
Development and Comparison of Dengue Vulnerability Indices Using GIS-Based Multi-Criteria Decision Analysis in Lao PDR and Thailand

 ,
,  , ,
, ,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
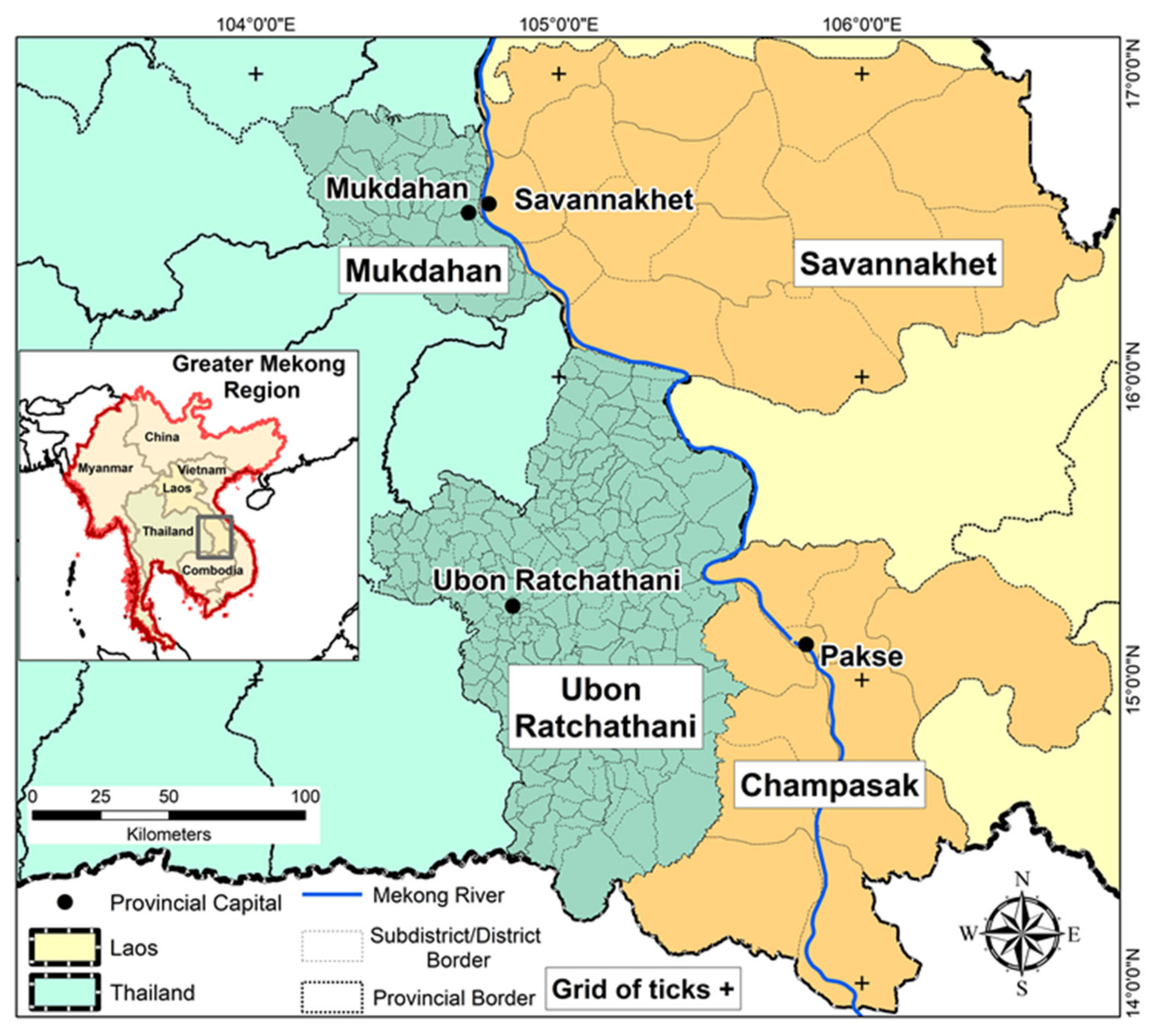
2.1. Study Area
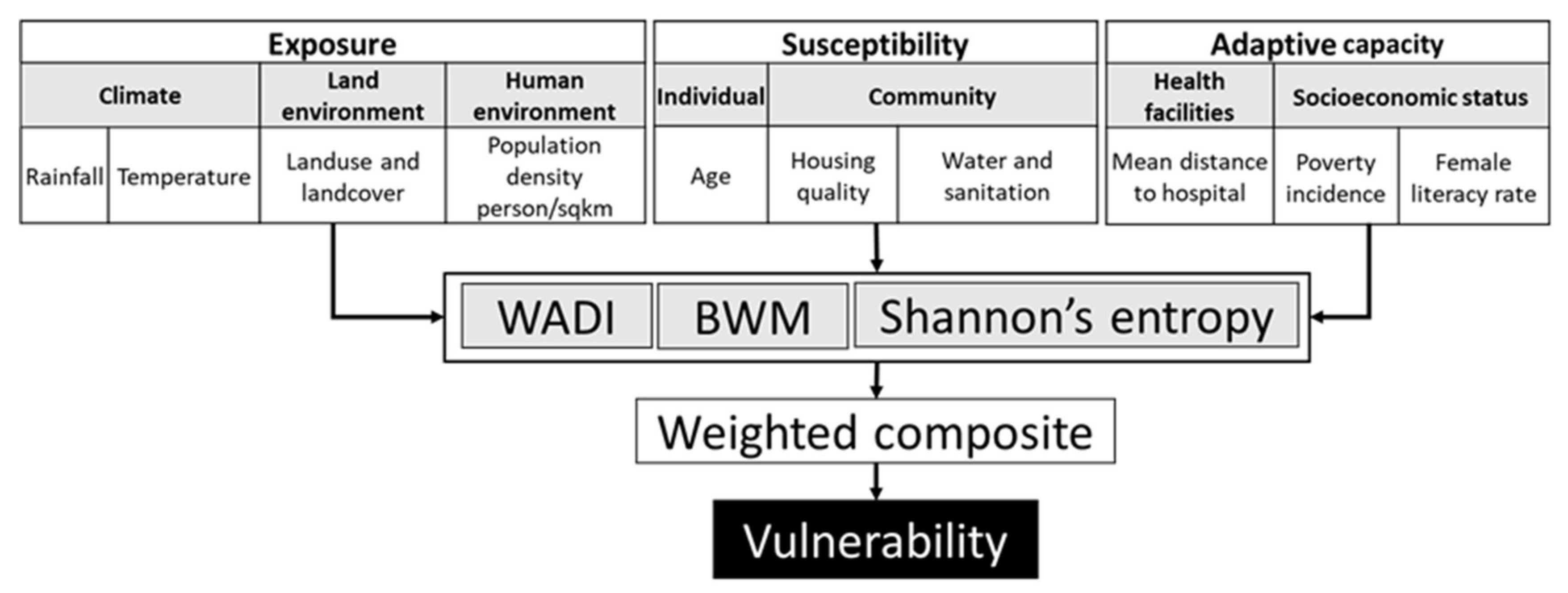
2.2. Conceptual Framework
2.3. Data Collection
2.4. Determinants and Indicators of Vulnerability Index
2.4.1. Exposure
2.4.2. Susceptibility
2.4.3. Adaptive Capacity
2.5. Index Construction
2.5.1. Index Based on Water Associated Disease Index (DVIWADI)
2.5.2. Index Based on Best-Worst Method—BWM (DVIBWM)
- i.
- Define a set of decision indicators that will be used to derive a decision process, where indicates the multiple indicators of each determinant (exposure, susceptibility, and adaptive capacity) (Table 2).
- ii.
- Define the best (most important) and the worst (least important) indictor for each determinant.
- iii.
- Experts determine the preference of the best and worst indicator over all the other indicators using a number between 1 to 9 (1 = Worst and 9 = Best). The resultant vector of Best-to-Others would bewhere indicates the preference of the best criterion B over criterion j, and = 1.
- iv.
- Preference of all the criteria over the worst criterion was determined using a value between 1 and 9. The resultant vector for Others-to-Worst would bewhere indicates the preference of the criterion j over the worst criterion W and =1.
- v.
