Changes in the Levels of Stress Perception, Experiencing Depressive Symptoms and Health-Related Quality of Life of Residents after the 2016 Gyeongju Earthquake


Abstract
:1. Introduction
2. Materials and Methods
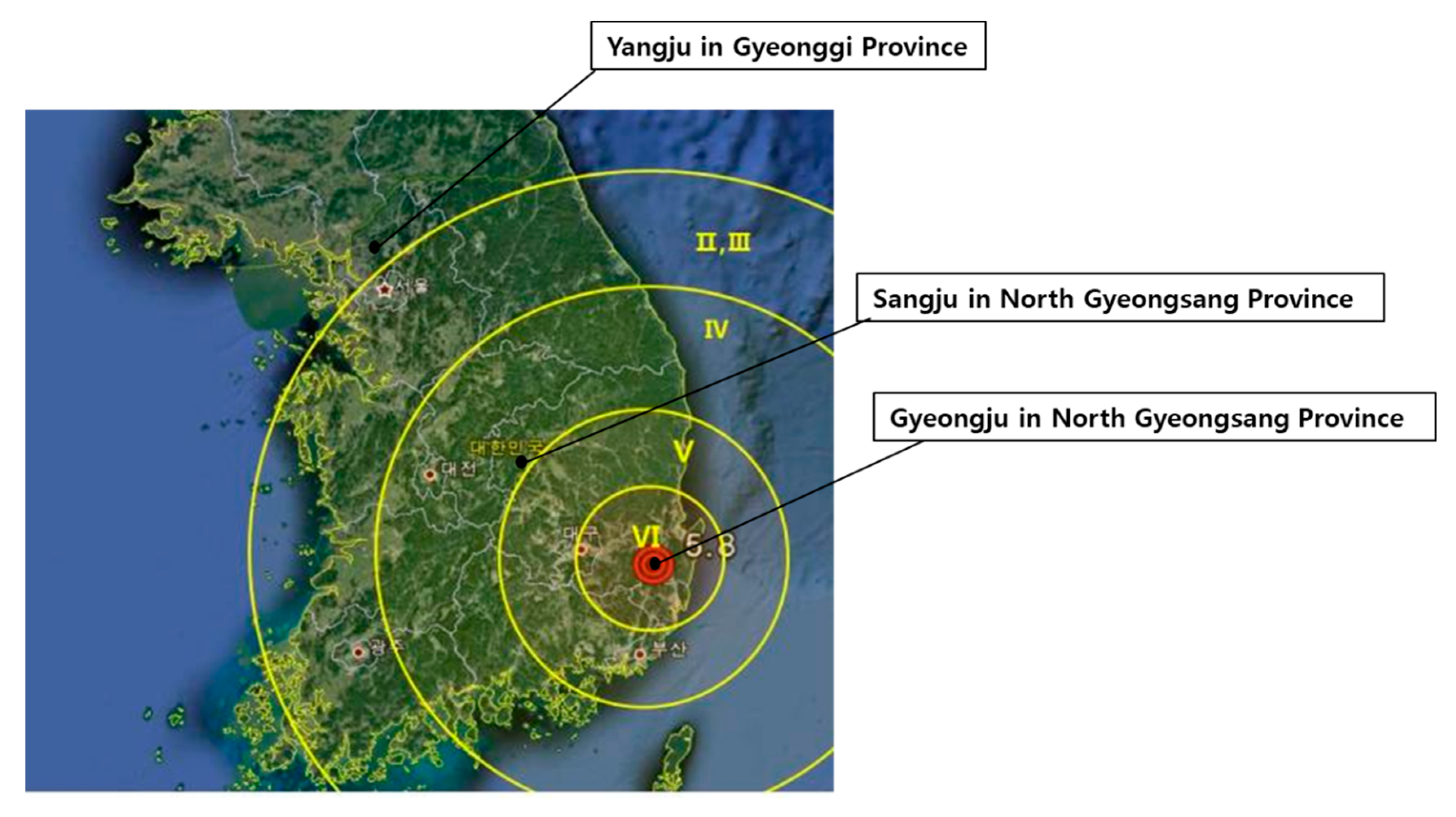
2.1. Study Population
2.2. Measurements
2.2.1. Stress Perception Rate
2.2.2. Rate of Experiencing Depressive Symptoms
2.2.3. Health-Related Quality of Life (HRQoL)
2.3. Statistical Analyses
3. Results
3.1. General Characteristics of the Subjects
3.2. The Change in Mental Health from 2015 to 2017 in Gyeongju and the Control Regions
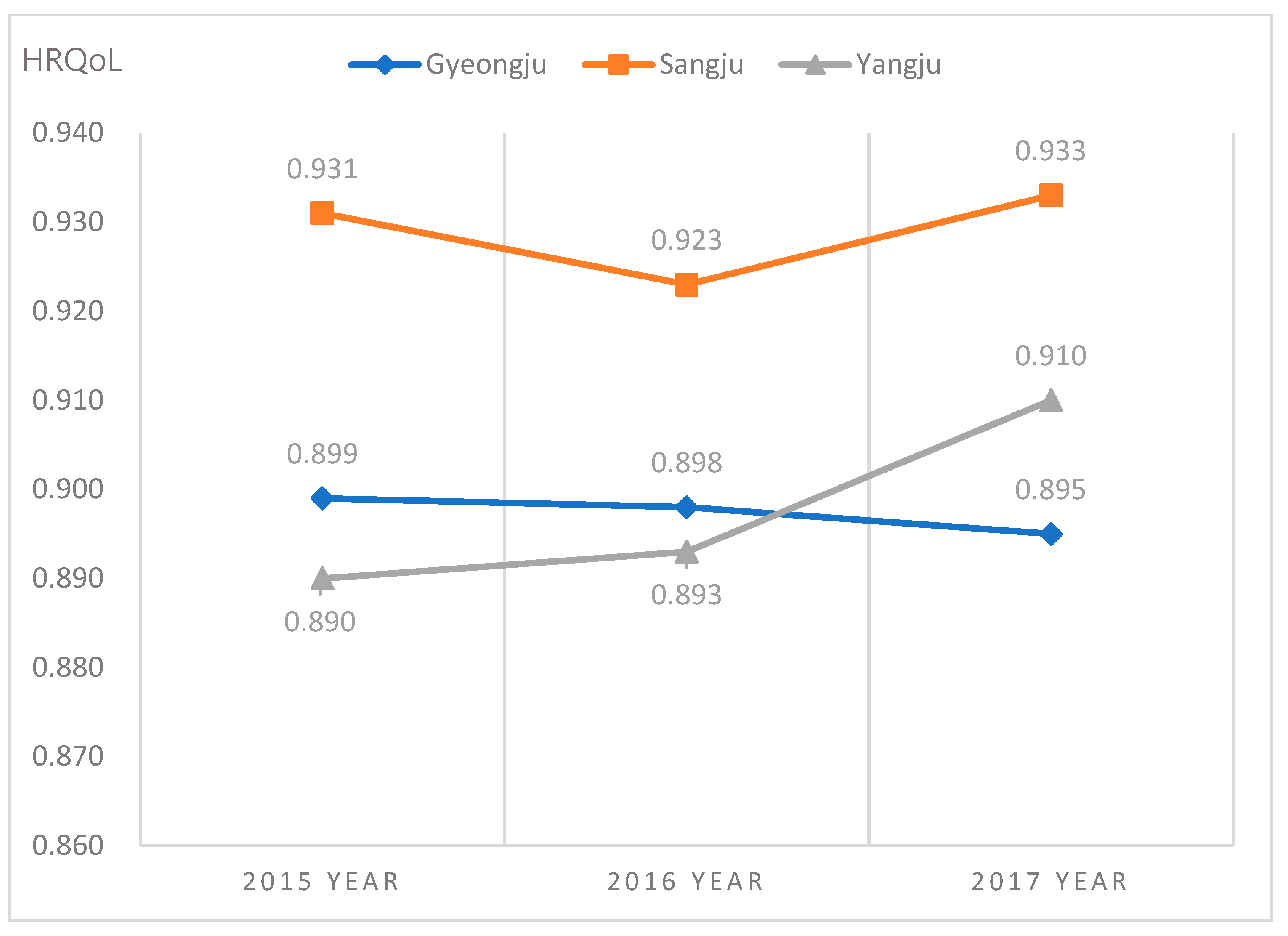
3.3. The Differences in HRQoL in Gyeongju and Control Regions from 2015 to 2017
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Choi, N.H.; Noh, J.K.; Son, Y.W.; Lee, J.E.; Ko, K.J.; Ko, B.Y.; Bea, J.L.; Yang, K.K.; Oh, S.S.; Lee, B.T.; et al. A Study on the Establishment of Support System for Psychological Support for Victims of Disaster; National Emergency Management Agency: Seoul, Korea, 2008; Report No.: 11-1660000-000120-14. [Google Scholar]
- Choi, N.H. Establishing the public support system for disaster survivors. Crisisonomy 2006, 2, 1–18. Available online: https://www.earticle.net/Article/A154198 (accessed on 14 November 2019).
