
The Burden of Burnout among Healthcare Professionals of Intensive Care Units and Emergency Departments during the COVID-19 Pandemic: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search and Inclusion Criteria
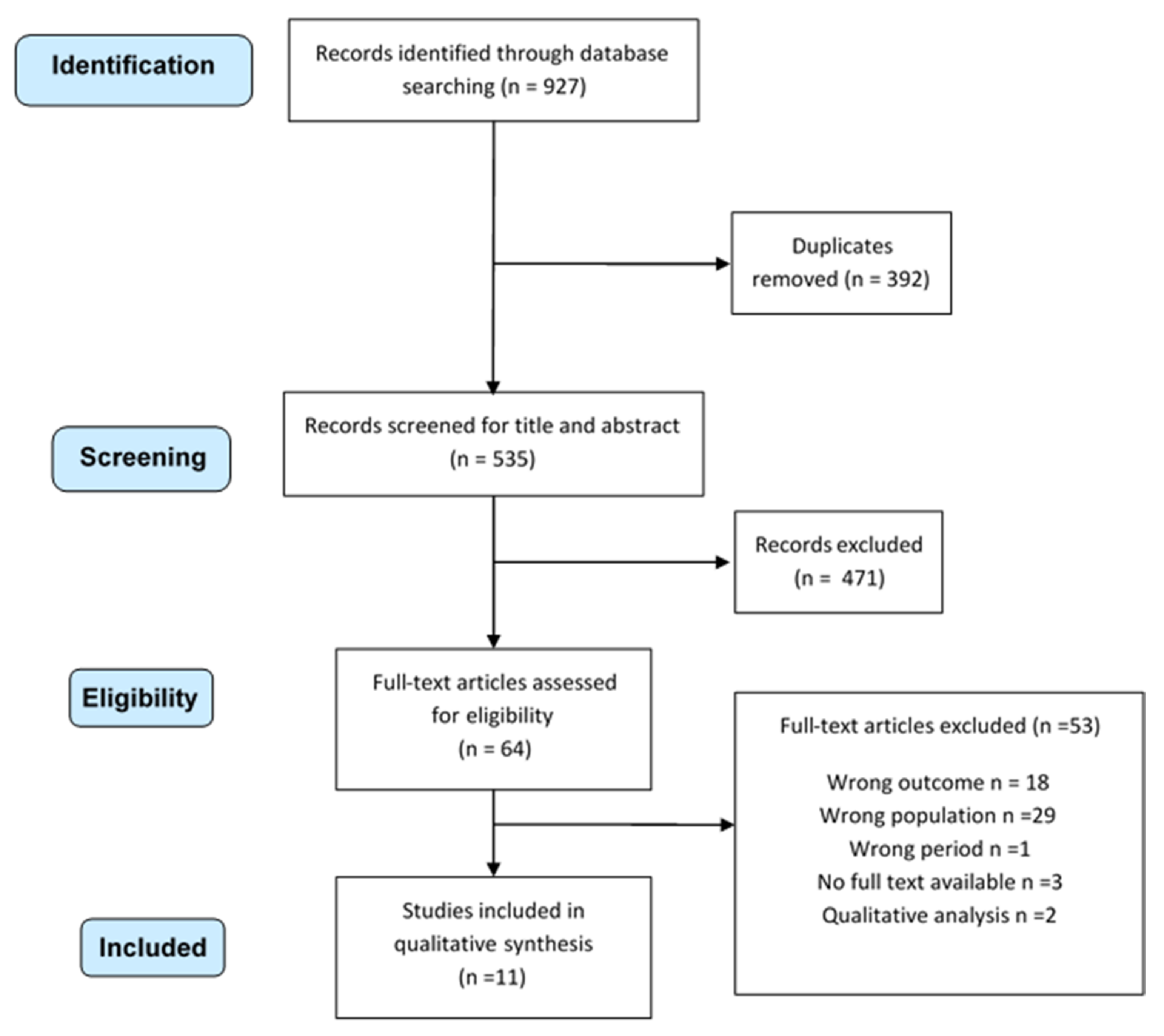
2.2. Study Selection, Data Extraction and Quality Assessment
3. Results

{kind=link}
| 1st Author | Country | Study Design | Setting | Participants | Length of Study | Burnout Evaluation Tool | Prevalence of Burnout | Mean Score for Burnout (SD) [Range] |
|---|---|---|---|---|---|---|---|---|
| Sharma M et al. [25] | USA | CS | ICU | Participants: 1651 Female Gender: 74% Mean age: NA Professional title: Physician 25% Nurse 47% Advanced Practice Provider 11% Respiratory therapist 17% | 04/23–05/07/20 | NA | All participants: 58% Physicians: 49% Physicians-in-training: 48% Nurses: 64% Advanced practice provider: 56% Respiratory therapist: 55% | _ |
| Ruiz-Fernàndez MD et al. [26] | Spain | CS | Primary care centers and other services, including ED/ICU and a COVID-19-specific unit | Participants All participants: 506 ICU/ED/COVID units: 171 (33.7%) Female gender: All participants 76.7% Mean age [range]: All participants 46.7 [23–67] Professional title: All participants: Physician 21.3% Nurse 78.7% | 03/30–04/16/20 | ProQoL Scale | _ | All participants: 24.7 (5.9) ICU: 25.1 (5.4) Emergency department: 24.6 (5.9) Specific COVID-19 unit: 28.9 (7.2) |
| de Wit K et al. [27] | Canada | MM | ED | Participants: 468 Female gender: 49% Median age [IQR]: 41 [35–50] Professional title: Physician 100% | 03/09–05/17/20 | MBI | High emotional exhaustion: Week 4: 18% Week 6: 17% Week 8:14% Week 10: 16% p = 0.632 High depersonalization: Week 4: 15% Week 6: 13% Week 8: 10% Week 10: 13% p = 0.155 No time trend in burnout levels found | _ |
| Buselli R et al. [28] | Italy | CS | Several departments, including ICU | Participants: All participants 265 ICU 78 (29.4%) Gender female: All participants 68.9% Mean age (SD) [range]: All participants: 40.4 ± (11.2), [19–63] Professional title: All participants: Physician 32.1% Nurse 50.2% Healthcare assistants 17.7% | 04/01–05/01/20 | ProQoL Scale | _ | All participants: 19.8 (5.0) [27–58] ICU staff: 19.9 (5.0) (vs. non ICU staff: p = 0.586) |
| Tsan SEH et al. [29] | Malaysia | CS | Anesthesia and ICU | Participants: 85 Female Gender: 63.5% Median age [range]: 31 [27–58] Professional title: Anesthetist 100% | May 2020 | MBI | Overall: 55.3% Burnout indices Emotional exhaustion Low 34.1%; Intermediate 34.1%; High 31.8% Depersonalization Low 21.2%; Intermediate 31.8%; High 47.1% Personal accomplishment Low 63.5%; Intermediate 27.1%; High 9.4% | Burnout indices: Emotional exhaustion: 21.35 (9.9), Depersonalization: 8.74 (4.9) Personal accomplishment: 29.2 (7.4) |
| Azoulay E et al. [24] | Europe, South America, North America, Asia, India, Australia–New Zealand, Africa | CS | ICU | Participants: 1001 MBI respondent: 846 (84.5%) Female gender: 34.2% Median age [IQR]: 45 [39–53] Professional title: Anesthetists 100% | 04/30–05/25/2020 | MBI | Data regarding 846 respondents: Overall burnout: Low: 25.3% Intermediate: 23% High: 51.8% Burnout indices: Emotional exhaustion Low 47,1; Intermediate 29.9%; High: 23% Depersonalization Low 42.7%; Intermediate34.3%; High 23% Symptoms of personal accomplishment Low 33.4%; Intermediate 35.2%; High 31,4% Prevalence of severe BO across region, range Australia–New Zealand, India, Middle Europe, Scandinavia: 20–40% East Europe, North America, Asia, South America, UK, South Europe, the Middle East: 50–70% | _ |