- Estimate the optimal weights The optimal weight for the indicator is the one where, for each pair of we have and . To find an optimal solution, the maximum absolute differences and for all j is minimized. Based on the non-negativity characteristic and sum condition of the weights, the following problem was also formulated:s.t., for all .Hence, the problem in Equation (2) can be transferred to the linear problem:
2.5.3. Index Based on Shannon’s Entropy—SE (DVISE)
2.6. Validation
3. Results
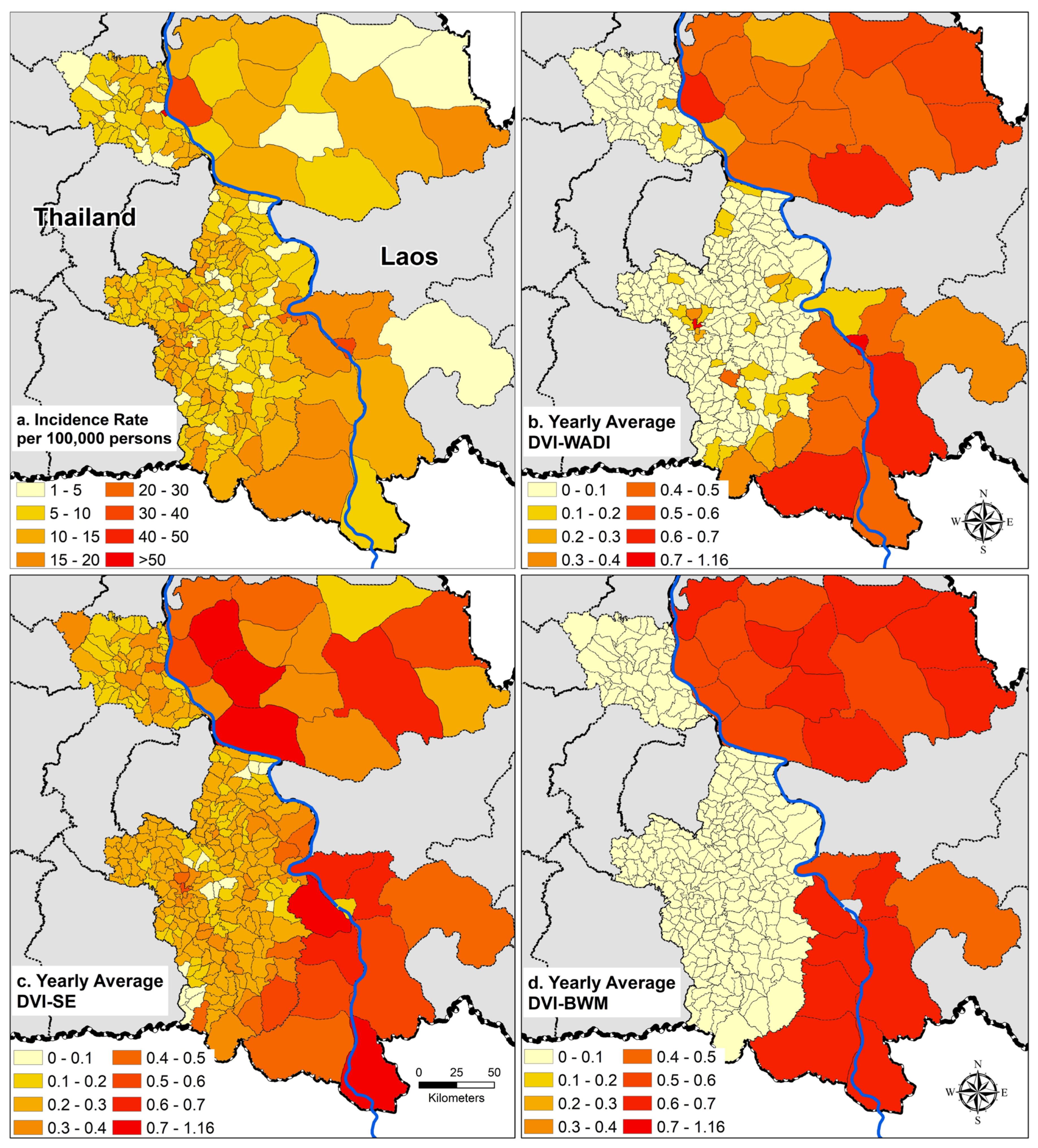
3.1. Dengue Incidence
3.2. Associations between Vulnerability Indices and Dengue Incidence
3.2.1. Laos
3.2.2. Thailand
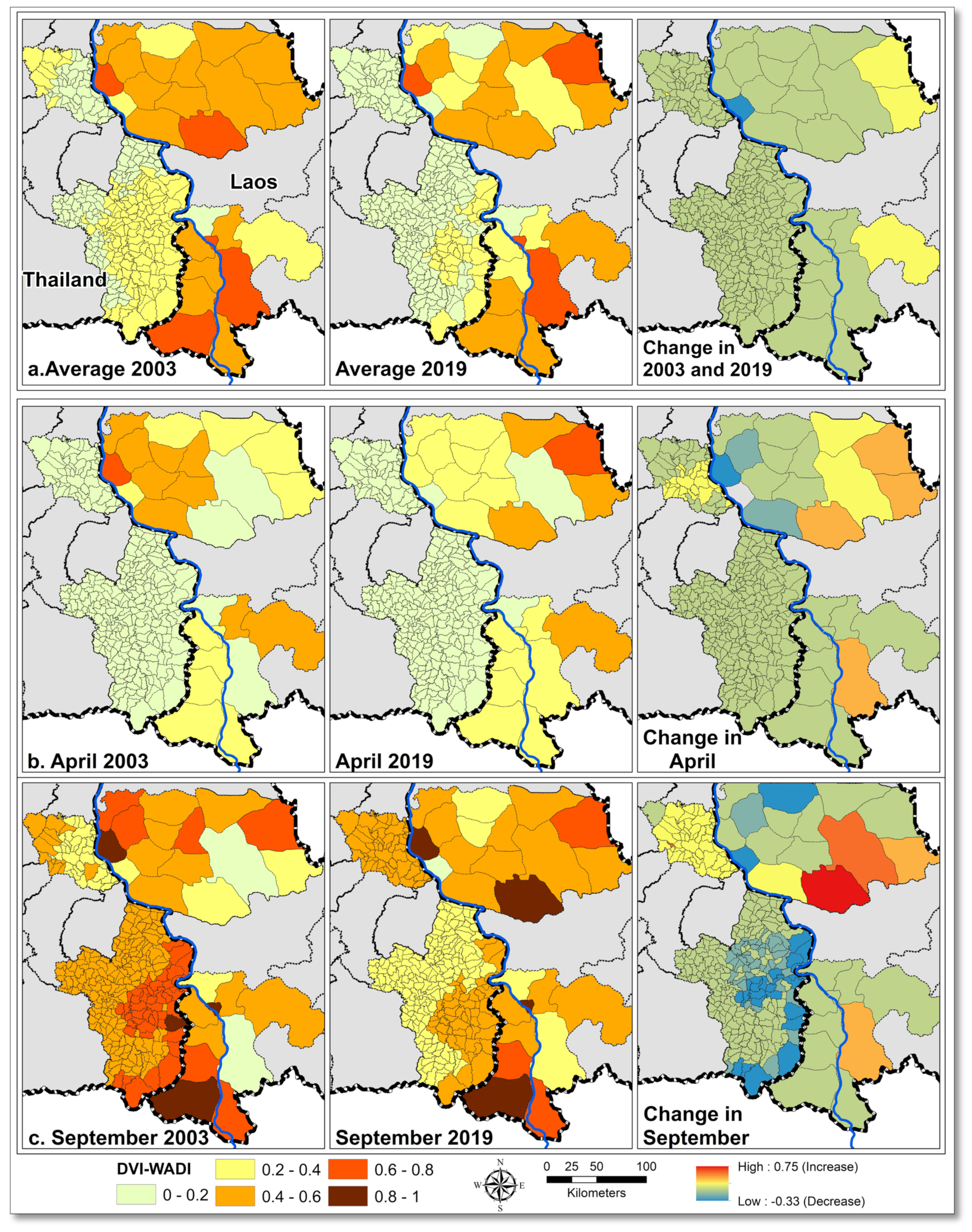
3.3. Spatiotemporal Variation of Dengue Vulnerability
3.3.1. Spatial Differences
3.3.2. Temporal Differences
3.3.3. Change in DVIWADI Components
4. Discussion
4.1. DVIWADI Spatial Variations
4.2. Change in DVIWADI during 2003–2019
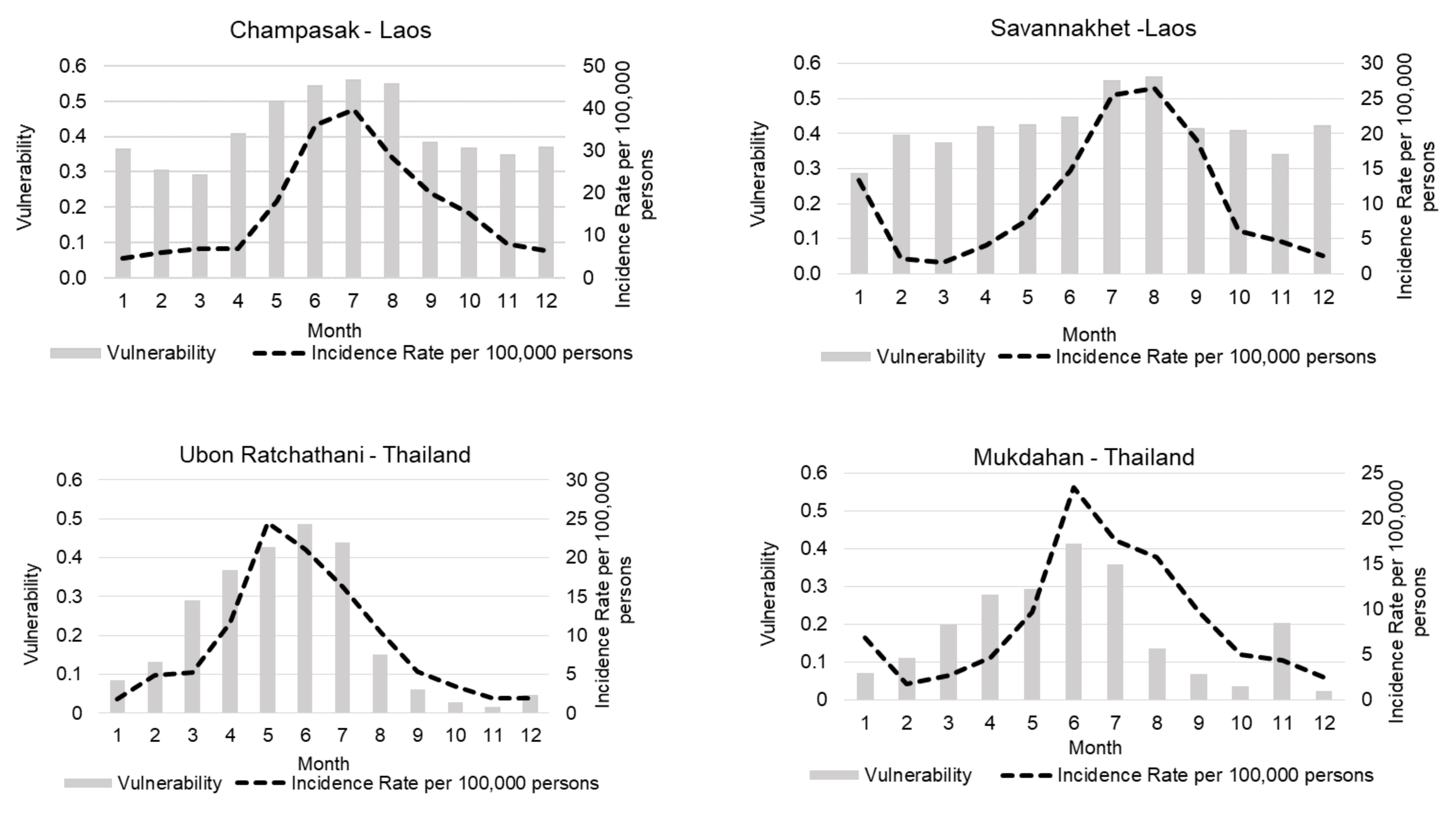
4.3. DVIWADI Temporal Variations
4.4. Change in Determinants of DVIWADI
- i.
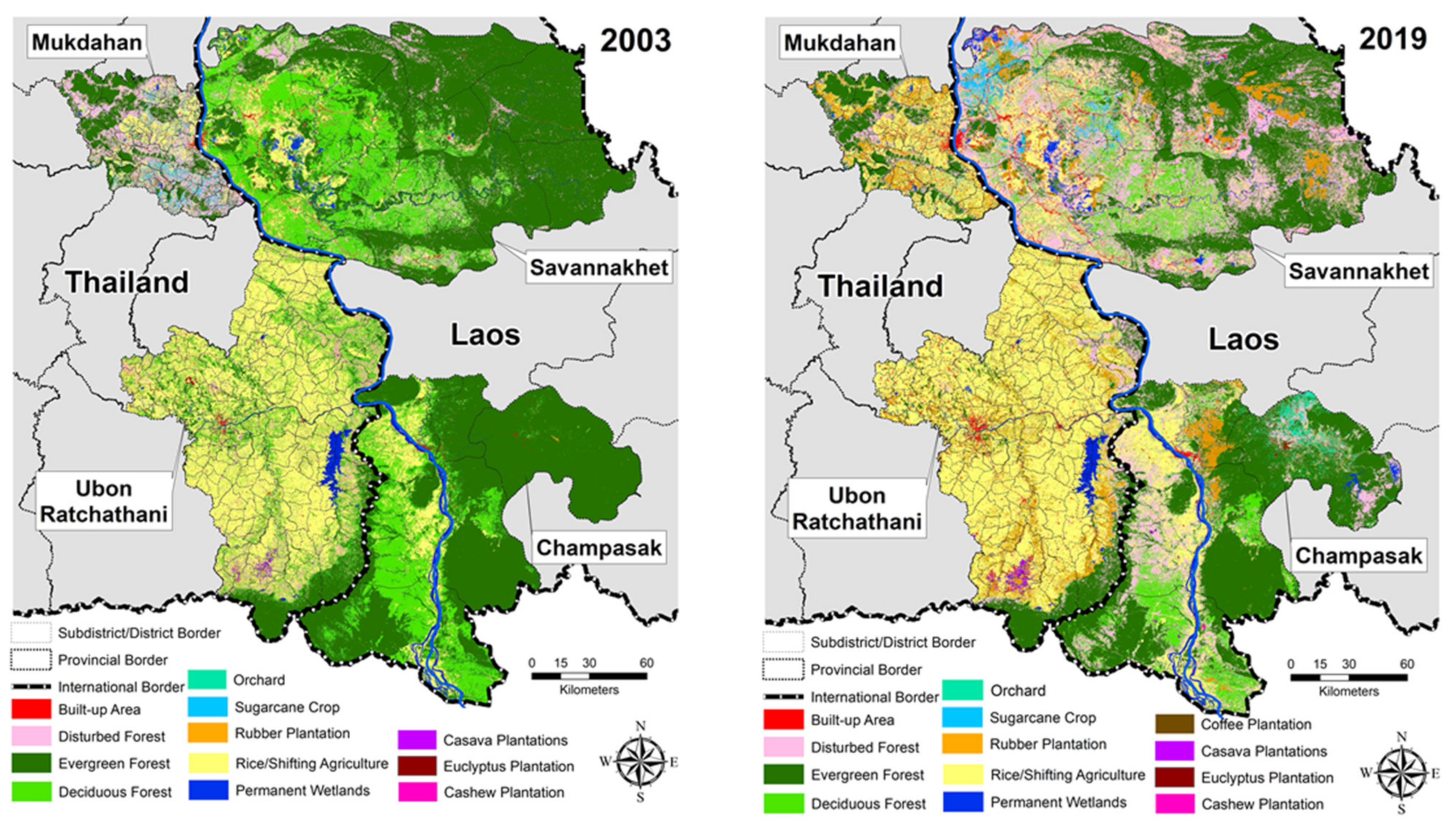
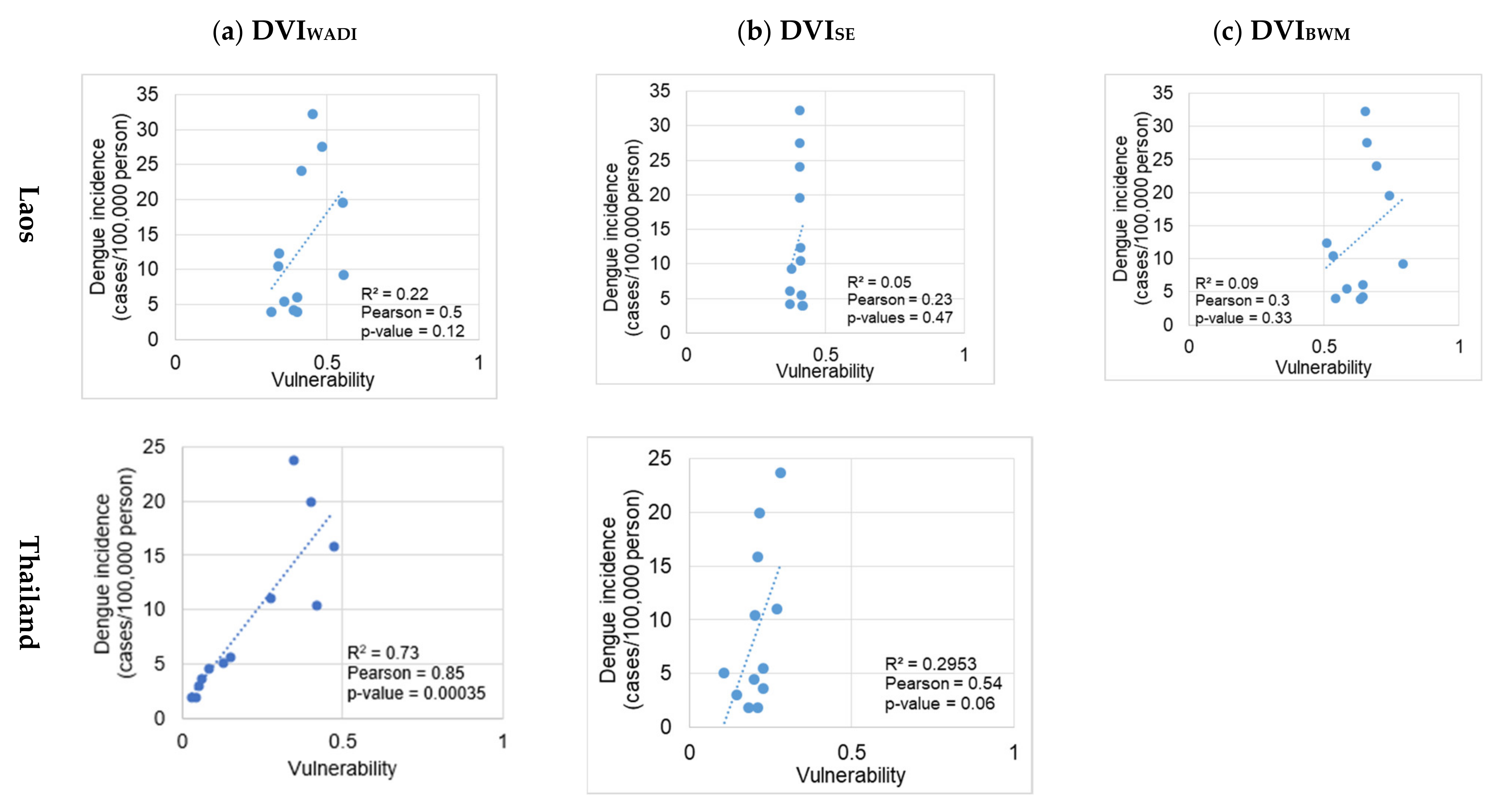
- Exposure: All four indicators of exposure including land cover, temperature, rainfall, and population density changed over the study period. An increase in exposure/risk with landcover and climate is also reported in other South East Asian countries such as Malaysia [68], Vietnam [72], Indonesia [73], and Timor-Leste [74]. The increasing risk with climate is also well reported for different parts of Thailand [21,51,75,76,77,78]. On average, exposure contributed 56% to the DVIWADI score in Thailand and only 11% in Laos. The relatively higher contribution of exposure to dengue vulnerability in Thailand could be a reason for the overall high correlation between DVIWADI and dengue incidence (R2 = 0.73 and r = 0.85), even if