
Quality Indicators for Avalanche Victim Management and Rescue

 , , ,
, , ,
Abstract
:1. Introduction
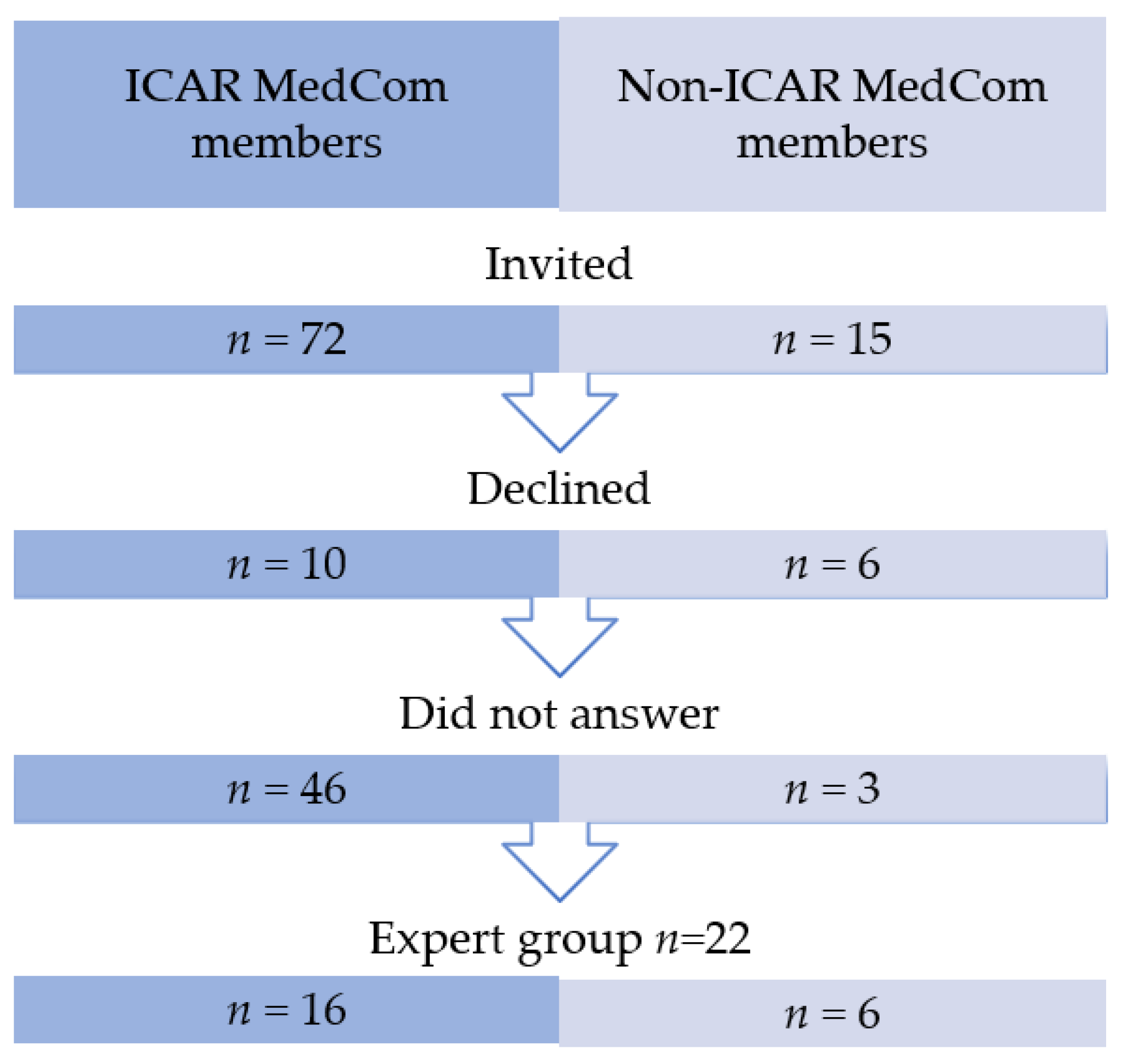
2. Materials and Methods
3. Results
4. Discussion
4.1. Prior to Rescue
4.2. Patient Assessment
4.3. Patient Management
4.4. Transport and In-Hospital Management
4.5. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Tilburg, C.; Grissom, C.K.; Zafren, K.; McIntosh, S.; Radwin, M.I.; Paal, P.; Haegeli, P.; Smith, W.W.; Wheeler, A.R.; Weber, D.; et al. Wilderness Medical Society Practice Guidelines for Prevention and Management of Avalanche and Nonavalanche Snow Burial Accidents. Wilderness Environ. Med. 2017, 28, 23–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lott, C.; Truhlar, A.; Alfonzo, A.; Barelli, A.; Gonzalez-Salvado, V.; Hinkelbein, J.; Nolan, J.P.; Paal, P.; Perkins, G.D.; Thies, K.C.; et al. European Resuscitation Council Guidelines 2021: Cardiac arrest in special circumstances. Resuscitation 2021, 161, 152–219. [Google Scholar] [CrossRef]
- Metrailler-Mermoud, J.; Hugli, O.; Carron, P.N.; Kottmann, A.; Frochaux, V.; Zen-Ruffinen, G.; Pasquier, M. Avalanche victims in cardiac arrest are unlikely to survive despite adherence to medical guidelines. Resuscitation 2019, 141, 35–43. [Google Scholar] [CrossRef]
- Pasquier, M.; Hugli, O. Reply to: Low incidence of avalanche victims in cardiac arrest calls for multi-centre studies and registries for the validation of resuscitation guidelines. Resuscitation 2019, 144, 197–198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moroder, L.; Mair, B.; Brugger, H.; Voelckel, W.; Mair, P. Outcome of avalanche victims with out-of-hospital cardiac arrest. Resuscitation 2015, 89, 114–118. [Google Scholar] [CrossRef]
- Strapazzon, G.; Plankensteiner, J.; Mair, P.; Ruttmann, E.; Dal Cappello, T.; Procter, E.; Brugger, H. Prehospital management and outcome of avalanche patients with out-of-hospital cardiac arrest: A retrospective study in Tyrol, Austria. Eur. J. Emerg. Med. 2017, 24, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Lossius, H.M.; Kruger, A.J.; Ringdal, K.G.; Sollid, S.J.; Lockey, D.J. Developing templates for uniform data documentation and reporting in critical care using a modified nominal group technique. Scand. J. Trauma Resusc. Emerg. Med. 2013, 21, 80. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Campbell, S.M.; Braspenning, J.; Hutchinson, A.; Marshall, M.N. Research methods used in developing and applying quality indicators in primary care. BMJ 2003, 326, 816–819. [Google Scholar] [CrossRef] [PubMed]
- National Quality Forum: Evaluation Criteria and Guidance for Evaluating Measures for Endorsement. Available online: http://www.qualityforum.org/WorkArea/linkit.aspx?LinkIdentifier=id&ItemID=86084 (accessed on 8 September 2021).
- Truhlar, A.; Deakin, C.D.; Soar, J.; Khalifa, G.E.; Alfonzo, A.; Bierens, J.J.; Brattebo, G.; Brugger, H.; Dunning, J.; Hunyadi-Anticevic, S.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 4. Cardiac arrest in special circumstances. Resuscitation 2015, 95, 148–201. [Google Scholar] [CrossRef]
- Brugger, H.; Durrer, B.; Elsensohn, F.; Paal, P.; Strapazzon, G.; Winterberger, E.; Zafren, K.; Boyd, J. Resuscitation of avalanche victims: Evidence-based guidelines of the International Commission for Mountain Emergency Medicine (ICAR MEDCOM): Intended for physicians and other advanced life support personnel. Resuscitation 2013, 84, 539–546. [Google Scholar] [CrossRef]
