
Assessment of SARS-CoV-2 Anti-Spike IgG Antibody in Women and Children in Madinah, Saudi Arabia: A Single-Center Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample Collection
2.2. Assessment of Outcome: SARS-CoV-2 Anti-Spike IgG Antibody Detection
2.3. Enzyme-Linked Immunosorbent Assay (ELISA)
2.4. Assessment of Predictors: Age, Sex, Blood Group, and Weight Status
2.5. Statistical Analysis
3. Results
3.1. General Characteristics
3.2. Prevalence of Anti-S IgG Antibody to SARS-CoV-2 among Participants
3.3. Association between SARS-CoV-2 Serological Status and the Characteristics of Participants
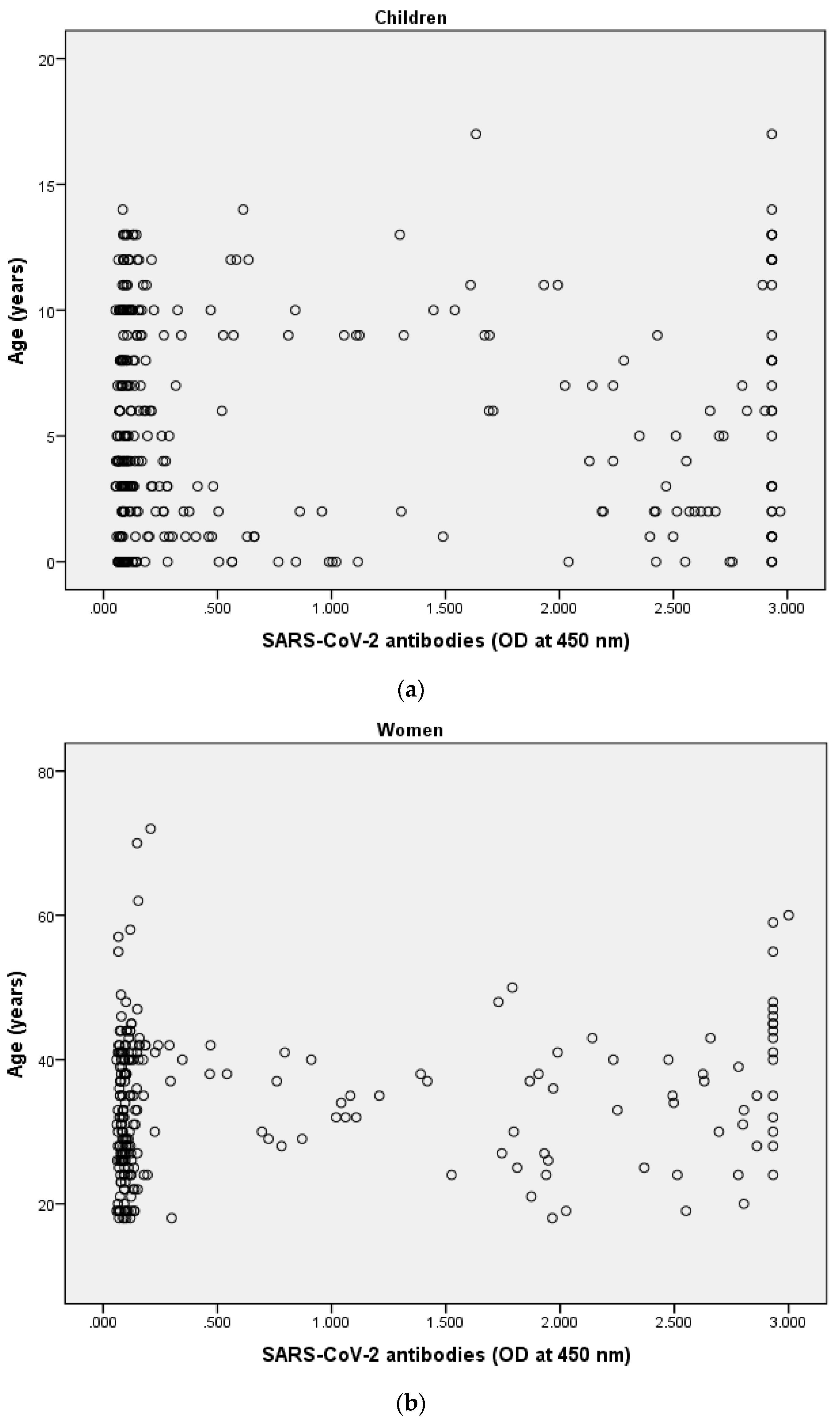
3.4. Correlation between SARS-CoV-2 Anti-S IgG Antibody and Age
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Lai, C.-C.; Wang, J.-H.; Hsueh, P.-R. Population-based seroprevalence surveys of anti-SARS-CoV-2 antibody: An up-to-date review. Int. J. Infect. Dis. 2020, 101, 314–322. [Google Scholar] [CrossRef]
- Al-Khani, A.M.; Khalifa, M.A.; Almazrou, A.; Saquib, N. The SARS-CoV-2 pandemic course in Saudi Arabia: A dynamic epidemiological model. Infect. Dis. Model. 2020, 5, 766–771. [Google Scholar] [CrossRef]
- Arevalo-Rodriguez, I.; Buitrago-Garcia, D.; Simancas-Racines, D.; Zambrano-Achig, P.; Del Campo, R.; Ciapponi, A.; Sued, O.; Martinez-García, L.; Rutjes, A.W.; Low, N.; et al. False-negative results of initial RT-PCR assays for COVID-19: A systematic review. PLoS ONE 2020, 15, e0242958. [Google Scholar] [CrossRef] [PubMed]
- Stringhini, S.; Wisniak, A.; Piumatti, G.; Azman, A.S.; Lauer, S.A.; Baysson, H.; De Ridder, D.; Petrovic, D.; Schrempft, S.; Marcus, K.; et al. Seroprevalence of anti-SARS-CoV-2 IgG antibodies in Geneva, Switzerland (SEROCoV-POP): A population-based study. Lancet 2020, 396, 313–319. [Google Scholar] [CrossRef]
- Kasztelewicz, B.; Janiszewska, K.; Burzyńska, J.; Szydłowska, E.; Migdał, M.; Dzierżanowska-Fangrat, K. Prevalence of IgG antibodies against SARS-CoV-2 among healthcare workers in a tertiary pediatric hospital in Poland. PLoS ONE 2021, 16, e0249550. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Mcgoogan, J.M. Characteristics of and Important Lessons From the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Singh, A.K.; Gillies, C.L.; Singh, R.; Singh, A.; Chudasama, Y.; Coles, B.; Seidu, S.; Zaccardi, F.; Davies, M.J.; Khunti, K. Prevalence of co-morbidities and their association with mortality in patients with COVID-19: A systematic review and meta-analysis. Diabetes Obes. Metab. 2020, 22, 1915–1924. [Google Scholar] [CrossRef]
- Wood, J.; Datta, D.; Hudson, B.L.; Co, K.; Tepner, S.; Hardwick, E.; John, C.C. Prevalence of Asymptomatic SARS-CoV-2 Infection in Children and Adults in Marion County, Indiana. Cureus 2020, 12, e9794. [Google Scholar] [PubMed]
