
Malaysia’s Health Systems Response to COVID-19

 , , ,
, , , 
Abstract
:1. Introduction
2. Materials and Methods
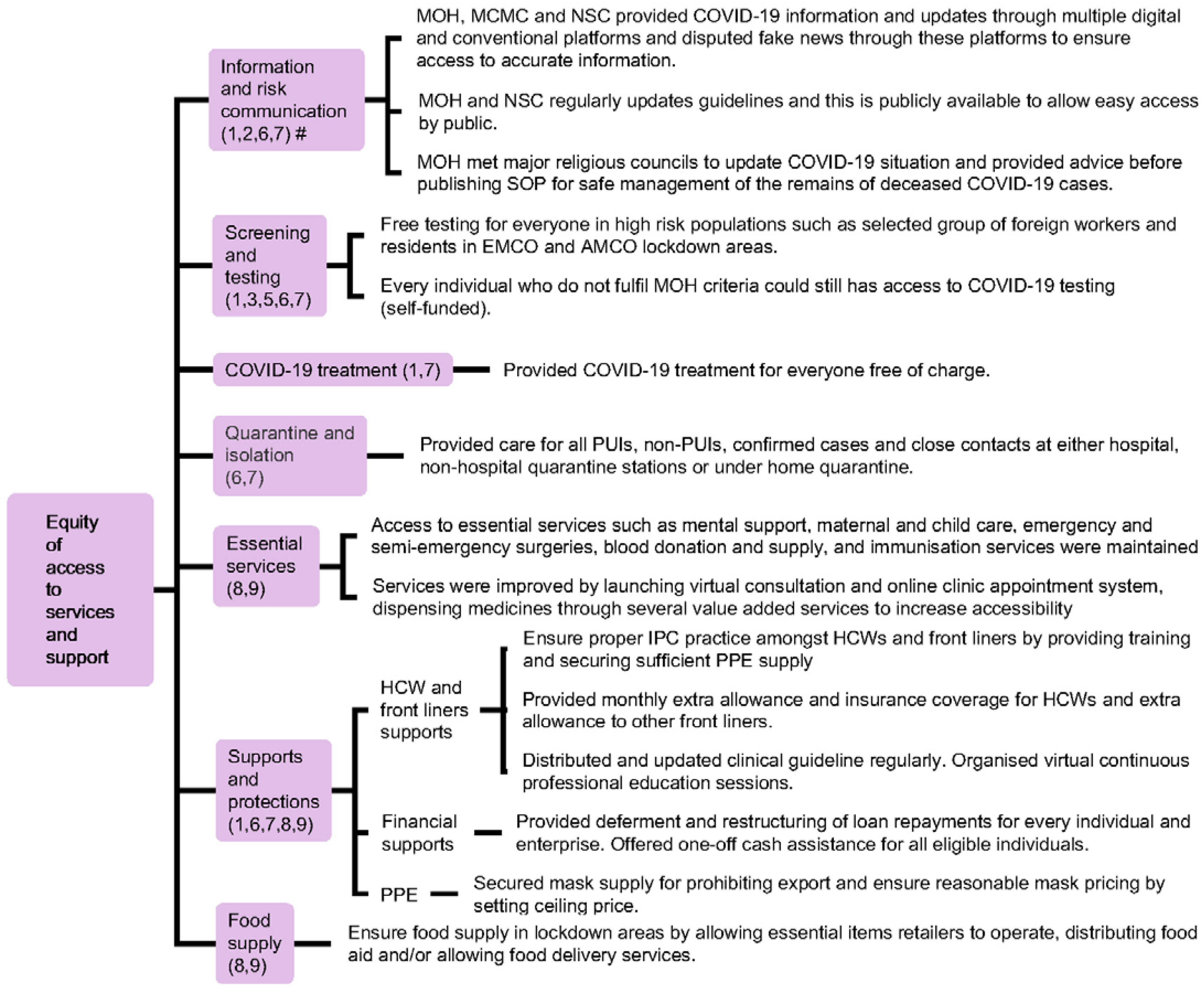
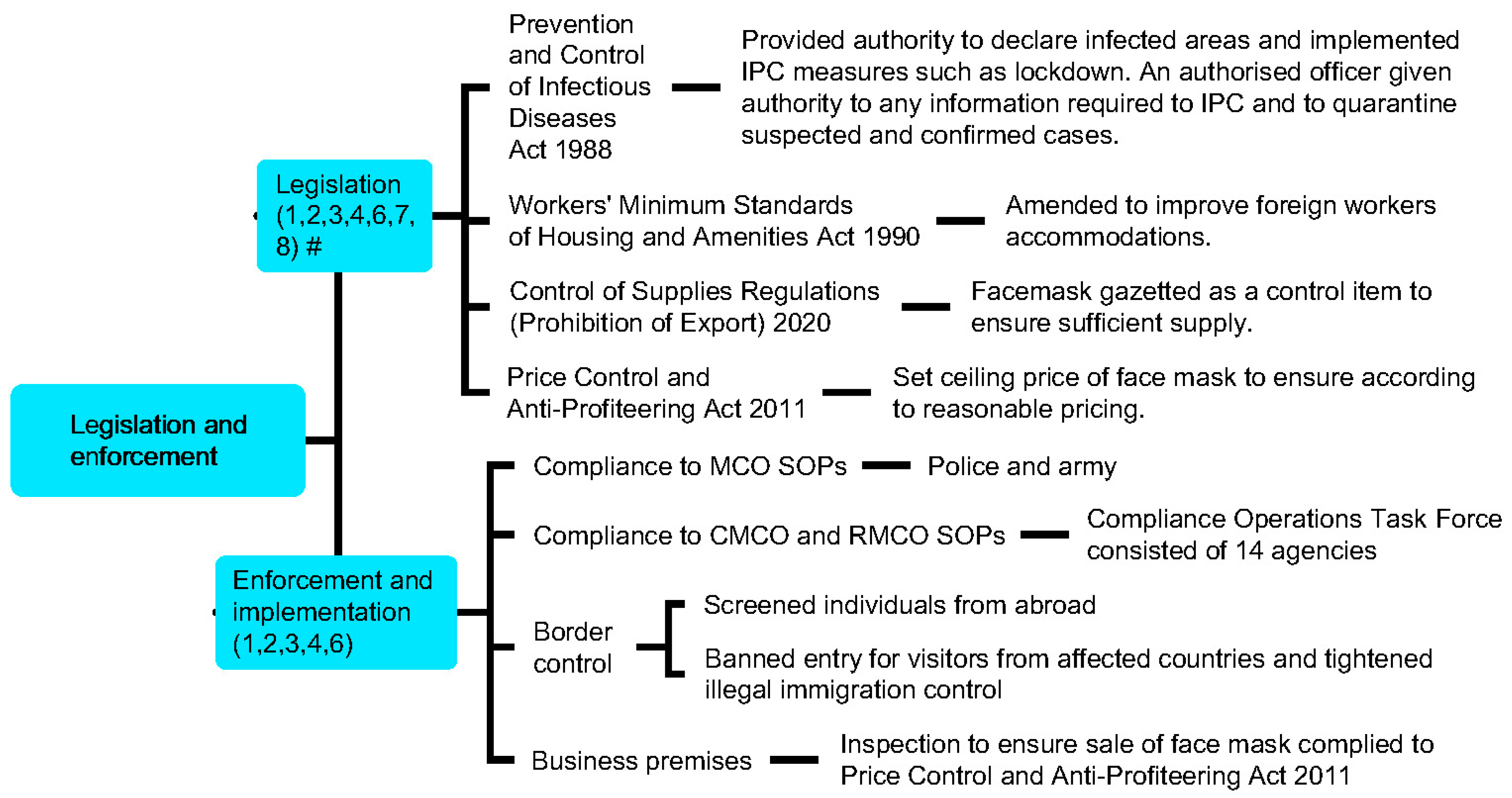
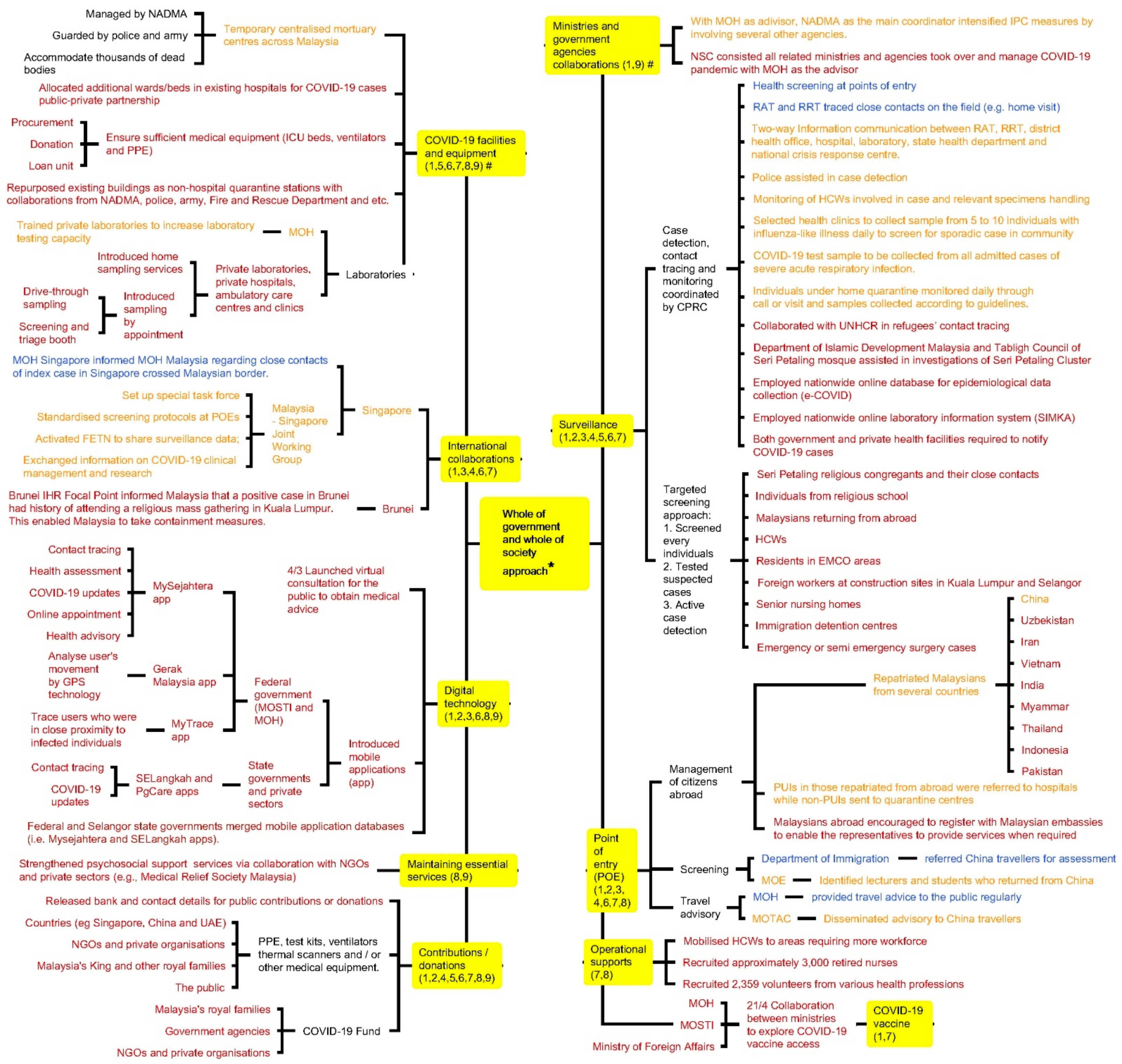
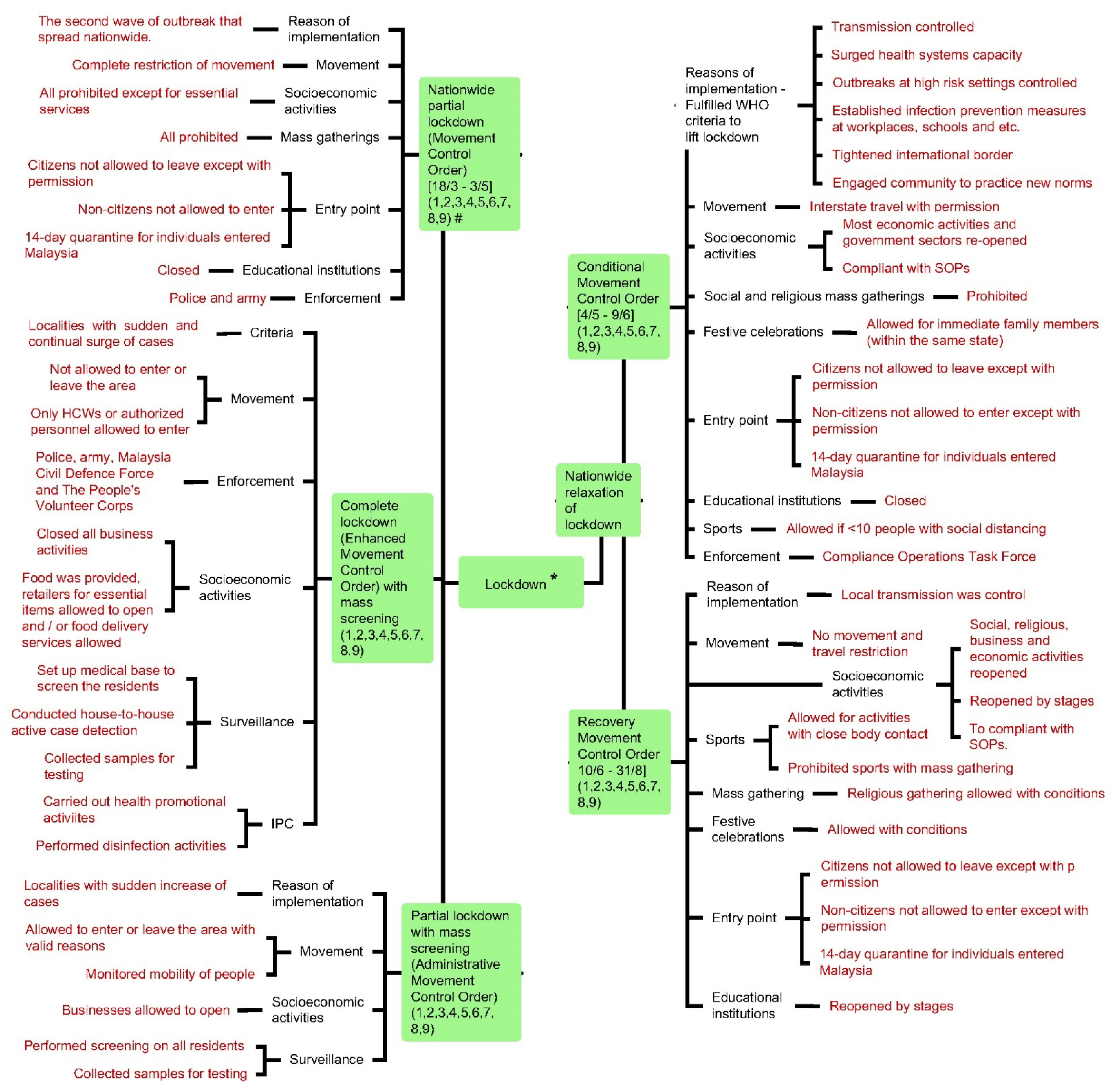
3. Results
4. Discussion
4.1. Principle Findings
4.2. Implications to the Stakeholders, Lessons Learnt, and Future Direction
4.2.1. Lockdown—The Rationale and Impact?
4.2.2. Mass Gathering—The Importance of Regulating a Mass Gathering in the Future
4.2.3. COVID-19 Surveillance—Expand the Eligibility for COVID-19 Testing and Conduct Mass Testing?
4.2.4. Adopting Digital Technology in Fighting the COVID-19 Pandemic
4.2.5. Information and Risk Communication—Addressing Infodemic Needs
4.2.6. Outbreak Containment in Custodial Settings
4.2.7. Importance of Developing Guidelines Suited to Local Culture and Context
4.3. Strengths and Weaknesses
4.4. Future Studies
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Problem | Concept | Context | ||
|---|---|---|---|---|
| COVID-19 or nCoV or novel coronavirus OR SARS-CoV-2 | and | response or measure or strategy or action | and | Malaysia |
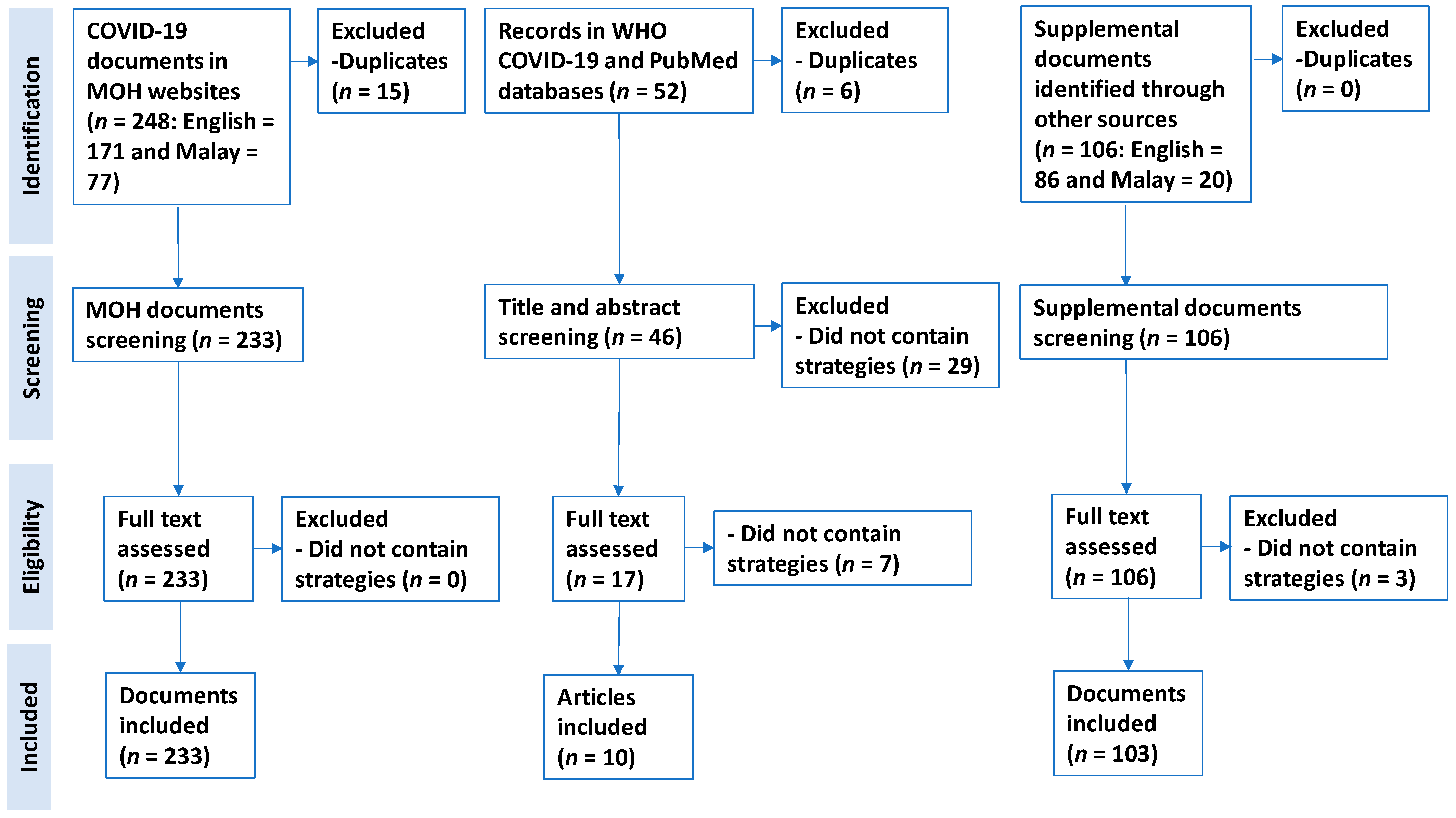
- MOH-affiliated official websites: documents in English or Malay from 31 December 2019 to 30 June 2020.
- PubMed and WHO global research on coronavirus disease databases: Journal articles (include preprints) in English from 31 December 2019 to 30 June 2020.
- Journal articles (including preprints) and documents that did not content health systems measure or strategy were excluded.
| Criteria | Document Review Step | MOH Related Websites | PubMed and WHO Database |
|---|---|---|---|
| Inclusion criteria | Title and abstract screening | The document was related to COVID-19 in Malaysia. | The journal article/preprint was related to COVID-19 in Malaysia. |
| Full text screening and data extraction | The document was related to COVID-19 in Malaysia. | The journal article/preprint was related to COVID-19 in Malaysia. | |