- Choi, N.H.; Byun, J.H.; Han, D.G.; Im, S.B. Psychological impact and depressive response of sufferers of natural disaster, a torrential downpour. J. Korean Acad. Psychiatr. Ment. Health Nurs. 2007, 16, 139–149. [Google Scholar]
- Kang, Y.H. An analysis of psychological support of disaster victims of Jeju Special Self-Governing Province in terms of Typhoon “Nari”. Tamla Cult. 2011, 38, 279–307. [Google Scholar]
- Yoo, M.R.; Choi, S.Y.; Han, H.L.; Seo, Y.M.; Noh, M.I. The effect of post-traumatic growth, resilience, and optimism on quality of life among the disaster victims. J. Mil. Nurs. Res. 2015, 33, 1–14. [Google Scholar]
- Hyun, Y.J.; Park, J.K.; Lee, Y.J.; Lee, J.H.; Lee, M.J.; Park, J.K.; Lee, B.S.; Lee, S.T.; Lee, T.K.; Lee, H.D.; et al. Environmental Impact of Earthquakes and Directions of Responses; Report No.: 2017-01; Korea Environment Institute: Sejong, Korea, 2017. [Google Scholar]
- Lee, K.Y.; Lee, Y.J.; Kim, K.M. An analysis of factors influencing life satisfaction of Gyeongju residents who experienced an earthquake: Focused on disaster-related awareness and experience. Korean J. Soc. Welf. Res. 2017, 54, 83–110. Available online: http://kiss.kstudy.com/thesis/thesis-view.asp?key=3548496 (accessed on 16 November 2019). [CrossRef]
- Fink, G. Chapter 1—Stress, Definitions, Mechanisms, and Effects Outlined: Lessons from Anxiety. In Stress: Concepts, Cognition, Emotion, and Behavior; Fink, G., Ed.; Academic Press: San Diego, CA, USA, 2016; pp. 3–11. [Google Scholar] [CrossRef]
- Foa, E.B.; Stein, D.J.; McFarlane, A.C. Symptomatology and psychopathology of mental health problems after disaster. J. Clin. Psychiatry 2006, 67, 15–25. [Google Scholar]
- Hussain, A.; Weisaeth, L.; Heir, T. Psychiatric disorders and functional impairment among disaster victims after exposure to a natural disaster: A population based study. J. Affect. Disord. 2011, 128, 135–141. [Google Scholar] [CrossRef]
- Li, X.; Aida, J.; Hikichi, H.; Kondo, K.; Kawachi, I. Association of Postdisaster Depression and Posttraumatic Stress Disorder With Mortality Among Older Disaster Survivors of the 2011 Great East Japan Earthquake and Tsunami. JAMA Net. Open 2019, 2, e1917550. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Horwood, L.J.; Boden, J.M.; Mulder, R.T. Impact of a Major Disaster on the Mental Health of a Well-Studied Cohort. JAMA Psychiatry 2014, 71, 1025–1031. [Google Scholar] [CrossRef] [Green Version]
- Fan, F.; Zhang, Y.; Yang, Y.; Mo, L.; Liu, X. Symptoms of posttraumatic stress disorder, depression, and anxiety among adolescents following the 2008 Wenchuan earthquake in China. J. Trauma Stress 2011, 24, 44–53. [Google Scholar] [CrossRef]
- OECD. Health at a Glance 2019: OECD Indicators; OECD Publishing: Paris, France, 2019. [Google Scholar] [CrossRef]
- Kim, G.E.; Jo, M.W.; Shin, Y.W. Increased prevalence of depression in South Korea from 2002 to 2013. Sci. Rep. 2020, 10, 16979. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.C. 9.12 Earthquake Response Report, 1st ed.; Korea Meteorological Administration: Seoul, Korea, 2017. [Google Scholar]
- Korean National Commission for UNESCO. Cultural Heritage in Korea. Available online: https://unesco.or.kr/etc/search/%ED%95%9C%EA%B5%AD%EC%9D%98%20%EB%AC%B8%ED%99%94%EC%9C%A0%EC%82%B0/ (accessed on 25 December 2020).
