |
| no | 108 (5.7) | 81 (4.5) | 19 (37.3) | 8 (11.9) | |
| 2. Surfaces touched by affected person | <0.001 | ||||
| yes | 1242 (65) | 1193 (66.6) | 14 (27.5) | 35 (52.2) | |
| no | 668 (35) | 599 (33.4) | 37 (72.5) | 32 (47.8) | |
| 3. Aerosol transmission | <0.001 | ||||
| yes | 1150 (60.2) | 1113 (62.1) | 10 (19.6) | 27 (40.3) | |
| no | 760 (39.8) | 679 (37.9) | 41 (80.4) | 40 (59.7) | |
| 4.Transmission through food and water | <0.001 | ||||
| yes | 858 (44.9) | 828 (46.2) | 6 (11.8) | 24 (35.8) | |
| no | 1052 (55.1) | 964 (53.8) | 45 (88.2) | 43 (64.2) | |
| 5. Oral–fecal transmission | <0.001 | ||||
| yes | 832 (43.6) | 806 (45.0) | 6 (11.8) | 20 (29.9) | |
| no | 1078 (56.4) | 986 (55.0) | 45 (88.2) | 47 (70.1) | |
| Common symptoms include | |||||
| 1. Fever and cough | <0.001 | ||||
| yes | 1792 (93.8) | 1706 (95.2) | 30 (58.8) | 56 (83.6) | |
| no | 118 (6.2) | 86 (4.8) | 21 (41.2) | 11 (16.4) | |
| 2. Shortness of breath, anorexia, fatigue, nausea, vomiting, diarrhea | <0.001 | ||||
| yes | 1532 (80.2) | 1478 (82.5) | 12 (23.5) | 42 (62.7) | |
| no | 378 (19.8) | 314 (17.5) | 39 (76.5) | 25 (37.3) | |
| 3. Panic and chest tightness | <0.001 | ||||
| yes | 1325 (69.4) | 1284 (71.7) | 7 (13.7) | 34 (50.7) | |
| no | 585 (30.6) | 508 (28.3) | 44 (86.3) | 33 (49.3) | |
| 4. Body aches | <0.001 | ||||
| yes | 1247 (65.3) | 1213 (67.7) | 6 (11.8) | 28 (41.8) | |
| no | 663 (34.7) | 579 (32.3) | 45 (88.2) | 39 (58.2) | |
| 5. Conjunctival congestion | <0.001 | ||||
| yes | 675 (35.3) | 656 (36.6) | 5 (9.8) | 14 (20.9) | |
| no | 1235 (64.7) | 1136 (63.4) | 46 (90.2) | 53 (79.1) | |
| Items | All | Attitude of Being Vaccinated | p | ||
|---|---|---|---|---|---|
| Willingness | Refusal | Hesitation | |||
| 1. When I meet my friends and colleagues, I will always greet them with a handshake | 0.017 | ||||
| agree | 422 (22.1) | 410 (22.9) | 3 (5.9) | 9 (13.4) | |
| uncertain | 508 (26.6) | 473 (26.4) | 14 (27.5) | 21 (31.3) | |
| disagree | 980 (51.3) | 909 (50.7) | 34 (66.7) | 37 (55.2) | |
| 2. When I meet my friends and colleagues, I will always greet them with a hug | 0.280 | ||||
| agree | 181 (9.5) | 176 (9.8) | 2 (3.9) | 3 (4.5) | |
| uncertain | 414 (21.7) | 390 (21.8) | 12 (23.5) | 12 (17.9) | |
| disagree | 1315 (68.8) | 1226 (68.4) | 37 (72.5) | 52 (77.6) | |
| 3. I wash my hands regularly and for enough period of time | <0.001 | ||||
| agree | 1760 (92.1) | 1702 (95) | 13 (25.5) | 45 (67.2) | |
| uncertain | 84 (4.4) | 63 (3.5) | 13 (25.5) | 8 (11.9) | |
| disagree | 66 (3.5) | 27 (1.5) | 25 (49) | 14 (20.9) | |
| 4. I usually put a facemask to protect myself from the risk of infection | <0.001 | ||||
| agree | 1798 (94.1) | 1695 (94.6) | 40 (78.4) | 63 (94) | |
| uncertain | 88 (4.6) | 79 (4.4) | 5 (9.8) | 4 (6) | |
| disagree | 24 (1.3) | 18 (1.0) | 6 (11.8) | 0 (0) | |
| 5. If I find that I contacted a person infected with the virus, I will inform the health authorities | <0.001 | ||||
| agree | 1846 (96.6) | 1756 (98.0) | 33 (64.7) | 57 (85.1) | |