- Hagmann, S.H.F. COVID-19 in children: More than meets the eye. Travel Med. Infect. Dis. 2020, 34, 101649. [Google Scholar] [CrossRef]
- Mallajosyula, V.; Ganjavi, C.; Chakraborty, S.; Mcsween, A.M.; Pavlovitch-Bedzyk, A.J.; Wilhelmy, J.; Nau, A.; Manohar, M.; Nadeau, K.C.; Davis, M.M. CD8(+) T cells specific for conserved coronavirus epitopes correlate with milder disease in COVID-19 patients. Sci. Immunol. 2021, 6, 1697–1701. [Google Scholar] [CrossRef]
- Chang, L.; Hou, W.; Zhao, L.; Zhang, Y.; Wang, Y.; Wu, L.; Xu, T.; Wang, L.; Wang, J.; Ma, J.; et al. The prevalence of antibodies to SARS-CoV-2 among blood donors in China. Nat. Commun. 2021, 12, 1383. [Google Scholar] [CrossRef]
- Mahallawi, W.H.; Al-Zalabani, A.H. The seroprevalence of SARS-CoV-2 IgG antibodies among asymptomatic blood donors in Saudi Arabia. Saudi J. Biol. Sci. 2020, 28, 1697–1701. [Google Scholar] [CrossRef]
- Crovetto, F.; Crispi, F.; Llurba, E.; Figueras, F.; Gomez-Roig, M.D.; Gratacos, E. Seroprevalence and presentation of SARS-CoV-2 in pregnancy. Lancet 2020, 396, 530–531. [Google Scholar] [CrossRef]
- Hippich, M.; Holthaus, L.; Assfalg, R.; Zapardiel-Gonzalo, J.; Kapfelsperger, H.; Heigermoser, M.; Haupt, F.; Ewald, D.A.; Welzhofer, T.C.; Marcus, B.A.; et al. A Public Health Antibody Screening Indicates a 6-Fold Higher SARS-CoV-2 Exposure Rate than Reported Cases in Children. Med 2021, 2, 149–163.e4. [Google Scholar] [CrossRef] [PubMed]
- Charan, J.; Biswas, T. How to calculate sample size for different study designs in medical research? Indian J. Psychol. Med. 2013, 35, 121–126. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mahallawi, W.H. A serological assay to detect human SARS-CoV-2 antibodies. J. Taibah Univ. Med. Sci. 2021, 16, 57–62. [Google Scholar]
- Liu, T.; Gong, D.; Xiao, J.; Hu, J.; He, G.; Rong, Z.; Ma, W. Cluster infections play important roles in the rapid evolution of COVID-19 transmission: A systematic review. Int. J. Infect. Dis. 2020, 99, 374–380. [Google Scholar] [CrossRef]
- Viner, R.M.; Mytton, O.T.; Bonell, C.; Melendez-Torres, G.J.; Ward, J.; Hudson, L.; Waddington, C.; Thomas, J.; Russell, S.; Van Der Klis, F.; et al. Susceptibility to SARS-CoV-2 Infection Among Children and Adolescents Compared with Adults: A Systematic Review and Meta-analysis. JAMA Pediatrics 2021, 175, 143–156. [Google Scholar] [CrossRef]
- Jeng, M.-J. Coronavirus disease 2019 in children: Current status. J. Chin. Med. Assoc. 2020, 83, 527–533. [Google Scholar] [CrossRef]
- Jung, C.-Y.; Park, H.; Kim, D.W.; Lim, H.; Chang, J.H.; Choi, Y.J.; Kim, S.W.; Chang, T.I. Association between Body Mass Index and Risk of Coronavirus Disease 2019 (COVID-19): A Nationwide Case-control Study in South Korea. Clin. Infect. Dis. 2020, 83, 527–533. [Google Scholar] [CrossRef]
