
Trends and Patterns of Knee Osteoarthritis in China: A Longitudinal Study of 17.7 Million Adults from 2008 to 2017

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Data Sources
2.2. Study Design and Participants
2.3. Definition of Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
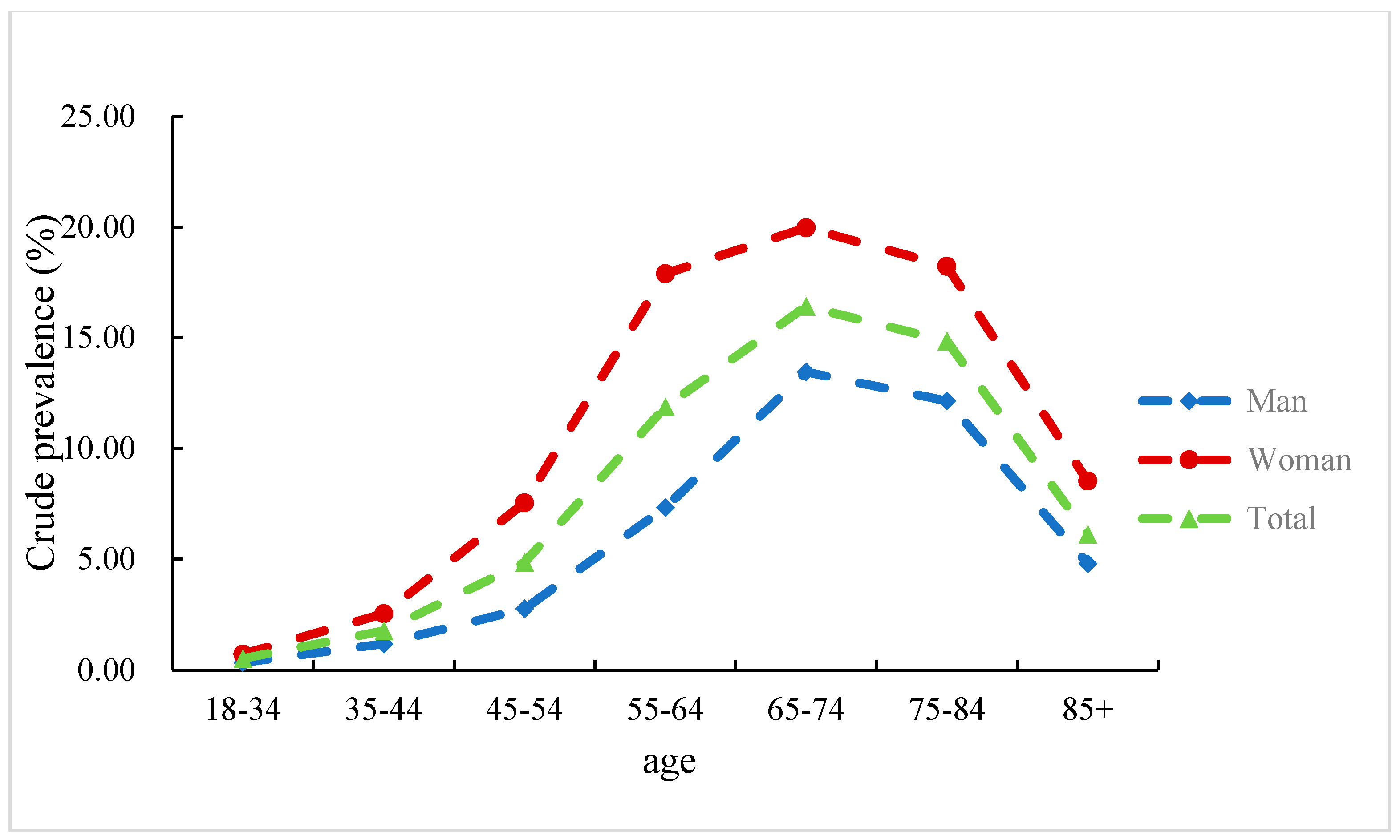
3.2. Prevalence and Incidence of KOA
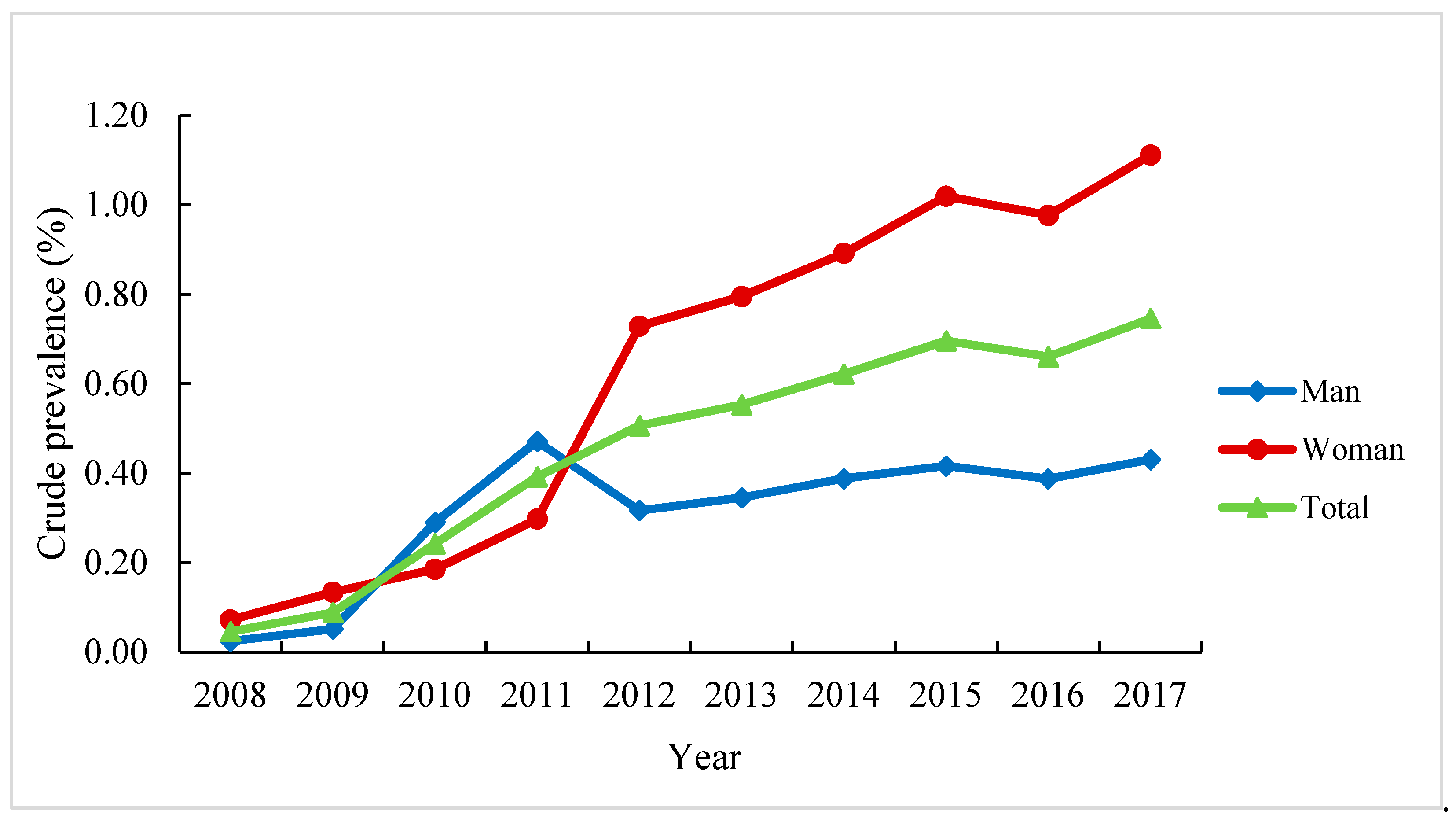
3.3. Trends in the Prevalence and Incidence of KOA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McAlindon, T.E.; Bannuru, R.; Sullivan, M.C.; Arden, N.K.; Berenbaum, F.; Bierma-Zeinstra, S.M.; Hawker, G.A.; Henrotin, Y.; Hunter, D.J.; Kawaguchi, H.; et al. OARSI guidelines for the non-surgical management of knee osteoarthritis. Osteoarthr. Cartil. 2014, 22, 363–388. [Google Scholar] [CrossRef] [Green Version]
- Cho, H.J.; Morey, V.; Kang, J.Y.; Kim, K.W.; Kim, T.K. Prevalence and Risk Factors of Spine, Shoulder, Hand, Hip, and Knee Osteoarthritis in Community-dwelling Koreans Older than Age 65 Years. Clin. Orthop. Relat. Res. 2015, 473, 3307–3314. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helmick, C.G.; Felson, D.T.; Lawrence, R.C.; Gabriel, S.; Hirsch, R.; Kwoh, C.K.; Liang, M.H.; Kremers, H.M.; Mayes, M.D.; Merkel, P.A. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States. Part, I. Arthritis Rheum. 2008, 58, 15–25. [Google Scholar] [CrossRef] [PubMed]
- Postler, A.; Ramos, A.L.; Goronzy, J.; Günther, K.P.; Lange, T.; Schmitt, J.; Zink, A.; Hoffmann, F. Prevalence and treatment of hip and knee osteoarthritis in people aged 60 years or older in Germany: An analysis based on health insurance claims data. Clin. Interv. Aging 2018, 13, 2339–2349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guillemin, F.; Rat, A.C.; Mazieres, B.; Pouchot, J.; Fautrel, B.; Euller-Ziegler, L.; Fardellone, P.; Morvan, J.; Roux, C.H.; Verrouil, E.; et al. Prevalence of symptomatic hip and knee osteoarthritis: A two-phase population-based survey. Osteoarthr. Cartil. 2011, 19, 1314–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeng, X.Y.; Qi, J.L.; Yin, P.; Wang, L.J.; Liu, Y.N.; Liu, J.M.; Zhou, M.G.; Liang, X.F. Burden of Disease Reports in China and Provincial Administrative Regions from 1990 to 2016. Chin. Circ. J. 2018, 246, 7–18. (In Chinese) [Google Scholar]