data for susceptibility and adaptive capacity determinants were limited (Figure 4). On average, exposure contributed 56% to the DVIWADI score in Thailand and 11% in Laos. Both countries went through similar environmental changes, but there were marked differences in population density; for example, population densities remained low in Savannakhet (below 100 person/km2 between 2003–2019). The low exposure in Laos can be an artifact because of larger spatial units considered as compared to Thailand where subdistricts are much smaller than districts in Laos.
- ii.
- Susceptibility: People’s susceptibility to dengue decreased in both countries with improved water and hygiene facilities (Supplementary File, Figure S5). In Laos, the population with improved access to water and sanitation increased by 18% between 2005 and 2010 alone and from 45% to 63% nationwide, exceeding the Millennium Development Goals target of 54% [79]. Similarly, in Thailand, nearly 93% of the population has access to improved hygiene and 96% to drinking water [80]. In Laos, susceptibility on average contributed 47% and in Thailand, only 17% to the DVIWADI score, which underlines the different living conditions and vulnerable population age groups in the study sites of these two countries. The relatively higher contribution of susceptibility and limited data (censuses in 2005 and 2015) in Laos might be the reason for an overall lower correlation between DVIWADI and dengue incidence (R2 = 0.22 and r = 0.5) (Figure 4).
- iii.
- Adaptive capacity: In Laos, the adaptive capacity on average contributed 42% to total DVIWADI score and in Thailand only 27%. Poverty and female literacy rates were the most critical indicators of adaptive capacity that can effectively help to reduce the dengue burden. Research from southern Brazil [81] reported 23–32% reduction in dengue