
First-Year Healthcare Resource Utilization Costs of Five Major Cancers in Japan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Statistical Analysis
3. Results
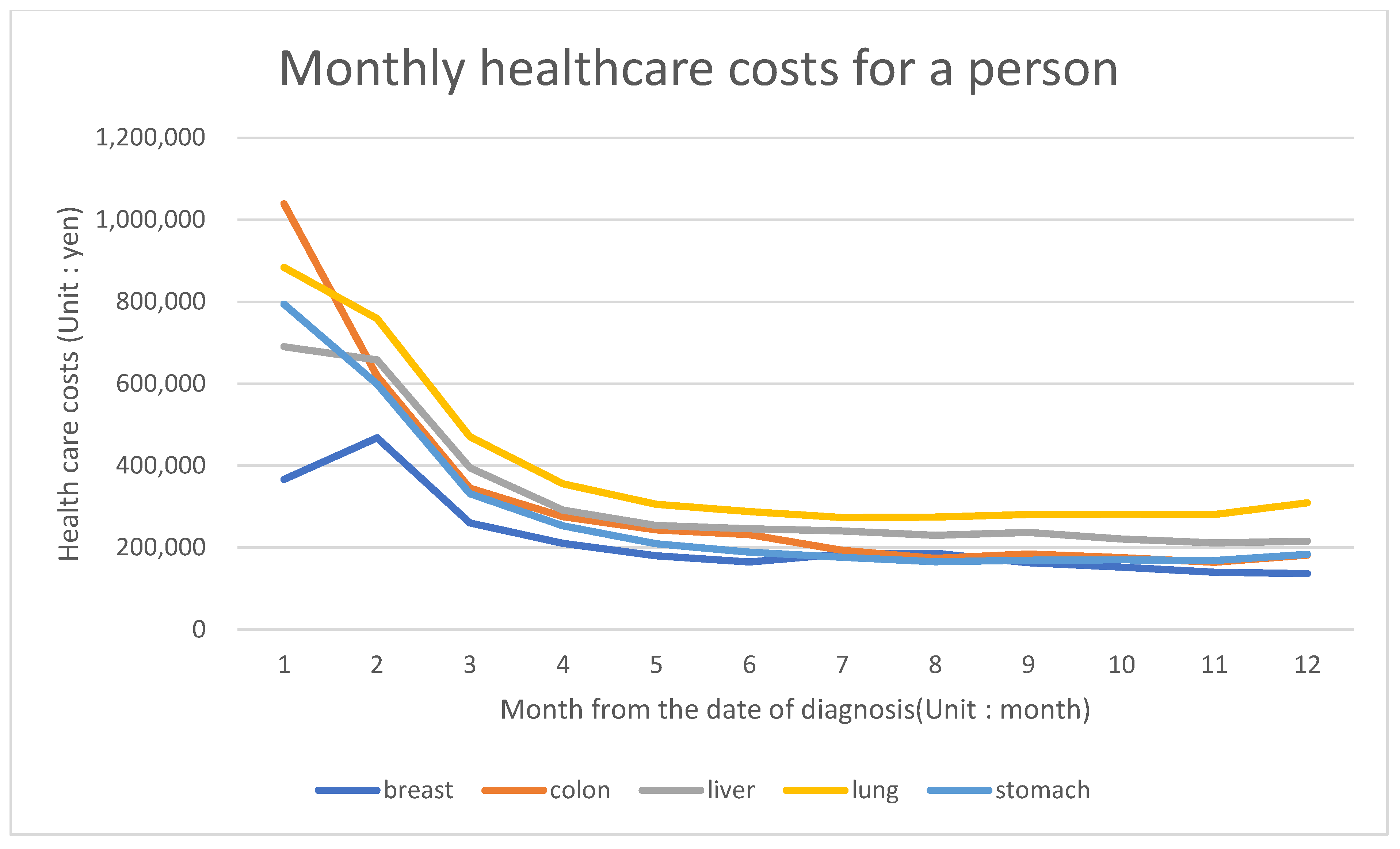
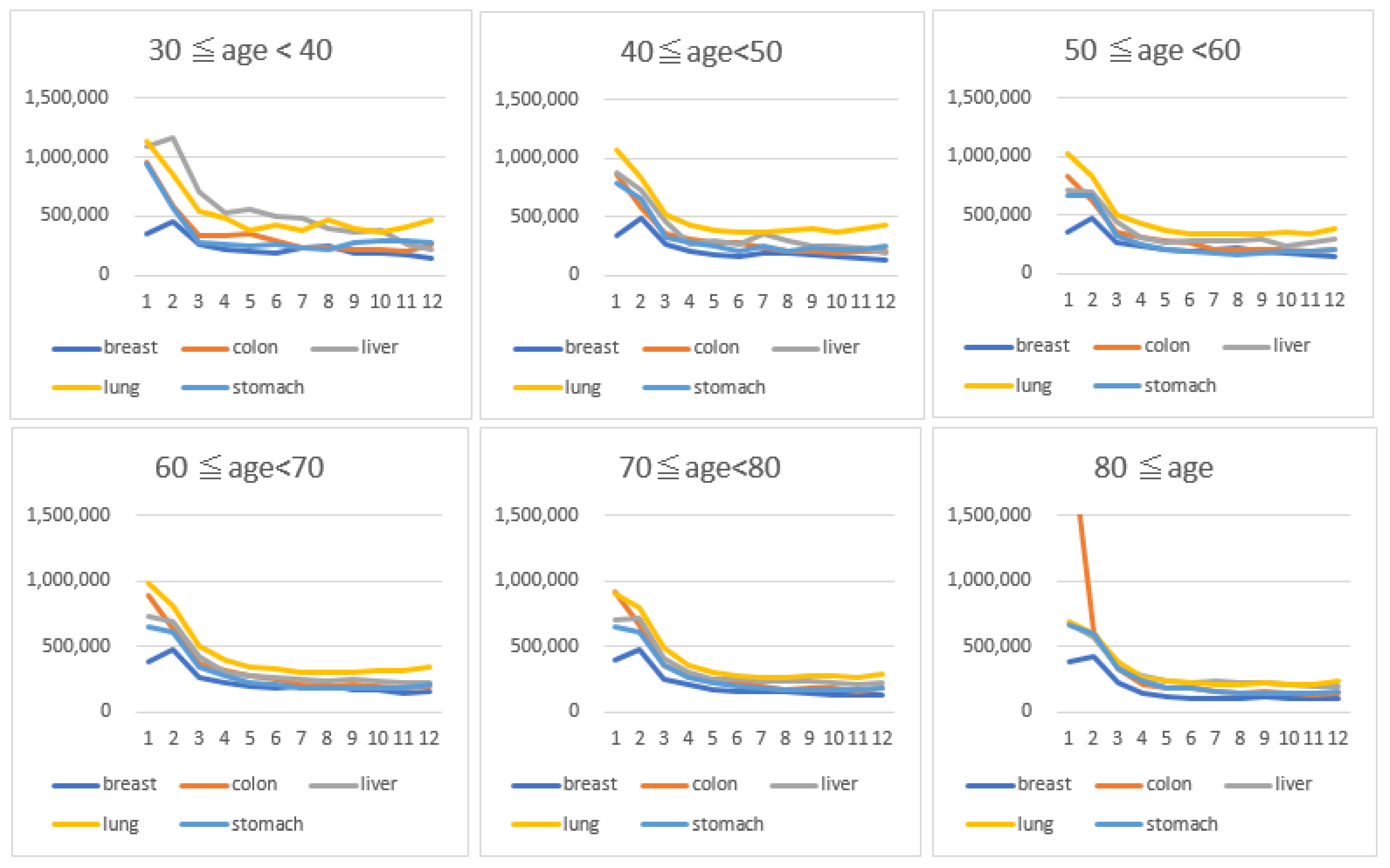
3.1. Costs in the First Year of Diagnosis
3.2. Number of Outpatient Visits in a Year
3.3. Average Hospitalization Duration
3.4. Statistical Variance of Cancer Care Costs
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Fitzmaurice, C.; Abate, D.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdel-Rahman, O.; Abdelalim, A.; Abdoli, A.; Abdollahpour, I.; Abdulle, A.S.M.; et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived with Disability, and Disability-Adjusted Life-Years for 29 Cancer Groups, 1990 to 2017: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 2019, 5, 1749–1768. [Google Scholar] [PubMed] [Green Version]
- Mariotto, A.B.; Yabroff, K.R.; Shao, Y.; Feuer, E.J.; Brown, M.L. Projections of the cost of cancer care in the United States: 2010–2020. J. Natl. Cancer Inst. 2011, 103, 117–128. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, R.; Peppercorn, J.; Sikora, K.; Zalberg, J.; Meropol, N.J.; Amir, E.; Khayat, D.; Boyle, P.; Autier, P.; Tannock, l.F.; et al. Delivering affordable cancer care in high-income countries. Lancet Oncol. 2011, 12, 933–980. [Google Scholar] [CrossRef]
- Aggarwal, A.; Ginsburg, O.; Fojo, T. Cancer economics, policy and politics: What informs the debate? Perspectives from the EU, Canada and US. J. Cancer Policy 2014, 2, 1–11. [Google Scholar] [CrossRef] [Green Version]