- Korea Center for Disease Control & Prevention. 2008–2019 Community Health Survey: See at a Glance; Korea Center for Disease Control & Prevention: Osong-eup, Korea, 2020. [Google Scholar]
- Statistics Korea. Resident Registered Population Status: Population by Administrative District; Ministry of the Interior and Security. Statistics Korea: Deajeon, Korea, 2020.
- Gyeongju City Hall. About Gyeongju. Available online: https://www.gyeongju.go.kr/open_content/ko/page.do?mnu_uid=296& (accessed on 25 December 2020).
- Sangju City Hall. History of Sangju: Modern Age. Available online: https://www.sangju.go.kr/eng/page/3674/1785.tc?protocol=http (accessed on 25 December 2020).
- Yangju City Hall. About Yangju: Regional Characteristics. Available online: https://www.yangju.go.kr/www/contents.do?key=320 (accessed on 25 December 2020).
- Sangju City Hall. About Sangju: Regional Characteristics. Available online: https://www.sangju.go.kr (accessed on 25 December 2020).
- Statistics Korea. 2017 Population and Housing Census; Statistics Korea: Deajeon, Korea, 2018.
- Korea Centers for Disease Control and Prevention. 2019 Community Health Survey; Korea Centers for Disease Control and Prevention: Osong-eup, Korea, 2019.
- Lee, O.C. Trends of nursing research on disasters in Korea. J. Korean Public Health Nurs. 2014, 28, 432–444. [Google Scholar] [CrossRef] [Green Version]
- Kwon, Y.S. Daily Life Experience of Natural Disaster Victims: Focused on the Gyeongju Earthquake. Ph.D. Thesis, HanYang University, Seoul, Korea, 2018. [Google Scholar]
- Choi, S.Y. A Structural Equation Model for Quality of Life of Adults who Experienced Natural Disaster: Focused on Kyeongju and Pohang Earthquakes in South Korea. Doctoral Dissertation, Yeonsei University, Seoul, Korea, 2018. [Google Scholar]
- Zhang, W.Q.; Liu, C.; Sun, T.S.; Zhao, J.; Han, J.Q.; Yang, Y.H.; Li, S.J.; Ma, Y.Q. Physical and mental health status of soldiers responding to the 2008 Wenchuan earthquake. Aust. N. Z. J. Public Health 2011, 35, 207–211. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.; Lee, E.; Choi, J.W.; Kim, H.J. PTSD and related factors among dispatched firefighters to rescue sites after the great Japanese earthquake. Korean J. Occup. Environ. Med. 2012, 24, 167–179. [Google Scholar] [CrossRef]
- Montazeri, A.; Baradaran, H.; Omidvari, S.; Azin, S.A.; Ebadi, M.; Garmaroudi, G.; Harirchi, A.M.; Shariati, M. Psychological distress among Bam earthquake survivors in Iran: A population-based study. BMC Public Health 2005, 5, 4. [Google Scholar] [CrossRef] [Green Version]
- Person, C.; Tracy, M.; Galea, S. Risk Factors for Depression after a Disaster. J. Nerv. Ment. Dis. 2006, 194, 659–666. [Google Scholar] [CrossRef]
- Guo, J.; Wu, P.; Tian, D.; Wang, X.; Zhang, W.; Zhang, X.; Qu, Z. Post-traumatic Stress Disorder among adult survivors of the Wenchuan Earthquake in China: A repeated cross-sectional study. J. Anxiety Disord. 2014, 28, 75–82. [Google Scholar] [CrossRef]
- Tsukinoki, R.; Murakami, Y.; Kawado, M.; Hashimoto, S. Comparison of standardised mortality ratios for renal failure before and after the 2011 Great East Japan Earthquake and Tsunami: An analysis of national vital statistics. BMJ Open 2018, 8, e023435. [Google Scholar] [CrossRef] [Green Version]
- Tashiro, A.; Sakisaka, K.; Okamoto, E.; Yoshida, H. Differences in infant and child mortality before and after the Great East Japan Earthquake and Tsunami: A large population-based ecological study. BMJ Open 2018, 8, e022737. [Google Scholar] [CrossRef]
- Boo, S.; FROELICHER, E.S. Secondary analysis of national survey datasets. Jpn. J. Nurs. Sci. 2013, 10, 130–135. [Google Scholar] [CrossRef]
- Ministry of Government Legislation. Ministry of Government Legislation. Regional Public Health Act. Sejong-si, South Korea. 2019. Available online: http://www.moleg.go.kr/main.html (accessed on 28 October 2019).
