
Identification of COVID-19 Waves: Considerations for Research and Policy

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods and Materials
2.1. Statistical Strategy
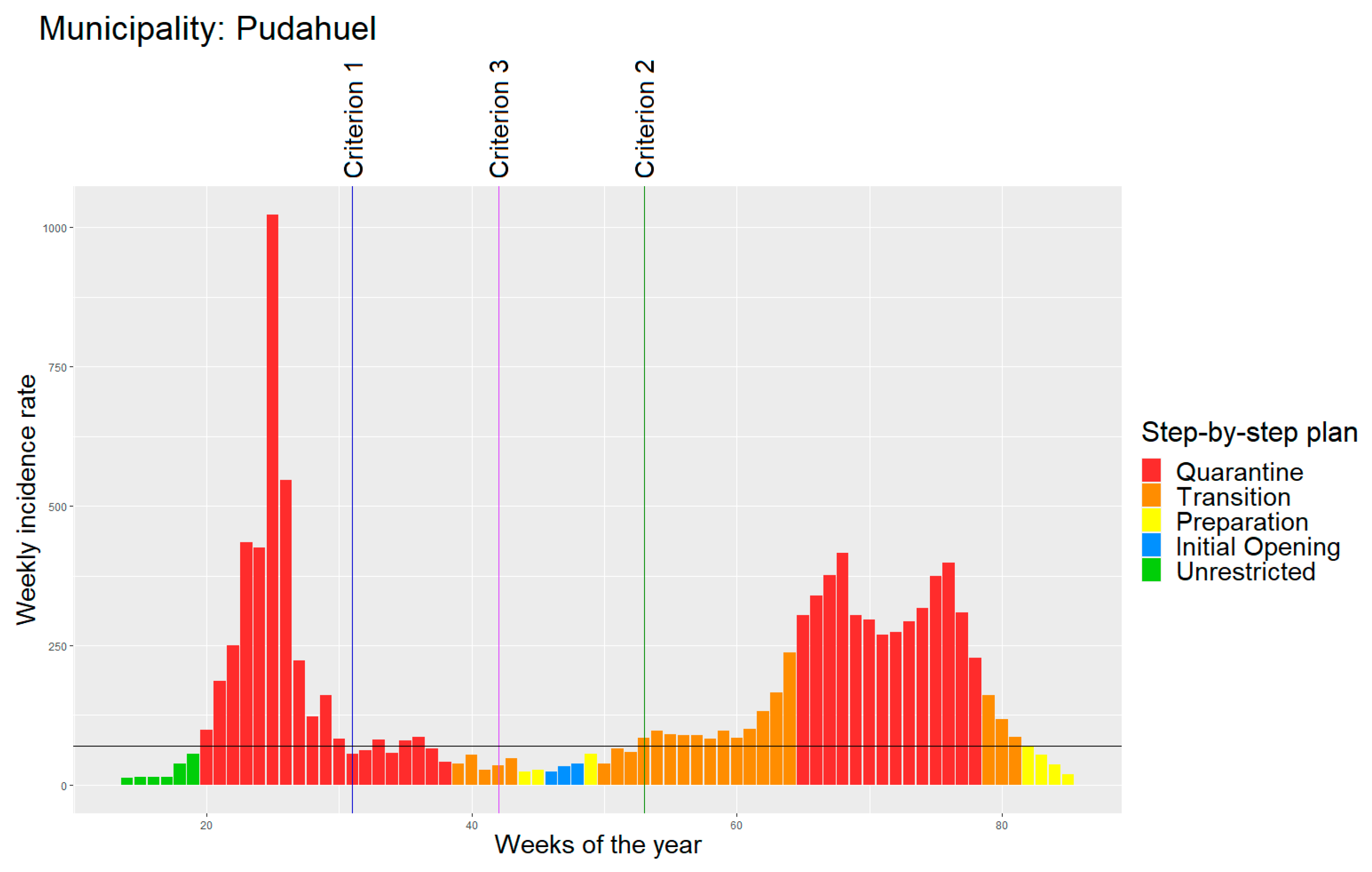
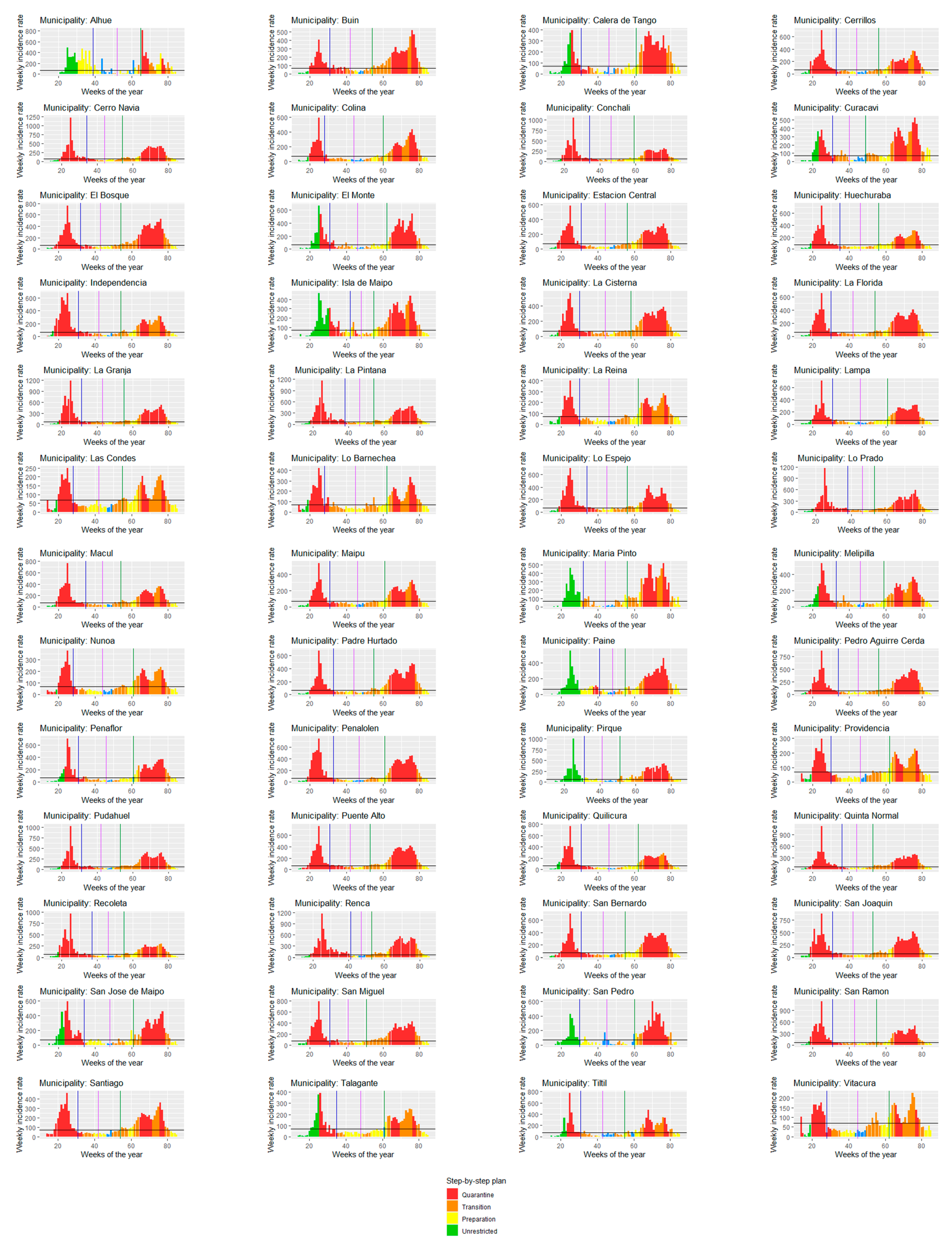
- Starting date: week of the first reported case.
- End of first wave (criterion 1): first week (since the starting date) that fulfilled the following conditions:
- Weekly incidence rate lower than 70 cases per 100,000 people (70/100,000 cases);
- Negative growth incidence rate for at least two consecutive weeks.
- Start of second wave (criterion 2): first week (since the end of the first wave) that fulfilled the following conditions:
- Weekly incidence rate higher than 70/100,000 cases;
- Positive growth incidence rate in at least one week in which the municipality presented over 70/100,000 cases.