| Chen R et al. [30] | China | CS | Several departments, including CCU | Participants: All participants: 12.596 Critical care units 3577 (28.4%) Intensive care 660 (5.2%) Female gender: All participants 95.6% Mean age (SD): All participants 33.1 (7.5) Professional title: Nurse 100% | April 2020 | MBI | Burnout indices: Emotional exhaustion low 47.8% moderate 27.5% high 24.7% Depersonalization low 54.0% moderate 24.8% high 21.1% Lack of personal accomplishment low 96.9% moderate 2.1% high 1.1% | Emotional exhaustion 20.1 (10.3) Depersonalization 5.9 (4.9) Lack of personal accomplishment: 19 (8.3) |
| Chor WPD et al. [31] | Singapore | CS | ED, UCC | Participants: 337 Female gender: 67.7% Median age: NA Professional title: Physician 37.7% Nurse 62.3% | May 2020 | CBI | Moderate to severe burnout 49.3% | 49.2 (18.6) Nurses 51.3 (19.6) Physicians 45.7 (16.2) (p = 0.005) |
| Gomez S et al. [32] | USA | MM | ICU | Participants: 21 Female gender: NA Mean age: NA Professional title: Physicians 71% | March–May 2020 | SPFI & WBI | 57% | _ |
| Cao J et al. [33] | China | CS | Fever clinic | Participants: 37 Female gender: 78.4% Mean age (SD): 32.8 (9.6) Professional title: Physician 43.2% Nurse 51.3% Clinical technicians 5.4% | - | MBI | Data regarding 32 responders Burnout indices: Emotional Exhaustion 3.1% Depersonalization 12.5% Personal Accomplishment 25% | _ |
| Wahlster S et al. [23] | World-wide (77 countries included) | CS | ICU | Participants: 2700 Female gender: 65% Mean age: NA Professional title: Physician 41% Nurse 40% Advanced practice provider: 8% Respiratory therapist: 11% | 04/23–05/7/2020 | NA | Overall burnout: 52% East Asia and Pacific 30% Europe and Central Asia 48% Latin America and the Caribbean 42% Middle East and North Africa 44% North America 57% South Asia 33% Sub-Saharan Africa 33% | _ |
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- WHO. Director-General’s Opening Remarks at the Media Briefing on COVID-19-11; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Moazzami, B.; Razavi-Khorasani, N.; Dooghaie Moghadam, A.; Farokhi, E.; Rezaei, N. COVID-19 and telemedicine: Immediate action required for maintaining healthcare providers well-being. J. Clin. Virol. 2020, 126, 104345. [Google Scholar] [CrossRef]
- Rossi, R.; Socci, V.; Pacitti, F.; Di Lorenzo, G.; Di Marco, A.; Siracusano, A.; Rossi, A. Mental Health Outcomes Among Frontline and Second-Line Health Care Workers During the Coronavirus Disease 2019 (COVID-19) Pandemic in Italy. JAMA Netw. Open 2020, 3, e2010185. [Google Scholar] [CrossRef]
- Magnavita, N.; Tripepi, G.; Di Prinzio, R.R. Symptoms in health care workers during the covid-19 epidemic. A cross-sectional survey. Int. J. Environ. Res. Public Health 2020, 17, 5218. [Google Scholar] [CrossRef]
