
COVID-19 Infection in Academic Dental Hospital Personnel; A Cross-Sectional Survey in Saudi Arabia

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
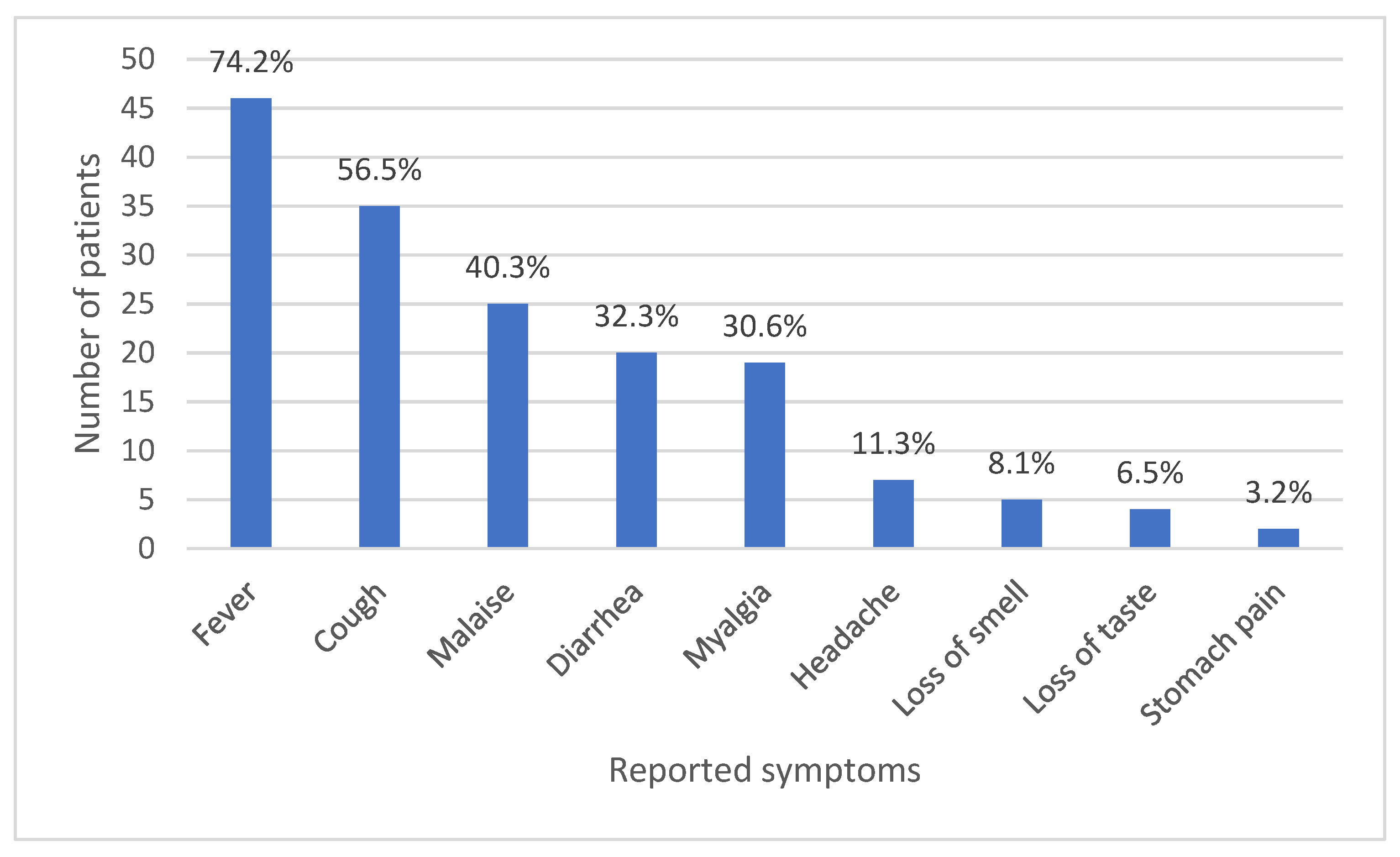
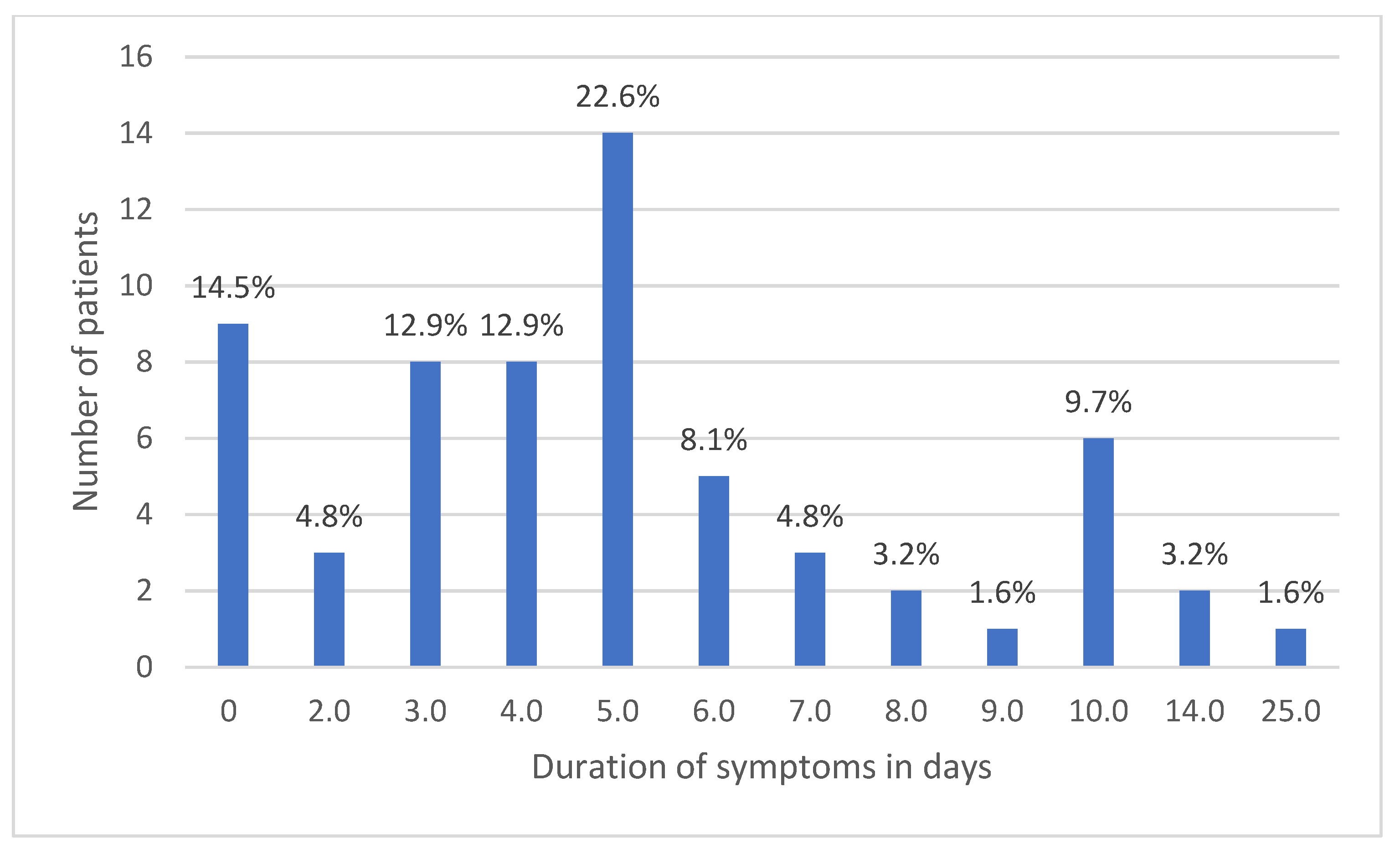
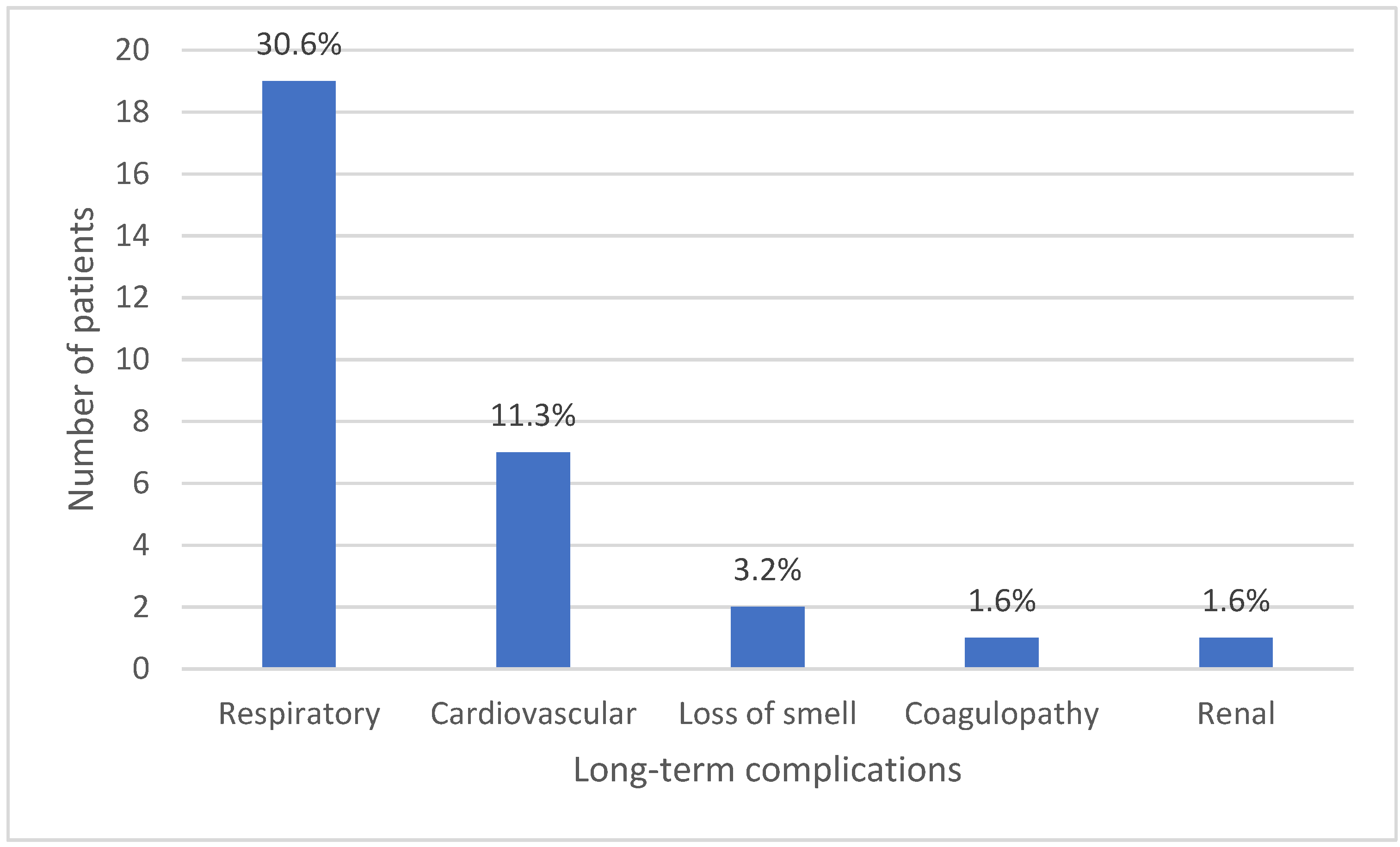
Characteristics of COVID-19 among Infected Personnel
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Elsayed, S.; Abu-Hammad, O.; Alolayan, A.; Althagafi, N.; Ayed, Y.; Dar-Odeh, N. Getting to Know SARS-CoV-2: Towards a Better Understanding of the Factors Influencing Transmission. Pesqui. Bras. Odontopediatr. Clin. Integr. 2020, 20. [Google Scholar] [CrossRef]
- Abdelgawad, N.; Elsayed, S.A.; Babkair, H.; Dar-Odeh, N. Verrucous leukoplakia affecting the tongue of a patient recovered from COVID-19. Minerva Dent. Oral Sci. 2021, 70, 128–130. [Google Scholar] [CrossRef] [PubMed]
- Abu-Hammad, S.; Dar-Odeh, N.; Abu-Hammad, O. SARS-CoV-2 and oral ulcers: A causative agent or a predisposing factor? Oral Dis. 2020. [Google Scholar] [CrossRef]