- National Cancer Center, Cancer Statistics in Japan. 2021. Available online: https://ganjoho.jp/public/qa_links/report/statistics/pdf/cancer_statistics_2021_data_E.pdf (accessed on 28 August 2021).
- International Agency for Research on Cancer, Japan. Available online: https://gco.iarc.fr/today/data/factsheets/populations/392-japan-fact-sheets.pdf (accessed on 28 August 2021).
- OECD. “Health Expenditure and Financing: Health Expenditure Indicators”, OECD Health Statistics (Database). 2021. Available online: https://doi.org/10.1787/data-00349-en (accessed on 28 August 2021).
- Higashi, T.; Nakamura, F.; Shibata, A.; Emori, Y.; Nishimoto, H. The national database of hospital-based cancer registries: A nationwide infrastructure to support evidence-based cancer care and cancer control policy in Japan. Jpn. J. Clin. Oncol. 2014, 44, 2–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iwamoto, M.; Nakamura, F.; Higashi, T. Monitoring and evaluating the quality of cancer care in Japan using administrative claims data. Cancer Sci. 2016, 107, 68–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yasunaga, H.; Ide, H.; Imamura, T.; Ohe, K. Impact of the Japanese Diagnosis Procedure Combination-based Payment System on cardiovascular medicine-related costs. Int. Heart J. 2005, 46, 855–866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Japan Health Policy Now. The Medical Service Fee System. Available online: https://japanhpn.org/en/section-7-2/ (accessed on 28 August 2021).