cases with an increase in mean income from approximately USD 100–200 to USD 200–300. Poverty incidence rates decreased in Laos provinces between 2005 and 2015 (Supplementary File, Figure S5). In Champasak, poverty incidence dropped to 21% from 28% and in Savannakhet from 49.3% to 32.2%. In Thailand, the poverty incidence rate also decreased between 2003 and 2019, from 8% to 1.3% in Mukdahan and from 2.5% to 1.1% in Ubon Ratchathani [24]. The average female literacy rate between 2005–2015 increased from 44.6% to 48.7% in Champasak province and from 38.8% to 42.6% in Savannakhet province [23]. The average female literacy rates in Mukdahan and Ubon Ratchathani in 2000 were 86% and 90%, respectively, and increased to 95% in both provinces in 2019 [24]. The average distance to a hospital or health care facility is a crucial indicator of community adaptive capacity. However, this distance remained unchanged in Laos between the 2005 and 2015 censuses [23]. In Laos, except for urban centers, the minimum average distance to the nearest health facility was 10–20 kilometers. The lack of geographical coverage of the health system was due to a sparse population in the country, with approximately 80% of the population living in rural areas and engaged in agriculture [82]. The current health facility network in Thailand showed good coverage, with the nearest health care facility between 1 and 10 kilometers.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bhatt, S.; Gething, P.W.; Brady, O.J.; Messina, J.P.; Farlow, A.W.; Moyes, C.L.; Drake, J.M.; Brownstein, J.S.; Hoen, A.G.; Sankoh, O.; et al. The global distribution and burden of dengue. Nature 2013, 496, 504–507. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Dengue and Severe Dengue. Available online: www.who.int/mediacentre/factsheets/fs117/en/index.html (accessed on 12 June 2018).