- Mahase, E. Covid-19: What do we know about ‘long covid’? BMJ 2020, 370, m2815. [Google Scholar] [CrossRef] [PubMed]
- Sivan, M.; Taylor, S. NICE guideline on long covid. BMJ 2020, 371, m4938. [Google Scholar] [CrossRef]
- Dar-Odeh, N.; Borzangy, S.; Babkair, H.; Farghal, L.; Shahin, G.; Fadhlalmawla, S.; Alhazmi, W.; Taher, S.; Abu-Hammad, O. Association of Dental Caries, Retained Roots, and Missing Teeth with Physical Status, Diabetes Mellitus and Hypertension in Women of the Reproductive Age. Int. J. Environ. Res. Public Health 2019, 16, 2565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alharbi, N.K.; Alghnam, S.; Algaissi, A.; Albalawi, H.; Alenazi, M.W.; Albargawi, A.M.; Alharbi, A.G.; Alhazmi, A.; Al Qarni, A.; Alfarhan, A.; et al. Nationwide Seroprevalence of SARS-CoV-2 in Saudi Arabia. J. Infect. Public Health 2021, 14, 832–838. [Google Scholar] [CrossRef]
- Hammad, O.A.; Alnazzawi, A.; Borzangy, S.S.; Abu-Hammad, A.; Fayad, M.; Saadaledin, S.; Abu-Hammad, S.; Odeh, N.D. Factors Influencing Global Variations in COVID-19 Cases and Fatalities; A Review. Healthcare 2020, 8, 216. [Google Scholar] [CrossRef]