- Shiroiwa, T.; Fukuda, T.; Ikeda, S.; Takura, T.; Moriwaki, K. Development of an official guideline for the economic evaluation of drugs/medical devices in Japan. Value Health 2017, 20, 372–378. [Google Scholar] [CrossRef] [Green Version]
- Luengo-Fernandez, R.; Leal, J.; Gray, A.; Sullivan, R. Economic burden of cancer across the European Union: A population-based cost analysis. Lancet Oncol. 2013, 14, 1165–1174. [Google Scholar] [CrossRef]
- Blakely, T.; Atkinson, J.; Kvizhinadze, G.; Wilson, N.; Davies, A.; Clarke, P. Patterns of cancer care costs in a country with detailed individual data. Med. Care 2015, 53, 302–309. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldsbury, D.E.; Yap, S.; Weber, M.F.; Veerman, L.; Rankin, N.; Banks, E.; Kanfell, K.; O’Connell, D.L. Health services costs for cancer care in Australia: Estimates from the 45 and up study. PLoS ONE 2018, 13, e0201552. [Google Scholar] [CrossRef] [PubMed]
- Damm, O.; Hodek, J.M.; Greiner, W. Methodological standards for cost-of-illness studies using breast cancer, prostate cancer and colon cancer as an example. Z. Evid. Fortbild. Qual. Gesundhwes. 2009, 103, 305–316. [Google Scholar] [CrossRef] [PubMed]
- Kriza, C.; Emmert, M.; Wahlster, P.; Niederländer, C.; Kolominsky-Rabas, P. Cost of illness in colorectal cancer: An international review. Pharmacoeconomics 2013, 31, 577–588. [Google Scholar] [CrossRef]
- National Cancer Center. Cancer Mortality Rate. 2018. Available online: https://ganjoho.jp/reg_stat/statistics/stat/summary.html (accessed on 1 July 2021).
