Acute Effects of Global Postural Re-Education on Non-Specific Low Back Pain. Does Time-of-Day Play a Role?

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
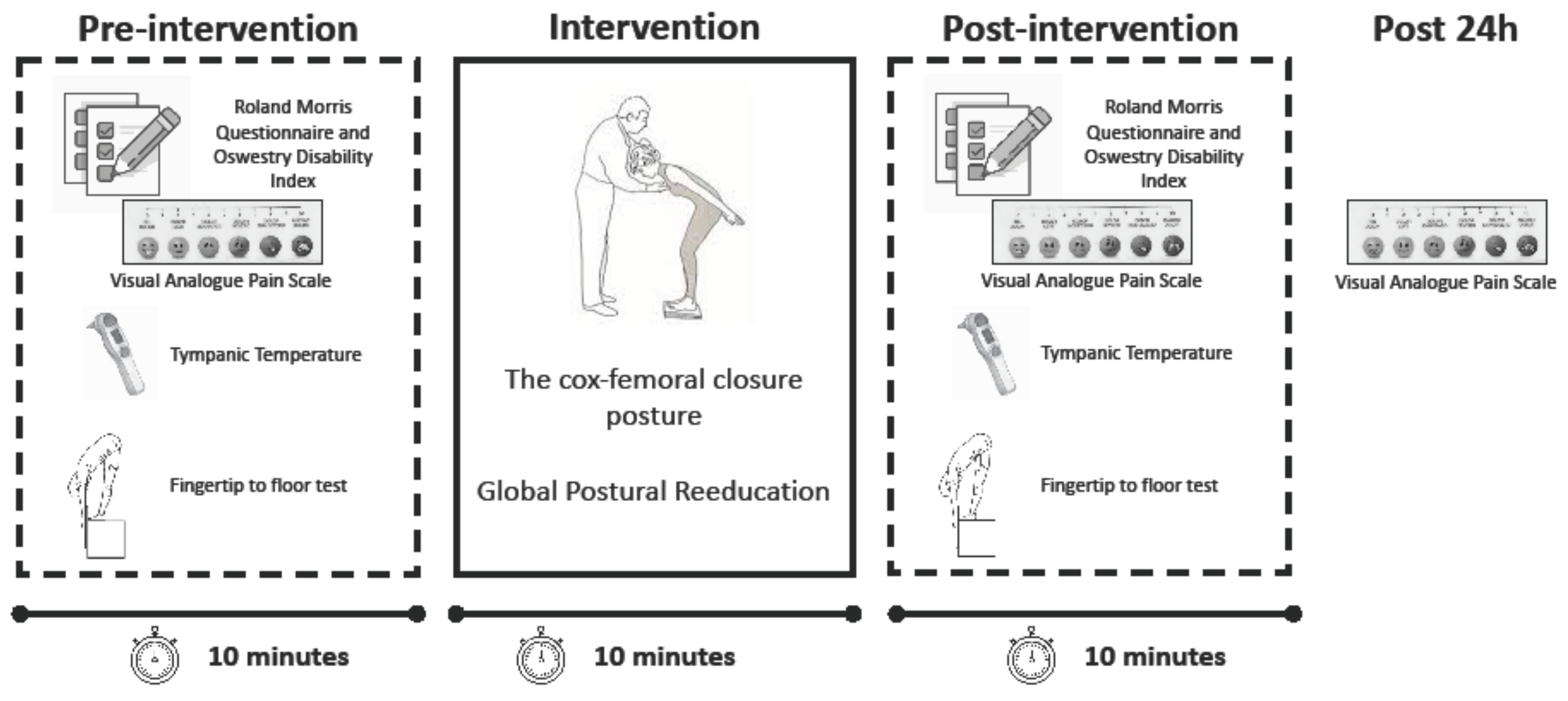
2.2. Study Design
2.3. Experimental Procedure
2.4. Fingertip to Floor Test
2.5. Visual Analogue Scale (VAS)
2.6. Roland Morris Questionnaire [RMQ] and Oswestry Disability Index (ODI)
2.7. Statistical Analysis
3. Results
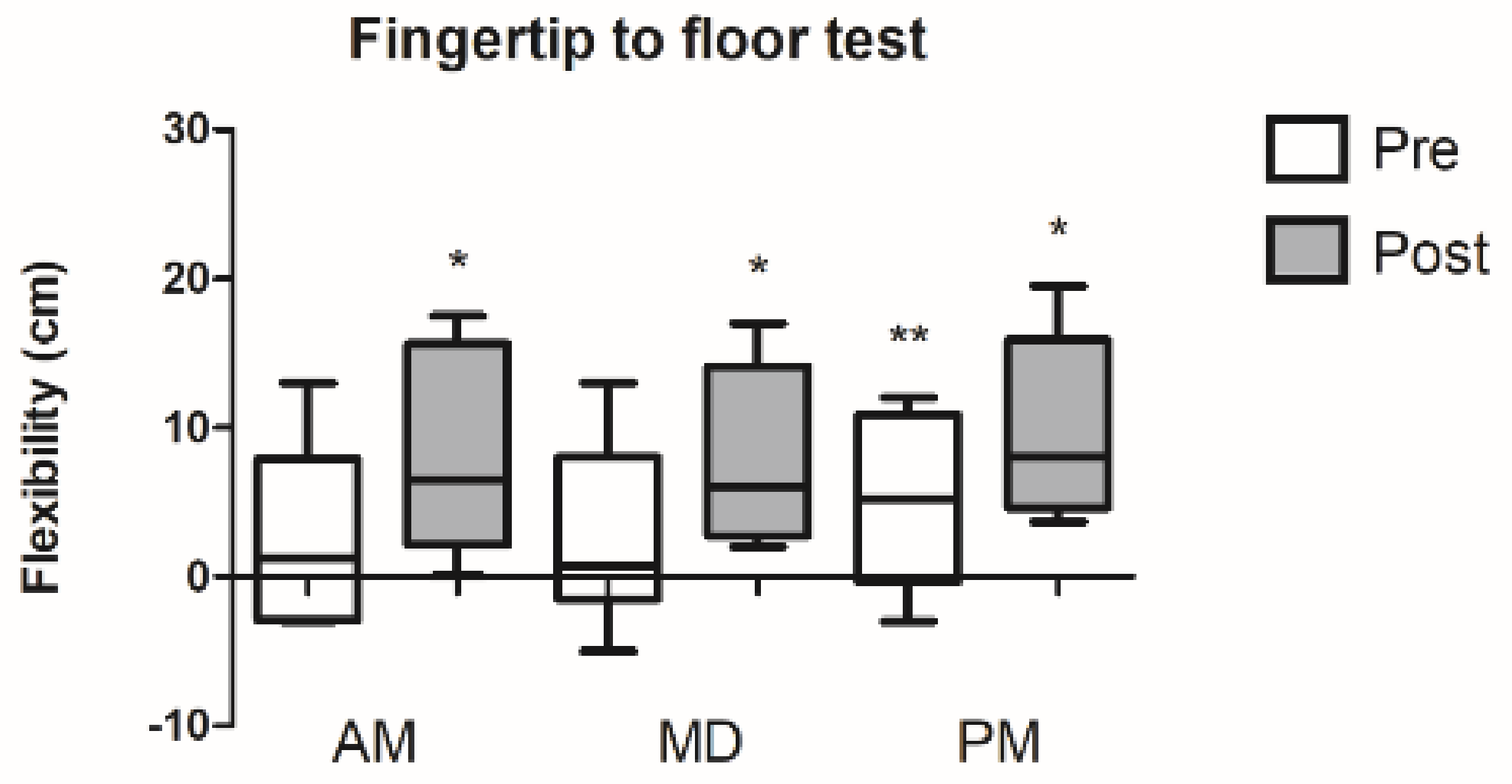
3.1. Fingertip to Floor Test
3.2. Low Back Pain
3.3. Roland Morris Questionnaire (RMQ) and Oswestry Disability Index (ODI)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Koes, B.W.; van Tulder, M.W.; Thomas, S. Diagnosis and treatment of low back pain. BMJ 2006, 332, 1430–1434. [Google Scholar] [CrossRef] [Green Version]
- Blyth, F.M.; Briggs, A.M.; Schneider, C.H.; Hoy, D.G.; March, L.M. The Global Burden of Musculoskeletal Pain-Where to From Here? Am. J. Public Health 2019, 109, 35–40. [Google Scholar] [CrossRef]
- Wong, A.Y.; Karppinen, J.; Samartzis, D. Low back pain in older adults: Risk factors, management options and future directions. Scoliosis Spinal Disord. 2017, 12, 14. [Google Scholar] [CrossRef]
- Andersson, G.B. Epidemiology of low back pain. Acta Orthop. Scand. 1998, 281, 28–31. [Google Scholar] [CrossRef] [Green Version]
- Miyamoto, G.C.; Lin, C.C.; Cabral, C.M.N.; van Dongen, J.M.; van Tulder, M.W. Cost-effectiveness of exercise therapy in the treatment of non-specific neck pain and low back pain: A systematic review with meta-analysis. Br. J. Sports Med. 2019, 53, 172–181. [Google Scholar] [CrossRef]
- Hoy, D.; March, L.; Woolf, A.; Blyth, F.; Brooks, P.; Smith, E.; Vos, T.; Barendregt, J.; Blore, J.; Murray, C.; et al. The global burden of neck pain: Estimates from the global burden of disease 2010 study. Ann. Rheum. Dis. 2014, 73, 1309–1315. [Google Scholar] [CrossRef]
- Longo, C.A.; Ferrari, S.; Lanza, A.; Vanti, C.; Stradiotti, P.; Ausenda, C.D. Effects of the standing posture with flexion of the trunk on the lumbar multifidus tropism in patients with chronic low back pain. A randomized, controlled pilot study study. Scienzia Riabilitativa 2016, 18, 5–12. [Google Scholar]
- Souchard, P. Rééducation Posturale Globale: RPG—La Méthode; Elsevier Masson: Paris, France, 2011. [Google Scholar]