| Health systems strategy to manage COVID-19 was mentioned in the document. | Health systems strategy or measure to manage COVID-19 was mentioned in the journal article/preprint. | ||
| The health systems strategy was implemented. | The health systems strategy was implemented. |
Appendix B
| Type of Document | Journal Article | Preprint | Press Statement | Website Article | Infographic | Act | Guidelines | Circular | News | Total | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Type of Source | Eng * | Eng | Eng | Mal * | Eng | Mal | Eng | Mal | Eng | Mal | Eng | Mal | Eng | Mal | Eng | Mal | ||
| Databases | PubMed database https://pubmed.ncbi.nlm.nih.gov/ (accessed on 26 August 2020) | 43 | 0 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 43 |
| WHO global research on coronavirus disease database https://search.bvsalud.org/global-literature-on-novel-coronavirus-2019-ncov/ (accessed on 24 March 2020, 18 April 2020 and 5 July 2020) | 6 | 3 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 9 | |
| MOH- affiliated websites | http://www.moh.gov.my (accessed on 27 March 2020, 18 April 2020, 1 July 2020 to 5 July 2020) | - | - | 1 | 21 | 0 | 0 | 0 | 1 | 0 | 0 | 42 | 11 | 0 | 8 | - | - | 84 |
| http://covid-19.moh.gov.my (accessed on 1 July 2020 to 5 July 2020) | - | - | 9 | 8 | 0 | 1 | 0 | 1 | 2 | 0 | 2 | 1 | 0 | 0 | - | - | 24 | |
| https://kpkesihatan.com (accessed on 27 March 2020, 18 April 2020, 1 July 2020 to 5 July 2020) | - | - | 115 | 24 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 139 | |
| medicalprac.moh.gov.my (accessed on 27 March 2020, 18 April 2020, 1 July 2020 to 5 July 2020) | - | - | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | - | - | 1 | |
| Supplemental search | 2 | 0 | 1 | 9 | 8 | 6 | 0 | 1 | 16 | 0 | 1 | 2 | 0 | 1 | 58 | 1 | 106 | |
Appendix C

Appendix D

Appendix E

Appendix F

Appendix G

Appendix H