- Acharya, B.K.; Cao, C.X.; Lakes, T.; Chen, W.; Naeem, S.; Pandit, S. Modeling the spatially varying risk factors of dengue fever in Jhapa district, Nepal, using the semi-parametric geographically weighted regression model. Int. J. Biometeorol. 2018, 62, 1973–1986. [Google Scholar] [CrossRef]
- Khormi, H.M.; Kumar, L.; Elzahrany, R.A. Modeling spatio-temporal risk changes in the incidence of dengue fever in Saudi Arabia: A geographical information system case study. Geospat. Health 2011, 6, 77–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Misslin, R.; Telle, O.; Daudé, E.; Vaguet, A.; Paul, R.E. Urban climate versus global climate change—What makes the difference for dengue? Ann. N. Y. Acad. Sci. 2016, 1382, 56–72. [Google Scholar] [CrossRef] [PubMed]
- Wu, P.C.; Lay, J.G.; Guo, H.R.; Lin, C.Y.; Lung, S.C.; Su, H.J. Higher temperature and urbanization affect the spatial patterns of dengue fever transmission in subtropical Taiwan. Sci. Total Environ. 2009, 407, 2224–2233. [Google Scholar] [CrossRef]
- WHO. Dengue Guidelines for Diagnosis, Treatment, Prevention and Control; World Health Organization (WHO) and the Special Programme for Research and Training in Tropical Diseases (TDR): Lyon, France, 2009; Volume 409, ISBN 9789241547. Available online: https://www.who.int/tdr/publications/documents/dengue-diagnosis.pdf (accessed on 5 September 2021).
- Bedran-Martins, A.M.; Lemos, M.C.; Philippi, A. Relationship between subjective well-being and material quality of life in face of climate vulnerability in NE Brazil. Clim. Chang. 2018, 147, 283–297. [Google Scholar] [CrossRef]
- Lippi, C.A.; Stewart-Ibarra, A.M.; Muñoz, Á.G.; Borbor-Cordova, M.J.; Mejía, R.; Rivero, K.; Castillo, K.; Cárdenas, W.B.; Ryan, S.J. The social and spatial ecology of dengue presence and burden during an outbreak in Guayaquil, Ecuador, 2012. Int. J. Environ. Res. Public Health 2018, 15, 827. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Yang, J.; Luo, L.; Yang, Z.; Liu, Q. Who is vulnerable to dengue fever? A community survey of the 2014 outbreak in Guangzhou, China. Int. J. Environ. Res. Public Health 2016, 13, 712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Füssel, H.M. Vulnerability: A generally applicable conceptual framework for climate change research. Glob. Environ. Chang. 2007, 17, 155–167. [Google Scholar] [CrossRef]
- Fullerton, L.; Dickin, S.; Schuster-Wallace, C.J. Mapping Global Vulnerability to Dengue Using the Water Associated Disease Index Waste to Wealth View Project; United Nations University: Hamilton, ON, Canada, 2014; ISBN 9789280860450. [Google Scholar]
- Moore, M.; Gelfeld, B.; Okunogbe, A.; Paul, C. Identifying Future Disease Hot Spots: Infectious Disease Vulnerability Index; RAND Corporation: Santa Monica, CA, USA, 2017; Volume 6, ISBN 9780833095749. [Google Scholar]
- Dickin, S.K.; Schuster-Wallace, C.J.; Elliott, S.J. Developing a Vulnerability Mapping Methodology: Applying the Water-Associated Disease Index to Dengue in Malaysia. PLoS ONE 2013, 8, e63584. [Google Scholar] [CrossRef] [Green Version]
- Pham, N.T.T.; Nguyen, C.T.; Vu, H.H. Assessing and modelling vulnerability to dengue in the Mekong Delta of Vietnam by geospatial and time-series approaches. Environ. Res. 2020, 186, 109545. [Google Scholar] [CrossRef] [PubMed]
- Dickin, S.K.; Schuster-Wallace, C.J. Assessing changing vulnerability to dengue in northeastern Brazil using a water-associated disease index approach. Glob. Environ. Chang. 2014, 29, 155–164. [Google Scholar] [CrossRef]
- Henry, S.; Mendonça, F.d.A. Past, present, and future vulnerability to dengue in jamaica: A spatial analysis of monthly variations. Int. J. Environ. Res. Public Health 2020, 17, 3156. [Google Scholar] [CrossRef] [PubMed]
- Tsheten, T.; Clements, A.C.A.; Gray, D.J.; Wangdi, K. Dengue risk assessment using multicriteria decision analysis: A case study of Bhutan. PLoS Negl. Trop. Dis. 2021, 15, e0009021. [Google Scholar] [CrossRef]
- Ali, S.A.; Ahmad, A. Mapping of mosquito-borne diseases in Kolkata Municipal Corporation using GIS and AHP based decision making approach. Spat. Inf. Res. 2019, 27, 351–372. [Google Scholar] [CrossRef]
- Dom, N.C.; Ahmad, A.H.; Latif, Z.A.; Ismail, R. Application of geographical information system-based analytical hierarchy process as a tool for dengue risk assessment. Asian Pac. J. Trop. Dis. 2016, 6, 928–935. [Google Scholar] [CrossRef]
- Jeefoo, P.; Tripathi, K.N. Dengue risk zone index (DRZI) for mapping dengue risk areas. Int. J. Geoinform. 2011, 7, 53–62. [Google Scholar]
- Cardona, O.D.; Van Aalst, M.K.; Birkmann, J.; Fordham, M.; Mc Gregor, G.; Rosa, P.; Pulwarty, R.S.; Schipper, E.L.F.; Sinh, B.T.; Décamps, H.; et al. Determinants of risk: Exposure and vulnerability. In Managing the Risks of Extreme Events and Disasters to Advance Climate Change Adaptation; A Special Report of Working Groups I and II of the Intergovernmental Panel on Climate Change (IPCC); Cambridge University Press: Cambridge, UK, 2012; pp. 65–108. ISBN 9781107025066. [Google Scholar] [CrossRef] [Green Version]
- Lao Statistics Bureau Lao Decide Info. Available online: http://www.decide.la/%0A (accessed on 15 January 2019).
- National Statistical Office of Thailand Registration Statistics System Official Statistics Registration Systems (Thailand). Available online: https://stat.bora.dopa.go.th/new_stat/webPage/statByYear.php (accessed on 15 January 2020).
- Dee, D.P.; Uppala, S.M.; Simmons, A.J.; Berrisford, P.; Poli, P.; Kobayashi, S.; Andrae, U.; Balmaseda, M.A.; Balsamo, G.; Bauer, P.; et al. The ERA-Interim reanalysis: Configuration and performance of the data assimilation system. Q. J. R. Meteorol. Soc. 2011, 137, 553–597. [Google Scholar] [CrossRef]
- European Centre for Medium-Range Weather Forecasts Copernicus Climate Data Store. Available online: cds.climate.copernicus.eu (accessed on 15 December 2020).
- Wong, J.; Stoddard, S.T.; Astete, H.; Morrison, A.C.; Scott, T.W. Oviposition site selection by the dengue vector Aedes aegypti and its implications for dengue control. PLoS Negl. Trop. Dis. 2011, 5, e1015. [Google Scholar] [CrossRef]
- Carvalho, F.D.; Moreira, L.A. Why is Aedes aegypti Linnaeus so Successful as a Species? Neotrop. Entomol. 2017, 46, 243–255. [Google Scholar] [CrossRef]
- Gratz, N.G. Critical review of the vector status of Aedes albopictus. Med. Vet. Entomol. 2004, 18, 215–227. [Google Scholar] [CrossRef]
- United States Geological Survey Landsat 5–8 Satellite Images. Available online: https://earthexplorer.usgs.gov/ (accessed on 5 January 2019).