- Dar-Odeh, N.; Othman, B.; Bahabri, R.; Alnazzawi, A.; Borzangy, S.; Fadel, H.; Alolayan, A.; Abu-Hammad, O. Antibiotic self-medication for oral conditions: Characteristics and associated factors. Pesqui. Bras. Odontopediatr. Clin. Integr. 2018, 18, 3890. [Google Scholar] [CrossRef] [Green Version]
- Araujo, M.W.B.; Estrich, C.G.; Mikkelsen, M.; Morrissey, R.; Harrison, B.; Geisinger, M.L.; Ioannidou, E.; Vujicic, M. COVID-2019 among dentists in the United States: A 6-month longitudinal report of accumulative prevalence and incidence. J. Am. Dent. Assoc. 2021, 152, 425–433, reprinted in J. Am. Dent. Assoc. 2021, 52, 588. [Google Scholar] [CrossRef]
- Gómez-Ochoa, S.A.; Franco, O.H.; Rojas, L.Z.; Raguindin, P.F.; Roa-Díaz, Z.M.; Wyssmann, B.M.; Guevara, S.L.R.; Echeverría, L.E.; Glisic, M.; Muka, T. COVID-19 in Health-Care Workers: A Living Systematic Review and Meta-Analysis of Prevalence, Risk Factors, Clinical Characteristics, and Outcomes. Am. J. Epidemiol. 2021, 190, 161–175, reprinted in Am. J. Epidemiol. 2021, 190, 187. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, K.; Kagaya, K.; Zarebski, A.; Chowell, G. Estimating the asymptomatic proportion of coronavirus disease 2019 (COVID-19) cases on board the Diamond Princess cruise ship, Yokohama, Japan, 2020. Eurosurveillance 2020, 25, 2000180. [Google Scholar] [CrossRef] [Green Version]
- Nishiura, H.; Kobayashi, T.; Miyama, T.; Suzuki, A.; Jung, S.M.; Hayashi, K.; Kinoshita, R.; Yang, Y.; Yuan, B.; Akhmetzhanov, A.R.; et al. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). Int. J. Infect. Dis. 2020, 94, 154–155. [Google Scholar] [CrossRef] [PubMed]
- Rivett, L.; Sridhar, S.; Sparkes, D.; Routledge, M.; Jones, N.K.; Forrest, S.; Young, J.; Pereira-Dias, J.; Hamilton, W.L.; Ferris, M.; et al. Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission. Elife 2020, 9, e58728. [Google Scholar] [CrossRef]
- COVID Live Update: 216,420,171 Cases and 4,502,965 Deaths from the Coronavirus—Worldometer. Available online: https://www.worldometers.info/coronavirus/#countries (accessed on 28 August 2021).