| uncertain | 48 (2.5) | 27 (1.5) | 13 (25.5) | 8 (11.9) | |
| disagree | 16 (0.8) | 9 (0.5) | 5 (9.8) | 2 (3) | |
| 6. If I have any of the symptoms associated with the disease, I will inform the health authorities | <0.001 | ||||
| agree | 1775 (92.9) | 1691 (94.4) | 31 (60.8) | 53 (79.1) | |
| uncertain | 108 (5.7) | 81 (4.5) | 15 (29.4) | 12 (17.9) | |
| disagree | 27 (1.4) | 20 (1.1) | 5 (9.8) | 2 (3) | |
| 7. If I find that I contacted a person infected with the virus, I agree to be isolated at home for a certain period of time until it is proven that I am free from the disease | <0.001 | ||||
| agree | 1786 (93.5) | 1686 (94.1) | 41 (80.4) | 59 (88.1) | |
| uncertain | 51 (2.7) | 41 (2.3) | 4 (7.8) | 6 (9) | |
| disagree | 73 (3.8) | 65 (3.6) | 6 (11.8) | 2 (3) | |
| 8. If I found that I contacted a person infected with the virus, I agree to be isolated at an isolation hospital for a certain period of time until it is proven that I am free from the disease | <0.001 | ||||
| agree | 1839 (96.3) | 1742 (97.2) | 41 (80.4) | 56 (83.6) | |
| uncertain | 55 (2.9) | 40 (2.2) | 5 (9.8) | 10 (14.9) | |
| disagree | 16 (0.8) | 10 (0.6) | 5 (9.8) | 1 (1.5) | |
| 9. If I am asked to be isolated for a certain period of time, I think my salary will continue during this period | 0.171 | ||||
| agree | 1139 (59.6) | 1071 (59.8) | 30 (58.8) | 38 (56.7) | |
| uncertain | 429 (22.5) | 409 (22.8) | 7 (13.7) | 13 (19.4) | |
| disagree | 342 (17.9) | 312 (17.4) | 14 (27.5) | 16 (23.9) | |
| 10. If I am asked to be isolated for a certain period of time, my salary should be continued during this period | 0.311 | ||||
| agree | 1389 (72.8) | 1299 (72.5) | 43 (84.3) | 47 (70.1) | |
| uncertain | 339 (17.7) | 319 (17.8) | 7 (13.7) | 13 (19.4) | |
| disagree | 182 (9.5) | 174 (9.7) | 1 (2) | 7 (10.4) | |
| 11. If there is an available lab test for detection of the virus, I am willing to do it | <0.001 | ||||
| agree | 1865 (97.6) | 1756 (98) | 48 (94.1) | 61 (91) | |
| uncertain | 40 (2.1) | 31 (1.7) | 3 (5.9) | 6 (9) | |
| disagree | 5 (0.3) | 5 (0.3) | 0 (0) | 0 (0) | |
| 12. If there is an available vaccine for the virus, I am willing to get it | <0.001 | ||||
| agree | 1773 (92.8) | 1740 (97.1) | 10 (19.6) | 23 (34.3) | |
| uncertain | 76 (4) | 43 (2.4) | 4 (7.8) | 29 (43.3) | |
| disagree | 61 (3.2) | 9 (0.5) | 37 (72.5) | 15 (22.4) | |
| 13. I usually follow the updates about the spread of the virus in my country | <0.001 | ||||
| agree | 1753 (91.8) | 1693 (94.5) | 16 (31.4) | 44 (65.7) | |
| uncertain | 116 (6.1) | 81 (4.5) | 20 (39.2) | 15 (22.4) | |
| disagree | 41 (2.1) | 18 (1) | 15 (29.4) | 8 (11.9) | |
| 14. I usually follow the updates about the spread of the virus worldwide | <0.001 | ||||
| agree | 1715 (89.8) | 1658 (92.5) | 14 (27.5) | 43 (64.2) | |
| uncertain | 149 (7.8) | 110 (6.1) | 22 (43.1) | 17 (25.4) | |
| disagree | 46 (2.4) | 24 (1.3) | 15 (29.4) | 7 (10.4) | |
| 15. If a lecture about the virus is organized near me, I will attend it | <0.001 | ||||