- Barello, S.; Palamenghi, L.; Graffigna, G. Burnout and somatic symptoms among frontline healthcare professionals at the peak of the Italian COVID-19 pandemic. Psychiatry Res. 2020, 290. [Google Scholar] [CrossRef]
- Luceño-Moreno, L.; Talavera-Velasco, B.; García-Albuerne, Y.; Martín-García, J. Symptoms of posttraumatic stress, anxiety, depression, levels of resilience and burnout in spanish health personnel during the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 5514. [Google Scholar] [CrossRef]
- Zerbini, G.; Ebigbo, A.; Reicherts, P.; Kunz, M.; Messman, H. Psychosocial burden of healthcare professionals in times of covid-19—A survey conducted at the university hospital augsburg. GMS Ger. Med. Sci. 2020, 18, 1–9. [Google Scholar] [CrossRef]
- Delgado-Gallegos, J.L.; Montemayor-Garza, R.D.J.; Padilla-Rivas, G.R.; Franco-Villareal, H.; Islas, J.F. Prevalence of Stress in Healthcare Professionals during the COVID-19 Pandemic in Northeast Mexico: A Remote, Fast Survey Evaluation, Using an Adapted COVID-19 Stress Scales. Int. J. Environ. Res. Public Health 2020, 17, 7624. [Google Scholar] [CrossRef]
- Chew, N.W.S.; Lee, G.K.H.; Tan, B.Y.Q.; Jing, M.; Goh, Y.; Ngiam, N.J.H.; Yeo, L.L.L.; Ahmad, A.; Ahmed Khan, F.; Napolean Shanmugam, G.; et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav. Immun. 2020, 88, 559–565. [Google Scholar] [CrossRef]
- Zhang, W.R.; Wang, K.; Yin, L.; Zhao, W.F.; Xue, Q.; Peng, M.; Min, B.Q.; Tian, Q.; Leng, H.X.; Du, J.L.; et al. Mental Health and Psychosocial Problems of Medical Health Workers during the COVID-19 Epidemic in China. Psychother. Psychosom. 2020, 89, 242–250. [Google Scholar] [CrossRef]
- Dong, Z.-Q.; Ma, J.; Hao, Y.-N.; Shen, X.-L.; Liu, F.; Gao, Y.; Zhang, L. The social psychological impact of the COVID-19 epidemic on medical staff in China: A cross-sectional study. Eur. Psychiatry 2020, 1–22. [Google Scholar] [CrossRef]
- Xiao, X.; Zhu, X.; Fu, S.; Hu, Y.; Li, X.; Xiao, J. Psychological impact of healthcare workers in China during COVID-19 pneumonia epidemic: A multi-center cross-sectional survey investigation. J. Affect. Disord. 2020, 274, 405–410. [Google Scholar] [CrossRef]
- Salazar de Pablo, G.; Vaquerizo-Serrano, J.; Catalan, A.; Arango, C.; Moreno, C.; Ferre, F.; Shin, J.I.; Sullivan, S.; Brondino, N.; Solmi, M.; et al. Impact of coronavirus syndromes on physical and mental health of health care workers: Systematic review and meta-analysis. J. Affect. Disord. 2020, 275, 48–57. [Google Scholar] [CrossRef]
- Da Silva, F.C.T.; Neto, M.L.R. Psychiatric symptomatology associated with depression, anxiety, distress, and insomnia in health professionals working in patients affected by COVID-19: A systematic review with meta-analysis. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 104, 110057. [Google Scholar] [CrossRef]
- Sheraton, M.; Deo, N.; Dutt, T.; Surani, S.; Hall-Flavin, D.; Kashyap, R. Psychological effects of the COVID 19 pandemic on healthcare workers globally: A systematic review. Psychiatry Res. 2020, 292. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, J.; Luo, C.; Hu, S.; Lin, X.; Anderson, A.E.; Bruera, E.; Yang, X.; Wei, S.; Qian, Y. A Comparison of Burnout Frequency Among Oncology Physicians and Nurses Working on the Frontline and Usual Wards During the COVID-19 Epidemic in Wuhan, China. J. Pain Symptom Manag. 2020, 60, e60–e65. [Google Scholar] [CrossRef]