| AMCO | Administrative Movement Control Order | MOH | Ministry of Health |
|---|---|---|---|
| App | Mobile application | MOSTI | Ministry of Science, Technology and Innovation |
| COVID-19 | Coronavirus disease 2019 | NADMA | National Disaster Management Agency |
| CMCO | Conditional Movement Control Order | NGO | Non-governmental organisation |
| CPRP | Crisis Preparedness and Response Centre | NSC | National Security Council |
| EMCO | Enhanced Movement Control Order | POE | Point of entry |
| FETN | Field Epidemiology Training Network | PPE | Personal protective equipment |
| GPS | Global Positioning System | PUI | Person Under Investigation |
| HCW | Health care worker | QR | Quick response |
| ICU | Intensive care unit | RAT | Rapid Assessment Team |
| IHR | International Health Regulations | RELA | People’s Volunteer Corps |
| IMR | Institute for Medical Research | RMCO | Recovery Movement Control Order |
| IPC | Infection prevention and control | RRT | Rapid response team |
| IT | Information technology | rRT-PCR | Real time reverse transcription polymerase chain reaction |
| MCCBCHST | Malaysian Consultative Council of Buddhism, Christianity, Hinduism, Sikhism and Taoism | SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| MCMC | Malaysian Communications and Multimedia Commission | SOP | Standard operating procedure |
| MCO | Movement Control Order | UAE | United Arab Emirates |
| MHPSS | Mental Health and Psychosocial Support Services | WHO | World Health Organisation |
| MKI | National Special Council for Islamic Religious Affairs of Malaysia | UNHCR | United Nations High Commissioner for Refugees |
| MOE | Ministry of Education | WHO SPRP | WHO COVID-19 Strategic Preparedness and Response Plan |
References
- World Health Organisation. WHO Timeline-COVID-19. World Health Organization; 2020 [Updated 25 April 2020]. Available online: https://www.who.int/news-room/detail/27-04-2020-who-timeline---Covid-19 (accessed on 25 April 2020).