- Age, Gender, and Territory of COVID-19 Infections and Fatalities—Publications Office of the EU. Available online: https://op.europa.eu/en/publication-detail/-/publication/6660b754-a930-11ea-bb7a-01aa75ed71a1/language-en (accessed on 29 August 2021).
- Dar-Odeh, N.; Elsayed, S.; Babkair, H.; Abu-Hammad, S.; Althagafi, N.; Bahabri, R.; Eldeen, Y.S.; Aljohani, W.; Abu-Hammad, O. What the dental practitioner needs to know about pharmaco-therapeutic modalities of COVID-19 treatment: A review. J. Dent. Sci. 2021, 16, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Kwon, S.; Joshi, A.D.; Lo, C.; Drew, D.A.; Nguyen, L.H.; Guo, C.; Ma, W.; Mehta, R.S.; Shebl, F.M.; Warner, E.T.; et al. Association of social distancing and face mask use with risk of COVID-19. Nat. Commun. 2021, 12, 3737. [Google Scholar] [CrossRef]
- Odeh, N.D.; Babkair, H.; Abu-Hammad, S.; Borzangy, S.; Abu-Hammad, A.; Abu-Hammad, O. COVID-19: Present and Future Challenges for Dental Practice. Int. J. Environ. Res. Public Health 2020, 17, 3151. [Google Scholar] [CrossRef]
- Li, Z.-Y.; Zhang, Y.; Peng, L.-Q.; Gao, R.-R.; Jing, J.-R.; Wang, J.-L.; Ren, B.-Z.; Xu, J.-G.; Wang, T. Demand for longer quarantine period among common and uncommon COVID-19 infections: A scoping review. Infect. Dis. Poverty 2021, 10, 56. [Google Scholar] [CrossRef]
- Elsayed, S.A.; Abu-Hammad, O.; Alolayan, A.B.; Eldeen, Y.S.; Dar-Odeh, N. Fallacies and Facts Around COVID-19: The Multifaceted Infection. J. Craniofac. Surg. 2020, 31, e643–e644. [Google Scholar] [CrossRef] [PubMed]
- Jones, R.; Davis, A.; Stanley, B.; Julious, S.; Ryan, D.; Jackson, D.J.; Halpin, D.M.; Hickman, K.; Pinnock, H.; Quint, J.K.; et al. Risk Predictors and Symptom Features of Long COVID Within a Broad Primary Care Patient Population Including Both Tested and Untested Patients. Pragmat. Obs. Res. 2021, 12, 93–104. [Google Scholar] [CrossRef]
- Ladds, E.; Rushforth, A.; Wieringa, S.; Taylor, S.; Rayner, C.; Husain, L.; Greenhalgh, T. Developing services for long COVID: Lessons from a study of wounded healers. Clin. Med. 2021, 21, 59–65, reprinted in Clin. Med. 2021, 21, 160. [Google Scholar] [CrossRef] [PubMed]
- Abu-Hammad, O.; Dar-Odeh, N.; Abu-Hammad, A.; Althagafi, N.; Eshky, R.; Abu-Hammad, S. Long-Term Complications of Coronavirus Disease 2019, What the Oral Surgeon Needs to Know. J. Craniofac. Surg. 2021, 32, e652–e655. [Google Scholar] [CrossRef]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631, reprinted in Nat. Med. 2021, 27, 1116. [Google Scholar] [CrossRef] [PubMed]
- Dubey, S.; Biswas, P.; Ghosh, R.; Chatterjee, S.; Dubey, M.J.; Chatterjee, S.; Lahiri, D.; Lavie, C.J. Psychosocial impact of COVID-19. Diabetes Metab. Syndr. 2020, 14, 779–788. [Google Scholar] [CrossRef] [PubMed]
- Hossain, M.M.; Tasnim, S.; Sultana, A.; Faizah, F.; Mazumder, H.; Zou, L.; McKyer, E.; Ahmed, H.U.; Ma, P. Epidemiology of mental health problems in COVID-19: A review. F1000Res 2020, 9, 636. [Google Scholar] [CrossRef]