- Fumis, R.R.L.; Junqueira Amarante, G.A.; de Fátima Nascimento, A.; Vieira Junior, J.M. Moral distress and its contribution to the development of burnout syndrome among critical care providers. Ann. Intensive Care 2017, 7, 1–8. [Google Scholar] [CrossRef]
- Sanfilippo, F.; Noto, A.; Foresta, G.; Santonocito, C.; Palumbo, G.J.; Arcadipane, A.; Maybauer, D.M.; Maybauer, M.O. Incidence and factors associated with burnout in anesthesiology: A systematic review. Biomed Res. Int. 2017, 2017, 8648925. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- Downes, M.J.; Brennan, M.L.; Williams, H.C.; Dean, R.S. Development of a critical appraisal tool to assess the quality of cross-sectional studies (AXIS). BMJ Open 2016, 6, e011458. [Google Scholar] [CrossRef] [PubMed]
- Wahlster, S.; Sharma, M.; Lewis, A.K.; Patel, P.V.; Hartog, C.S.; Jannotta, G.; Blissitt, P.; Kross, E.K.; Kassebaum, N.J.; Greer, D.M.; et al. The Coronavirus Disease 2019 Pandemic’s Effect on Critical Care Resources and Health-Care Providers: A Global Survey. Chest 2021, 159, 619–633. [Google Scholar] [CrossRef]
- Azoulay, E.; Cariou, A.; Bruneel, F.; Demoule, A.; Kouatchet, A.; Reuter, D.; Souppart, V.; Combes, A.; Klouche, K.; Argaud, L.; et al. Symptoms of anxiety, depression, and peritraumatic dissociation in critical care clinicians managing patients with COVID-19 a cross-sectional study. Am. J. Respir. Crit. Care Med. 2020, 202, 1388–1398. [Google Scholar] [CrossRef]
- Sharma, R.; Saxena, A.; Magoon, R.; Jain, M.K. A cross-sectional analysis of prevalence and factors related to depression, anxiety, and stress in health care workers amidst the COVID-19 pandemic. Indian J. Anaesth. 2020, 64, S242–S244. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Fernández, M.D.; Ramos-Pichardo, J.D.; Ibáñez-Masero, O.; Cabrera-Troya, J.; Carmona-Rega, M.I.; Ortega-Galán, Á.M. Compassion fatigue, burnout, compassion satisfaction and perceived stress in healthcare professionals during the COVID-19 health crisis in Spain. J. Clin. Nurs. 2020, 29, 4321–4330. [Google Scholar] [CrossRef]
- De Wit, K.; Mercuri, M.; Wallner, C.; Clayton, N.; Archambault, P.; Ritchie, K.; Gérin-Lajoie, C.; Gray, S.; Schwartz, L.; Chan, T.; et al. Canadian emergency physician psychological distress and burnout during the first 10 weeks of COVID-19: A mixed-methods study. J. Am. Coll. Emerg. Physicians Open 2020, 1, 1030–1038. [Google Scholar] [CrossRef]
- Buselli, R.; Corsi, M.; Baldanzi, S.; Chiumiento, M.; Lupo, E.D.; Dell’oste, V.; Bertelloni, C.A.; Massimetti, G.; Dell’osso, L.; Cristaudo, A.; et al. Professional quality of life and mental health outcomes among health care workers exposed to SARS-CoV-2 (COVID-19). Int. J. Environ. Res. Public Health 2020, 17, 6180. [Google Scholar] [CrossRef]