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 24 January 2020—Tindakan KKM Bagi Pengesanan Kontak (Contact Tracing) Kepada Kes Pertama Positif Novel Coronavirus di Negara Singapura Pada 24 January 2020 [Ministry of Health Malaysia Press Statement on 24 January 2020—MOH Actions for Contact Tracing on the First Positive Case of Coronavirus Novel in Singapore on 24 January 2020]. Malaysia: Ministry of Health Malaysia; 2020 [Updated 24 January 2020]. Available online: https://kpkesihatan.com/2020/01/24/kenyataan-akhbar-kpk-24-januari-2020-tindakan-kkm-bagi-pengesanan-kontak-contact-tracing-kepada-kes-pertama-positif-novel-coronavirus-di-negara-singapura-pada-24-januari-2020/ (accessed on 25 April 2020).
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 25 January 2020—Pengesanan Kes Baharu Yang Disahkan Dijangkiti 2019 Novel Coronavirus (2019-nCoV) di Malaysia [Ministry of Health Malaysia Press Statement on 25 January 2020—Detection of New Confirmed Cases of Novel Coronavirus 2019 (2019-nCoV) in Malaysia]. Malaysia: Ministry of Health Malaysia; 2020 [Updated 25 January 2020]. Available online: https://kpkesihatan.com/2020/01/25/kenyataan-akhbar-kpk-25-januari-2020-pengesanan-kes-baharu-yang-disahkan-dijangkiti-2019-novel-coronavirus-2019-ncov-di-malaysia/ (accessed on 25 April 2020).
- Liu, Y.; Gayle, A.A.; Wilder-Smith, A.; Rocklöv, J. The reproductive number of COVID-19 is higher compared to SARS coronavirus. J. Travel Med. 2020, 27, taaa021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organisation. COVID-19 Strategic Preparedness and Response Plan Operational Planning Guidelines to Support Country Preparedness and Response. 2020 [Updated 03 February 2020]. Available online: https://www.who.int/publications-detail/strategic-preparedness-and-response-plan-for-the-new-coronavirus (accessed on 20 July 2020).
- World Health Organisation. COVID-19 Strategic Preparedness and Response Plan Operational Planning Guidelines to Support Country Preparedness and Response (Draft Updated on 22 May 2020). 2020. [updated 02 May 2020]. Available online: https://www.who.int/docs/default-source/coronaviruse/covid-19-sprp-operational-planning-guidelines-to-support-country-preparedness-and-response-(22may20).pdf (accessed on 1 July 2020).
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 6 Januari 2020—Makluman Kejadian Kejadian Kluster Radang Paru-Paru (Pneumonia) di Wuhan, Republik Rakyat China [Ministry of Health Malaysia Press Statement on 6 January 2020—Updates On The Occurence of Pneumonia Clusters in Wuhan, People Republic of China Situation]. Malaysia: Ministry of Health; 2020 [updated 6 January 2020]. Available online: https://kpkesihatan.com/2020/01/06/kenyataan-akhbar-kpk-6-januari-2020-makluman-kejadian-kejadian-kluster-radang-paru-paru-pneumonia-di-wuhan-republik-rakyat-china/ (accessed on 24 March 2020).
- Minister of Health Malaysia. Kenyataan Akhbar KPK 16 Januari 2020—Kesiapsiagaan dan Respons KKM dalam Menghadapi Potensi Penularan Novel Coronavirus, Wuhan, China [Press Statement MOH 16 January 2020-Preparedness and Responds MOH in Facing the Potential Outbreak of Novel Coronavirus, Wuhan, China]. Malaysia: Ministry of Health; 2020. Available online: https://kpkesihatan.com/2020/01/16/kenyataan-akhbar-kpk-16-januari-2020-kesiapsiagaan-dan-respons-kkm-dalam-menghadapi-potensi-penularan-novel-coronavirus-wuhan-china/ (accessed on 18 April 2020).
- World Health Organisation. Updated Country Preparedness and Response Status for COVID-19 as of 16 March 2020. World Health Organization; 2020 [Updated 16 March 2020]. Available online: https://www.who.int/who-documents-detail/updated-country-preparedness-and-response-status-for-covid-19-as-of-16-march-2020 (accessed on 20 May 2020).
- World Health Organisation. Updated Country Preparedness and Response Status for COVID-19 as of 11 May 2020. World Health Organization; 2020 [Updated 11/05/2020]. Available online: https://www.who.int/who-documents-detail/updated-country-preparedness-and-response-status-for-covid-19-as-of-11-may-2020 (accessed on 5 July 2020).
- World Health Organisation. International Health Regulations (2005): State Party Self-Assessment Annual Reporting Tool. 2018. Available online: https://apps.who.int/iris/bitstream/handle/10665/272432/WHO-WHE-CPI-2018.16-eng.pdf?sequence=1 (accessed on 18 April 2020).
- Tang, J.W.; Tambyah, P.A.; Hui, D.S.C. Emergence of a novel coronavirus causing respiratory illness from Wuhan, China. J. Infect. 2020, 80, 350–371. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Langlois, E.V.; Straus, S.E. Alliance for Health Policy Systems Research, World Health Organisation. In Rapid Reviews to Strengthen Health Policy and Systems: A Practical Guide; World Health Organisation: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organisation. Global research on coronavirus disease (COVID-19). World Health Organization; 2020. Available online: https://search.bvsalud.org/global-literature-on-novel-coronavirus-2019-ncov/ (accessed on 27 March 2020).
- Moher, D.; Liberati, A.T.J.; Altman, D.P.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 7, e1000097. Available online: https://pubmed.ncbi.nlm.nih.gov/19621072/ (accessed on 2 August 2020).
- Tricco, A.C.; Antony, J.; Zarin, W.; Strifler, L.; Ghassemi, M.; Ivory, J.; Perrier, L.; Hutton, B.; Moher, D.; Straus, S.E.; et al. A scoping review of rapid review methods. BMC Med. 2015, 13, 224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Center for Disease Control and Prevention. Severe Acute Respiratory Syndrome (SARS) II. Lessons Learned. USA: Center for Disease Control and Prevention; 2005. Available online: https://www.cdc.gov/sars/guidance/d-quarantine/lessons.html (accessed on 6 October 2021).
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 11 Mac 2020—Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia [Ministry of Health Malaysia Press Statement on 11 March 2020-Updates On The Coronavirus Disease 2019 (COVID-19) Situation In Malaysia]. Malaysia: Ministry of Health Malaysia; 2020 [Updated 11 March 2020]. Available online: https://kpkesihatan.com/2020/03/11/kenyataan-akhbar-kpk-11-mac-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 18 April 2020).
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 13 March 2020—Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia [Ministry of Health Malaysia Press Statement on 13 March 2020-Updates on the Coronavirus Disease 2019 (COVID-19) Situation in Malaysia]. Malaysia: Ministry of Health; 2020 [Updated 13 March 2020]. Available online: https://kpkesihatan.com/2020/03/13/kenyataan-akhbar-kpk-13-mac-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 18 April 2020).