- Murphy, A.; Wakai, A.; Walsh, C.; Cummins, F.; O’Sullivan, R. Development of key performance indicators for prehospital emergency care. Emerg. Med. J. 2016, 33, 286–292. [Google Scholar] [CrossRef]
- Brugger, H.; Strapazzon, G.; Wallner, B.; Paal, P. Low incidence of avalanche victims in cardiac arrest calls for multi-centre studies and registries for the validation of resuscitation guidelines. Resuscitation 2019, 144, 195–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coats, T.J. A revised Utstein Template for trauma. Emerg. Med. J. 2010, 27, 339. [Google Scholar] [CrossRef] [PubMed]
- Tomazin, I.; Vegnuti, M.; Ellerton, J.; Reisten, O.; Sumann, G.; Kersnik, J. Factors impacting on the activation and approach times of helicopter emergency medical services in four Alpine countries. Scand. J. Trauma Resusc. Emerg. Med. 2012, 20, 56. [Google Scholar] [CrossRef] [Green Version]
- Procter, E.; Strapazzon, G.; Dal Cappello, T.; Zweifel, B.; Wurtele, A.; Renner, A.; Falk, M.; Brugger, H. Burial duration, depth and air pocket explain avalanche survival patterns in Austria and Switzerland. Resuscitation 2016, 105, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Strapazzon, G.; Brugger, H. On-site treatment of snow avalanche victims: From bench to mountainside. High. Alt. Med. Biol. 2018, 19, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Brugger, H.; Durrer, B.; Adler-Kastner, L.; Falk, M.; Tschirky, F. Field management of avalanche victims. Resuscitation 2001, 51, 7–15. [Google Scholar] [CrossRef]
- Boyd, J.; Haegeli, P.; Abu-Laban, R.B.; Shuster, M.; Butt, J.C. Patterns of death among avalanche fatalities: A 21-year review. CMAJ 2009, 180, 507–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McIntosh, S.E.; Grissom, C.K.; Olivares, C.R.; Kim, H.S.; Tremper, B. Cause of death in avalanche fatalities. Wilderness Environ. Med. 2007, 18, 293–297. [Google Scholar] [CrossRef] [Green Version]
- Kottmann, A.; Carron, P.N.; Theiler, L.; Albrecht, R.; Tissi, M.; Pasquier, M. Identification of the technical and medical requirements for HEMS avalanche rescue missions through a 15-year retrospective analysis in a HEMS in Switzerland: A necessary step for quality improvement. Scand. J. Trauma Resusc. Emerg. Med. 2018, 26, 54. [Google Scholar] [CrossRef]
- Hohlrieder, M.; Thaler, S.; Wuertl, W.; Voelckel, W.; Ulmer, H.; Brugger, H.; Mair, P. Rescue missions for totally buried avalanche victims: Conclusions from 12 years of experience. High. Alt. Med. Biol. 2008, 9, 229–233. [Google Scholar] [CrossRef]
- Pasquier, M.; Hugli, O.; Paal, P.; Darocha, T.; Blancher, M.; Husby, P.; Silfvast, T.; Carron, P.N.; Rousson, V. Hypothermia outcome prediction after extracorporeal life support for hypothermic cardiac arrest patients: The HOPE score. Resuscitation 2018, 126, 58–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pasquier, M.; Rousson, V.; Darocha, T.; Bouzat, P.; Kosinski, S.; Sawamoto, K.; Champigneulle, B.; Wiberg, S.; Wanscher, M.C.J.; Brodmann Maeder, M.; et al. Hypothermia outcome prediction after extracorporeal life support for hypothermic cardiac arrest patients: An external validation of the HOPE score. Resuscitation 2019, 139, 321–328. [Google Scholar] [CrossRef]
- Walls, R.M. Manual of Emergency Airway Management, 4th ed.; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2012. [Google Scholar]