- Kiadaliri, A.A.; Lohmander, L.S.; Moradi-Lakeh, M.; Petersson, I.F.; Englund, M. High and rising burden of hip and knee osteoarthritis in the Nordic region, 1990-2015. Acta Orthop 2018, 89, 177–183. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gao, X.R. How Many Artificial Knee and Hip Replacement Surgeries Did China Do in 2018? What Is the Amount? Available online: https://www.haodf.com/zhuanjiaguandian/gaoxurendr_7591652124.htm (accessed on 1 December 2020). (In Chinese).
- Nguyen, U.S.D.; Zhang, Y.; Zhu, Y.; Niu, J.B.; Zhang, B.; Felson, D.T. Increasing prevalence of knee pain and symptomatic knee osteoarthritis: Survey and cohort data. Ann. Intern. Med. 2011, 155, 725–732. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, B.R.; Katz, J.N.; Solomon, D.H.; Yelin, E.H.; Hunter, D.J.; Messier, S.P.; Suter, L.G.; Losina, E. Number of Persons With Symptomatic Knee Osteoarthritis in the US: Impact of Race and Ethnicity, Age, Sex, and Obesity. Arthritis Care Res. 2016, 68, 1743–1750. [Google Scholar] [CrossRef]
- Holt, H.L.; Katz, J.N.; Reichmann, W.M.; Gerlovin, H.; Wright, E.A.; Hunter, D.J.; Jordan, J.M.; Kessler, C.L.; Losina, E. Forecasting the burden of advanced knee osteoarthritis over a 10-year period in a cohort of 60-64 year-old US adults. Osteoarthr. Cartil. 2011, 19, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Zang, C.H.; Zeng, Q.Y.; Li, X.F.; Dong, H.Y.; Zhang, A.L. Epidemiological study of knee osteoarthritis in Taiyuan. Chin. J. Intern. Med. 2006, 45, 533–536. (In Chinese) [Google Scholar]
- Jiang, L.; Rong, J.; Zhang, Q.; Hu, F.; Zhang, S.; Li, X.; Zhao, Y.; Tao, T. Prevalence and associated factors of knee osteoarthritis in a community-based population in Heilongjiang, Northeast China. Rheumatol. Int. 2012, 32, 1189–1195. [Google Scholar] [CrossRef]
- Wu, Y.; Yang, C.; Xi, H.; Zhang, Y.; Zhou, Z.; Hu, Y. Prescription of antibacterial agents for acute upper respiratory tract infections in Beijing, 2010-2012. Eur. J. Clin. Pharmacol. 2016, 72, 359–364. [Google Scholar] [CrossRef] [Green Version]
- Wu, J.; Wu, Y.; Tian, Y.; Wu, Y.Q.; Hu, Y.H. Association between ambient fine particulate matter and adult hospital admissions for pneumonia in Beijing, China. Atmos. Environ. 2020, 231, 117497. [Google Scholar] [CrossRef]
