
Not Just a ‘Breath of Death’: Indirect Consequences of Working in a COVID-19 Unit


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Aim, Questionnaire Design and Distribution
2.2. Participants Selection Criteria
2.3. Data Analysis
2.4. Compliance with Ethical Standards
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- COVID Live Update: 194,488,251 Cases and 4,167,414 Deaths from the Coronavirus—Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 24 July 2021).
- CDC. Scientific Brief: SARS-CoV-2 Transmission. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/science-briefs/sars-cov-2-transmission.html (accessed on 24 July 2021).
- Jeon, Y.W.; Park, E.S.; Jung, S.J.; Kim, Y.; Choi, J.Y.; Kim, H.C. Protection of Healthcare Workers against COVID-19 at a Large Teaching Hospital in Seoul, Korea. Yonsei Med. J. 2020, 61, 631–634. [Google Scholar] [CrossRef] [PubMed]
- Satiani, B.; Zigrang, T.A.; Bailey-Wheaton, J.L. COVID-19 Financial Resources for Physicians. J. Vasc. Surg. 2020, 72, 1161–1165. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization, Regional Office for Europe. Strengthening the Health Financing Response to COVID-19 in Europe; World Health Organization, Regional Office for Europe: Geneva, Switzerland, 2020. [Google Scholar]
- Talevi, D.; Socci, V.; Carai, M.; Carnaghi, G.; Faleri, S.; Trebbi, E.; di Bernardo, A.; Capelli, F.; Pacitti, F. Mental Health Outcomes of the CoViD-19 Pandemic. Riv. Psichiatr. 2020, 55, 137–144. [Google Scholar] [PubMed]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of Depression, Anxiety, and Insomnia among Healthcare Workers during the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.; et al. A Multinational, Multicentre Study on the Psychological Outcomes and Associated Physical Symptoms amongst Healthcare Workers during COVID-19 Outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef] [PubMed]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental Health Outcomes among Frontline and Second-Line Health Care Workers during the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef] [PubMed]
- Giorgi, G.; Lecca, L.I.; Alessio, F.; Finstad, G.L.; Bondanini, G.; Lulli, L.G.; Arcangeli, G.; Mucci, N. COVID-19-Related Mental Health Effects in the Workplace: A Narrative Review. Int. J. Environ. Res. Public Health 2020, 17, 7857. [Google Scholar] [CrossRef] [PubMed]