- Matos, F.P.; Dantas, E.H.M.; de Oliveira, F.B.; de Castro, J.B.P.; Conceicao, M.; Nunes, R.A.M.; Vale, R.G.S. Analysis of pain symptoms, flexibility and hydroxyproline concentration in individuals with low back pain submitted to Global Postural Re-education and stretching. Pain Manag. 2020, 10, 167–177. [Google Scholar] [CrossRef]
- Lawand, P.; Lombardi Junior, I.; Jones, A.; Sardim, C.; Ribeiro, L.H.; Natour, J. Effect of a muscle stretching program using the global postural reeducation method for patients with chronic low back pain: A randomized controlled trial. Jt. Bone Spine 2015, 82, 272–277. [Google Scholar] [CrossRef]
- Cunha, A.C.; Burke, T.N.; Franca, F.J.; Marques, A.P. Effect of global posture reeducation and of static stretching on pain, range of motion, and quality of life in women with chronic neck pain: A randomized clinical trial. Clinics 2008, 63, 763–770. [Google Scholar] [CrossRef] [Green Version]
- Fozzatti, M.C.; Palma, P.; Herrmann, V.; Dambros, M. Impact of global postural reeducation for treatment of female stress urinary incontinence. Revista da Associacao Medica Brasileira 2008, 54, 17–22. [Google Scholar] [CrossRef] [Green Version]
- Fozzatti, C.; Herrmann, V.; Palma, T.; Riccetto, C.L.; Palma, P.C. Global Postural Re-education: An alternative approach for stress urinary incontinence? Eur. J. Obstet. Gynecol. Reprod. Biol. 2010, 152, 218–224. [Google Scholar] [CrossRef]
- Coksevim, N.H.; Durmus, D.; Kuru, O. Effects of global postural reeducation exercise and anti-TNF treatments on disease activity, function, fatigue, mobility, sleep quality and depression in patients with active Ankylosing spondylitis: A prospective follow-up study. J. Back Musculoskelet. Rehabil. 2018, 31, 1005–1012. [Google Scholar] [CrossRef] [PubMed]
- Fernandez-de-Las-Penas, C.; Alonso-Blanco, C.; Morales-Cabezas, M.; Miangolarra-Page, J.C. Two exercise interventions for the management of patients with ankylosing spondylitis: A randomized controlled trial. Am. J. Phys. Med. Rehabil. 2005, 84, 407–419. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Medina, G.; Perez-Cabezas, V.; Marin-Paz, A.J.; Galan-Mercant, A.; Ruiz-Molinero, C.; Jimenez-Rejano, J.J. Effectiveness of Global Postural Reeducation in Ankylosing Spondylitis: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2696. [Google Scholar] [CrossRef] [PubMed]