- Naranbhai, V.; Chang, C.C.; Beltran, W.F.G.; Miller, T.E.; Astudillo, M.G.; Villalba, J.A.; Yang, D.; Gelfand, J.; Bernstein, B.E.; Feldman, J.; et al. High Seroprevalence of Anti-SARS-CoV-2 Antibodies in Chelsea, Massachusetts. J. Infect. Dis. 2020, 222, 1955–1959. [Google Scholar] [CrossRef]
- Paul, L.A.; Daneman, N.; Schwartz, K.L.; Science, M.; Brown, K.A.; Whelan, M.; Chan, E.; Buchan, S.A. Association of Age and Pediatric Household Transmission of SARS-CoV-2 Infection. JAMA Pediatrics 2021, 6, 1697–1701. [Google Scholar]
- Wang, R.; Jin, F.; Cao, S.; Yuan, H.; Qu, J.; Zhang, J.; Li, Y.; Chen, X.; Song, W.; XIE, Z. Seroprevalence of SARS-CoV-2 infections among children visiting a hospital. Pediatric Investig. 2020, 4, 236–241. [Google Scholar] [CrossRef]
- Mahallawi, W.H.; Alsamiri, A.D.; Dabbour, A.F.; Alsaeedi, H.; Al-Zalabani, A.H. Association of Viral Load in SARS-CoV-2 Patients with Age and Gender. Front. Med. 2021, 8, 608215. [Google Scholar] [CrossRef]
- Mahallawi, W. Persistence of hepatitis B surface antibody and immune memory to hepatitis B vaccine among medical college students in Madinah. Ann. Saudi Med. 2018, 38, 413–419. [Google Scholar] [CrossRef]
- Bonfante, F.; Costenaro, P.; Cantarutti, A.; Di Chiara, C.; Bortolami, A.; Petrara, M.R.; Carmona, F.; Pagliari, M.; Cosma, C.; Cozzani, S.; et al. Mild SARS-CoV-2 Infections and Neutralizing Antibody Titers. Pediatrics 2021, 148, e2021052173. [Google Scholar] [CrossRef]
- Yang, H.S.; Costa, V.; Racine-Brzostek, S.E.; Acker, K.P.; Yee, J.; Chen, Z.; Karbaschi, M.; Zuk, R.; Rand, S.; Sukhu, A.; et al. Association of Age with SARS-CoV-2 Antibody Response. JAMA Netw. Open 2021, 4, e214302. [Google Scholar] [CrossRef]
- Flannery, D.D.; Gouma, S.; Dhudasia, M.B.; Mukhopadhyay, S.; Pfeifer, M.R.; Woodford, E.C.; Triebwasser, J.E.; Gerber, J.S.; Morris, J.S.; Weirick, M.E.; et al. Assessment of Maternal and Neonatal Cord Blood SARS-CoV-2 Antibodies and Placental Transfer Ratios. JAMA Pediatrics 2021, 175, 594–600. [Google Scholar] [CrossRef]
- Breslin, N.; Baptiste, C.; Gyamfi-Bannerman, C.; Miller, R.; Martinez, R.; Bernstein, K.; Ring, L.; Landau, R.; Purisch, S.; Friedman, A.M.; et al. Coronavirus disease 2019 infection among asymptomatic and symptomatic pregnant women: Two weeks of confirmed presentations to an affiliated pair of New York City hospitals. Am. J. Obstet. Gynecol. MFM 2020, 2, 100118. [Google Scholar] [CrossRef]
- Chen, H.; Guo, J.; Wang, C.; Luo, F.; Yu, X.; Zhang, W.; Li, J.; Zhao, D.; Xu, D.; Gong, Q.; et al. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: A retrospective review of medical records. Lancet 2020, 395, 809–815. [Google Scholar] [CrossRef] [Green Version]