- Average threshold (criterion 3): average week between the end of the first wave and the start of the second wave.
2.2. Data
3. Results
4. Discussion
4.1. Perspectives
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koffman, J.; Gross, J.; Etkind, S.N.; Selman, L. Uncertainty and COVID-19: How are we to respond? J. R. Soc. Med. 2020, 113, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Rutter, H.; Wolpert, M.; Greenhalgh, T. Managing uncertainty in the covid-19 era. BMJ 2020, 370. [Google Scholar] [CrossRef] [PubMed]
- Van Damme, W.; Dahake, R.; Delamou, A.; Ingelbeen, B.; Wouters, E.; Vanham, G.; Van De Pas, R.; Dossou, J.-P.; Ir, P.; Abimbola, S.; et al. The COVID-19 pandemic: Diverse contexts; different epidemics—How and why? BMJ Glob. Health 2020, 5, e003098. [Google Scholar] [CrossRef] [PubMed]
- Glenn, J.; Chaumont, C.; Villalobos Dintrans, P. Public health leadership in the times of COVID-19: A comparative case study of three countries. Int. J. Public Leadersh. 2020, 17, 81–94. [Google Scholar] [CrossRef]
- Iftimie, S.; López-Azcona, A.F.; Vallverdú, I.; Hernández-Flix, S.; De Febrer, G.; Parra, S.; Hernández-Aguilera, A.; Riu, F.; Joven, J.; Andreychuk, N.; et al. First and second waves of coronavirus disease-19: A comparative study in hospitalized patients in Reus, Spain. PLoS ONE 2021, 16, e0248029. [Google Scholar] [CrossRef]
- Soriano, V.; Ganado-Pinilla, P.; Sanchez-Santos, M.; Gómez-Gallego, F.; Barreiro, P.; De Mendoza, C.; Corral, O. Main differences between the first and second waves of COVID-19 in Madrid, Spain. Int. J. Infect. Dis. 2021, 105, 374–376. [Google Scholar] [CrossRef] [PubMed]
- Salyer, S.J.; Maeda, J.; Sembuche, S.; Kebede, Y.; Tshangela, A.; Moussif, M.; Ihekweazu, C.; Mayet, N.; Abate, E.; Ouma, A.O.; et al. The first and second waves of the COVID-19 pandemic in Africa: A cross-sectional study. Lancet 2021, 397, 1265–1275. [Google Scholar] [CrossRef]
- Jain, V.K.; Iyengar, K.P.; Vaishya, R. Differences between First wave and Second wave of COVID-19 in India. Diabetes Metab. Syndr. 2021, 15, 1047–1048. [Google Scholar] [CrossRef] [PubMed]
- Coccia, M. The impact of first and second wave of the COVID-19 pandemic in society: Comparative analysis to support control measures to cope with negative effects of future infectious diseases. Environ. Res. 2021, 197, 111099. [Google Scholar] [CrossRef] [PubMed]
- Chowell, G.; Rothenberg, R.; Roosa, K.; Tariq, A.; Hyman, J.M.; Luo, R. Sub-epidemic model forecasts for COVID-19 pandemic spread in the USA and European hotspots. MedRxiv 2020. [Google Scholar] [CrossRef]
- COVID-19 Explorer. Available online: https://worldhealthorg.shinyapps.io/covid/ (accessed on 20 August 2021).
- Available online: https://coronavirus.jhu.edu (accessed on 20 August 2021).
- Castillo, C.; Villalobos Dintrans, P.; Maddaleno, M. The successful COVID-19 vaccine rollout in Chile: Factors and challenges. Vaccine X 2021, 9. [Google Scholar] [CrossRef]
- Villalobos Dintrans, P.; Castillo, C.; De La Fuente, F.; Maddaleno, M. COVID-19 incidence and mortality in the Metropolitan Region, Chile: Time, space, and structural factors. PLoS ONE 2021, 16, e0250707. [Google Scholar] [CrossRef]
- Mena, G.E.; Martinez, P.P.; Mahmud, A.S.; Marquet, P.A.; Buckee, C.O.; Santillana, M. Socioeconomic status determines COVID-19 incidence and related mortality in Santiago, Chile. Sci. 2021, 372, eabg5298. [Google Scholar] [CrossRef]
- Proyecciones de Población. Available online: https://www.ine.cl/estadisticas/sociales/demografia-y-vitales/proyecciones-de-poblacion (accessed on 20 August 2021).