- Tsan, S.E.H.; Kamalanathan, A.; Lee, C.K.; Zakaria, S.A.; Wang, C.Y. A survey on burnout and depression risk among anaesthetists during COVID-19: The tip of an iceberg? Anaesthesia 2021, 76, 8–10. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Sun, C.; Chen, J.J.; Jen, H.J.; Kang, X.L.; Kao, C.C.; Chou, K.R. A Large-Scale Survey on Trauma, Burnout, and Posttraumatic Growth among Nurses during the COVID-19 Pandemic. Int. J. Ment. Health Nurs. 2021, 30, 102–116. [Google Scholar] [CrossRef]
- Chor, W.P.D.; Ng, W.M.; Cheng, L.; Situ, W.; Chong, J.W.; Ng, L.Y.A.; Mok, P.L.; Yau, Y.W.; Lin, Z. Burnout amongst emergency healthcare workers during the COVID-19 pandemic: A multi-center study. Am. J. Emerg. Med. 2020, 46, 700–702. [Google Scholar] [CrossRef]
- Gomez, S.; Anderson, B.J.; Yu, H.; Gutsche, J.; Jablonski, J.; Martin, N.; Kerlin, M.P.; Mikkelsen, M.E. Benchmarking Critical Care Well-Being: Before and After the Coronavirus Disease 2019 Pandemic. Crit. Care Explor. 2020, 2, e0233. [Google Scholar] [CrossRef] [PubMed]
- Cao, J.; Wei, J.; Zhu, H.; Duan, Y.; Geng, W.; Hong, X.; Jiang, J.; Zhao, X.; Zhu, B. A Study of Basic Needs and Psychological Wellbeing of Medical Workers in the Fever Clinic of a Tertiary General Hospital in Beijing during the COVID-19 Outbreak. Psychother. Psychosom. 2020, 89, 252–254. [Google Scholar] [CrossRef] [PubMed]
- Chuang, C.H.; Tseng, P.C.; Lin, C.Y.; Lin, K.H.; Chen, Y.Y. Burnout in the intensive care unit professionals: A systematic review. Medcine 2016, 95, e5629. [Google Scholar] [CrossRef] [PubMed]
- Sanfilippo, F.; Palumbo, G.J.; Noto, A.; Pennisi, S.; Mineri, M.; Vasile, F.; Dezio, V.; Busalacchi, D.; Murabito, P.; Astuto, M. Prevalence of burnout among intensive care physicians: A systematic review. Rev. Bras. Ter. Intensiv. 2020, 32, 458–467. [Google Scholar] [CrossRef]
- Verougstraete, D.; Hachimi Idrissi, S. The impact of burn-out on emergency physicians and emergency medicine residents: A systematic review. Acta Clin. Belg. Int. J. Clin. Lab. Med. 2020, 75, 57–79. [Google Scholar] [CrossRef]
- Li, H.; Cheng, B.; Zhu, X.P. Quantification of burnout in emergency nurses: A systematic review and meta-analysis. Int. Emerg. Nurs. 2018, 39, 46–54. [Google Scholar] [CrossRef]
- Zhang, Q.; Mu, M.C.; He, Y.; Cai, Z.L.; Li, Z.C. Burnout in emergency medicine physicians: A meta-analysis and systematic review. Medicine 2020, 99, e21462. [Google Scholar] [CrossRef]
- Magnavita, N.; Chirico, F.; Garbarino, S.; Bragazzi, N.L.; Santacroce, E.; Zaffina, S. Sars/mers/sars-cov-2 outbreaks and burnout syndrome among healthcare workers. An umbrella systematic review. Int. J. Environ. Res. Public Health 2021, 18, 4361. [Google Scholar] [CrossRef] [PubMed]
- Amanullah, S.; Shankar, R.R. The impact of covid-19 on physician burnout globally: A review. Multidiscip. Digit. Publ. Inst. 2020, 8, 421. [Google Scholar] [CrossRef] [PubMed]
- Schneider, J.; Talamonti, D.; Gibson, B.; Forshaw, M. Factors mediating the psychological well-being of healthcare workers responding to global pandemics: A systematic review. J. Health Psychol. 2021, 135910532110127. [Google Scholar] [CrossRef]
- Danet Danet, A. Psychological impact of COVID-19 pandemic in Western frontline healthcare professionals. A systematic review. Med. Clín. 2021, 156, 449–458. [Google Scholar] [CrossRef]