- Lomas-Vega, R.; Garrido-Jaut, M.V.; Rus, A.; Del-Pino-Casado, R. Effectiveness of Global Postural Re-education for Treatment of Spinal Disorders: A Meta-analysis. Am. J. Phys. Med. Rehabil. 2017, 96, 124–130. [Google Scholar] [CrossRef]
- Monteiro, W.; de Oliveira Dantas da Gama, T.F.; dos Santos, R.M.; Collange Grecco, L.A.; Pasini Neto, H.; Oliveira, C.S. Effectiveness of global postural reeducation in the treatment of temporomandibular disorder: Case report. J. Bodyw. Mov. Ther. 2013, 17, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Manzi, V.; Iellamo, F.; Alashram, A.R.; D’Onofrio, R.; Padua, E.; Casasco, M.; Annino, G. Effects of three different stretching protocols on hamstring muscle flexibility in professional soccer players: A randomized study. J. Sports Med. Phys. Fit. 2020, 60, 999–1004. [Google Scholar] [CrossRef]
- Reilly, T.; Waterhouse, J. Sports performance: Is there evidence that the body clock plays a role? Eur. J. Appl. Physiol. 2009, 106, 321–332. [Google Scholar] [CrossRef]
- Sujino, M.; Nagano, M.; Fujioka, A.; Shigeyoshi, Y.; Inouye, S.T. Temporal profile of circadian clock gene expression in a transplanted suprachiasmatic nucleus and peripheral tissues. Eur. J. Neurosci. 2007, 26, 2731–2738. [Google Scholar] [CrossRef]
- Schroder, E.A.; Esser, K.A. Circadian rhythms, skeletal muscle molecular clocks, and exercise. Exerc. Sport Sci. Rev. 2013, 41, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Yeung, C.C.; Schjerling, P.; Heinemeier, K.M.; Boesen, A.P.; Dideriksen, K.; Kjaer, M. Investigating circadian clock gene expression in human tendon biopsies from acute exercise and immobilization studies. Eur. J. Appl. Physiol. 2019, 119, 1387–1394. [Google Scholar] [CrossRef] [PubMed]
- Sherratt, M.J.; Hopkinson, L.; Naven, M.; Hibbert, S.A.; Ozols, M.; Eckersley, A.; Newton, V.L.; Bell, M.; Meng, Q.J. Circadian rhythms in skin and other elastic tissues. Matrix Biol. 2019, 84, 97–110. [Google Scholar] [CrossRef] [PubMed]
- Gifford, L.S. Circadian variation in human flexibility and grip strength. Aust. J. Physiother. 1987, 33, 3–9. [Google Scholar] [CrossRef] [Green Version]
- Portaluppi, F.; Smolensky, M.H.; Touitou, Y. Ethics and methods for biological rhythm research on animals and human beings. Chronobiol. Int. 2010, 27, 1911–1929. [Google Scholar] [CrossRef]
- Perret, C.; Poiraudeau, S.; Fermanian, J.; Colau, M.M.; Benhamou, M.A.; Revel, M. Validity, reliability, and responsiveness of the fingertip-to-floor test. Arch. Phys. Med. Rehabil. 2001, 82, 1566–1570. [Google Scholar] [CrossRef]