- Guha, A.; Plzak, J.; Schalek, P.; Chovanec, M. Extremely Wicked, Shockingly Evil and Undoubtedly COVID-19: The Silent Serial Killer. Eur. Arch. Otorhinolaryngol. 2021, 278, 2101–2106. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Zhou, M.; Tang, F.; Wang, Y.; Nie, H.; Zhang, L.; You, G. Knowledge, Attitude, and Practice Regarding COVID-19 among Healthcare Workers in Henan, China. J. Hosp. Infect. 2020, 105, 183–187. [Google Scholar] [CrossRef] [PubMed]
- Abdel Wahed, W.Y.; Hefzy, E.M.; Ahmed, M.I.; Hamed, N.S. Assessment of Knowledge, Attitudes, and Perception of Health Care Workers Regarding COVID-19, A Cross-Sectional Study from Egypt. J. Community Health 2020, 45, 1242–1251. [Google Scholar] [CrossRef] [PubMed]
- Martinese, F.; Keijzers, G.; Grant, S.; Lind, J. How Would Australian Hospital Staff React to an Avian Influenza Admission, or an Influenza Pandemic? Emerg. Med. Australas. 2009, 21, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Skoda, E.-M.; Teufel, M.; Stang, A.; Jöckel, K.-H.; Junne, F.; Weismüller, B.; Hetkamp, M.; Musche, V.; Kohler, H.; Dörrie, N.; et al. Psychological Burden of Healthcare Professionals in Germany during the Acute Phase of the COVID-19 Pandemic: Differences and Similarities in the International Context. J. Public Health 2020, 42, 688–695. [Google Scholar] [CrossRef] [PubMed]
- Gholami, M.; Fawad, I.; Shadan, S.; Rowaiee, R.; Ghanem, H.; Hassan Khamis, A.; Ho, S.B. COVID-19 and Healthcare Workers: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2021, 104, 335–346. [Google Scholar] [CrossRef] [PubMed]
- Derek, M.; Tsai, F.-J.; Kim, J.; Tejamaya, M.; Putri, V.; Muto, G.; Reginald, A.; Phanprasit, W.; Granadillos, N.; Zainal Farid, M.B.; et al. Overview of Legal Measures for Managing Workplace COVID-19 Infection Risk in Several Asia-Pacific Countries. Saf. Health Work 2021. [Google Scholar] [CrossRef] [PubMed]
- Guha, A.; Plzak, J.; Chovanec, M. Face to Face with COVID-19: Highlights of Challenges Encountered in Various ENT Practices across the Czech Republic (a National Survey). Eur. Arch. Otorhinolaryngol. 2021, 278, 807–812. [Google Scholar] [CrossRef] [PubMed]