- Laurent, A.; Fournier, A.; Lheureux, F.; Louis, G.; Nseir, S.; Jacq, G.; Goulenok, C.; Muller, G.; Badie, J.; Bouhemad, B.; et al. Mental health and stress among ICU healthcare professionals in France according to intensity of the COVID-19 epidemic. Ann. Intensive Care. 2021, 11, 90. [Google Scholar] [CrossRef]
- Laurent, A.; Bonnet, M.; Capellier, G.; Aslanian, P.; Hebert, P. Emotional Impact of End-of-Life Decisions on Professional Relationships in the ICU: An Obstacle to Collegiality? Crit. Care Med. 2017, 45, 2023–2030. [Google Scholar] [CrossRef] [PubMed]
- Ritchie, H.; Ortiz-Ospina, E.; Beltekian, D.; Mathieu, E.; Hasell, J.; Macdonald, B.; Giattino, C.; Appel, C.; Rodés-Guirao, L.; Roser, M. Coronavirus Pandemic (COVID-19). 2020, Published Online at OurWorldInData.org. Available online: https://ourworldindata.org/coronavirus (accessed on 26 July 2021).
- Galanis, P.; Vraka, I.; Fragkou, D.; Bilali, A.; Kaitelidou, D. Nurses’ burnout and associated risk factors during the COVID-19 pandemic: A systematic review and meta-analysis. J. Adv. Nurs. 2021, 77, 3286–3302. [Google Scholar] [CrossRef]
- Varghese, A.; George, G.; Kondaguli, S.V.; Naser, A.Y.; Khakha, D.C.; Chatterji, R. Decline in the mental health of nurses across the globe during COVID-19: A systematic review and meta-analysis. J. Glob. Health 2021, 11, 5009. [Google Scholar] [CrossRef]
- De Brier, N.; Stroobants, S.; Vandekerckhove, P.; De Buck, E. Factors affecting mental health of health care workers during coronavirus disease outbreaks (SARS, MERS & COVID-19): A rapid systematic review. PLoS ONE 2020, 15, e0244052. [Google Scholar]
- Sharifi, M.; Asadi-Pooya, A.A.; Mousavi-Roknabadi, R.S. Burnout among Healthcare Providers of COVID-19; a Systematic Review of Epidemiology and Recommendations. Arch. Acad. Emerg. Med. 2020, 9, 1–17. [Google Scholar]
- Della Monica, A.; Ferrara, P.; Dal Mas, F.; Cobianchi, L.; Scannapieco, F.; Ruta, F. The impact of Covid-19 healthcare emergency on the psychological well-being of health professionals: A review of literature. Ann. Ig. 2021. [Google Scholar] [CrossRef]
- Yan, H.; Ding, Y.; Guo, W. Mental Health of Medical Staff during the Coronavirus Disease 2019 Pandemic: A Systematic Review and Meta-Analysis. Psychosom. Med. 2021, 83, 387–396. [Google Scholar] [CrossRef]
- Sahebi, A.; Nejati-Zarnaqi, B.; Moayedi, S.; Yousefi, K.; Torres, M.; Golitaleb, M. The prevalence of anxiety and depression among healthcare workers during the COVID-19 pandemic: An umbrella review of meta-analyses. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 107, 110247. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Scherer, N.; Felix, L.; Kuper, H. Prevalence of depression, anxiety and posttraumatic stress disorder in health care workers during the COVID-19 pandemic: A systematic review and meta-Analysis. PLoS ONE 2021, 16, e0246454. [Google Scholar] [CrossRef]
- Mealer, M.; Moss, M. Should all ICU clinicians regularly be tested for burnout? We are not sure: Conceptual considerations that precede screening for burnout syndrome in ICU clinicians. Intensive Care Med. 2018, 44, 687–689. [Google Scholar] [CrossRef] [PubMed]