- The EuroQol Group. EuroQol—A new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [Google Scholar] [CrossRef]
- Lee, Y.K.; Nam, H.S.; Chuang, L.H.; Kim, K.Y.; Yang, H.K.; Kwon, I.S.; MPhil, P.K.; Kweon, S.S.; Kim, Y.T. South Korean Time Trade-Off Values for EQ-5D Health States: Modeling with Observed Values for 101 Health States. Value Health 2009, 12, 1187–1193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.H.; Cho, Y.S.; Uhm, W.S.; Kim, S.; Bae, S.-C. Cross-cultural adaptation and validation of the Korean version of the EQ-5D in patients with rheumatic diseases. Qual. Life Res. 2005, 14, 1401–1406. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.W.; Han, Y.R.; Kim, S.K.; Jeong, H.S. The frequency of impairments in everyday activities due to the overuse of the internet, gaming, or smartphone, and its relationship to health-related quality of life in Korea. BMC Public Health 2020, 20, 954. [Google Scholar] [CrossRef]
- Aslam, N.; Tariq, N. Trauma, depression, anxiety, and stress among individuals living in earthquake affected and unaffected areas. Pak. J. Psychol. Res. 2010, 131–148. Available online: http://www.pjprnip.edu.pk/pjpr/index.php/pjpr/article/view/52 (accessed on 14 December 2019).
- Nygaard, E.; Heir, T. World assumptions, posttraumatic stress and quality of life after a natural disaster: A longitudinal study. Health Qual. Life Outcomes 2012, 10, 76. [Google Scholar] [CrossRef] [Green Version]
- Yang, H.J.; Cheong, H.K.; Choi, B.Y.; Shin, M.-H.; Yim, H.W.; Kim, D.-H.; Kim, G.; Lee, S.Y. Community mental health status six months after the Sewol ferry disaster in Ansan, Korea. Epidemiol. Health 2015, 37, e2015046. [Google Scholar] [CrossRef] [Green Version]
- Tracy, M.; Norris, F.H.; Galea, S. Differences in the determinants of posttraumatic stress disorder and depression after a mass traumatic event. Depress. Anxiet. 2011, 28, 666–675. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Gao, L.; Zhang, H.; Zhao, C.; Shen, Y.; Shinfuku, N. Post-earthquake quality of life and psychological well-being: Longitudinal evaluation in a rural community sample in northern China. Psychiatry Clin. Neurosci. 2000, 54, 427–433. [Google Scholar] [CrossRef]
- Rodda, J.; Walker, Z.; Carter, J. Depression in older adults. BMJ 2011, 343, d5219. [Google Scholar] [CrossRef]
- Ceyhan, E.; Ceyhan, A.A. Earthquake survivors’ quality of life and academic achievement six years after the earthquakes in Marmara, Turkey. Disasters 2007, 31, 516–529. [Google Scholar] [CrossRef]