- Umor, S.M.; Mokhtar, M.B.; Surip, N.; Ahmad, A. Generating a dengue risk map (DRM) based on environmental factors using remote sensing and GIS technologies. In Proceedings of the Asian Association on Remote Sensing, 28th Asian Conference on Remote Sensing, Kuala Lumpur, Malaysia, 12–16 November 2007; Volume 2, pp. 867–881. [Google Scholar]
- Struchiner, C.J.; Rockloev, J.; Wilder-Smith, A.; Massad, E. Increasing dengue incidence in Singapore over the past 40 years: Population growth, climate and mobility. PLoS ONE 2015, 10, e0136286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berman, T.; Zohary, T.; Nishri, A.; Sukenik, A.; Kuşçu Şimşek, Ç.; Ödül, H.; Food and Agriculture Organization of the United Nations; Ford, J.D.; Pearce, T.; McDowell, G.; et al. Epidemiological Trends of Dengue Disease in Thailand (2000–2011): A Systematic Literature Review. PLoS Negl. Trop. Dis. 2014, 8, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Khampapongpane, B.; Lewis, H.C.; Ketmayoon, P.; Phonekeo, D.; Somoulay, V.; Khamsing, A.; Phengxay, M.; Sisouk, T.; Vongphrachanh, P.; Bryant, J.E. National dengue surveillance in the Lao People’s Democratic Republic, 2006–2012: Epidemiological and laboratory findings. West. Pacific Surveill. Response J. WPSAR 2014, 5, 7–13. [Google Scholar] [CrossRef] [Green Version]
- Reiter, P.; Lathrop, S.; Bunning, M.; Biggerstaff, B.; Singer, D.; Tiwari, T.; Baber, L.; Amador, M.; Thirion, J.; Hayes, J.; et al. Texas lifestyle limits transmission of dengue virus. Emerg. Infect. Dis. 2003, 9, 86. [Google Scholar] [CrossRef] [PubMed]
- Vannavong, N.; Seidu, R.; Stenström, T.A.; Dada, N.; Overgaard, H.J. Effects of socio-demographic characteristics and household water management on Aedes aegypti production in suburban and rural villages in Laos and Thailand. Parasites Vectors 2017, 10, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Telle, O.; Nikolay, B.; Kumar, V.; Benkimoun, S.; Pal, R.; Nagpal, B.; Paul, R.E. Social and environmental risk factors for dengue in Delhi city: A retrospective study. PLoS Negl. Trop. Dis. 2021, 15, e0009024. [Google Scholar] [CrossRef]
- Mulligan, K.; Dixon, J.; Sinn, C.L.J.; Elliott, S.J. Is dengue a disease of poverty? A systematic review. Pathog. Glob. Health 2015, 109, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Laddey, R.; Kumamoto, M.; Treichel, P. Africa Adaptation Programme Experiences Gender and Climate Change: Advancing Development Through an Integrated Gender Perspective; Discussion Paper Series; United Nations Development Programme: New York, NY, USA, 2011; Volume 1. [Google Scholar]
- Gesler, W. The uses of spatial analysis in medical geography: A review. Soc. Sci. Med. 1986, 23, 963–973. [Google Scholar] [CrossRef]
- Khun, S.; Manderson, L. Community and school-based health education for dengue control in rural Cambodia: A process evaluation. PLoS Negl. Trop. Dis. 2007, 1, e143. [Google Scholar] [CrossRef]
- Hersbach, H.; Bell, B.; Berrisford, P.; Hirahara, S.; Horányi, A.; Muñoz-Sabater, J.; Nicolas, J.; Peubey, C.; Radu, R.; Schepers, D.; et al. The ERA5 global reanalysis. Q. J. R. Meteorol. Soc. 2020, 146, 1999–2049. [Google Scholar] [CrossRef]
- Zafar, S.; Overgaard, H.J.; Shipin, O.; Paul, R.E.; Mayxay, M.; Pientong, C.; Aromseree, S.; Poolphol, P.; Pongvongsa, T.; Vannavong, N.; et al. Environmental and climatic drivers of dengue fever in Lao People’s Democratic. Int. J. Environ. Res. Public Health 2021. (submitted). [Google Scholar]
- Siraj, A.S.; Oidtman, R.J.; Huber, J.H.; Kraemer, M.U.G.; Brady, O.J.; Johansson, M.A.; Perkins, T.A. Temperature modulates dengue virus epidemic growth rates through its effects on reproduction numbers and generation intervals. PLoS Negl. Trop. Dis. 2017, 11, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Liu-Helmersson, J.; Stenlund, H.; Wilder-Smith, A.; Rocklöv, J. Vectorial capacity of Aedes aegypti: Effects of temperature and implications for global dengue epidemic potential. PLoS ONE 2014, 9, e89783. [Google Scholar] [CrossRef] [Green Version]
- Carrington, L.B.; Armijos, M.V.; Lambrechts, L.; Scott, T.W. Fluctuations at a Low Mean Temperature Accelerate Dengue Virus Transmission by Aedes aegypti. PLoS Negl. Trop. Dis. 2013, 7, e2190. [Google Scholar] [CrossRef] [PubMed]
- Kuno, G. Review of the Factors Modulating Dengue Transmission. Epidemiol. Rev. 1995, 17, 321–335. [Google Scholar] [CrossRef]
- Ehelepola, N.D.B.; Ariyaratne, K.; Buddhadasa, W.M.N.P.; Ratnayake, S.; Wickramasinghe, M. A study of the correlation between dengue and weather in Kandy City, Sri Lanka (2003–2012) and lessons learned. Infect. Dis. Poverty 2015, 4, 1–15. [Google Scholar] [CrossRef] [Green Version]
- Castillo, K.C.; Körbl, B.; Stewart, A.; Gonzalez, J.F.; Poncec, F.; Cordeiro, R.; Donalisio, M.R.; Andrade, V.R.; Mafra, A.C.N.; Nucci, L.B.; et al. Dengue fever occurrence and vector detection by larval survey, ovitrap and mosquiTRAP: A space-time clusters analysis. Sci. Total Environ. 2011, 7, 1–11. [Google Scholar] [CrossRef]
- Gubler, D.J. Dengue, Urbanization and globalization: The unholy trinity of the 21 st century. Trop. Med. Health 2011, 39, 3–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thammapalo, S.; Chongsuwiwatwong, V.; Geater, A.; Lim, A.; Choomalee, K. Socio-demographic and environmental factors associated with Aedes breeding places in Phuket, Thailand. Southeast Asian J. Trop. Med. Public Health 2005, 36, 426–433. [Google Scholar] [PubMed]
- De Mattos Almeida, M.C.; Caiaffa, W.T.; Assunção, R.M.; Proietti, F.A. Spatial vulnerability to dengue in a Brazilian urban area during a 7-year surveillance. J. Urban Health 2007, 84, 334–345. [Google Scholar] [CrossRef] [Green Version]
- Daudé, É.; Mazumdar, S.; Solanki, V. Widespread fear of dengue transmission but poor practices of dengue prevention: A study in the slums of Delhi, India. PLoS ONE 2017, 12, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Mayxay, M.; Cui, W.; Thammavong, S.; Khensakhou, K.; Vongxay, V.; Inthasoum, L.; Sychareun, V.; Armstrong, G. Dengue in peri-urban Pak-Ngum district, Vientiane capital of Laos: A community survey on knowledge, attitudes and practices. BMC Public Health 2013, 13, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Danis-Lozano, R.; Rodríguez, M.H.; Hernández-Avila, M. Gender-related family head schooling and Aedes aegypti larval breeding risk in Southern Mexico. Salud Publica Mex. 2002, 44, 237–242. [Google Scholar] [CrossRef] [Green Version]
- Ali, M.; Wagatsuma, Y.; Emch, M.; Breiman, R.F. Use of a geographic information system for defining spatial risk for dengue transmission in Bangladesh: Role for Aedes albopictus in an urban outbreak. Am. J. Trop. Med. Hyg. 2003, 69, 634–640. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNicoll, G. Human Development Report 1995; United Nations Development Programme: New York, NY, USA, 1995; Volume 21, ISBN 9780230284456. [Google Scholar]
- Drobne, S.; Lisec, A. Multi-attribute decision analysis in GIS: Weighted linear combination and ordered weighted averaging. Informatica 2009, 33, 459–474. [Google Scholar]
- Al-Abadi, A.M.; Pourghasemi, H.R.; Shahid, S.; Ghalib, H.B. Spatial Mapping of Groundwater Potential Using Entropy Weighted Linear Aggregate Novel Approach and GIS. Arab. J. Sci. Eng. 2017, 42, 1185–1199. [Google Scholar] [CrossRef]
- Rezaei, J. Best-worst multi-criteria decision-making method. Omega 2015, 53, 49–57. [Google Scholar] [CrossRef]
- Devarakonda, P.; Sadasivuni, R.; Nobrega, R.A.A.; Wu, J. Application of spatial multicriteria decision analysis in healthcare: Identifying drivers and triggers of infectious disease outbreaks using ensemble learning. J. Multi-Criteria Decis. Anal. 2021, 1–14. [Google Scholar] [CrossRef]
- WHO. Technical Handbook for Dengue Surveillance, Dengue Outbreak Prediction/Detection and Outbreak Response (“Model Contingency Plan”); WHO Library Cataloguing-in-Publication Data; World Health Organisation: Geneva, Switzerland, 2016; Volume 92. [Google Scholar]
- Hasnan, S.N.A.; Che-Dom, N.; Abd-Latif, Z.; Madzlan, F. Surveillance of Aedes mosquitoes in different residential types in central zone of Shah Alam, Selangor. Asian Pac. J. Trop. Dis 2017, 7, 332–340. [Google Scholar] [CrossRef]
- Lin, H.; Liu, T.; Song, T.; Lin, L.; Xiao, J.; Lin, J.; He, J.; Zhong, H.; Hu, W.; Deng, A.; et al. Community Involvement in Dengue Outbreak Control: An Integrated Rigorous Intervention Strategy. PLoS Negl. Trop. Dis. 2016, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Zahir, A. Community Participation, Dengue Fever Prevention and Practices for Control in Swat, Pakistan. Int. J. MCH AIDS 2016, 5, 39–45. [Google Scholar] [CrossRef]
- Morris, J.; Fiorino, F. Power Surge—The Impacts of Rapid Dam Development in Laos; International Rivers: Berkeley, CA, USA, 2008; Volume 169, ISBN 9780971885875. [Google Scholar]
- Thomas, I.L. Drivers of Forest Change in the Greater Mekong Subregion, Vientiane, Laos. 2015. Available online: https://www.leafasia.org/library/drivers-forest-change-greater-mekong-subregion-vietnam (accessed on 5 September 2021).