- Ellis, P.M.; Vandermeer, R. Delays in the diagnosis of lung cancer. J. Thorac. Dis. 2011, 3, 183–188. [Google Scholar]
- Yajima, S.; Shimizu, H.; Sakamaki, H.; Ikeda, S.; Ikegami, N.; Murayama, J.I. Real-world cost analysis of chemotherapy for colorectal cancer in Japan: Detailed costs of various regimens during the entire course of chemotherapy. BMC Health Serv. Res. 2016, 16, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fine, M.J.; Pratt, H.M.; Obrosky, D.S.; Lave, J.R.; Mclntosh, L.J.; Singer, E.D.; Coley, C.M.; Kapoor, W.N. Relation between length of hospital stay and costs of care for patients with community-acquired pneumonia. Am. J. Med. 2000, 109, 378–385. [Google Scholar] [CrossRef]
- OECD. Average Length of Stay in Hospitals. Available online: https://www.oecd-ilibrary.org/sites/0d8bb30a-en/index.html?itemId=/content/component/0d8bb30aen#:~:text=In%202017%2C%20the%20aveage%20length,over%2016%20days%20per%20patient (accessed on 1 July 2021).
- Muramatsu, N.; Liang, J. Hospital length of stay in the United States and Japan: A case study of myocardial infarction patients. Int. J. Health Serv. 1999, 29, 189–209. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Mikami, M.; Katabuchi, H.; Kato, S.; Kaneuchi, M.; Takahashi, M.; Nakai, H.; Nagase, S.; Niikura, H.; Mandai, M.; et al. Quality indicators for cervical cancer care in Japan. J. Gynecol. Oncol. 2018, 29, e83. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Liver | Stomach | Colorectal | Lung | Breast | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| n | 15,808 | 69,695 | 90,912 | 70,264 | 58,019 | |||||
| Mean age (SD) | 72.7 (10.2) | 72.2 (10.4) | 70.2 (11.5) | 71.7 (10.4) | 60.6 (14.1) | |||||
| Stage (%) | ||||||||||
| 0 | - | - | - | 23,086 | 25.4 | 156 | 0.2 | 7584 | 13.1 | |
| I | 7375 | 46.7 | 44,312 | 63.6 | 17,542 | 19.3 | 28,310 | 40.3 | 23,997 | 41.4 |
| II | 4156 | 26.3 | 6292 | 9 | 17,737 | 19.5 | 5708 | 8.1 | 17,320 | 29.9 |
| III | 2665 | 16.9 | 6935 | 10 | 17,905 | 19.7 | 11,753 | 16.7 | 5938 | 10.2 |
| IV | 1274 | 8.1 | 11,205 | 16.1 | 13,540 | 14.9 | 23,173 | 33 | 2965 | 5.1 |
| unknown | 338 | 2.1 | 951 | 1.4 | 1102 | 1.2 | 1164 | 1.7 | 215 | 0.4 |
| Age group (%) | ||||||||||
| 0–29 | 17 | 0.1 | 66 | 0.1 | 138 | 0.2 | 50 | 0.1 | 219 | 0.4 |
| 30–39 | 49 | 0.3 | 497 | 0.7 | 862 | 1 | 312 | 0.4 | 2678 | 4.6 |
| 40–49 | 331 | 2.1 | 1785 | 2.6 | 4120 | 4.5 | 1681 | 2.4 | 12,939 | 22.3 |
| 50–59 | 1183 | 7.5 | 4919 | 7.1 | 9947 | 10.9 | 5268 | 7.5 | 11,685 | 20.1 |
| 60–69 | 3962 | 25.1 | 18,317 | 26.3 | 25,719 | 28.3 | 20,024 | 28.5 | 13,947 | 24 |