- Wen, J.; Shi, Y.K.; Li, Y.P.; Yuan, P.; Wang, F. Quality of life, physical diseases, and psychological impairment among survivors 3 years after Wenchuan earthquake: A population based survey. PLoS ONE 2012, 7, e43081. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ardalan, A.; Mazaheri, M.; Vanrooyen, M.; Mowafi, H.; Nedjat, S.; Naieni, K.H.; Russel, M. Post-disaster quality of life among older survivors five years after the Bam earthquake: Implications for recovery policy. Ageing Soc. 2011, 32, 179–196. [Google Scholar] [CrossRef]
- Choung, Y.C.; Choy, I.S.; Bae, Y.G. Social security aimed disaster response policy based on Big Data application. J. Korea Inst. Inf. Commun. Eng. 2016, 20, 683–690. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | Characteristics | Gyeongju | Sangju | Yangju | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | 2015 | 2016 | 2017 | 2015 | 2016 | 2017 | ||
| Total 903 | 896 | 898 | 897 | 900 | 891 | 912 | 909 | 896 | ||
| n (% *) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||
| Age (years) | 19–44 | 270 (38.8) | 277 (37.8) | 248 (35.6) | 199 (29.7) | 197 (29.1) | 190 (29.5) | 382 (46.4) | 364 (45) | 303 (44) |
| 45–64 | 376 (40.1) | 265 (39.1) | 339 (38.7) | 344 (39.1) | 361 (39.1) | 347 (38.4) | 332 (36.6) | 344 (37.9) | 345 (38.6) | |
| 65– | 25 7(21.1) | 254 (23.1) | 311 (25.7) | 354 (31.2) | 342 (31.8) | 354 (32.1) | 198 (17) | 201 (17.1) | 248 (17.4) | |
| Sex | Male | 397 (49.6) | 396 (49.6) | 385 (49.8) | 390 (48.3) | 409 (48.3) | 401 (48.4) | 417 (50.7) | 405 (50.6) | 410 (50.8) |
| Female | 506 (50.4) | 500 (50.6) | 513 (50.2) | 507 (51.7) | 491 (51.7) | 490 (51.6) | 495 (49.3) | 504 (49.4) | 486 (49.2) | |
| Marital status | Married | 632 (67.7) | 621 (67) | 649 (70.3) | 598 (66.8) | 632 (68.5) | 611 (67.1) | 639 (68.5) | 613 (67.2) | 621 (67.4) |
| Unmarried | 107 (17.5) | 118 (18.1) | 99 (17.4) | 106 (15.4) | 113 (16.9) | 102 (15.6) | 132 (17.9) | 158 (18.9) | 139 (22) | |
| Other | 163 (14.8) | 156 (14.9) | 150 (12.3) | 193 (17.9) | 155 (14.6) | 178 (17.3) | 141 (13.6) | 138 (13.9) | 136 (10.6) | |
| Education level | Below elementary school | 48 (20.3) | 219 (20.2) | 250 (20.6) | 358 (31.8) | 310 (27.9) | 354 (33) | 153 (13.9) | 182 (16.4) | 149 (10.5) |
| Middle school | 113 (11.1) | 98 (9.5) | 100 (10) | 120 (12.1) | 139 (13.9) | 120 (12.3) | 112 (11.4) | 109 (10.6) | 108 (9.8) | |
| High school | 281 (35.4) | 306 (38) | 282 (35.7) | 233 (29.2) | 259 (31.9) | 244 (30.3) | 365 (41.8) | 373 (42.8) | 381 (46.3) | |
| Above university | 257 (33.2) | 268 (32.3) | 266 (33.7) | 186 (26.8) | 192 (26.3) | 173 (24.5) | 282 (32.8) | 245 (30.1) | 258 (33.5) | |
| Occupations | Yes | 533 (61.9) | 516 (61.2) | 488 (58.7) | 645 (72.4) | 649 (72.6) | 636 (72.1) | 579 (65.8) | 576 (65.6) | 579 (68.7) |
| No | 366 (38.1) | 375 (38.8) | 410 (41.3) | 252 (27.6) | 251 (27.4) | 255 (27.9) | 333 (34.2) | 333 (34.4) | 317 (31.3) | |
| Perceived health status | Good | 258 (31.8) | 235 (28) | 265 (33.3) | 311 (37.8) | 288 (36.4) | 299 (36.9) | 353 (41.1) | 417 (46.1) | 327 (40.2) |