- Hayes, M.; Paterson, D. Experimental development of the graphic rating method. Psychol. Bull. 1921, 18, 98–99. [Google Scholar]
- Kovacs, F.M.; Llobera, J.; Gil Del Real, M.T.; Abraira, V.; Gestoso, M.; Fernandez, C.; Primaria Group, K.A. Validation of the spanish version of the Roland-Morris questionnaire. Spine 2002, 27, 538–542. [Google Scholar] [CrossRef] [Green Version]
- Roland, M.; Morris, R. A study of the natural history of back pain. Part I: Development of a reliable and sensitive measure of disability in low-back pain. Spine 1983, 8, 141–144. [Google Scholar] [CrossRef]
- Riddle, D.L.; Stratford, P.W. Roland-Morris scale reliability. Phys. Ther. 2002, 82, 512–515. [Google Scholar] [CrossRef]
- Lakens, D. Calculating and reporting effect sizes to facilitate cumulative science: A practical primer for t-tests and ANOVAs. Front. Psychol. 2013, 4, 863. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavalcanti, I.F.; Antonino, G.B.; Monte-Silva, K.K.D.; Guerino, M.R.; Ferreira, A.P.L.; das Gracas Rodrigues de Araujo, M. Global Postural Re-education in non-specific neck and low back pain treatment: A pilot study. J. Back Musculoskelet. Rehabil. 2020, 33, 823–828. [Google Scholar] [CrossRef]
- Cornwell, A.; Nelson, A.G.; Sidaway, B. Acute effects of stretching on the neuromechanical properties of the triceps surae muscle complex. Eur. J. Appl. Physiol. 2002, 86, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Bishop, D. Warm up I: Potential mechanisms and the effects of passive warm up on exercise performance. Sports Med. 2003, 33, 439–454. [Google Scholar] [CrossRef]
- Decostre, V.; Bianco, P.; Lombardi, V.; Piazzesi, G. Effect of temperature on the working stroke of muscle myosin. Proc. Natl. Acad. Sci. USA 2005, 102, 13927–13932. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starkie, R.L.; Hargreaves, M.; Lambert, D.L.; Proietto, J.; Febbraio, M.A. Effect of temperature on muscle metabolism during submaximal exercise in humans. Exp. Physiol. 1999, 84, 775–784. [Google Scholar] [CrossRef]
- Bonetti, F.; Curti, S.; Mattioli, S.; Mugnai, R.; Vanti, C.; Violante, F.S.; Pillastrini, P. Effectiveness of a “Global Postural Reeducation” program for persistent low back pain: A non-randomized controlled trial. BMC Musculoskelet. Disord. 2010, 11, 285. [Google Scholar] [CrossRef] [Green Version]