- Zahir Izuan, A.; Chen, X.; Mariam, M.; Mohd Shahril, A. COVID-19 Review: An Epidemiological Perspective and Malaysian Scenario in Handling the Pandemic (January–May 2020). J. Clin. Health Sci. 2020, 5, 26–41. Available online: https://jchs-medicine.uitm.edu.my/images/manuscript/vol5issue1/reviews/4COVID-19_Review_An_Epidemiological_Perspective_and_Malaysian_Scenario_in_Handling_the_Pandemic_January__May_2020.pdf (accessed on 7 October 2020).
- Shah, A.U.M.; Safri, S.N.A.; Thevadas, R.; Noordin, N.K.; Rahman, A.A.; Sekawi, Z.; Ideris, A.; Sultan, M.T.H. COVID-19 outbreak in Malaysia: Actions taken by the Malaysian government. Int. J. Infect. Dis. 2020, 97, 108–116. Available online: https://pubmed.ncbi.nlm.nih.gov/32497808 (accessed on 5 July 2020). [CrossRef] [PubMed]
- Safuan, S.; Edinur, H.A. Sri Petaling COVID-19 cluster in Malaysia: Challenges and the mitigation strategies. Acta Biomed. 2020, 91, e2020154. Available online: https://pubmed.ncbi.nlm.nih.gov/33525245 (accessed on 2 August 2021).
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 10 April 2020—Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia [Ministry of Health Malaysia Press Statement on 10 April 2020, updates on the Coronavirus Disease 2019 (COVID-19) Situation in Malaysia]. Malaysia: Ministry of Health; 2020 [Updated 10 April 2020]. Available online: https://kpkesihatan.com/2020/04/10/kenyataan-akhbar-kpk-10-april-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 18 April 2020).
- Abdul Karim, L.A. COVID-19: Peningkatan Kes Kerana Saringan di 3 PKPD [COVID-19: Increase in Cases due to Screening in 3 EMCO Areas]. Berita Harian Online, 2020. Available online: https://www.bharian.com.my/berita/nasional/2020/04/673353/covid-19-peningkatan-kes-kerana-saringan-di-3-pkpd (accessed on 9 August 2020).
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 19 June 2020—Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia [Ministry of Health Malaysia Press Statement on 19 June 2020, Updates on the Coronavirus Disease 2019 (COVID-19) Situation in Malaysia]. In: Abdullah DDNHb, Editor. Malaysia: Ministry of Health, 2020. Available online: https://kpkesihatan.com/2020/06/19/kenyataan-akhbar-kpk-19-jun-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 9 August 2020).
- Ministry of Health Malaysia. Jumlah Keseluruhan Taburan Kes COVID-19 Di Malaysia Sehingga 30 June 2020, 12 Tengah Hari [Total COVID-19 Case Distribution in Malaysia as of 12 Noon, 30 June 2020]. Malaysia 2020 [Updated 30 June 2020]. Available online: http://covid-19.moh.gov.my/user/pages/02.terkini/062020/situasi-terkini-30-jun-2020/taburankes.jpg (accessed on 5 July 2020).
- Osseni, I.A. Benin responds to covid-19: Sanitary cordon without generalized containment or lockdown? Trop. Med. Health 2020, 48, 46. [Google Scholar] [CrossRef]
- Pachetti, M.; Marini, B.; Giudici, F.; Benedetti, F.; Angeletti, S.; Ciccozzi, M.; Masciovecchio, C.; Ippodrino, R.; Zella, D. Impact of lockdown on Covid-19 case fatality rate and viral mutations spread in 7 countries in Europe and North America. J. Transl. Med. 2020, 18, 338. [Google Scholar] [CrossRef]
- Ihekweazu, C.; Agogo, E. Africa’s response to COVID-19. BMC Med. 2020, 18, 151. [Google Scholar] [CrossRef]
- Casares, M.; Khan, H. The Timing and Intensity of Social Distancing to Flatten the COVID-19 Curve: The Case of Spain. Int. J. Environ. Res. Public Health 2020, 17, 7283. [Google Scholar] [CrossRef] [PubMed]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. Available online: http://www.sciencedirect.com/science/article/pii/S0140673620304608 (accessed on 7 October 2020). [CrossRef] [Green Version]
- Shrestha, D.B.; Thapa, B.B.; Katuwal, N.; Shrestha, B.; Pant, C.; Basnet, B.; Mandal, P.; Gurung, A.; Agrawal, A.; Rouniyar, R.; et al. Psychological distress in Nepalese residents during COVID-19 pandemic: A community level survey. BMC Psychiatry 2020, 20, 491. [Google Scholar] [CrossRef] [PubMed]
- Galbraith, N.; Boyda, D.; McFeeters, D.; Hassan, T. The mental health of doctors during the COVID-19 pandemic. BJPsych Bull. 2020, 45, 93–97. Available online: https://pubmed.ncbi.nlm.nih.gov/32340645 (accessed on 20 August 2020). [CrossRef] [PubMed]
- Man, M.A.; Toma, C.; Motoc, N.S.; Necrelescu, O.L.; Bondor, C.I.; Chis, A.F.; Lesan, A.; Pop, C.M.; Todea, D.A.; Dantes, E.; et al. Disease Perception and Coping with Emotional Distress During COVID-19 Pandemic: A Survey Among Medical Staff. Int. J. Environ. Res. Public Health 2020, 17, 4899. Available online: https://pubmed.ncbi.nlm.nih.gov/32645962 (accessed on 20 September 2020). [CrossRef] [PubMed]
- Dahal, M.; Khanal, P.; Maharjan, S.; Panthi, B.; Nepal, S. Mitigating violence against women and young girls during COVID-19 induced lockdown in Nepal: A wake-up call. Glob. Health 2020, 16, 84. [Google Scholar] [CrossRef]
- Ashraf, B.N. Economic impact of government interventions during the COVID-19 pandemic: International evidence from financial markets. J. Behav. Exp. Financ. 2020, 27, 100371. Available online: http://www.sciencedirect.com/science/article/pii/S2214635020302422 (accessed on 7 October 2020). [CrossRef]
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 14 May 2020—Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia [Ministry of Health Malaysia Press Statement on 14 May 2020, Updates on the Coronavirus Disease 2019 (COVID-19) Situation in Malaysia]. Malaysia: Ministry of Health; 2020 [Updated 14 May 2020]. Available online: https://kpkesihatan.com/2020/05/14/kenyataan-akhbar-kpk-14-mei-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 7 October 2020).
- Prime Minister’s Office of M. Additional PRIHATIN SME Economic Stimulus Package (PRIHATIN SME+). Malaysia: Prime Minister’s Office; 2020 [Updated 06 April 2020]. Available online: https://www.pmo.gov.my/2020/04/langkah-tambahan-bagi-pakej-rangsangan-ekonomi-prihatin-rakyat-prihatin/ (accessed on 17 May 2020).
- Prime Minister’s Office of Malaysia. Prihatin Rakyat Economic Stimulus Package (PRIHATIN) Speech Text. Malaysia: Prime Minister’s Office; 2020 [Updated 27 March 2020]. Available online: https://www.pmo.gov.my/2020/03/speech-text-prihatin-esp/ (accessed on 28 May 2020).
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 12 March 2020—Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia [Ministry of Health Malaysia Press Statement on 12 March 2020, Updates on the Coronavirus Disease 2019 (COVID-19) Situation in Malaysia]. Malaysia: Ministry of Health; 2020 [Updated 12 March 2020]. Available online: https://kpkesihatan.com/2020/03/12/kenyataan-akhbar-kpk-12-mac-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 18 April 2020).
- Korean Society of Infectious Diseases; Korean Society of Pediatric Infectious Diseases; Korean Society of Epidemiology; Korean Society for Antimicrobial Therapy; Korean Society for Healthcare-associated Infection Control and Prevention; Korea Centers for Disease Control and Prevention. Report on the Epidemiological Features of Coronavirus Disease 2019 (COVID-19) Outbreak in the Republic of Korea from 19 January to 2 March 2020. J. Korean Med. Sci. 2020, 35, 10. Available online: https://jkms.org/DOIx.php?id=10.3346/jkms.2020.35.e112 (accessed on 16 March 2020).