- Chen, R.; Zhang, Y.; Huang, L.; Cheng, B.H.; Xia, Z.Y.; Meng, Q.T. Safety and efficacy of different anesthetic regimens for parturients with COVID-19 undergoing Cesarean delivery: A case series of 17 patients. Can. J. Anaesth. 2020, 67, 655–663. [Google Scholar] [CrossRef] [Green Version]
- Wastnedge, E.A.N.; Reynolds, R.M.; Van Boeckel, S.R.; Stock, S.J.; Denison, F.C.; Maybin, J.A.; Critchley, H.O.D. Pregnancy and COVID-19. Physiol. Rev. 2020, 101, 303–318. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.P.; Flaxman, S.; Gallinat, A.S.; Kinosian, S.P.; Stemkovski, M.; Unwin, H.J.T.; Watson, O.J.; Whittaker, C.; Cattarino, L.; Dorigatti, I.; et al. Temperature and population density influence SARS-CoV-2 transmission in the absence of nonpharmaceutical interventions. Proc. Natl. Acad. Sci. USA 2021, 118, e2019284118. [Google Scholar] [CrossRef]
- Alsayb, M.A.; Alsamiri, A.D.D.; Makhdoom, H.Q.; Alwasaidi, T.; Osman, H.M.; Mahallawi, W.H. Prolonged humoral and cellular immunity in COVID-19-recovered patients. Saudi J. Biol. Sci. 2021, 28, 4010–4015. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Children (n = 332) | |
|---|---|
| Age in years, mean ± SD median (IQR) | 5.42 ± 4.23 5.00 (2.00–9.00) |
| Children aged ≤ 1 year, n (%) | |
| Yes | 75 (22.6) |
| No | 257 (77.4) |
| Newborn, n (%) | |
| Yes | 17 (22.7) |
| No | 58 (77.3) |
| Sex, n (%) | |
| Male | 178 (53.6) |
| Female | 154 (46.4) |
| Nationality, n (%) | |
| Saudi | 279 (84.0) |
| Non-Saudi | 53 (16.0) |
| Blood group, n (%) | |
| A | 102 (30.7) |
| B | 63 (19.0) |
| AB | 15 (4.50) |
| O | 152 (45.8) |
| Women (n = 247) | |
| Age in years, mean ± SD median (IQR) | 33.4 ± 9.80 33.0 (26.0–40.0) |
| Nationality, n (%) | |
| Saudi | 213 (86.2) |
| Non-Saudi | 34 (13.8) |
| Blood group, n (%) | |
| A | 78 (31.6) |
| B | 43 (17.4) |
| AB | 7 (2.80) |
| O | 119 (48.2) |
| Weight status 1, n (%) | |
| Underweight | 3 (1.36) |
| Healthy weight | 57 (25.8) |
| Overweight | 74 (33.5) |
| Obese | 87 (39.4) |
| Children (n = 332) | |||
|---|---|---|---|
| Negative (n = 137) | Positive (n = 195) | p-Value | |
| Age in years, mean ± SD Median (IQR) | 5.36 ± 4.11 4.00 (2.00–9.50) | 5.47 ± 4.32 5.00 (2.00–9.00) | 0.963 |
| Children aged ≤ 1 year, n (%) | |||
| Yes | 30 (40.0) | 45 (60.0) | 0.894 |
| No | 107 (41.6) | 150 (58.4) | |
| Newborn, n (%) | |||
| Yes | 9 (52.9) | 8 (47.1) | 0.325 |
| No | 128 (40.6) | 187 (59.4) | |
| Sex, n (%) | |||
| Male | 68 (38.2) | 110 (61.8) | 0.264 |
| Female | 69 (44.8) | 85 (55.2) | |
| Nationality, n (%) | |||
| Saudi | 117 (42.1) | 162 (58.1) | 0.649 |
| Non-Saudi | 20 (37.7) | 33 (62.3) | |
| Blood group, n (%) | |||
| A | 41 (40.2) | 61 (59.8) | 0.516 |
| B | 22 (34.9) | 41 (65.1) | |