| 70–79 | 5886 | 37.2 | 26,431 | 37.9 | 30,353 | 33.4 | 27,856 | 39.6 | 10,780 | 18.6 |
| 80– | 4380 | 27.7 | 17,680 | 25.4 | 19,773 | 21.8 | 15,073 | 21.5 | 5771 | 10 |
| Types of treatment * | ||||||||||
| Surgery | 12,887 | 81.5 | 59,369 | 85.2 | 81,231 | 89.4 | 39,005 | 55.5 | 51,245 | 88.3 |
| Chemotherapy | 7106 | 45 | 17,929 | 25.7 | 27,848 | 30.6 | 32,065 | 45.6 | 19,826 | 34.2 |
| Radiation | 1199 | 7.6 | 3106 | 4.5 | 4507 | 5 | 16,746 | 23.8 | 21,262 | 36.6 |
| Unit | 0 | I | II | III | IV | Unknown | All Stages | Total (Outpatient + Inpatient) | |
|---|---|---|---|---|---|---|---|---|---|
| Liver (n = 15,808) | Outpatient | 300,931 | 329,004 | 219,278 | 87,479 | 78,362 | 287,589 | ||
| 618,592 | 631,108 | 500,150 | 517,268 | 284,751 | 586,611 | 2,078,843 | |||
| Inpatient | 1,452,499 | 1,819,571 | 2,159,867 | 1,304,000 | 1,113,121 | 1,623,739 | 2,671,490 | ||
| 1,826,721 | 2,284,767 | 2,618,544 | 1,855,085 | 1,918,391 | 2,084,879 | ||||
| Stomach (n = 69,695) | Outpatient | 185,434 | 372,081 | 569,867 | 364,153 | 62,096 | 214,528 | ||
| 292,830 | 521,520 | 790,280 | 1,071,880 | 320,411 | 488,600 | 1,839,530 | |||
| Inpatient | 918,689 | 2,011,916 | 2,290,073 | 1,876,265 | 916,390 | 1,509,190 | 2,421,138 | ||
| 1,654,133 | 2,487,039 | 2,754,346 | 2,253,904 | 1,456,846 | 1,932,538 | ||||
| Colorectal (n = 90,912) | Outpatient | 93,885 | 204,391 | 242,377 | 702,285 | 921,884 | 40,656 | 222,396 | |
| 230,635 | 323,130 | 441,633 | 852,293 | 1,691,874 | 408,588 | 631,870 | 2,058,540 | ||
| Inpatient | 371,859 | 1,632,299 | 1,872,095 | 2,009,314 | 2,345,584 | 1,141,618 | 1,630,101 | 2,713,002 | |
| 728,364 | 1,849,647 | 2,361,973 | 3,198,947 | 2,875,019 | 1,668,914 | 2,081,132 | |||
| Lung (n = 70,264) | Outpatient | 155,190 | 255,066 | 391,025 | 537,181 | 383,286 | 82,491 | 317,223 | |
| 210,582 | 414,857 | 683,542 | 1,231,550 | 1,681,510 | 401,530 | 990,358 | 2,508,789 | ||
| Inpatient | 1,700,838 | 1,899,493 | 2,432,563 | 2,518,769 | 1,910,023 | 937,621 | 1,979,050 | 3,366,480 | |
| 1,846,962 | 2,069,106 | 2,785,343 | 2,849,596 | 2,460,904 | 1,438,782 | 2,376,122 | |||
| Breast (n = 58,019) | Outpatient | 233,410 | 590,118 | 809,373 | 1,367,112 | 1,313,672 | 265,459 | 647,501 | |
| 386,271 | 728,104 | 1,076,681 | 1,537,909 | 2,239,234 | 800,032 | 947,850 | 1,559,274 | ||
| Inpatient | 726,813 | 744,886 | 928,522 | 1,085,048 | 809,365 | 376,633 | 820,950 | 2,012,925 | |
| 919,149 | 970,355 | 1,133,881 | 1,353,685 | 1,253,190 | 676,353 | 1,065,075 |
| Unit | 0 | I | II | III | IV | Unknown | Total | |