- Ministry of Health Malaysia. Press Statement Ministry of Health Malaysia 28 April 2020—Updates on the Coronavirus Disease 2019 (COVID-19) Situation in Malaysia. Malaysia: Ministry of Health; 2020 [Updated 28 April 2020]. Available online: http://covid-19.moh.gov.my/terkini/042020/situasi-terkini-28-april-2020/98%20Kenyataan%20Akhbar%20KPK%20COVID-19%20(28%20April%202020)%20-%20EN.pdf (accessed on 9 May 2020).
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 26 April 2020—Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia [Ministry of Health Malaysia Press Statement on 26 April 2020, updates on the Coronavirus Disease 2019 (COVID-19) Situation in Malaysia]. Malaysia: Ministry of Health; 2020 [Updated 26 April 2020]. Available online: https://kpkesihatan.com/2020/04/26/kenyataan-akhbar-kpk-26-april-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 5 July 2020).
- Ministry of Health Malaysia. Guidelines COVID-19 Management-Annex 1: Case Definition of COVID-19. Malaysia: Ministry of Health Malaysia; 2020 [Updated 26 February 2020]. Available online: http://www.moh.gov.my/moh/resources/Penerbitan/Garis%20Panduan/Pengurusan%20KEsihatan%20&%20kawalan%20pykit/2019-nCOV/Bil%204%20%202020/Annex%201%20case%20definition%20COVID%2026022020.pdf (accessed on 24 March 2020).
- World Health Organisation. Laboratory Testing Strategy Recommendations for COVID-19: Interim Guidance. World Health Organization; 2020 [Updated 21 March 2020]. Available online: https://www.who.int/publications-detail/laboratory-testing-strategy-recommendations-for-covid-19-interim-guidance (accessed on 1 June 2020).
- World Health Organisation. Public Health Surveillance for COVID-19. 2020. Available online: https://apps.who.int/iris/bitstream/handle/10665/333752/WHO-2019-nCoV-SurveillanceGuidance-2020.7-eng.pdf (accessed on 20 September 2020).
- European Centre for Disease Prevention and Control. Population-Wide Testing of SARS-CoV-2: Country Experiences and Potential Approaches in the EU/EEA and the United Kingdom. 2020 [Updated 19 August 2020]. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-population-wide-testing-country-experiences.pdf (accessed on 20 October 2020).
- Department of Health and Human Services. Taking the Test. World Health Organization; 2020 [Updated 1 September 2020]. Available online: https://www.dhhs.vic.gov.au/taking-test-covid-19#why-should-i-get-tested (accessed on 28 September 2020).
- Raffle, A.E.; Pollock, A.M.; Harding-Edgar, L. Covid-19 mass testing programmes. BMJ 2020, 370, m3262. Available online: http://www.bmj.com/content/370/bmj.m3262.abstract (accessed on 28 September 2020). [CrossRef]
- Speechley, M.; Kunnilathu, A.; Aluckal, E.; Balakrishna, M.S.; Mathew, B.; George, E.K. Screening in Public Health and Clinical Care: Similarities and Differences in Definitions, Types, and Aims—A Systematic Review. J. Clin. Diagn. Res. 2017, 11, LE01–LE04. Available online: https://pubmed.ncbi.nlm.nih.gov/28511418 (accessed on 28 September 2020). [CrossRef] [PubMed]
- Lavezzo, E.; Franchin, E.; Ciavarella, C.; Cuomo-Dannenburg, G.; Barzon, L.; Del Vecchio, C.; Rossi, L.; Manganelli, R.; Loregian, A.; Navarin, N.; et al. Suppression of a SARS-CoV-2 outbreak in the Italian municipality of Vo’. Nature 2020, 584, 425–429. [Google Scholar] [CrossRef]
- The Government of United Kingdom. Coronavirus (COVID-19): Getting Tested. The Government of United Kingdom; 2020 [Updated 30 September 2020]. Available online: https://www.gov.uk/guidance/coronavirus-covid-19-getting-tested#who-can-be-tested (accessed on 8 November 2020).
- The Government of the Hong Kong Special Administrative Region. COVID-19 Testing Service for Designated High-Risk Groups. Hong Kong: The Government of the Hong Kong Special Administrative Region; 2020 [Updated 7 October 2020]. Available online: https://www.coronavirus.gov.hk/eng/testing-service-highrisk.html (accessed on 7 October 2020).
- The Government of the Hong Kong Special Administrative Region. Summary of Results of the Universal Community Testing Programme. Hong Kong: The Government of the Hong Kong Special Administrative Region; 2020 [Updated 15 September 2020]. Available online: https://www.info.gov.hk/gia/general/202009/15/P2020091500931.htm (accessed on 8 November 2020).
- The Government of United Kingdom. Testing in United Kingdom—Tests processed by Pillar. The Government of United Kingdom; 2020 [Updated 8 November 2020]. Available online: https://coronavirus.data.gov.uk/details/testing (accessed on 8 November 2020).
- The Government of United Kingdom. Coronavirus (COVID-19) Testing in the UK. The Government of United Kingdom; 2020 [Updated 5 November 2020]. Available online: https://www.gov.uk/government/publications/nhs-test-and-trace-statistics-england-methodology/nhs-test-and-trace-statistics-england-methodology#section-3 (accessed on 8 November 2020).
- The Government of United Kingdom. National COVID-19 Surveillance Data Report: 2 October 2020 (Week 40). The Government of United Kingdom; 2017 [Updated 2 October 2020]. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/923669/Weekly_COVID19_report_data_w40.xlsx (accessed on 8 October 2020).
- Li, J.; Wu, C.; Zhang, X.; Chen, L.; Wang, X.; Guan, X.; Li, J.; Lin, Z.; Xiong, N. Postpandemic Testing of Severe Acute Respiratory Syndrome Coronavirus 2 in the Huanan Seafood Market Area in Wuhan, China. Clin. Infect. Dis. 2020, 72, 2203–2205. [Google Scholar] [CrossRef]
- The Government of the Hong Kong Special Administrative Region. Statistics Related to Epidemiological Investigation of the Universal Community Testing Programme. Hong Kong: The Government of the Hong Kong Special Administrative Region; 2020 [Updated 15 September 2020]. Available online: https://gia.info.gov.hk/general/202009/15/P2020091500931_349441_1_1600184634005.pdf (accessed on 8 November 2020).
- European Centre for Disease Prevention and Control. Transmission of COVID-19. 2020. [Updated 7 September 2020]. Available online: https://www.ecdc.europa.eu/en/covid-19/latest-evidence/transmission (accessed on 20 October 2020).
- Lim, I. Health D-G: Malaysia Using Targeted Covid-19 Testing Approach for ‘High Impact, Reasonable Cost’. Kuala Lumpur 2020 [Updated 14 May 2020]. Available online: https://www.malaymail.com/news/malaysia/2020/05/14/health-d-g-malaysia-using-targeted-covid-19-testing-approach-for-high-impac/1866184 (accessed on 24 June 2020).
- Tang, A. Experts Divided over Mass Testing. Malaysia: The Star; 2020 [Updated 18 May 2020]. Available online: https://www.thestar.com.my/news/nation/2020/05/18/experts-divided-over-mass-testing (accessed on 24 June 2020).
- Korea Centers for Disease Control & Prevention. Contact Transmission of COVID-19 in South Korea: Novel Investigation Techniques for Tracing Contacts. Osong Public Health Res. Perspect 2020, 11, 60–63. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7045882/ (accessed on 17 June 2020). [CrossRef] [PubMed] [Green Version]
- Minister of Health and Welfare Korea. Korean Government’s Response System (as of 25 February 2020). Minister of Health and Welfare Korea; 2020. Available online: http://ncov.mohw.go.kr/en/baroView.do?brdId=11&brdGubun=111&dataGubun=&ncvContSeq=&contSeq=&board_id=&gubun= (accessed on 25 June 2020).
- Minister of Health and Welfare Korea. Regular Briefing of Central Disaster and Safety Countermeasure Headquarters on COVID-19. Korea: Minister of Health and Welfare Korea; 2020 [Updated 7 April 2020]. Available online: http://ncov.mohw.go.kr/en/tcmBoardView.do?brdId=12&brdGubun=125&dataGubun=&ncvContSeq=353968&contSeq=353968&board_id=1365&gubun= (accessed on 5 May 2020).
