
Polypharmacy Exposure, Aging Populations, and COVID-19: Considerations for Healthcare Providers and Public Health Practitioners in Africa


{kind=link}
Abstract
:1. COVID-19 and an Older Nigerian Couple
2. Polypharmacy in the African Context
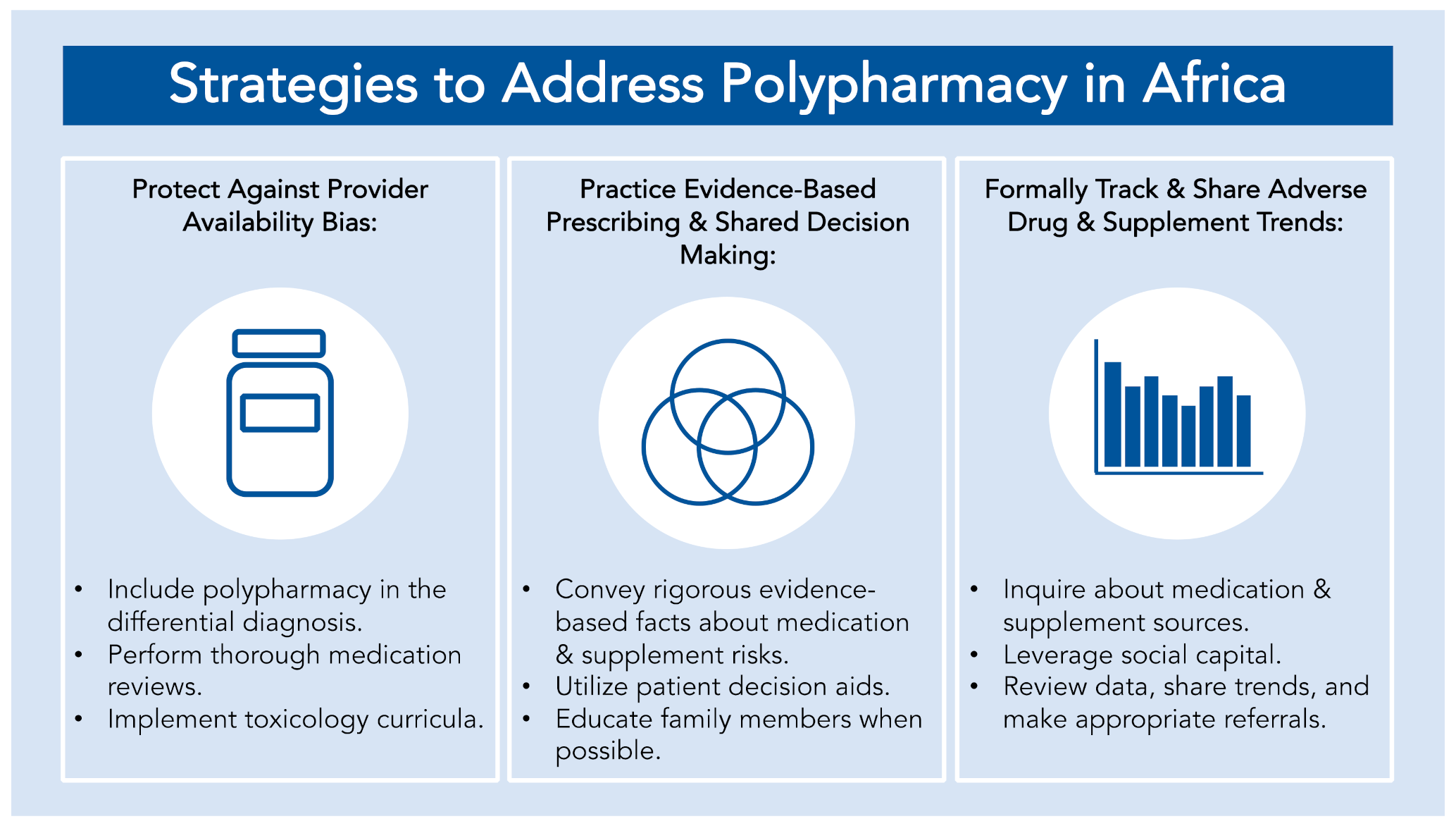
3. Strategies for African Providers and Public Health Practitioners
3.1. Bolstering Training to Safeguard against Provider Availability Biases
3.2. Continue the Practice of Evidence-Based Prescribing and Shared Decision Making
3.3. Formally Track and Share Local Trends and Patterns
4. Conclusion: Building to Last
Author Contributions
Funding
Conflicts of Interest
References
- Chary, M.A.; Barbuto, A.F.; Izadmehr, S.; Hayes, B.D.; Burns, M.M. COVID-19: Therapeutics and Their Toxicities. J. Med. Toxicol. 2020, 16, 284–294. [Google Scholar] [CrossRef] [PubMed]
- Masnoon, N.; Shakib, S.; Kalisch-Ellett, L.; Caughey, G.E. What Is Polypharmacy? A Systematic Review of Definitions. BMC Geriatr. 2017, 17, 230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, S.; Singh, K.; Dhingra, S.; Charan, J.; Sharma, P.; Islam, S.; Jahan, D.; Iskandar, K.; Samad, N.; Haque, M. The Double Burden of the COVID-19 Pandemic and Polypharmacy on Geriatric Population—Public Health Implications. Clin. Risk Manag. 2020, 16, 1007–1022. [Google Scholar] [CrossRef] [PubMed]
- Padma, T.V. COVID Vaccines to Reach Poorest Countries in 2023—Despite Recent Pledges. Nature 2021, 595, 342–343. [Google Scholar] [CrossRef]