- Gallè, F.; Sabella, E.; Roma, P.; De Giglio, O.; Caggiano, G.; Tafuri, S.; Da Molin, G.; Ferracuti, S.; Montagna, M.; Liguori, G.; et al. Knowledge and Acceptance of COVID-19 Vaccination among Undergraduate Students from Central and Southern Italy. Vaccines 2021, 9, 638. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Socio-Professional Demographics | COVID-19 InfectionN (%) | p-Value |
|---|---|---|
| Gender | 0.262 | |
| Females | 30 (17.3%) | |
| Males | 32 (22.4%) | |
| Age (years) | 0.816 | |
| <40 | 53 (19.4%) | |
| ≥40 | 9 (20.9%) | |
| Role in College | 0.109 | |
| Faculty member | 14 (14.3%) | |
| Student | 48 (22.0%) |
| Infection Aspects | Frequency (%) |
|---|---|
| Source of infection | |
| Do not know | 21 (33.9%) |
| Family/friends | 25 (40.3%) |
| Dental hospital | 15 (24.2%) |
| Marketplace | 1 (1.6%) |
| Failure of proper cross infection control practices | |
| Face masks | 10 (16.1%) |
| Hand washing | 14 (22.6%) |
| Distancing | 38 (61.3%) |
| Quarantine practiced | |
| Yes | 55 (88.7%) |
| No | 7 (11.3%) |
| Duration of Symptoms | Long-Term Complications | |||
|---|---|---|---|---|
| ≤5 Days | >5 Days | No | Yes | |
| Age (years) | ||||
| <40 | 39 (73.6%) | 14 (26.4%) | 31 (58.5%) | 22 (41.5%) |
| ≥40 | 3 (33.3%) | 6 (66.7%) | 7 (77.8%) | 2 (22.2%) |
| p-value | 0.017 | 0.272 | ||
| Gender | ||||
| Female | 15 (50.0%) | 15 (50.0%) | 25 (83.3%) | 5 (16.7%) |
| Male | 27 (84.4%) | 5 (15.6%) | 13 (40.6%) | 19 (59.4%) |
| p-value | 0.004 | 0.001 | ||
| Role groups | ||||
| Faculty member | 6 (42.9%) | 8 (57.1%) | 12 (85.7%) | 2 (14.3%) |
| Student | 36 (75.0%) | 12 (25.0%) | 26 (54.2%) | 22 (45.8%) |
| p-value | 0.024 | 0.033 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abu-Hammad, O.; Alnazzawi, A.; Babkair, H.; Jambi, S.; Mirah, M.; Abdouh, I.; Aljohani, R.S.; Ayeq, R.; Ghazi, L.; Al-subhi, H.; et al. COVID-19 Infection in Academic Dental Hospital Personnel; A Cross-Sectional Survey in Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 10911. https://doi.org/10.3390/ijerph182010911
Abu-Hammad O, Alnazzawi A, Babkair H, Jambi S, Mirah M, Abdouh I, Aljohani RS, Ayeq R, Ghazi L, Al-subhi H, et al. COVID-19 Infection in Academic Dental Hospital Personnel; A Cross-Sectional Survey in Saudi Arabia. International Journal of Environmental Research and Public Health. 2021; 18(20):10911. https://doi.org/10.3390/ijerph182010911
Chicago/Turabian StyleAbu-Hammad, Osama, Ahmad Alnazzawi, Hamzah Babkair, Safa Jambi, Maher Mirah, Ismail Abdouh, Rahaf Saeed Aljohani, Rahaf Ayeq, Layan Ghazi, Heba Al-subhi, and et al. 2021. "COVID-19 Infection in Academic Dental Hospital Personnel; A Cross-Sectional Survey in Saudi Arabia" International Journal of Environmental Research and Public Health 18, no. 20: 10911. https://doi.org/10.3390/ijerph182010911