- PGCare. FAQ. Malaysia: PGCare; 2020 [Updated 31 August 2020]. Available online: https://pgcare.my/faq (accessed on 28 September 2020).
- National Disaster Management Agency. Soalan Lazim FAQ—Mengenai Applikasi MySejahtera MKN 2 June 2020 [National Disaster Management Agency, Frequently Asked Questions Regarding MySejahtera NSC Application 2 June 2020]. Malaysia: National Disaster Management Agency; 2020 [updated 2 June 2020]. Available online: http://portalbencana.nadma.gov.my/index.php/component/content/article/48-covid-19/faq/1553-soalan-lazim-faq-mengenai-applikasi-mysejahtera-mkn-02-06-2020 (accessed on 19 June 2020).
- Selangor State Government’s Task Force for Covid 19. SELangkah Frequently Asked Questions. Malaysia: Selangor State Government’s Task Force for Covid 19; 2020 [Updated 3 August 2020]. Available online: https://www.selangkah.my/web/#FAQ (accessed on 25 August 2020).
- Xin Hua She [Xin Hua News Agency]. Yituo Quanguo Yitihua Zhengwu Fuwu Ping Tai Gongxiang Xunxi Quanguo Jueda Bufen Diqu “Jiankangma” Yike Shixian “Yimatongxing” [Relying on the National Integrated Government Information Sharing Service Platform, the “Health QR Code” in Most Areas of the Countries Achieved “Passage by Unified Health QR Code”]. China: Xin Hua News Agency; 2020 [Updated 21 March 2020]. Available online: https://kpkesihatan.com/2020/05/06/kenyataan-akhbar-kpk-6-mei-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 25 June 2020).
- Ida Nadirah, I. SELangkah Merges with Malaysia’s MySejahtera App, Says Selangor MB. Malaysia: Media Selangor; 2020 [Updated 5 June 2020]. Available online: https://selangorjournal.my/2020/06/selangkah-merges-with-malaysias-mysejahtera-app-says-selangor-mb/ (accessed on 14 August 2020).
- PGCare. Thank You to Everyone. Malaysia: PGCare; 2020 [Updated 31 August 2020]. Available online: https://pgcare.my/home (accessed on 28 September 2020).
- Yusof, A.N.M.; Muuti, M.Z.; Ariffin, L.A.; Tan, M.K.M. Sharing Information on COVID-19: The ethical challenges in the Malaysian setting. Asian Bioeth. Rev. 2020, 12, 1–13. Available online: https://pubmed.ncbi.nlm.nih.gov/32837556/ (accessed on 5 July 2020). [CrossRef]
- Government of Singapore. Public Places Visited by Cases in the Community during Infectious Period. Singapore: Government of Singapore; 2020 [Updated 25 June 2020]. Available online: https://www.gov.sg/article/covid-19-public-places-visited-by-cases-in-the-community-during-infectious-period (accessed on 25 June 2020).
- The Government of the Hong Kong Special Administrative Region. Coronavirus Disease (COVID-19) in HK. Hong Kong: The Government of the Hong Kong Special Administrative Region; 2020 [Updated 7 October 2020]. Available online: https://chp-dashboard.geodata.gov.hk/covid-19/en.html (accessed on 7 October 2020).
- Ministry of Health Malaysia. MyHDW–Build Once, Use Many. Malaysia: Ministry of Health; 2017 [updated 20 April 2017]. Available online: https://kpkesihatan.com/2017/04/20/myhdw-build-once-use-many/ (accessed on 8 October 2020).
- Ministry of Health Malaysia. Malaysian Health Data Warehouse (MyHDW) 2015–2016 Start Up: Initiation. Malaysia: Ministry of Health Malaysia; 2017. Available online: https://myhdw.moh.gov.my/public/documents/20186/169489/MyHDW+2015-2016/86b7603a-eab4-40c0-aa94-35ded673838d (accessed on 8 October 2020).
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 26 Oktober 2020—Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia [Ministry of Health Malaysia Press Statement on 26 October 2020—Updates on the Coronavirus Disease 2019 (COVID-19) Situation in Malaysia]. Malaysia: Ministry of Health; 2020 [Updated 26 October 2020]. Available online: https://kpkesihatan.com/2020/10/26/kenyataan-akhbar-kpk-26-oktober-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 29 October 2020).
- Minister of Health Malaysia. Guidelines COVID-19 Management Annex 27 COVID-19: Management Guidelines for Special Settings. Minister of Health Malaysia; 2020 [Updated 25 March 2020]. Available online: http://www.moh.gov.my/moh/resources/Penerbitan/Garis%20Panduan/COVID19/Annex_27_COVID_guide_for_special_settings_25032020_.pdf (accessed on 18 April 2020).
- Akiyama, M.J.; Spaulding, A.C.; Rich, J.D. Flattening the Curve for Incarcerated Populations—Covid-19 in Jails and Prisons. N. Engl. J. Med. 2020, 382, 2075–2077. [Google Scholar] [CrossRef] [PubMed]
- Kinner, S.A.; Young, J.T.; Snow, K.; Southalan, L.; Lopez-Acuña, D.; Ferreira-Borges, C.; O’Moore, É. Prisons and custodial settings are part of a comprehensive response to COVID-19. Lancet Public Health 2020, 5, e188–e189. [Google Scholar] [CrossRef]
- Minister of Health Malaysia. Annex 27a Tindakan Pencegahan, Kawalan Infeksi dan Penggunaan Personal Protective Equipment (PPE) di Fasiliti Penjara, Lokap, Depot Imigresen, PUSPEN dan Rumah Perlindungan [Annex 27a Infection Prevention and Control and Usage of Personal Protective Equipment (PPE) at Prisons, Lockups, Immigration Depots, PUSPEN and Shelter Homes]. Minister of Health Malaysia; 2020 [Updated 26 June 2020]. Available online: http://covid-19.moh.gov.my/garis-panduan/garis-panduan-kkm/Annex_27a_SOP_IPC_Pusat_Tahanan_&_Rumah_Perlindungan.pdf (accessed on 8 October 2020).
- Ministry of Health Malaysia. Kenyataan Akhbar KPK 7 September 2020—Situasi Semasa Jangkitan Penyakit Coronavirus 2019 (COVID-19) di Malaysia [Ministry of Health Malaysia Press Statement on 7 September 2020—Updates on the Coronavirus Disease 2019 (COVID-19) Situation in Malaysia]. Malaysia: Ministry of Health; 2020 [Updated 7 September 2020]. Available online: https://kpkesihatan.com/2020/09/07/kenyataan-akhbar-kpk-7-september-2020-situasi-semasa-jangkitan-penyakit-coronavirus-2019-covid-19-di-malaysia/ (accessed on 8 October 2020).
- Bedi, R. Infected Detainees Could Have Been Initially Tested Negative When Virus Was Still in Incubation Period, Says Dr Noor Hisham. Malaysia: The Star; 2020 [Updated 4 June 2020]. Available online: https://www.thestar.com.my/news/nation/2020/06/04/infected-detainees-could-have-been-initially-tested-negative-when-virus-was-still-in-incubation-period-says-dr-noor-hisham (accessed on 8 October 2020).
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction–Based SARS-CoV-2 Tests by Time Since Exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef] [PubMed]
- Palasamy, Y. Govt Launches Ops Benteng to Prevent Foreigners Sneaking into Malaysia after Raya via ‘Rat Lanes’. Malaysia: Malay Mail; 2020 [Updated 28 May 2020]. Available online: https://www.malaymail.com/news/malaysia/2020/05/28/govt-launches-ops-benteng-to-prevent-foreigners-sneaking-into-malaysia-afte/1870289 (accessed on 8 October 2020).
- Bernama. Health D-G: No Discrimination in Handling of Covid-19 Cases. Malaysia: Bernama; 2020 [Updated 8 July 2020]. Available online: https://www.nst.com.my/news/nation/2020/07/606989/health-d-g-no-discrimination-handling-covid-19-cases (accessed on 8 October 2020).