- Zghebi, S.S.; Steinke, D.T.; Carr, M.J.; Rutter, M.K.; Emsley, R.A.; Ashcroft, D.M. Examining trends in type 2 diabetes incidence, prevalence and mortality in the UK between 2004 and 2014. Diabetes Obes. Metab. 2017, 19, 1537–1545. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.J.; Fay, M.P.; Feuer, E.J.; Midthune, D.N. Permutation tests for joinpoint regression with applications to cancer rates. Stat. Med. 2000, 19, 335–351. [Google Scholar] [CrossRef]
- Clegg, L.X.; Hankey, B.F.; Tiwari, R.; Feuer, E.J.; Edwards, B.K. Estimating average annual per cent change in trend analysis. Stat. Med. 2009, 28, 3670–3682. [Google Scholar] [CrossRef] [Green Version]
- Laxafoss, E.; Jacobsen, S.; Gosvig, K.K.; Holm, S.S. Case definitions of knee osteoarthritis in 4,151 unselected subjects: Relevance for epidemiological studies: The Copenhagen Osteoarthritis Study. Skelet. Radiol. 2010, 39, 859–866. [Google Scholar] [CrossRef]
- Leyland, K.M.; Hart, D.J.; Javaid, M.K.; Judge, A.; Kiran, A.; Soni, A.; Goulston, L.M.; Cooper, C.; Spector, T.D.; Arden, N.K. The natural history of radiographic knee osteoarthritis: A fourteen-year population-based cohort study. Arthritis Rheum. 2012, 64, 2243–2251. [Google Scholar] [CrossRef]
- Kulkarni, K.; Karssiens, T.; Kumar, V.; Pandit, H. Obesity and osteoarthritis. Maturitas 2016, 89, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Physical Activity. Available online: http://www.who.int/mediacentre/factsheets/fs385/en/ (accessed on 1 December 2020).
- Dekker, J.; Van Dijk, G.M.; Veenhof, C. Risk factors for functional decline in osteoarthritis of the hip or knee. Curr. Opin. Rheumatol. 2009, 21, 520–524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bala, K.; Bavoria, S.; Sahni, B.; Bhagat, P.; Langeh, S.; Sobti, S. Prevalence, risk factors, and health seeking behavior for knee osteoarthritis among adult population in rural Jammu—A Community based Cross Sectional Study. J. Family Med. Prim. Care 2020, 9, 5282–5287. [Google Scholar]
- Pal, C.P.; Singh, P.; Chaturvedi, S.; Pruthi, K.K.; Vij, A. Epidemiology of knee osteoarthritis in India and related factors. Indian J. Orthop. 2016, 50, 518–522. [Google Scholar] [CrossRef]
- Blagojevic, M.; Jinks, C.; Jeffery, A.; Jordan, K.P. Risk factors for onset of osteoarthritis of the knee in older adults: A systematic review and meta-analysis. Osteoarthr. Cartil. 2010, 18, 24–33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikesky, A.E.; Mazzuca, S.A.; Brandt, K.D.; Perkins, S.M.; Damush, T.; Lane, K.A. Effects of strength training on the incidence and progression of knee osteoarthritis. Arthritis Rheum. 2006, 55, 690–699. [Google Scholar] [CrossRef] [PubMed]