- Husnina, Z.; Clements, A.C.A.; Wangdi, K. Forest cover and climate as potential drivers for dengue fever in Sumatra and Kalimantan 2006–2016: A spatiotemporal analysis. Trop. Med. Int. Health 2019, 24, 888–898. [Google Scholar] [CrossRef]
- Hurni, K.; Fox, J. The expansion of tree-based boom crops in mainland Southeast Asia: 2001 to 2014. J. Land Use Sci. 2018, 13, 198–219. [Google Scholar] [CrossRef]
- Ramachandran, V.G.; Roy, P.; Das, S.; Mogha, N.S.; Bansal, A.K. Empirical model for estimating dengue incidence using temperature, rainfall, and relative humidity: A 19-year retrospective analysis in East Delhi. Epidemiol. Health 2016, 38, e2016052. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, R.; Sontisirikit, S.; Iamsirithaworn, S.; Prendinger, H. Prediction of dengue outbreaks based on disease surveillance, meteorological and socio-economic data. BMC Infect. Dis. 2019, 19, 272. [Google Scholar] [CrossRef] [PubMed]
- Raghwani, J.; Rambaut, A.; Holmes, E.C.; Hang, V.T.; Hien, T.T.; Farrar, J.; Wills, B.; Lennon, N.J.; Birren, B.W.; Henn, M.R.; et al. Endemic dengue associated with the co-circulation of multiple viral lineages and localized density-dependent transmission. PLoS Pathog. 2011, 7, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tosepu, R.; Tantrakarnapa, K.; Worakhunpiset, S.; Nakhapakorn, K. Climatic factors influencing dengue hemorrhagic fever in Kolaka district, Indonesia. Environ. Nat. Resour. J. 2018, 16, 1–10. [Google Scholar] [CrossRef]
- Wangdi, K.; Clements, A.C.A.; Du, T.; Nery, S.V. Spatial and temporal patterns of dengue infections in Timor-Leste, 2005–2013. Parasites Vectors 2018, 11, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Wongkoon, S.; Jaroensutasinee, M.; Jaroensutasinee, K. Climatic Variability and Dengue Virus Transmission in Chiang Rai, Thailand. Biomedica 2011, 27, 5. [Google Scholar]
- Wongkoon, S.; Jaroensutasinee, M.; Jaroensutasinee, K. Spatio-temporal climate-based model of dengue infection in Southern, Thailand. Trop. Biomed. 2016, 33, 55–70. [Google Scholar] [PubMed]
- Phanitchat, T.; Zhao, B.; Haque, U.; Pientong, C.; Ekalaksananan, T.; Aromseree, S.; Thaewnongiew, K.; Fustec, B.; Bangs, M.J.; Alexander, N.; et al. Spatial and temporal patterns of dengue incidence in northeastern Thailand 2006–2016. BMC Infect. Dis. 2019, 19, 743. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rahman, M.S.; Ekalaksananan, T.; Zafar, S.; Poolphol, P.; Shipin, O.; Haque, U.; Paul, R.; Rocklöv, J.; Pientong, C.; Overgaard, H.J. Ecological, social and other environmental determinants of dengue vector abundance in urban and rural areas of Northeastern Thailand. Int. J. Environ. Res. Public Health 2021, 18, 5971. [Google Scholar] [CrossRef]
- The World Bank. Economic Assessment of Sanitation Interventions in Lao People’s Democratic Republic; The World Bank: Jakarta, Indonesia, 2012. [Google Scholar]
- WHO. Thailand: Sanitation, Drinking-Water and Hygiene Status Overview; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Bavia, L.; Melanda, F.N.; de Arruda, T.B.; Mosimann, A.L.P.; Silveira, G.F.; Aoki, M.N.; Kuczera, D.; Sarzi, M.L.; Junior, W.L.C.; Conchon-Costa, I.; et al. Epidemiological study on dengue in southern Brazil under the perspective of climate and poverty. Sci. Rep. 2020, 10, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Pacific Bridge Medical Healthcare in Laos. Available online: https://www.pacificbridgemedical.com/publication/healthcare-in-laos/ (accessed on 14 July 2021).
- WHO. Coordinated, intersectoral action to improve public health. In Advancing the Right to Health: The Vital Role of Law; World Health Organization: Geneva, Switzerland, 2016; pp. 79–101. [Google Scholar]
- Thailand Office of the Council of State. Constitution of the Kingdom of Thailand, Unofficial Translation, Thailand. 2007. Available online: http://www.ilo.org/wcmsp5/groups/public/@ed_protect/@protrav/@ilo_aids/documents/legaldocument/wcms_117898.pdf (accessed on 5 September 2021).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Determinants | Indicators | Rationale for Selection | Data Source | |
|---|---|---|---|---|
| Exposure | Climate | Mean Monthly Temperature (°C) | Higher temperatures favor vectorial reproduction such as the laying of eggs, egg hatching, and development of larva and pupa. The inverse relationship of temperature with the extrinsic incubation period of DENV in Aedes mosquitoes promotes viral transmission at higher temperatures (Carrington et al., 2013; Kuno, 1995). | Copernicus Climate Data Store [25,26] https://cds.climate.copernicus.eu/#!/home (accessed on 5 September 2021) |
| Monthly Rainfall (mm) | Generation of aquatic habitats for oviposition [27]. | |||
| Land environment | Forest, Plantations, cropland, or built-up land uses (%) | Human environments are favored by Aedes aegypti [28] and natural environments such as plantations by Aedes albopictus [29]. | United States Geological Survey (USGS) [30], https://earthexplorer.usgs.gov (accessed on 5 September 2021) | |
| Human environment | Population density (person/km2.) | Availability of host reservoirs of virus, required for dengue transmission [31,32]. | Total population [24] divided by Area | |
| Determinants | Indicators | Rationale for selection | Data source | |
| Susceptibility | Individual | Age under 15 years and greater than 60 years (%) | In Laos and Thailand, children 0–15 years have been reported to have a higher susceptibility to dengue than the adult population [33,34]. According to past 17 years of data used in this study, an increase in dengue cases is observed in the elderly population of an age greater than 60 years old (Supplementary File, Figure S1: Age group distribution of reported dengue cases (DF, DHF, and DSS) in Savannakhet and Champasak provinces in Laos and Mukdahan and Ubon Ratchathani provinces in Thailand between 2003 and 2019). | National censuses Laos in 2005 and 2015 [23]. National annual socio-economic survey in Thailand in 2003–2019 [24]. |
| Community | Housing quality (%) | Houses with porous floors, unplastered walls, and bathrooms without tiles can cause increased indoor humidity, conducive to vector survival [35]. | National censuses Laos in 2005 and 2015 [23]. Not available for Thailand at the subdistrict level | |