- Actualización al Plan PASO a PASO Nos Cuidamos. Available online: https://s3.amazonaws.com/gobcl-prod/public_files/Campañas/Corona-Virus/documentos/paso-a-paso/Documento_actualizacion_Paso_a_Paso.pdf (accessed on 20 August 2021).
- Actualización de la Estrategia Gradual “Paso a Paso nos Cuidamos”. Available online: http://www.seguridadciudadana.gob.cl/media/2021/01/210111-Actualizacion-Paso-a-Paso.pdf (accessed on 20 August 2021).
- Encuesta de Caracterización Socioeconómica Nacional CASEN 2017. Available online: http://observatorio.ministeriodesarrollosocial.gob.cl/encuesta-casen-2017 (accessed on 20 August 2021).
- Actualización de la Definición de Caso Sospechoso, Probable y Confirmado Para Vigilancia Epidemiológica Ante Pandemia de COVID-19 en Chile. Available online: https://www.minsal.cl/wp-content/uploads/2021/02/ORD-536-04-02-2021.pdf (accessed on 20 August 2021).
- Plan de acción coronavirus COVID-19: Tipo de Caso y Contacto COVID19. Available online: https://saludresponde.minsal.cl/tipos-de-caso-y-contacto-covid19/#:~:text=Si%20por%20cualquier%20motivo%2C%20un,realizar%20aislamiento%20como%20caso%20confirmado (accessed on 20 August 2021).
- MinCiencia/Datos-COVID19. Available online: https://github.com/MinCiencia/Datos-COVID19 (accessed on 9 August 2021).
- Available online: https://deis.minsal.cl/#datosabiertos (accessed on 9 August 2021).
- Hale, T.; Angrist, N.; Hale, A.J.; Kira, B.; Majumdar, S.; Petherick, A.; Phillips, T.; Sridhar, D.; Thompson, R.N.; Webster, S.; et al. Government responses and COVID-19 deaths: Global evidence across multiple pandemic waves. PLoS ONE 2021, 16, e0253116. [Google Scholar] [CrossRef] [PubMed]
- Villalobos Dintrans, P.; Chaumont, C. Examining the relationship between human resources and mortality: The effects of methodological choices. Int. J. Public Health 2017, 62, 361–370. [Google Scholar] [CrossRef] [PubMed]
- Zhang, S.X.; Arroyo Marioli, F.; Gao, R.; Wang, S. A Second Wave? What Do People Mean by COVID Waves?–A Working Definition of Epidemic Waves. Risk Manag. Healthc. Policy 2021, 14, 3775–3782. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | Criterion 1: End of First Wave | Criterion 2: Start of Second Wave | Criterion 3: Average Threshold | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Max | Min | Moran I | Mean | Max | Min | Moran I | Mean | Max | Min | Moran I | |
| Duration (days) | 130.981 | 193 | 95 | 0.111 * | 300.596 | 340 | 249 | 0.253 *** | 215.481 | 240 | 186 | 0.070 |
| Cases | 3403.787 | 6281.746 | 1406.369 | 0.381 *** | 4536.999 | 6965.738 | 2689.269 | 0.336 *** | 3940.650 | 6471.989 | 1914.770 | 0.374 *** |
| Deaths | 125.465 | 271.645 | 33.464 | 0.431 *** | 174.446 | 387.238 | 41.831 | 0.392 *** | 153.225 | 336.377 | 33.464 | 0.411 *** |
| Cases/duration | 25.789 | 45.613 | 13.788 | 0.399 *** | 15.270 | 24.595 | 8.704 | 0.426 *** | 18.336 | 30.461 | 8.664 | 0.437 *** |
| Deaths/duration | 0.951 | 2.245 | 0.314 | 0.405 *** | 0.586 | 1.340 | 0.137 | 0.445 *** | 0.712 | 1.633 | 0.167 | 0.411 *** |
| Variable | First 100 Days | Criterion 1 | Criterion 2 | Criterion 3 | |||