- Bruns, D.P.; Kraguljac, N.V.; Bruns, T.R. COVID-19: Facts, Cultural Considerations, and Risk of Stigmatization. J. Transcult Nurs. 2020, 31, 326–332. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7324134/pdf/10.1177_1043659620917724.pdf (accessed on 7 October 2020). [CrossRef]
- Jaja, I.F.; Anyanwu, M.U.; Iwu Jaja, C.-J. Social distancing: How religion, culture and burial ceremony undermine the effort to curb COVID-19 in South Africa. Emerg. Microbes Infect. 2020, 9, 1077–1079. Available online: https://www.tandfonline.com/doi/full/10.1080/22221751.2020.1769501 (accessed on 7 October 2020). [CrossRef]
- Khoo, L.S.; Hasmi, A.H.; Ibrahim, M.A.; Mahmood, M.S. Management of the dead during COVID-19 outbreak in Malaysia. Forensic Sci. Med. Pathol. 2020, 16, 463–470. Available online: https://pubmed.ncbi.nlm.nih.gov/32519316 (accessed on 5 July 2020). [CrossRef]
- World Health Organisation. Infection Prevention and Control for the Safe Management of a Dead Body in the Context of COVID-19. World Health Organisation; 2020. Available online: https://apps.who.int/iris/rest/bitstreams/1272796/retrieve (accessed on 7 October 2020).






| Types of Lockdown | Nationwide Partial Lockdown | Localised Partial Lockdown with Mass Screening | Localised Complete Lockdown with Mass Screening | ||
|---|---|---|---|---|---|
| Name | Movement Control Order | Conditional Movement Control Order | Recovery Movement Control Order | Administrative Movement Control Order | Enhanced Movement Control Order |
| Period of time | 18 March–4 May | 5 May–9 June | 10 Jun–31 August | 2–5 weeks until screening completed | |
| Reason(s) of implementation | Second wave of outbreak spread nationwide | Fulfilled 6 WHO criteria to lift lockdown | Local transmission controlled | Localities with sudden increase of cases | Localities with sudden and continual surge of cases |
| Movement restriction | Highly regulated restriction of movement | Interstate travel allowed with permission | No restriction | Allowed movement within the localities | Highly regulated restriction of movement |
| Socioeconomic activities | All closed except essential services |
|
| All closed except retailers for essential items and/or food delivery services allowed to operate | All closed. Food was provided, retailers for essential items and/or food delivery services allowed to operate |
| Mass gatherings | Prohibited | Prohibited except festival celebrations allowed for immediate family members | Religious gathering and festival celebrations allowed with conditions | Prohibited | Prohibited |
| Points of entry |
| Allowed to enter or leave the area with valid reasons | Not allowed to enter or leave the area except authorised personnel | ||
| Educational institutions | Closed | Closed | Reopened by stages | Closed | Closed |
| Surveillance approach | Targeted screening approach |
| |||
| Enforcement agency | Police and army | Compliance Operations Task Force |
| ||
| WHO SPRP pillars | Measures implemented in all lockdowns straddled crossed Pillars 1–9 | ||||
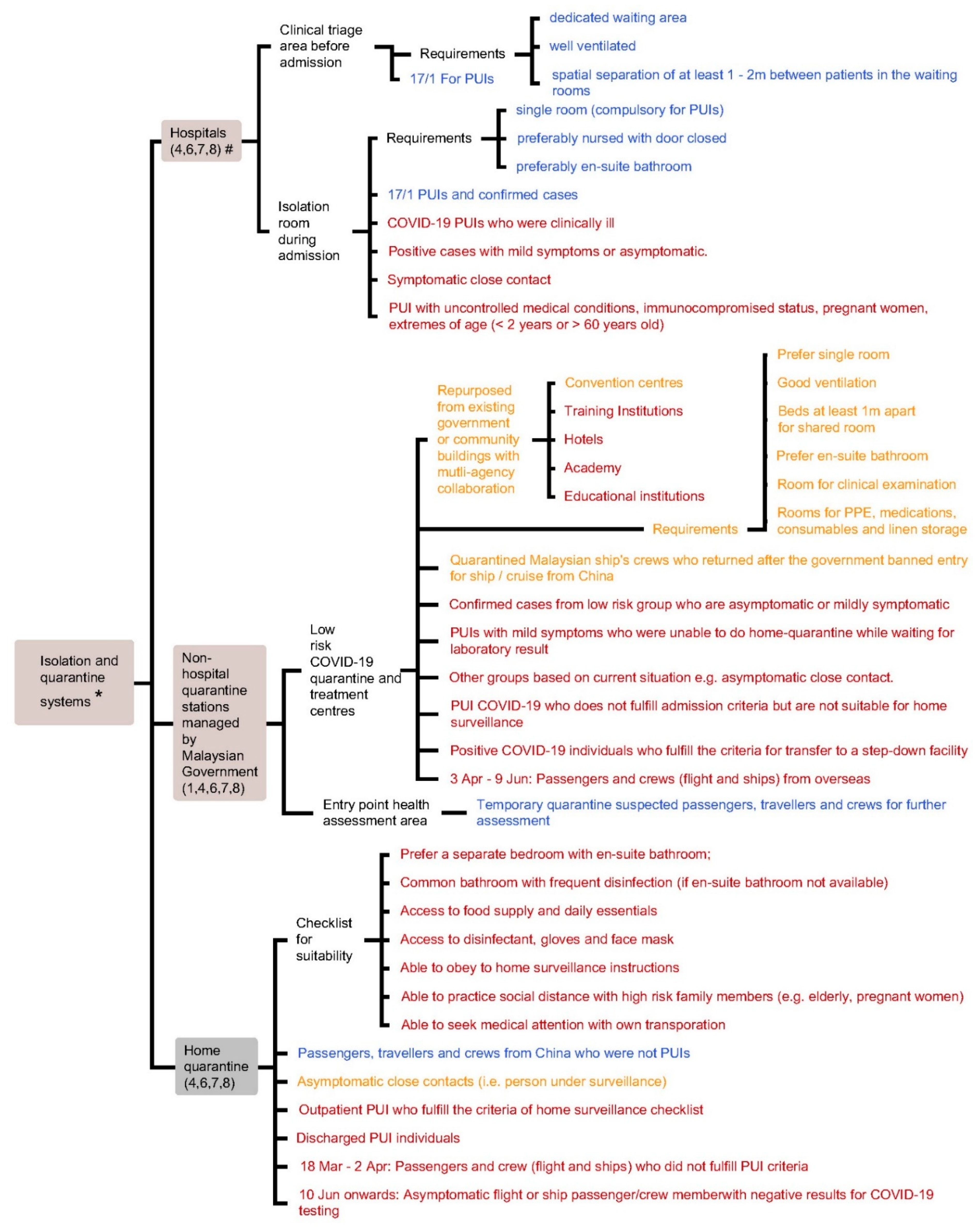
| Quarantine Stations | Institutionalised Quarantine Systems | Home Quarantine | |
|---|---|---|---|
| Hospital Isolation Room | Non-Hospital—Low Risk Quarantine and Treatment Centres | ||
| Facility requirements | Single room (compulsory for PUIs) preferably with closed door and en-suite bathroom |
|
|
| Criteria for admission |
| After 18 Mar:
|
|
| WHO SPRP pillars | 4,6,7,8 | 1,4,6,7,8 | 4,6,7,8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ang, Z.Y.; Cheah, K.Y.; Shakirah, M.S.; Fun, W.H.; Anis-Syakira, J.; Kong, Y.-L.; Sararaks, S. Malaysia’s Health Systems Response to COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 11109. https://doi.org/10.3390/ijerph182111109
Ang ZY, Cheah KY, Shakirah MS, Fun WH, Anis-Syakira J, Kong Y-L, Sararaks S. Malaysia’s Health Systems Response to COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(21):11109. https://doi.org/10.3390/ijerph182111109
Chicago/Turabian StyleAng, Zen Yang, Kit Yee Cheah, Md. Sharif Shakirah, Weng Hong Fun, Jailani Anis-Syakira, Yuke-Lin Kong, and Sondi Sararaks. 2021. "Malaysia’s Health Systems Response to COVID-19" International Journal of Environmental Research and Public Health 18, no. 21: 11109. https://doi.org/10.3390/ijerph182111109