- Schwartz, H.P.; Bigham, M.T.; Schoettker, P.J.; Meyer, K.; Trautman, M.S.; Insoft, R.M. Quality metrics in neonatal and pediatric critical care transport: A national Delphi project. Pediatric Crit. Care Med. 2015, 16, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Dietrichs, E.S.; Tveita, T.; Smith, G. Hypothermia and cardiac electrophysiology: A systematic review of clinical and experimental data. Cardiovasc. Res. 2019, 115, 501–509. [Google Scholar] [CrossRef]
- Hohlrieder, M.; Brugger, H.; Schubert, H.M.; Pavlic, M.; Ellerton, J.; Mair, P. Pattern and severity of injury in avalanche victims. High. Alt. Med. Biol. 2007, 8, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Boue, Y.; Payen, J.F.; Torres, J.P.; Blancher, M.; Bouzat, P. Full neurologic recovery after prolonged avalanche burial and cardiac arrest. High. Alt. Med. Biol. 2014, 15, 522–523. [Google Scholar] [CrossRef] [PubMed]
- Eidenbenz, D.; Techel, F.; Kottmann, A.; Rousson, V.; Carron, P.N.; Albrecht, R.; Pasquier, M. Survival probability in avalanche victims with long burial (>/=60 min): A retrospective study. Resuscitation 2021. [Google Scholar] [CrossRef] [PubMed]
- Kottmann, A.; Blancher, M.; Pasquier, M.; Brugger, H. Avalanche Victim Resuscitation Checklist adaption to the 2015 ERC Resuscitation guidelines. Resuscitation 2017, 113, e3–e4. [Google Scholar] [CrossRef] [Green Version]
- Kottmann, A.; Blancher, M.; Spichiger, T.; Elsensohn, F.; Letang, D.; Boyd, J.; Strapazzon, G.; Ellerton, J.; Brugger, H. The Avalanche Victim Resuscitation Checklist, a new concept for the management of avalanche victims. Resuscitation 2015, 91, e7–e8. [Google Scholar] [CrossRef]
- Donabedian, A. The quality of care. How can it be assessed? JAMA 1988, 260, 1743–1748. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| QI Nr | Indicator | Definition |
|---|---|---|
| Prior to the Avalanche Rescue Mission | ||
| QI 1 | Time between alarm at dispatch centre and arrival on scene (BS) | Time between emergency call at the dispatch centre and the arrival of the first organised rescue team on scene. |
| QI 2 | Time between accident and arrival on scene (BS) | Time between the accident and the arrival of the first organised rescue team on scene. |
| QI 3 | Burial time [10,11] (BS) | Time between the avalanche accident and the exposure of the face. |
| QI 4 | CPR by bystanders [10] | Proportion of victims without signs of life at extrication, for whom CPR was performed by companions, bystanders or first responders (e.g., ski patrollers) just after extrication. |
| Patient Assessment | ||
| QI 5 | Airway patency [10,11] | Proportion of long (>60 min) complete burial (USA-critical burial) victims whose airway patency was assessed at face exposure. |
| QI 6 | Documentation of air pocket [1] | Proportion of completely buried victims for whom the existence of an air pocket was documented and reported (air pocket: airways free of snow AND any space in front of mouth and nose). |
| QI 7 | ECG monitoring [11] | Proportion of victims without signs of life and who did not have clear signs of death *, for whom ECG monitoring was performed on site. |
| QI 8 | Site of temperature measurement [10] | Proportion of correct site of core temperature measurement (epitympanic in non-intubated victims not in cardiac arrest; esophageal in victims in cardiac arrest and/or intubated), amongst all victims who required temperature measurement, or when temperature was measured. |
| QI 9 | Temperature measurement on scene [10] | Proportion of victims whose core temperature was measured at the avalanche site compared to avalanche victims for whom core temperature should have been measured. |
| Patient Management | ||