- Borges, B. Flexibilidade de atletas de basquetebol submetidos a postura em pe com inclinicao anterior do Método de Reeducao Postural Global. Revista Brasileira de Ciencia e Movimiento 2006, 14, 39–46. [Google Scholar]
- Castagnoli, C.; Cecchi, F.; Del Canto, A.; Paperini, A.; Boni, R.; Pasquini, G.; Vannetti, F.; Macchi, C. Effects in Short and Long Term of Global Postural Reeducation (GPR) on Chronic Low Back Pain: A Controlled Study with One-Year Follow-Up. Sci. World J. 2015, 2015, 271436. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Fingertip to Floor Test | RMQ | ODI |
|---|---|---|---|
| Morning (7:00–9:00) | |||
| Pre | 2.68 ± 6.01 | 3.50 ± 2.83 | 11.75 ± 5.39 |
| Post | 8.18 ± 7.12 | 3.88 ± 3.73 | 11.00 ± 7.17 |
| %Change | 75.40 ± 58.70 | 5.25 ± 11.73 | 7.13 ± 18.09 |
| ES | 0.83 | 0.11 | 0.12 |
| Midday (12:00–14:00) | |||
| Pre | 2.69 ± 5.96 | 4.50 ± 3.93 | 13.50 ± 6.99 |
| Post | 7.94 ± 5.84 | 4.38 ± 4.37 | 12.25 ± 7.67 |
| %Change | 39.30 ± 31.30 | 1.85 ± 3.71 | 11.03 ± 23.60 |
| ES | 0.88 | 0.03 | 0.17 |
| Afternoon (18:00–20:00) | |||
| Pre | 5.19 ± 5.78 | 3.75 ±4.13 | 10.00 ± 7.78 |
| Post | 9.90 ± 5.99 | 3.63 ± 4.03 | 10.25 ± 8.45 |
| %Change | 55.71 ± 57.05 | 1.48 ± 8.53 | 1.38 ± 3.09 |
| ES | 0.80 | 0.03 | 0.03 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Merinero, D.; Rodríguez-Aragón, M.; Álvarez-González, J.; López-Samanes, Á.; López-Pascual, J. Acute Effects of Global Postural Re-Education on Non-Specific Low Back Pain. Does Time-of-Day Play a Role? Int. J. Environ. Res. Public Health 2021, 18, 713. https://doi.org/10.3390/ijerph18020713
Merinero D, Rodríguez-Aragón M, Álvarez-González J, López-Samanes Á, López-Pascual J. Acute Effects of Global Postural Re-Education on Non-Specific Low Back Pain. Does Time-of-Day Play a Role? International Journal of Environmental Research and Public Health. 2021; 18(2):713. https://doi.org/10.3390/ijerph18020713
Chicago/Turabian StyleMerinero, David, Manuel Rodríguez-Aragón, Javier Álvarez-González, Álvaro López-Samanes, and Joaquín López-Pascual. 2021. "Acute Effects of Global Postural Re-Education on Non-Specific Low Back Pain. Does Time-of-Day Play a Role?" International Journal of Environmental Research and Public Health 18, no. 2: 713. https://doi.org/10.3390/ijerph18020713