- Felson, D.T.; Zhang, Y.; Hannan, M.T.; Naimark, A.; Weissman, B.; Aliabadi, P.; Levy, D. Risk factors for incident radiographic knee osteoarthritis in the elderly: The Framingham Study. Arthritis Rheum. 1997, 40, 728–733. [Google Scholar] [CrossRef]
- Andersson, C.; Vasan, R.S. Epidemiology of cardiovascular disease in young individuals. Nat. Rev. Cardiol. 2018, 15, 230–240. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.J.; Wu, Y.; Wu, J.H.; Wang, M.Y.; Wang, X.W.; Wang, J.T.; Wu, T.; Wu, Y.Q.; Hu, Y.H. Trends in prevalence and incidence of type 2 diabetes among adults in Beijing, China, from 2008 to 2017. Diabet. Med. 2020, 38, e14487. [Google Scholar]
- Kodama, R.; Muraki, S.; Oka, H.; Iidaka, T.; Teraguchi, M.; Kagotani, R.; Asai, Y.; Yoshida, M.; Morizaki, Y.; Tanaka, S.; et al. Prevalence of hand osteoarthritis and its relationship to hand pain and grip strength in Japan: The third survey of the ROAD study. Mod. Rheumatol. 2016, 26, 767–773. [Google Scholar] [CrossRef]
- Tang, X.; Wang, S.; Zhan, S.; Niu, J.; Tao, K.; Zhang, Y.; Lin, J. The prevalence of symptomatic knee osteoarthritis in China: Results from the China Health and Retirement Longitudinal Study. Arthritis Rheumatol. 2016, 68, 648–653. [Google Scholar] [CrossRef] [PubMed]
- Prieto-Alhambra, D.; Judge, A.; Javaid, M.K.; Cooper, C.; Diez-Perez, A.; Arden, N.K. Incidence and risk factors for clinically diagnosed knee, hip and hand osteoarthritis: Influences of age, gender and osteoarthritis affecting other joints. Ann. Rheum. Dis. 2014, 73, 1659–1664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sun, X.; Zhen, X.; Hu, X.; Li, Y.; Gu, S.; Gu, Y.; Dong, H. Osteoarthritis in the middle-aged and elderly in China: Prevalence and influencing factors. Int. J. Environ. Res. Public Health 2019, 16, 4701. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Su, Y.; Zhu, Z.; Cai, Y.; Jin, D.; Xue, Q. Epidemiological study on symptomatic knee osteoarthritis in middle-aged and elderly people in Guangzhou area. Chin. J. Jt. Surg. 2010, 4, 2–6. [Google Scholar]
- Zhou, Z.; Zou, Z. Investigation on some factors affecting patient’s medical treatment behavior. Chin. Hosp. Manag. 1994, 14, 28–31. (In Chinese) [Google Scholar]