- Therapeutics and COVID-19: Living Guideline. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-therapeutics-2021.2 (accessed on 21 September 2021).
- Chandler, R.E. Serious Neurological Adverse Events after Ivermectin—Do They Occur beyond the Indication of Onchocerciasis? Am. J. Trop. Med. Hyg. 2018, 98, 382–388. [Google Scholar] [CrossRef] [Green Version]
- Chaccour, C.J.; Hammann, F.; Alustiza, M.; Castejon, S.; Tarimo, B.B.; Abizanda, G.; Irigoyen Barrio, Á.; Martí Soler, H.; Moncada, R.; Bilbao, J.I.; et al. Cytochrome P450/ABC Transporter Inhibition Simultaneously Enhances Ivermectin Pharmacokinetics in the Mammal Host and Pharmacodynamics in Anopheles Gambiae. Sci. Rep. 2017, 7, 8535. [Google Scholar] [CrossRef] [Green Version]
- Geller, A.I.; Shehab, N.; Weidle, N.J.; Lovegrove, M.C.; Wolpert, B.J.; Timbo, B.B.; Mozersky, R.P.; Budnitz, D.S. Emergency Department Visits for Adverse Events Related to Dietary Supplements. N. Engl. J. Med. 2015, 373, 1531–1540. [Google Scholar] [CrossRef]
- Bureau, U.C. Census Bureau Releases New Report on Aging in Africa. Available online: https://www.census.gov/newsroom/press-releases/2020/aging-in-africa.html (accessed on 19 January 2021).
- Schneider, M.; Ho Tu Nam, N. Africa and Counterfeit Pharmaceuticals in the Times of COVID-19. J. Intellect. Prop. Law Pract. 2020, 15, 417–418. [Google Scholar] [CrossRef]
- Fake COVID-19 Vaccines Pose New Threat in Africa—WSJ. Available online: https://www.wsj.com/articles/fake-covid-19-vaccines-pose-new-threat-in-africa-11622971955 (accessed on 21 September 2021).