| Water and sanitation (%) | Unavailability of reliable piped water supply, water storage for drinking, and flush toilets increase oviposition sites [36,37,38]. | |||
| Determinants | Indicators | Rationale for selection | Data source | |
| Adaptive Capacity | Female literacy rate (%) | Families with increased female education and literacy possess higher adaptive capacities [39]. | National censuses Laos in 2005 and 2015 [23]. Not available for Thailand at subdistrict level | |
| Health facility in proximity/Mean distance to hospital (km) | Delay in medical attention of infant and child dengue patients; poor diagnosis and lack of appropriate care cause hospitalization and deaths [40,41]. | National censuses Laos in 2005 and 2015 [23]. For Thailand mapped and calculated using Google Earth. | ||
| Poverty incidence % | Households with low family income have low capacity to invest in health care [38]. | National censuses Laos in 2005 and 2015 [23]. National annual socio-economic survey in Thailand in 2003–2019 [24]. | ||
| Determinants | Indicators (Unit) | Dimensions | Thresholds and Scores |
|---|---|---|---|
| Exposure | Temperature (°C) | Monthly mean temperature, 1-month lag | 24–29 °C: linear increase in exposure up to 1 |
| <24 °C or >29 °C: 0 Exposure | |||
| Rainfall (mm) | Monthly cumulative rainfall, 1-month lag | <300 mm precipitation: linear increase in exposure up to 1 | |
| >300: 0 Exposure | |||
| Land use/Land cover (km2) | Built-up area | 1 | |
| Wetland area | 0 | ||
| Rubber/cassava/cashew/coffee plantation area | 0.5 | ||
| Forest area | 0 | ||
| Disturbed forest area | 0.25 | ||
| Rice and sugarcane crop area | 0.25 | ||
| Population density (person/km2) | 0–200 | 0.25 | |
| 200–400 | 0.5 | ||
| >400 | 1 | ||
| Susceptibility | Age (%) | The proportion of population <15 to >60 years | 1 |
| The proportion of population >15 to <60 years | 0.5 | ||
| Living conditions/Housing quality (%) | The proportion of houses made of both concrete and wood | 0.25 | |
| The proportion of houses made of wood | 0.5 | ||
| The proportion of houses made of bamboo and both bamboo and wood | 1 | ||
| Toilet type (%) | The proportion of households with modern toilet | 0 | |
| The proportion of households with squat and pit toilet | 1 | ||
| Adaptive Capacity | Female literacy rate (%) | 0–50 | 1 |
| 50–100 | 0.25 | ||
| Mean distance to hospital (km) | 0–5 | 0.25 | |
| 10–15 | 0.5 | ||
| >15 | 1 | ||
| Poverty incidence (%) | 0–20 | 0.25 | |
| 20–40 | 0.5 | ||
| >40 | 1 |
| Exposure | Best to others: Temperature (°C) | Others to the Worst: Landcover (km2) | Weights | Consistency Index | ||
| Temperature (°C) | 1 | Temperature (°C) | 2 | 0.39 | 0.07 | |
| Rainfall (mm) | 2 | Rainfall (mm) | 2 | 0.23 | ||
| Landcover (km2) | 2 | Landcover (km2) | 2 | 0.15 | ||
| Population density (person/km2) | 2 | Population density (person/km2) | 1 | 0.23 | ||
| Susceptibility | Best to others: Population (Density person/km2) | Others to the Worst: Age | 0.04 | |||
| Living conditions | 2 | Living conditions | 2 | 0.54 | ||
| Toilet type | 3 | Toilet type | 2 | 0.29 | ||
| Age <15 and >60 | 4 | Age <15 and >60 | 1 | 0.17 | ||
| Adaptive capacity | Best to others: Literacy Rate (%) | Others to the Worst: Mean Distance to Hospital (km2) | 0.04 | |||
| Female literacy rate (%) | 1 | Female literacy rate (%) | 3 | 0.54 | ||
| Poverty incidence (%) | 2 | Poverty incidence (%) | 2 | 0.29 | ||
| Mean distance to hospital (km2) | 3 | Mean distance to hospital (km2) | 1 | 0.17 | ||
| Vulnerability | Best to others: Exposure | Others to the Worst: Adaptive Capacity | 0.04 | |||
| Exposure | 1 | Exposure | 3 | 0.54 | ||
| Susceptibility | 2 | Susceptibility | 3 | 0.32 | ||
| Adaptive capacity | 3 | Adaptive capacity | 1 | 0.17 | ||
| Year | Laos | Thailand | ||||
|---|---|---|---|---|---|---|
| Observed Cases | Average IR | Maximum IR | Observed Cases | Average IR | Maximum IR | |
| 2003 | 5075 | 24.2 | 405.9 (October) | 3709 | 13.5 | 340.4 (May) 553.8 (June) |
| 2004 | 1452 | 6.6 | 349.3 (July) | 1013 | 4.0 | 245.8 |
| 2005 | 2282 | 10.6 | 203.8 | 978 | 3.9 | 260.6 |
| 2006 | 1501 | 7.4 | 128.9 | 1021 | 3.9 | 277.8 |
| 2007 | 2146 | 10.9 | 132.4 | 1379 | 5.9 | 247.0 |
| 2008 | 3468 | 19.5 | 160.6 | 871 | 3.3 | 170.3 |
| 2009 | 1087 | 5.2 | 70.2 | 1059 | 4.5 | 533.0 (July) |
| 2010 | 5391 | 26.2 | 345.4 (September) | 2704 | 10.8 | 481.0 (June) 481.4 (July) 350.0 (August) |
| 2011 | 572 | 3.0 | 73.5 | 1197 | 4.9 | 295.7 |
| 2012 | 1163 | 6.0 | 159.3 | 1135 | 4.3 | 160.8 |
| 2013 | 9294 | 44.0 | 487.0 (June) 578.9 (July) 312.0 (August) | 4102 | 15.9 | 316.0 (March) 303.0 (May) 1404.2 (June) 637.0 (July) 405.0 (August) |
| 2014 | 116 | 0.6 | 25.8 | 601 | 2.6 | 400.0 (June) |
| 2015 | 210 | 1.0 | 98.9 | 5370 | 19.7 | 554.0 (July) 724.6 (August) 329.0 (September) |
| 2016 | 1998 | 9.5 | 433.1 (June) | 2644 | 10.1 | 402.9 (September) |
| 2017 | 1688 | 9.0 | 148.4 | 1056 | 4.0 | 263.8 |
| 2018 | 1944 | 8.8 | 203.9 | 2284 | 8.8 | 418.7 (May) 395.0 (June) |
| 2019 | 9465 | 33.0 | 336.0 (July) 575.3 (August) 411.0 (September) | 8321 | 30.3 | 303.4 (April) 510.0 (May) 730.0 (June) 434.0 (July) 372.0 (August) |
| Mean | 2874 | 12.6 | – | 2320 | 8.9 | – |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zafar, S.; Shipin, O.; Paul, R.E.; Rocklöv, J.; Haque, U.; Rahman, M.S.; Mayxay, M.; Pientong, C.; Aromseree, S.; Poolphol, P.; et al. Development and Comparison of Dengue Vulnerability Indices Using GIS-Based Multi-Criteria Decision Analysis in Lao PDR and Thailand. Int. J. Environ. Res. Public Health 2021, 18, 9421. https://doi.org/10.3390/ijerph18179421
Zafar S, Shipin O, Paul RE, Rocklöv J, Haque U, Rahman MS, Mayxay M, Pientong C, Aromseree S, Poolphol P, et al. Development and Comparison of Dengue Vulnerability Indices Using GIS-Based Multi-Criteria Decision Analysis in Lao PDR and Thailand. International Journal of Environmental Research and Public Health. 2021; 18(17):9421. https://doi.org/10.3390/ijerph18179421
Chicago/Turabian StyleZafar, Sumaira, Oleg Shipin, Richard E. Paul, Joacim Rocklöv, Ubydul Haque, Md. Siddikur Rahman, Mayfong Mayxay, Chamsai Pientong, Sirinart Aromseree, Petchaboon Poolphol, and et al. 2021. "Development and Comparison of Dengue Vulnerability Indices Using GIS-Based Multi-Criteria Decision Analysis in Lao PDR and Thailand" International Journal of Environmental Research and Public Health 18, no. 17: 9421. https://doi.org/10.3390/ijerph18179421