| Average | 417 (47.7) | 452 (51.5) | 401 (45.4) | 352 (39.6) | 393 (43) | 340 (39.6) | 373 (41.2) | 326 (37.1) | 372 (42.7) | |
| Not good | 224 (20.5) | 204 (20.5) | 232 (21.3) | 234 (22.6) | 219 (20.5) | 252 (23.5) | 186 (17.7) | 166 (16.8) | 197 (17.1) | |
| Year | Stress | 2015 a | 2016 b | 2017 c | χ2 (p 2) | |
|---|---|---|---|---|---|---|
| Area | n (%) 1 | n (%) | n (%) | Post-hoc 3 | ||
| Gyeongju | Yes | 208 (23.3) | 199 (22.2) | 226 (26.3) | 3.48 (0.031) | |
| No | 695 (76.7) | 697 (77.8) | 672 (73.7) | b < c | ||
| Sangju | Yes | 184 (21.4) | 151 (17.1) | 116 (13.7) | 9.84 (0.001) | |
| No | 713 (78.6) | 750 (82.9) | 775 (86.3) | c < b < a | ||
| Yangju | Yes | 307 (33.8) | 244 (28.6) | 238 (24.8) | 8.37 (0.001) | |
| No | 609 (66.2) | 665 (71.4) | 671 (75.2) | b, c < a | ||
| Year | Depression | 2015 a | 2016 b | 2017 c | χ2 (p 2) | |
|---|---|---|---|---|---|---|
| Area | n (%) 1 | n (%) | n (%) | Post-hoc 3 | ||
| Gyeongju | Yes | 126 (12.9) | 101 (10.3) | 73 (8.1) | 5.41 (0.005) | |
| No | 777 (87.1) | 795 (89.7) | 825 (91.9) | c < a | ||
| Sangju | Yes | 53 (4.9) | 27 (2.7) | 11 (1.1) | 11.58 (0.001) | |
| No | 844 (95.1) | 874 (97.3) | 880 (98.9) | b, c < a | ||
| Yangju | Yes | 56 (5.8) | 65 (7) | 46 (4.7) | 1.96 (0.142) | |
| No | 860 (94.2) | 844 (93) | 863 (95.3) | |||
| EQ-5D-3L | Gyeongju | Sangju | Yangju | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2015 | 2016 | 2017 | χ2 or F(p 2) | 2015 | 2016 | 2017 | χ2 or F(p) | 2015 a | 2016 b | 2017 c | χ2 or F(p) | |
| n (%1) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | n (%) | ||||
| M ± SD | 0.899 ± 0.00 | 0.898 ± 0.00 | 0.895 ± 0.00 | 0.18 (0.837) | 0.931 ± 0.00 | 0.923 ± 0.00 | 0.933 ± 0.00 | 2.87 (0.057) | 0.890 ± 0.00 | 0.893 ±0.00 | 0.910 ± 0.00 | 12.26 (0.001) a, b < c |
| Mobility | ||||||||||||
| No | 710 (78.63) | 705 (78.68) | 708 (78.84) | 2.858 (0.582) | 746 (83.17) | 737 (81.80) | 747 (83.84) | 2.850 (0.583) | 785 (85.70) | 762 (83.83) | 784 (86.25) | 8.670 (0.070) |
| Some | 185 (20.49) | 183 (20.42) | 182 (20.27) | 149 (16.61) | 160 (17.76) | 142 (15.94) | 125 (13.65) | 141 (15.51) | 121 (123.31) | |||
| Extreme | 8 (0.89) | 8 (0.89) | 8 (0.89) | 2 (0.22) | 4 (0.44) | 2 (0.22) | 6 (0.66) | 6 (0.66) | 4 (0.44) | |||
| Self-care | ||||||||||||
| No | 813 (90.03) | 833 (92.97) | 827 (92.09) | 6.362 (0.173) | 859 (95.76) | 856 (95.01) | 860 (96.52) | 3.714 (0.928) | 868 (94.76) | 850 (93.51) | 872 (95.93) | 12.387 (0.014) |
| Some | 82 (9.08) | 60 (6.70) | 62 (6.90) | 35 (3.90) | 40 (4.44) | 28 (3.14) | 45 (4.91) | 52 (5.72) | 31 (3.41) | |||
| Extreme | 8 (0.89) | 3 (0.33) | 9 (1.00) | 3 (0.33) | 5 (0.55) | 3 (0.34) | 3 (0.33) | 7 (0.77) | 6 (0.66) | |||