| AB | 8 (53.3) | 7 (46.7) | |
| O | 66 (43.4) | 86 (56.6) | |
| Women (n = 247) | |||
| Negative (n = 123) | Positive (n = 124) | p-Value | |
| Age in years, mean ± SD Median (IQR) | 31.5 ± 8.55 30.0 (26.0–38.0) | 35.4 ± 10.6 35.0 (27.0–42.0) | 0.004 1 |
| Nationality, n (%) | |||
| Saudi | 107 (50.2) | 106 (49.8) | 0.356 |
| Non-Saudi | 14 (41.2) | 20 (58.8) | |
| Blood group, n (%) | |||
| A | 32 (41.0) | 46 (59.0) | 0.434 |
| B | 22 (51.2) | 21 (48.8) | |
| AB | 5 (71.4) | 2 (28.6) | |
| O | 62 (52.1) | 57 (47.9) | |
| Weight status 2, n (%) | |||
| Underweight | 2 (66.7) | 1 (33.3) | 0.076 |
| Healthy weight | 27 (47.4) | 30 (52.6) | |
| Overweight | 44 (59.5) | 30 (40.5) | |
| Obese | 35 (40.2) | 52 (59.8) | |
| OR | 95% Confidence Interval | p-Value | |
|---|---|---|---|
| Children | |||
| Age, years | 1.01 | 0.96 to 1.06 | 0.817 |
| Sex | |||
| Male | Refrence catogary | ||
| Female | 0.76 | 0.49 to 1.18 | 0.223 |
| Nationality | |||
| Saudi | Refrence catogary | ||
| Non-Saudi | |||
| Blood group | |||
| A | Refrence catogary | ||
| B | 1.25 | 0.65 to 2.40 | 0.50 |
| AB | 0.59 | 0.20 to 1.75 | 0.339 |
| O | 0.88 | 0.53 to 1.46 | 0.610 |
| Women | |||
| Age, years | 1.04 | 1.02 to 1.07 | 0.002 1 |
| Nationality | |||
| Saudi | Refrence catogary | ||
| Non-Saudi | 1.48 | 0.71 to 3.09 | 0.292 |
| Blood group | |||
| A | Refrence catogary | ||
| B | 0.74 | 0.35 to 1.56 | 0.424 |
| AB | 0.31 | 0.06 to 1.69 | 0.176 |
| O | 0.71 | 0.40 to 1.26 | 0.243 |
| Weight status | |||
| Underweight | Refrence catogary | ||
| Healthy weight | 2.06 | 0.18 to 23.9 | 0.562 |
| Overweight | 1.38 | 0.12 to 15.8 | 0.80 |
| Obese | 2.70 | 0.24 to 30.8 | 0.42 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahallawi, W.H.; Ibrahim, N.A.; Aljohani, A.S.; Shaikh, E.A.; Nafe, R.H.; Khan, A.M.; Mumena, W.A. Assessment of SARS-CoV-2 Anti-Spike IgG Antibody in Women and Children in Madinah, Saudi Arabia: A Single-Center Study. Int. J. Environ. Res. Public Health 2021, 18, 9971. https://doi.org/10.3390/ijerph18199971
Mahallawi WH, Ibrahim NA, Aljohani AS, Shaikh EA, Nafe RH, Khan AM, Mumena WA. Assessment of SARS-CoV-2 Anti-Spike IgG Antibody in Women and Children in Madinah, Saudi Arabia: A Single-Center Study. International Journal of Environmental Research and Public Health. 2021; 18(19):9971. https://doi.org/10.3390/ijerph18199971
Chicago/Turabian StyleMahallawi, Waleed H., Nadir A. Ibrahim, Ammar S. Aljohani, Ehab A. Shaikh, Rayan H. Nafe, Anas M. Khan, and Walaa A. Mumena. 2021. "Assessment of SARS-CoV-2 Anti-Spike IgG Antibody in Women and Children in Madinah, Saudi Arabia: A Single-Center Study" International Journal of Environmental Research and Public Health 18, no. 19: 9971. https://doi.org/10.3390/ijerph18199971