{kind=link}
{kind=link}
| Characteristics | Overall (n = 2,447,990) | Men (n = 984,823) | Women (n = 1,463,167) | p-Value ‡ |
|---|---|---|---|---|
| Level of hospital, % | ||||
| Primary | 21 | 22 | 21 | <0.001 |
| Secondary | 27 | 28 | 26 | |
| Tertiary | 52 | 50 | 53 | |
| Age group *, % | ||||
| 18–34 years | 9 | 8 | 11 | <0.001 |
| 35–44 years | 12 | 11 | 13 | |
| 45–54 years | 21 | 17 | 24 | |
| 55–64 years | 28 | 29 | 27 | |
| 65–74 years | 17 | 20 | 14 | |
| 65–84 years | 11 | 13 | 9 | |
| ≥85 years | 2 | 2 | 2 | |
| Area, % | ||||
| Urban | 76 | 73 | 78 | <0.001 |
| Rural | 24 | 27 | 22 | |
| Working state, % | ||||
| On work | 42 | 47 | 38 | <0.001 |
| Retired | 58 | 53 | 62 |
| 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | |
|---|---|---|---|---|---|---|---|---|---|---|
| Prevalence (%, 95% CI) | ||||||||||
| Overall | 1.567 (1.566, 1.568) | 2.124 (2.123, 2.125) | 3.412 (3.411, 3.413) | 4.499 (4.498, 4.500) | 5.054 (5.053, 5.055) | 5.007 (5.006, 5.008) | 6.040 (6.038, 6.041) | 6.480 (6.479, 6.481) | 5.855 (5.854, 5.856) | 5.935 (5.933, 5.936) |
| Men | 1.867 (1.866, 1.868) | 2.489 (2.487, 2.490) | 2.100 (2.098, 2.101) | 2.827 (2.826, 2.829) | 2.932 (2.930, 2.933) | 2.962 (2.962, 2.964) | 3.751 (3.749, 3.752) | 4.106 (4.104, 4.108) | 3.737 (3.736, 3.739) | 3.842 (3.840, 4.843) |
| Women | 1.262 (1.260, 1.263) | 1.752 (1.751, 1.753) | 4.752 (4.751, 4.754) | 6.206 (6.204, 6.207) | 7.222 (7.219, 7.224) | 7.095 (7.093, 7.098) | 8.377 (8.374, 8.379) | 8.905 (8.902, 8.907) | 8.019 (8.017, 8.020) | 8.072 (8.069, 8.073) |
| Incidence (per 1000 person-years, 95% CI) | ||||||||||
| Overall | 15.21 (15.20, 15.22) | 20.73 (20.72, 20.74) | 22.45 (22.44, 22.46) | 30.45 (20.72, 30.46) | 31.21 (31.20, 31.22) | 26.92 (26.91, 26.94) | 33.85 (33.84, 33.86) | 27.95 (27.94, 27.96) | 22.60 (22.59, 22.61) | 20.60 (20.59, 20.61) |
| Men | 8.10 (8.09, 8.11) | 11.66 (11.65, 11.67) | 13.15 (13.14, 13.16) | 18.15 (18.14, 18.16) | 18.96 (18.95, 18.98) | 17.24 (17.23, 17.25) | 23.05 (23.04, 23.06) | 19.71 (19.69, 19.72) | 16.14 (16.13, 16.15) | 15.01 (15.00, 15.02) |
| Women | 22.48 (22.47, 22.49) | 29.99 (29.98, 30.00) | 31.93 (31.92, 31.95) | 43.00 (42.98, 43.02) | 43.73 (43.72, 43.75) | 36.81 (36.79, 36.83) | 44.89 (44.87, 44.91) | 36.36 (36.35, 36.38) | 29.19 (29.18, 29.21) | 26.31 (26.30, 26.32) |