| Usual activities | ||||||||||||
| No | 742 (82.17) | 744 (83.04) | 730 (81.29) | 2.168 (0.704) | 792 (88.29) | 780 (86.57) | 798 (89.56) | 7.000 (0.135) | 807 (88.10) | 790 (86.91) | 823 (90.54) | 9.465 (0.050) |
| Some | 151 (16.72) | 137 (15.29) | 156 (17.37) | 100 (11.15) | 115 (12.76) | 84 (9.43) | 104 (11.35) | 110 (12.10) | 80 (8.80) | |||
| Extreme | 10 (1.11) | 15 (16.67) | 12 (1.34) | 5 (0.56) | 6 (0.67) | 9 (1.01) | 5 (0.55) | 9 (0.99) | 6 (0.66) | |||
| Pain or discomfort | ||||||||||||
| No | 615 (68.11) | 625 (69.75) | 521 (58.02) | 18.165 (0.001) | 673 (75.03) | 65 8(73.03) | 629 (70.59) | 6.230 (0.182) | 584 (63.76) | 644 (70.85) | 669 (73.60) | 41.472 (<0.000) |
| Some | 251 (27.80) | 237 (26.45) | 342 (38.08) | 216 (24.08) | 223 (24.75) | 245 (27.50) | 298 (32.53) | 228 (28.08) | 231 (25.41) | |||
| Extreme | 37 (4.10) | 34 (3.79) | 35 (3.90) | 8 (0.89) | 20 (2.22) | 17 (1.91) | 34 (3.71) | 37 (4.07) | 9 (0.99) | |||
| Anxiety or depression | ||||||||||||
| No | 763 (84.50) | 761 (84.93) | 712 (79.29) | 10.697 (0.030) | 824 (91.86) | 828 (91.90) | 827 (92.82) | 1.693 (0.792) | 719 (78.49) | 783 (86.14) | 802 (88.23) | 26.891 (<0.000) |
| Some | 127 (14.06) | 123 (13.73) | 177 (19.71) | 68 (7.58) | 68 (7.55) | 62 (6.96) | 190 (20.74) | 117 (12.87) | 99 (10.89) | |||
| Extreme | 13 (1.44) | 12 (1.34) | 9 (1.00) | 5 (0.56) | 5 (0.55) | 2 (0.22) | 7 (0.76) | 9 (0.99) | 8 (0.88) | |||
| Variables | Sum of Squares | Degrees of Freedom | Mean Square | F | p1 |
|---|---|---|---|---|---|
| Regions | 0.730 | 2 | 0.365 | 26.07 | <0.0001 |
| Years | 0.057 | 2 | 0.028 | 2.02 | 0.1323 |
| Regions × Years | 0.273 | 4 | 0.068 | 4.87 | 0.0006 |
| Error | 113.560 | 8111 | 0.014 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, Y.R.; Jeong, Y.W.; Kim, S.K.; Jeong, H.S. Changes in the Levels of Stress Perception, Experiencing Depressive Symptoms and Health-Related Quality of Life of Residents after the 2016 Gyeongju Earthquake. Int. J. Environ. Res. Public Health 2021, 18, 540. https://doi.org/10.3390/ijerph18020540
Han YR, Jeong YW, Kim SK, Jeong HS. Changes in the Levels of Stress Perception, Experiencing Depressive Symptoms and Health-Related Quality of Life of Residents after the 2016 Gyeongju Earthquake. International Journal of Environmental Research and Public Health. 2021; 18(2):540. https://doi.org/10.3390/ijerph18020540
Chicago/Turabian StyleHan, Young Ran, Yeo Won Jeong, Sang Kyu Kim, and Han Seok Jeong. 2021. "Changes in the Levels of Stress Perception, Experiencing Depressive Symptoms and Health-Related Quality of Life of Residents after the 2016 Gyeongju Earthquake" International Journal of Environmental Research and Public Health 18, no. 2: 540. https://doi.org/10.3390/ijerph18020540