|---|---|---|---|---|---|---|---|---|
| Liver | Outpatient | - | 12 | 13 | 9 | 3 | 4 | 12 |
| 14 | 14 | 11 | 8 | 7 | 13 | |||
| Inpatient | - | 2 | 2 | 2 | 1 | 1 | 2 | |
| 2 | 2 | 2 | 2 | 2 | 2 | |||
| Stomach | Outpatient | - | 10 | 15 | 18 | 12 | 3 | 11 |
| 12 | 16 | 19 | 15 | 8 | 13 | |||
| Inpatient | - | 1 | 1 | 2 | 2 | 1 | 1 | |
| 2 | 2 | 2 | 3 | 2 | 2 | |||
| Colorectal | Outpatient | 5 | 11 | 12 | 17 | 19 | 2 | 11 |
| 8 | 13 | 14 | 18 | 19 | 8 | 14 | ||
| Inpatient | 1 | 1 | 1 | 2 | 2 | 1 | 1 | |
| 1 | 2 | 2 | 2 | 3 | 2 | 2 | ||
| Lung | Outpatient | 8 | 12 | 17 | 19 | 11 | 4 | 13 |
| 10 | 14 | 19 | 21 | 15 | 9 | 15 | ||
| Inpatient | 1 | 1 | 2 | 3 | 2 | 1 | 2 | |
| 1 | 2 | 3 | 3 | 3 | 2 | 2 | ||
| Breast | Outpatient | 16 | 25 | 27 | 37 | 22 | 10 | 25 |
| 21 | 26 | 30 | 37 | 24 | 16 | 27 | ||
| Inpatient | 1 | 1 | 1 | 1 | 1 | 1 | 1 | |
| 1 | 1 | 2 | 2 | 1 | 1 | 1 |
| 0 | I | II | III | IV | Unknown | Total | |
|---|---|---|---|---|---|---|---|
| Liver | - | 17 | 23 | 34 | 28 | 20 | 21 |
| 25 | 32 | 42 | 36 | 32 | 31 | ||
| Stomach | - | 12 | 23 | 29 | 34 | 22 | 16 |
| 19 | 34 | 40 | 43 | 32 | 27 | ||
| Colorectal | 4 | 16 | 22 | 24 | 34 | 23 | 18 |
| 9 | 23 | 31 | 33 | 43 | 33 | 26 | |
| Lung | 10 | 12 | 28 | 46 | 37 | 19 | 22 |
| 14 | 18 | 39 | 53 | 48 | 31 | 36 | |
| Breast | 8 | 8 | 10 | 13 | 10 | 6 | 9 |
| 10 | 11 | 14 | 19 | 23 | 13 | 13 |
| Liver | Stomach | Colorectal | Lung | Breast | |
|---|---|---|---|---|---|
| Grand mean | 2,605,715 | 2,493,774 | 2,823,430 | 3,311,205 | 2,118,407 |
| Facility level (SD) | 904,880 | 2,589,735 | 4,077,456 | 485,880 | 2,015,123 |
| Individual level (SD) | 2,398,249 | 39,439,543 | 41,150,914 | 2,513,716 | 1,609,051 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Watanabe, T.; Goto, R.; Yamamoto, Y.; Ichinose, Y.; Higashi, T. First-Year Healthcare Resource Utilization Costs of Five Major Cancers in Japan. Int. J. Environ. Res. Public Health 2021, 18, 9447. https://doi.org/10.3390/ijerph18189447
Watanabe T, Goto R, Yamamoto Y, Ichinose Y, Higashi T. First-Year Healthcare Resource Utilization Costs of Five Major Cancers in Japan. International Journal of Environmental Research and Public Health. 2021; 18(18):9447. https://doi.org/10.3390/ijerph18189447
Chicago/Turabian StyleWatanabe, Tomone, Rei Goto, Yoko Yamamoto, Yuichi Ichinose, and Takahiro Higashi. 2021. "First-Year Healthcare Resource Utilization Costs of Five Major Cancers in Japan" International Journal of Environmental Research and Public Health 18, no. 18: 9447. https://doi.org/10.3390/ijerph18189447