|---|---|---|---|---|---|---|---|
| Cases | Cases | Cases/Duration | Cases | Cases/Duration | Cases | Cases/Duration | |
| Population density | 4.25 × 10−5 * | 4.276 × 10−7 *** | 1.444 × 10−7 | 1.898 × 10−7 | |||
| Multidimensional poverty | 5.691 *** | 7.573 *** | 4.146 × 10−2 *** | 6.466 *** | 0.026 *** | 7.381 *** | 7.577 × 10−3 |
| Distance to health center | 2.678 ** | 1.395 × 10−2 * | 3.121 *** | 0.013 | 2.624 ** | 0.033 *** | |
| Use public transportation | 4.697 *** | 5.775 *** | 4.381 ** | 7.614 × 10−3 * | 5.415 *** | ||
| Difficult getting healthcare | −31.23 | ||||||
| Years of education | 0.019 | ||||||
| Constant | 33.57 | −1804.636 | 1.816 | −530.253 | −0.626 | −1104.243 | −0.668 |
| R-squared | 0.568 | 0.531 | 0.427 | 0.489 | 0.500 | 0.519 | 0.507 |
| Adjusted R-squared | 0.532 | 0.502 | 0.391 | 0.457 | 0.458 | 0.489 | 0.465 |
| Moran’s I (residuals) | 0.081 | 0.11979 * | 0.180 ** | 0.131 ** | 0.141 | 0.143 ** | 0.168 ** |
| Variables | First 100 Days | Criterion 1 | Criterion 2 | Criterion 3 | |||
|---|---|---|---|---|---|---|---|
| Deaths | Deaths | Deaths/ Duration | Deaths | Deaths/ Duration | Deaths | Deaths/ Duration | |
| People 65+ | 0.147 * | 0.216 × 10−1 * | 1.783 × 10−3 ** | 0.292 * | 9.697 × 10−4 * | 0.256 * | 1.185 × 10−3 * |
| Population density | 2.61 × 10−6 *** | 3.081 × 10−6 *** | 2.194 × 10−8 *** | 3.328 × 10−6 ** | 1.206 × 10−8 *** | 3.143 × 10−6 *** | 1.504 × 10−8 *** |
| Rurality | −0.056 *** | −0.083 *** | −6.043 × 10−4 *** | −0.120 *** | −3.910 × 10−4 *** | −0.118 *** | −5.235 × 10−4 *** |
| Multidimensional poverty | 0.115 * | 0.174 ** | 8.034 × 10−4 * | 0.163 * | 6.161 × 10−4 * | 0.182 ** | 7.561 × 10−4 ** |
| Distance to health center | −0.0016 | ||||||
| Cumulative incidence | 0.023 *** | 0.022 *** | 0.023 *** | 0.023 *** | 0.024 *** | 0.020 *** | 2.179 × 10−2 *** |
| Constant | −15.59 | −23.61 | −0.108 | −12.04 | −0.071 | −5.104 | −0.039 |
| R-squared | 0.805 | 0.7845 | 0.7214 | 0.678 | 0.7155 | 0.725 | 0.726 |
| Adjusted R-squared | 0.780 | 0.7611 | 0.6911 | 0.643 | 0.6845 | 0.695 | 0.696 |
| Moran’s I (residuals) | −0.0056 | −0.032755 | −0.04043 | −0.020 | −0.013448 | −3.154 × 10−5 | −0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayala, A.; Villalobos Dintrans, P.; Elorrieta, F.; Castillo, C.; Vargas, C.; Maddaleno, M. Identification of COVID-19 Waves: Considerations for Research and Policy. Int. J. Environ. Res. Public Health 2021, 18, 11058. https://doi.org/10.3390/ijerph182111058
Ayala A, Villalobos Dintrans P, Elorrieta F, Castillo C, Vargas C, Maddaleno M. Identification of COVID-19 Waves: Considerations for Research and Policy. International Journal of Environmental Research and Public Health. 2021; 18(21):11058. https://doi.org/10.3390/ijerph182111058
Chicago/Turabian StyleAyala, Andrés, Pablo Villalobos Dintrans, Felipe Elorrieta, Claudio Castillo, Claudio Vargas, and Matilde Maddaleno. 2021. "Identification of COVID-19 Waves: Considerations for Research and Policy" International Journal of Environmental Research and Public Health 18, no. 21: 11058. https://doi.org/10.3390/ijerph182111058