- Sawe, H.R.; Akomeah, A.; Mfinanga, J.A.; Runyon, M.S.; Noste, E. Emergency Medicine Residency Training in Africa: Overview of Curriculum. BMC Med. Educ. 2019, 19, 294. [Google Scholar] [CrossRef] [Green Version]
- Kretchy, I.A.; Asiedu-Danso, M.; Kretchy, J.-P. Medication Management and Adherence during the COVID-19 Pandemic: Perspectives and Experiences from Low-and Middle-Income Countries. Res. Soc. Adm. Pharm. 2021, 17, 2023–2026. [Google Scholar] [CrossRef]
- Ogunleye, O.O.; Basu, D.; Mueller, D.; Sneddon, J.; Seaton, R.A.; Yinka-Ogunleye, A.F.; Wamboga, J.; Miljković, N.; Mwita, J.C.; Rwegerera, G.M.; et al. Response to the Novel Corona Virus (COVID-19) Pandemic Across Africa: Successes, Challenges, and Implications for the Future. Front. Pharmacol. 2020, 11, 1205. [Google Scholar] [CrossRef]
- Seidu, A.-A.; Hagan, J.E.; Ameyaw, E.K.; Ahinkorah, B.O.; Schack, T. The Role of Testing in the Fight against COVID-19: Current Happenings in Africa and the Way Forward. Int. J. Infect. Dis. 2020, 98, 237–240. [Google Scholar] [CrossRef]
- Mulu, A.; Bekele, A.; Abdissa, A.; Balcha, T.T.; Habtamu, M.; Mihret, A.; Alemayehu, D.H.; Beyene, G.T.; Bayih, A.G. The Challenges of COVID-19 Testing in Africa: The Ethiopian Experience. Pan. Afr. Med. J. 2021, 38, 6. [Google Scholar] [CrossRef]
- Amexo, M.; Tolhurst, R.; Barnish, G.; Bates, I. Malaria Misdiagnosis: Effects on the Poor and Vulnerable. Lancet 2004, 364, 1896–1898. [Google Scholar] [CrossRef]
- A-Elgayoum, S.M.E.; El-Feki, A.E.-K.A.; Mahgoub, B.A.; El-Rayah, E.-A.; Giha, H.A. Malaria Overdiagnosis and Burden of Malaria Misdiagnosis in the Suburbs of Central Sudan: Special Emphasis on Artemisinin-Based Combination Therapy Era. Diagn. Microbiol. Infect. Dis. 2009, 64, 20–26. [Google Scholar] [CrossRef]
- Onchiri, F.M.; Pavlinac, P.; Singa, B.O.; Mulongo, J.N.; Farquhar, C.; John-Stewart, G.C.; Walson, J. Frequency and Correlates of Malaria Overdiagnosis and Treatment in Western Kenya. Lancet Glob. Health 2014, 2, S45. [Google Scholar] [CrossRef] [Green Version]
- Owoyemi, A.; Owoyemi, J.; Osiyemi, A.; Boyd, A. Artificial Intelligence for Healthcare in Africa. Front. Digit. Health 2020, 2, 6. [Google Scholar] [CrossRef]
- Aneni, E.; De Beer, I.H.; Hanson, L.; Rijnen, B.; Brenan, A.T.; Feeley, F.G. Mobile Primary Healthcare Services and Health Outcomes of Children in Rural Namibia. Rural Remote Health 2013, 13, 2380. [Google Scholar]
- Amimo, F.; Lambert, B.; Magit, A.; Hashizume, M. A Review of Prospective Pathways and Impacts of COVID-19 on the Accessibility, Safety, Quality, and Affordability of Essential Medicines and Vaccines for Universal Health Coverage in Africa. Glob. Health 2021, 17, 42. [Google Scholar] [CrossRef]
- Social Innovation in Health Initiative | Chipatala Cha Pa Foni: Health Centre by Phone. Available online: https://www.who.int/tdr/news/2017/sihi-update/en/ (accessed on 30 November 2017).
- Broniatowski, D.A.; Klein, E.Y.; Reyna, V.F. Germs Are Germs, and Why Not Take a Risk? Patients’ Expectations for Prescribing Antibiotics in an Inner-City Emergency Department. Med. Decis. Mak. 2015, 35, 60–67. [Google Scholar] [CrossRef] [Green Version]
- Llor, C.; Bjerrum, L. Antimicrobial Resistance: Risk Associated with Antibiotic Overuse and Initiatives to Reduce the Problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [Green Version]
- Vedasto, O.; Morris, B.; Furia, F.F. Shared Decision-Making between Health Care Providers and Patients at a Tertiary Hospital Diabetic Clinic in Tanzania. BMC Health Serv. Res. 2021, 21, 8. [Google Scholar] [CrossRef]
- Jull, J.; Giles, A.; Boyer, Y.; Stacey, D.; Lodge, M. Cultural Adaptation of a Shared Decision Making Tool with Aboriginal Women: A Qualitative Study. BMC Med. Inform. Decis. Mak. 2015, 15, 1–3. [Google Scholar] [CrossRef] [Green Version]
- National Institutes of Health Statement on Ivermectin. Available online: https://www.covid19treatmentguidelines.nih.gov/statement-on-ivermectin/ (accessed on 25 January 2021).