- Glatter, K.A.; Finkelman, P. History of the Plague: An Ancient Pandemic for the Age of COVID-19. Am. J. Med. 2021, 134, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Prentice, M.B.; Rahalison, L. Plague. Lancet 2007, 369, 1196–1207. [Google Scholar] [CrossRef]
- Kugeler, K.J.; Staples, J.E.; Hinckley, A.F.; Gage, K.L.; Mead, P.S. Epidemiology of Human Plague in the United States, 1900–2012. Emerg. Infect. Dis. 2015, 21, 16–22. [Google Scholar] [CrossRef]
- Danforth, M.; Novak, M.; Petersen, J.; Mead, P.; Kingry, L.; Weinburke, M.; Buttke, D.; Hacker, G.; Tucker, J.; Niemela, M.; et al. Investigation of and Response to 2 Plague Cases, Yosemite National Park, California, USA, 2015. Emerg. Infect. Dis. 2016, 22, 2045–2053. [Google Scholar] [CrossRef] [Green Version]
- Guardian Staff Reporter. Teenage Boy Dies of Bubonic Plague in Mongolia after Eating Marmot. The Guardian, 15 July 2020. [Google Scholar]



{kind=link}
{kind=link}
| Type of Question | Options for Responses |
|---|---|
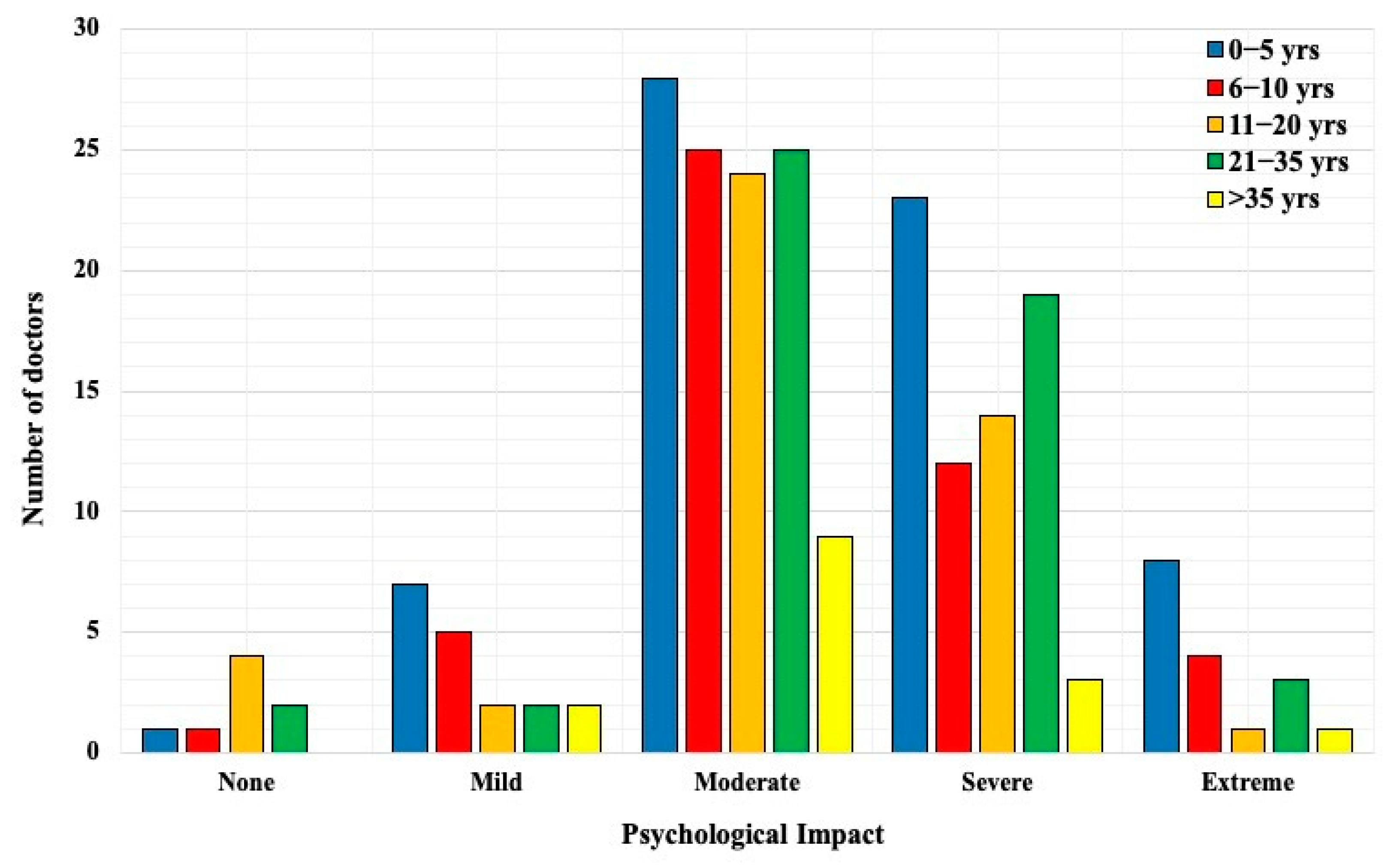
| How do you perceive the psychological impact of working in a COVID-19 unit? | 5—point Likert scale from None to Extreme |
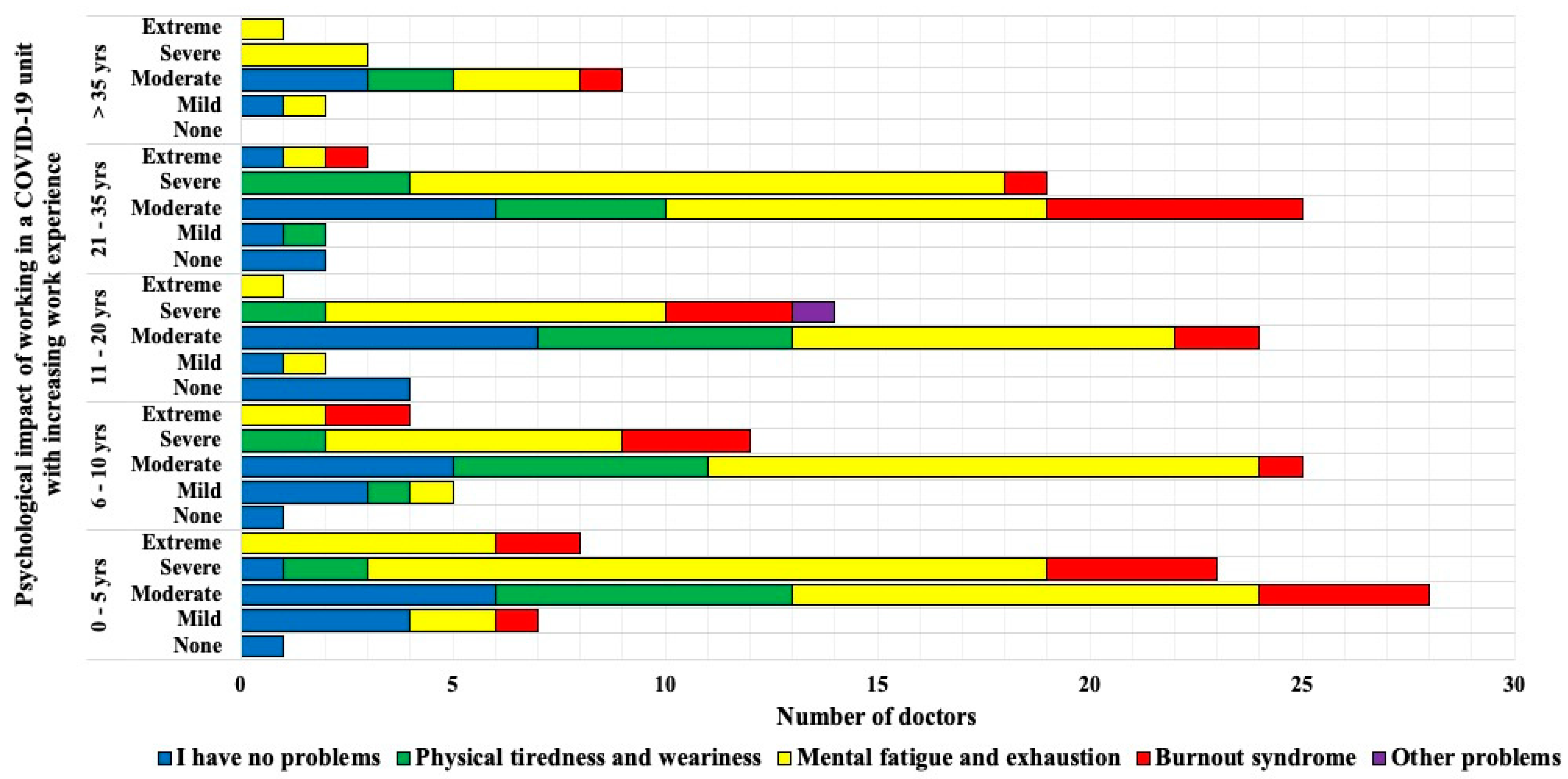
| Do you have any psychosomatic problems whilst working in the COVID-19 unit? | 5 options were available (select 1 option) □ No problems □ Physical tiredness and weariness □ Mental fatigue and exhaustion □ Burnout syndrome □ Other problems * If selected other problems, option to comment was available |
| Have you tested positive for SARS-CoV-2 antigen or were you quarantined whilst working in the COVID-19 unit? | □ Yes □ No * If selected ‘yes’, appropriate course of disease to be selected from 4 options (□ quarantined/not □ mild □ moderate □ severe) * If selected ‘no’, select if quarantined or not |
| What support is provided by employer If an employee contracts COVID-19 disease? | 5 options were available (select 1 option) □ unaware □ none □ medical □ financial □ medical + financial |
| What services should be provided by employers for employees working at a COVID-19 unit? | 5 options were available (select single best option) □ unaware □ psychological counselling □ medical □ financial □ all of the above |