| agree | 1317 (69) | 1280 (71.4) | 10 (19.6) | 27 (40.3) | |
| uncertain | 526 (27.5) | 459 (25.6) | 32 (62.7) | 35 (52.2) | |
| disagree | 67 (3.5) | 53 (3) | 9 (17.6) | 5 (7.5) | |
| 16. If flyers or brochures that include information about the disease are distributed, I will read them and follow the instructions mentioned in them | <0.001 | ||||
| agree | 1767 (92.5) | 1693 (94.5) | 23 (45.1) | 51 (76.1) | |
| uncertain | 117 (6.1) | 82 (4.6) | 21 (41.2) | 14 (20.9) | |
| disagree | 26 (1.4) | 17 (0.9) | 7 (13.7) | 2 (3) | |
| Items | All | Attitude of Being Vaccinated | p | ||
|---|---|---|---|---|---|
| Willingness | Refusal | Hesitation | |||
| Total score of DrVac-COVID19S | 68 (62.76) | 69 (63.77) | 57 (49.63) | 55 (49.62) | <0.001 |
| value | 18 (17.21) | 19 (18.21) | 16 (12.18) | 15 (13.18) | <0.001 |
| impacts | 16 (14.19) | 17 (14.19) | 15 (12.18) | 14 (12.17) | <0.001 |
| knowledge | 16 (14.19) | 16 (14.19) | 9 (7.11) | 11 (9.13) | <0.001 |
| autonomy traits | 18 (15.20) | 18 (15.20) | 18 (16.18) | 14 (12.17) | <0.001 |
| 1. Vaccination is a very effective way to protect me against COVID-19. | <0.001 | ||||
| agree | 1494 (78.2) | 1430 (79.8) | 30 (58.8) | 34 (50.7) | |
| uncertain | 305 (16) | 261 (14.6) | 18 (35.3) | 26 (38.8) | |
| disagree | 111 (5.8) | 101 (5.6) | 3 (5.9) | 7 (10.4) | |
| 2. I know very well how vaccination protects me from COVID-19. | <0.001 | ||||
| agree | 1401 (73.4) | 1378 (76.9) | 6 (11.8) | 17 (25.4) | |
| uncertain | 337 (17.6) | 310 (17.3) | 4 (7.8) | 23 (34.3) | |
| disagree | 172 (9) | 104 (5.8) | 41 (80.4) | 27 (40.3) | |
| 3. It is important that I get the COVID-19 jab. | <0.001 | ||||
| agree | 1811 (94.8) | 1726 (96.3) | 36 (70.6) | 49 (73.1) | |
| uncertain | 75 (3.9) | 49 (2.7) | 13 (25.5) | 13 (19.4) | |
| disagree | 24 (1.3) | 17 (0.9) | 2 (3.9) | 5 (7.5) | |
| 4. Vaccination greatly reduces my risk of catching COVID-19. | <0.001 | ||||
| agree | 1757 (92) | 1675 (93.5) | 35 (68.6) | 47 (70.1) | |
| uncertain | 128 (6.7) | 100 (5.6) | 14 (27.5) | 14 (20.9) | |
| disagree | 25 (1.3) | 17 (0.9) | 2 (3.9) | 6 (9) | |
| 5. I understand how the flu jab helps my body fight the COVID-19 virus. | <0.001 | ||||
| agree | 1534 (80.3) | 1465 (81.8) | 30 (58.8) | 39 (58.2) | |
| uncertain | 315 (16.5) | 280 (15.6) | 15 (29.4) | 20 (29.9) | |
| disagree | 61 (3.2) | 47 (2.6) | 6 (11.8) | 8 (11.9) | |
| 6. The COVID-19 jab plays an important role in protecting my life and that of others. | <0.001 | ||||
| agree | 1727 (90.4) | 1649 (92) | 33 (64.7) | 45 (67.2) | |
| uncertain | 147 (7.7) | 112 (6.2) | 16 (31.4) | 19 (28.4) | |
| disagree | 36 (1.9) | 31 (1.7) | 2 (3.9) | 3 (4.5) | |
| 7. I feel under pressure to get the COVID-19 jab. | <0.001 | ||||
| agree | 267 (14) | 243 (13.6) | 6 (11.8) | 18 (26.9) | |
| uncertain | 206 (10.8) | 183 (10.2) | 6 (11.8) | 17 (25.4) | |
| disagree | 1437 (75.2) | 1366 (76.2) | 39 (76.5) | 32 (47.8) | |