| QI 10 | Airway management [10] | Proportion of transported victims who successfully underwent advanced airway management when it was attempted. |
| QI 11 | Occurrence of rescue collapse (EXP) | Proportion of patients who developed cardiac arrest during extrication and transport to hospital (i.e., until hospital admission). |
| QI 12 | Long-burial CPR start [11] | Proportion of victims without signs of life and without evident signs of death * with temperature <30 °C or burial time >60 min and patent or unknown airway for whom resuscitation (CPR) was initiated. |
| QI 13 | Chest compression and ventilation during resuscitation [11] | Proportion of avalanche victims in cardiac arrest who received CPR, including ventilation by the rescue team (except for victims with long burial AND obstructed airway). |
| QI 14 | Short-burial termination of CPR [10] | Proportion of victims with core temperature >30 °C AND asystole AND absence of reversible causes of cardiac arrest, for whom CPR was terminated according to guidelines (only for avalanche accidents with one victim in cardiac arrest). |
| QI 15 | Long-burial AND termination of CPR [10] | Proportion of victims with burial time >60 min AND asystole AND obstructed airway, for whom CPR was terminated or withheld. |
| QI 16 | Insulation [10,11] (BS) | Proportion of hypothermic victims insulated with whole-body insulation. |
| QI 17 | Use of avalanche checklist [1](RGP) | Proportion of victims without signs of life for whom an “avalanche victim resuscitation checklist” was filled out during the prehospital phase and transmitted to the hospital team at handover. |
| QI 18 | Completeness of documentation (RGP) | Proportion of interventions where all required information was documented (i.e., burial time, vital signs, airway patency if required, air pocket if required, ECG if required, core temperature if required, and serum potassium if required). |
| Transport | ||
| QI 19 | Adequate transport to ECLS [11] | Proportion of hypothermic patients transported to an ECLS centre according to guidelines. |
| In-hospital Management | ||
| QI 20 | Appropriate rewarming [10,11] | Proportion of hypothermic victims who received appropriate in-hospital rewarming. |
| QI 21 | Serum potassium [10] | Proportion of victims for whom serum potassium was measured when recommended by guidelines. |
| QI 22 | Hospital rewarming [10,11] | Proportion of hypothermic victims in cardiac arrest with a patent or unknown airway who were rewarmed to a core temperature >32 °C before a decision about declaration of death was made. |
| QI 23 | Adequate patients to ECMO or CPB (EXP) | Proportion of victims in CA who received ECMO or CPB (ECLS) therapy according to guidelines. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kottmann, A.; Pasquier, M.; Strapazzon, G.; Zafren, K.; Ellerton, J.; Paal, P. Quality Indicators for Avalanche Victim Management and Rescue. Int. J. Environ. Res. Public Health 2021, 18, 9570. https://doi.org/10.3390/ijerph18189570
Kottmann A, Pasquier M, Strapazzon G, Zafren K, Ellerton J, Paal P. Quality Indicators for Avalanche Victim Management and Rescue. International Journal of Environmental Research and Public Health. 2021; 18(18):9570. https://doi.org/10.3390/ijerph18189570
Chicago/Turabian StyleKottmann, Alexandre, Mathieu Pasquier, Giacomo Strapazzon, Ken Zafren, John Ellerton, and Peter Paal. 2021. "Quality Indicators for Avalanche Victim Management and Rescue" International Journal of Environmental Research and Public Health 18, no. 18: 9570. https://doi.org/10.3390/ijerph18189570