| In your opinion, what strategies could help improve the situation with COVID-19 in Czech Republic? | 9 options were available (select as many as applicable) |
| Specialty | Gender | Severity | ||||
|---|---|---|---|---|---|---|
| None | Mild | Moderate | Severe | Extreme | ||
| Medical | Males | 2 | 6 | 27 | 13 | 2 |
| Females | 2 | 2 | 22 | 18 | 13 | |
| Surgical | Males | 4 | 8 | 40 | 22 | 1 |
| Females | 0 | 2 | 22 | 18 | 1 | |
| Specialty | Type of Support | ||||
|---|---|---|---|---|---|
| Unaware | Psychological Counselling | Medical | Financial | All Services | |
| Surgical | 6 | 8 | 6 | 14 | 84 |
| Medical | 6 | 13 | 0 | 9 | 79 |
| Option | Strategies in Reducing COVID-19 in Czech Republic | Respondents |
|---|---|---|
| 1 | Preventive measures in combination with vaccination | 196 |
| 2 | Private doctors should, if necessary, supplement hospital staff in order to maintain the efficient operation of hospitals in a pandemic situation | 80 |
| 3 | Nonadherence to lockdown rules & preventive measures resulting in imprisonment or penalty | 74 |
| 4 | Dividing Czech Republic into different categories of risk zones and enforcing lockdown and other measures accordingly | 61 |
| 5 | Stricter guidelines to general practitioners on referral of patients to hospitals | 60 |
| 6 | Utilizing telemedicine | 60 |
| 7 | Reinforcing travel restrictions and quarantine guidelines | 20 |
| 8 | All of the above | 13 |
| 9 | None of the above | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guha, A.; Schalek, P.; Chovanec, M.; Kraml, P.; Bala, J.; Plzak, J. Not Just a ‘Breath of Death’: Indirect Consequences of Working in a COVID-19 Unit. Int. J. Environ. Res. Public Health 2021, 18, 10802. https://doi.org/10.3390/ijerph182010802
Guha A, Schalek P, Chovanec M, Kraml P, Bala J, Plzak J. Not Just a ‘Breath of Death’: Indirect Consequences of Working in a COVID-19 Unit. International Journal of Environmental Research and Public Health. 2021; 18(20):10802. https://doi.org/10.3390/ijerph182010802
Chicago/Turabian StyleGuha, Anasuya, Petr Schalek, Martin Chovanec, Pavel Kraml, Jakub Bala, and Jan Plzak. 2021. "Not Just a ‘Breath of Death’: Indirect Consequences of Working in a COVID-19 Unit" International Journal of Environmental Research and Public Health 18, no. 20: 10802. https://doi.org/10.3390/ijerph182010802