| 8. The contribution of the COVID-19 jab to my health and well-being is very important. | <0.001 | ||||
| agree | 1669 (87.4) | 1603 (89.5) | 29 (56.9) | 37 (55.2) | |
| uncertain | 201 (10.5) | 156 (8.7) | 20 (39.2) | 25 (37.3) | |
| disagree | 40 (2.1) | 33 (1.8) | 2 (3.9) | 5 (7.5) | |
| 9. I can choose whether to get a COVID-19 jab or not. | <0.001 | ||||
| agree | 1742 (91.2) | 1647 (91.9) | 46 (90.2) | 49 (73.1) | |
| uncertain | 68 (3.6) | 52 (2.9) | 4 (7.8) | 12 (17.9) | |
| disagree | 100 (5.2) | 93 (5.2) | 1 (2) | 6 (9) | |
| 10. How the COVID-19 jab works to protect my health is a mystery to me. | <0.001 | ||||
| agree | 464 (24.3) | 383 (21.4) | 44 (86.3) | 37 (55.2) | |
| uncertain | 371 (19.4) | 344 (19.2) | 6 (11.8) | 21 (31.3) | |
| disagree | 1075 (56.3) | 1065 (59.4) | 1 (2) | 9 (13.4) | |
| 11. I get the COVID-19 jab only because I am required to do so. | <0.001 | ||||
| agree | 262 (13.7) | 242 (13.5) | 2 (3.9) | 18 (26.9) | |
| uncertain | 139 (7.3) | 118 (6.6) | 8 (15.7) | 13 (19.4) | |
| disagree | 1509 (79) | 1432 (79.9) | 41 (80.4) | 36 (53.7) | |
| 12. Getting the COVID-19 jab has a positive influence on my health. | <0.001 | ||||
| agree | 1113 (58.3) | 1055 (58.9) | 24 (47.1) | 34 (50.7) | |
| uncertain | 317 (16.6) | 266 (14.8) | 24 (47.1) | 27 (40.3) | |
| disagree | 480 (25.1) | 471 (26.3) | 3 (5.9) | 6 (9) | |
| B | S.E. | p | OR | 95% CI | ||
|---|---|---|---|---|---|---|
| Place of residence | −0.576 | 0.398 | 0.147 | 0.562 | 0.258 | 1.226 |
| Marital status | −1.023 | 0.499 | 0.040 * | 0.360 | 0.135 | 0.956 |
| Educational level | 0.096 | 0.130 | 0.461 | 1.100 | 0.853 | 1.418 |
| Yearly per capita income | 0.075 | 0.209 | 0.718 | 1.078 | 0.716 | 1.623 |
| Health status | −1.026 | 0.422 | 0.015 * | 0.359 | 0.157 | 0.820 |
| Item 1-knowledge of COVID-19 spreads | 0.142 | 0.596 | 0.812 | 1.152 | 0.358 | 3.705 |
| Item 2-knowledge of COVID-19 spreads | 0.412 | 0.399 | 0.302 | 1.510 | 0.690 | 3.302 |
| Item 3-knowledge of COVID-19 spreads | −0.374 | 0.413 | 0.365 | 0.688 | 0.306 | 1.545 |
| Item 4-knowledge of COVID-19 spreads | 0.504 | 0.411 | 0.220 | 1.655 | 0.740 | 3.703 |
| Item 5-knowledge of COVID-19 spreads | −0.210 | 0.427 | 0.623 | 0.811 | 0.351 | 1.871 |
| Item 1-knowledge of COVID-19 symptoms | −1.800 | 0.532 | 0.001 * | 0.165 | 0.058 | 0.469 |
| Item 2-knowledge of COVID-19 symptoms | 0.043 | 0.462 | 0.925 | 1.044 | 0.422 | 2.581 |
| Item 3-knowledge of COVID-19 symptoms | 0.490 | 0.455 | 0.282 | 1.632 | 0.668 | 3.983 |
| Item 4-knowledge of COVID-19 symptoms | −0.786 | 0.445 | 0.077 | 0.455 | 0.190 | 1.090 |
| Item 5-knowledge of COVID-19 symptoms | −0.112 | 0.430 | 0.794 | 0.894 | 0.385 | 2.076 |
| Item 1-knowledge of COVID-19 vaccination | 0.339 | 0.265 | 0.201 | 1.404 | 0.835 | 2.360 |
| Item 2-knowledge of COVID-19 vaccination | 0.329 | 0.281 | 0.242 | 1.390 | 0.801 | 2.413 |
| Item 3-knowledge of COVID-19 vaccination | 0.664 | 0.459 | 0.148 | 1.943 | 0.791 | 4.776 |
| Item 4-knowledge of COVID-19 vaccination | 0.304 | 0.432 | 0.482 | 1.355 | 0.581 | 3.160 |