| Trend 1 | Trend 2 | Average Annual Percentage Change (95% CI) | ||||
|---|---|---|---|---|---|---|
| Period | Annual Percentage Change (95% CI) | Period | Annual Percentage Change (95% CI) | |||
| Prevalence | Overall | 2008–2011 | 48.9 (8.5, 91.1) * | 2011–2017 | 4.7 (−0.6, 10.0) | 16.8 (8.0, 25.6) * |
| Gender | ||||||
| Men | – | – | – | – | 7.7 (4.7, 10.9) * | |
| Women | 2008–2011 | 79.3 (20.0, 158.3) * | 2011–2017 | 3.5 (–1.7, 9.3) | 24.0 (12.3, 36.1) * | |
| Age group, years | ||||||
| 18–34 | 2008–2011 | 113.5 (54.3, 189.5) * | 2011–2017 | 9.4 (5.9, 13.0) * | 36.6 (25.8, 47.2) * | |
| 35–44 | 2008–2012 | 68.1 (33.0, 115.2) * | 2012–2017 | 4.3 (−1.7, 10.4) | 29.5 (18.7, 40.1) * | |
| ≥45 | 2008–2011 | 49.1 (11.8, 90.0) * | 2011–2017 | 3.8 (−1.0, 9.1) | 16.3 (7.8, 25.3) * | |
| Incidence | Overall | – | – | – | – | 1.3 (–5.0, 7.4) |
| Gender | ||||||
| Men | – | – | – | – | 4.3 (–2.5, 11.5) | |
| Women | – | – | – | – | 0.2(–6.1, 6.9) | |
| Age group, years | ||||||
| 18–34 | 2008–2012 | 56.3 (26.4, 88.7) * | 2012–2017 | 2.6 (–3.0, 8.5) | 22.9 (14.3, 31.5) * | |
| 35–44 | 2008–2012 | 59.3 (17.7, 103.5) * | 2012–2017 | −3.6 (−11.5, 4.8) | 19.1 (7.6, 32.9) * | |
| ≥45 | 2008–2012 | 17.5(−1.6, 37.1) | 2012–2017 | −10.7 (−19.5, 0) | 0.8(–6.1, 8.5) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.; Wu, J.; Wang, Z.; Wu, Y.; Wu, T.; Wu, Y.; Wang, M.; Wang, S.; Wang, X.; Wang, J.; et al. Trends and Patterns of Knee Osteoarthritis in China: A Longitudinal Study of 17.7 Million Adults from 2008 to 2017. Int. J. Environ. Res. Public Health 2021, 18, 8864. https://doi.org/10.3390/ijerph18168864
Chen H, Wu J, Wang Z, Wu Y, Wu T, Wu Y, Wang M, Wang S, Wang X, Wang J, et al. Trends and Patterns of Knee Osteoarthritis in China: A Longitudinal Study of 17.7 Million Adults from 2008 to 2017. International Journal of Environmental Research and Public Health. 2021; 18(16):8864. https://doi.org/10.3390/ijerph18168864
Chicago/Turabian StyleChen, Hongbo, Junhui Wu, Zijing Wang, Yao Wu, Tao Wu, Yiqun Wu, Mengying Wang, Siyue Wang, Xiaowen Wang, Jiating Wang, and et al. 2021. "Trends and Patterns of Knee Osteoarthritis in China: A Longitudinal Study of 17.7 Million Adults from 2008 to 2017" International Journal of Environmental Research and Public Health 18, no. 16: 8864. https://doi.org/10.3390/ijerph18168864