- WHO Advises That Ivermectin Only Be Used to Treat COVID-19 within Clinical Trials. Available online: https://www.who.int/news-room/feature-stories/detail/who-advises-that-ivermectin-only-be-used-to-treat-covid-19-within-clinical-trials (accessed on 21 September 2021).
- Mowafi, H.; Ngaruiya, C.; O’Reilly, G.; Kobusingye, O.; Kapil, V.; Rubiano, A.; Ong, M.; Puyana, J.C.; Rahman, A.F.; Jooma, R.; et al. Emergency Care Surveillance and Emergency Care Registries in Low-Income and Middle-Income Countries: Conceptual Challenges and Future Directions for Research. BMJ Glob. Health 2019, 4, e001442. [Google Scholar] [CrossRef]
- Amoah, P.A.; Phillips, D.R. Strengthening the Referral System through Social Capital: A Qualitative Inquiry in Ghana. Healthcare 2017, 5, 80. [Google Scholar] [CrossRef] [Green Version]
- Bossyns, P.; Van Lerberghe, W. The Weakest Link: Competence and Prestige as Constraints to Referral by Isolated Nurses in Rural Niger. Hum. Resour. Health 2004, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Shobiye, H.O.; Bolarinwa, O.A.; Fasiku, M.M.; Akande, T.M.; Janssens, W. What Medicines Do Households Keep in Their Cabinets? Understanding the Possession and Use of Medicines at Home and the Role of Health Insurance in Nigeria. PLoS ONE 2021, 16, e0247591. [Google Scholar] [CrossRef]
- Ssonko, M.; Stanaway, F.; Mayanja, H.K.; Namuleme, T.; Cumming, R.; Kyalimpa, J.L.; Karamagi, Y.; Mukasa, B.; Naganathan, V. Polypharmacy among HIV Positive Older Adults on Anti-Retroviral Therapy Attending an Urban Clinic in Uganda. BMC Geriatr. 2018, 18, 125. [Google Scholar] [CrossRef] [Green Version]
- Ayenew, W.; Asmamaw, G.; Bitew, T. Antipsychotic Polypharmacy Among Patients With Schizophrenia in Africa: A Systematic Review and Meta-Analysis. Int. J. Neuropsychopharmacol. 2021, 20, 1–9. [Google Scholar] [CrossRef]
- James, P.B.; Wardle, J.; Steel, A.; Adams, J. Traditional, Complementary and Alternative Medicine Use in Sub-Saharan Africa: A Systematic Review. BMJ Glob. Health 2018, 3, e000895. [Google Scholar] [CrossRef] [Green Version]
- Sambo, L.G.; Kirigia, J.M. Evaluation of Health-Related Programmes in Africa: A Vision for 2020. East. Afr. Med. J. 2001, 78, S20–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nwanaji-Enwerem, J.C.; Boyer, E.W.; Olufadeji, A. Polypharmacy Exposure, Aging Populations, and COVID-19: Considerations for Healthcare Providers and Public Health Practitioners in Africa. Int. J. Environ. Res. Public Health 2021, 18, 10263. https://doi.org/10.3390/ijerph181910263
Nwanaji-Enwerem JC, Boyer EW, Olufadeji A. Polypharmacy Exposure, Aging Populations, and COVID-19: Considerations for Healthcare Providers and Public Health Practitioners in Africa. International Journal of Environmental Research and Public Health. 2021; 18(19):10263. https://doi.org/10.3390/ijerph181910263
Chicago/Turabian StyleNwanaji-Enwerem, Jamaji C., Edward W. Boyer, and Ayobami Olufadeji. 2021. "Polypharmacy Exposure, Aging Populations, and COVID-19: Considerations for Healthcare Providers and Public Health Practitioners in Africa" International Journal of Environmental Research and Public Health 18, no. 19: 10263. https://doi.org/10.3390/ijerph181910263