| Item 5-knowledge of COVID-19 vaccination | 0.304 | 0.275 | 0.268 | 1.355 | 0.791 | 2.321 |
| Item 6-knowledge of COVID-19 vaccination | −1.044 | 0.481 | 0.030 * | 0.352 | 0.137 | 0.903 |
| Item 7-knowledge of COVID-19 vaccination | −0.348 | 0.201 | 0.083 | 0.706 | 0.477 | 1.046 |
| Item 8-knowledge of COVID-19 vaccination | 0.602 | 0.373 | 0.107 | 1.826 | 0.879 | 3.795 |
| Item 9-knowledge of COVID-19 vaccination | −0.381 | 0.285 | 0.181 | 0.683 | 0.391 | 1.194 |
| Item 10-knowledge of COVID-19 vaccination | −0.240 | 0.236 | 0.310 | 0.787 | 0.495 | 1.250 |
| Item 11-knowledge of COVID-19 vaccination | −0.410 | 0.204 | 0.045 * | 0.664 | 0.445 | 0.990 |
| Item 12-knowledge of COVID-19 vaccination | −0.208 | 0.209 | 0.320 | 0.812 | 0.539 | 1.224 |
| Item 1-preventive measure of COVID-19 | 0.068 | 0.193 | 0.724 | 1.070 | 0.734 | 1.562 |
| Item 3-preventive measure of COVID-19 | 0.695 | 0.394 | 0.078 | 2.003 | 0.925 | 4.339 |
| Item 4-preventive measure of COVID-19 | −1.543 | 0.543 | 0.004 * | 0.214 | 0.074 | 0.619 |
| Item 5-preventive measure of COVID-19 | 1.134 | 0.767 | 0.139 | 3.109 | 0.692 | 13.973 |
| Item 6-preventive measure of COVID-19 | −0.875 | 0.702 | 0.213 | 0.417 | 0.105 | 1.651 |
| Item 7-preventive measure of COVID-19 | −0.227 | 0.571 | 0.691 | 0.797 | 0.260 | 2.438 |
| Item 8-preventive measure of COVID-19 | −0.074 | 0.798 | 0.926 | 0.928 | 0.194 | 4.434 |
| Item 11-preventive measure of COVID-19 | −0.873 | 0.617 | 0.157 | 0.418 | 0.125 | 1.400 |
| Item 12-preventive measure of COVID-19 | 3.056 | 0.345 | <0.001 * | 21.237 | 10.794 | 41.785 |
| Item 13-preventive measure of COVID-19 | 0.527 | 0.811 | 0.515 | 1.694 | 0.346 | 8.297 |
| Item 14-preventive measure of COVID-19 | −0.962 | 0.816 | 0.238 | 0.382 | 0.077 | 1.892 |
| Item 15-preventive measure of COVID-19 | −0.481 | 0.339 | 0.156 | 0.618 | 0.318 | 1.201 |
| Item 16-preventive measure of COVID-19 | −0.102 | 0.493 | 0.836 | 0.903 | 0.344 | 2.371 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dong, C.; Liang, Q.; Ji, T.; Gu, J.; Feng, J.; Shuai, M.; Zhang, X.; Zhao, R.; Gu, Z. Determinants of Vaccine Acceptance against COVID-19 in China: Perspectives on Knowledge and DrVac-COVID19S Scale. Int. J. Environ. Res. Public Health 2021, 18, 11192. https://doi.org/10.3390/ijerph182111192
Dong C, Liang Q, Ji T, Gu J, Feng J, Shuai M, Zhang X, Zhao R, Gu Z. Determinants of Vaccine Acceptance against COVID-19 in China: Perspectives on Knowledge and DrVac-COVID19S Scale. International Journal of Environmental Research and Public Health. 2021; 18(21):11192. https://doi.org/10.3390/ijerph182111192
Chicago/Turabian StyleDong, Chen, Qian Liang, Tanao Ji, Jun Gu, Jian Feng, Min Shuai, Xiaoming Zhang, Rui Zhao, and Zhifeng Gu. 2021. "Determinants of Vaccine Acceptance against COVID-19 in China: Perspectives on Knowledge and DrVac-COVID19S Scale" International Journal of Environmental Research and Public Health 18, no. 21: 11192. https://doi.org/10.3390/ijerph182111192