- West, C.P.; Dyrbye, L.N.; Erwin, P.J.; Shanafelt, T.D. Interventions to prevent and reduce physician burnout: A systematic review and meta-analysis. Lancet 2016, 388, 2272–2281. [Google Scholar] [CrossRef]
- Xu, H.; Kynoch, K.; Tuckett, A.; Eley, R. Effectiveness of interventions to reduce emergency department staff occupational stress and/or burnout: A systematic review. JBI Evid. Synth. 2020, 18, 1156–1188. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, F.C.T.; Barbosa, C.P. The impact of the COVID-19 pandemic in an intensive care unit (ICU): Psychiatric symptoms in healthcare professionals. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2021, 110, 110299. [Google Scholar] [CrossRef] [PubMed]
- Pollock, A.; Campbell, P.; Cheyne, J.; Cowie, J.; Davis, B.; McCallum, J.; McGill, K.; Elders, A.; Hagen, S.; McClurg, D.; et al. Interventions to support the resilience and mental health of frontline health and social care professionals during and after a disease outbreak, epidemic or pandemic: A mixed methods systematic review. Cochrane Database Syst. Rev. 2020, 11, CD013779. [Google Scholar]

| PICOS Strategy | |
|---|---|
| Population | HCWs (e.g., physicians, residents, nurses, administrative, pharmacists, therapists) employed in ICU/ED |
| Intervention | Working in a critical department (ICU/ED) during the COVID-19 pandemic |
| Comparison | None |
| Outcomes | Prevalence of burnout or level of burnout during the COVID-19 pandemic |
| Studies | Any type |
| 1st Author | Risk Factors for Burnout in ICU/ED Healthcare Workers |
|---|---|
| Sharma M et al. [25] | Adjusted relative risk: aRR [IC 95%] Insufficient access to PPE: 1.43 [1.32–1.55]; p < 0.01 Poor communication from supervisors: 1.13 [1.06–1.21]; p < 0.01 Worries about financial situation: 1.09 [1.01–1.18]; p 0.02 Social stigma from community: 1.32 [1.24–1.41]; p < 0.01 |
| de Wit K et al. [27] | Factors associated with emotional exhaustion: Having being tested for COVID-19 [OR = 11.5, 95% CI (3.1–42.5)] Number of shifts worked [(OR = 1.3, 95% CI (1.1–1.5) per additional shift, per week] Factors associated with depersonalization: Having been tested for COVID-19 [(OR 4.3, 95% CI (1.1–17.8)] |
| Buselli R et al. [28] | Burnout presented a significant positive association with the PHQ-9 scores [b = 0.4 (SE = 0.10), p < 0.001] and with the GAD-7 scores [(b = 0.20 (SE = 0.06), p = 0.001)] |
| Tsan SEH et al. [29] | Burnout and depression risk were associated each other (p < 0.0001). Burnout is associated with number of calls per week (p = 0.038) and worry regarding COVID-19 (p = 0.014) |
| Azoulay E et al. [24] | Age and female gender were also associated with a higher prevalence of severe burnout (45 [37–51] vs. 47 years [40–55], p = 0.0001, and 38.2% vs. 30.1%, p = 0.02). Clinicians with symptoms of anxiety, depression, or severe burnout were more frequently smoking or taking sleeping pills, whereas alcohol consumption was not affected. The number of COVID-19 patients managed was not associated with the prevalence of the psychological burden. Factors independently associated with symptoms of severe burnout included age (HR 0.98/year [0.97–0.99]) and clinician’s rating about the ethical climate (HR 0.76 [0.69–0.82]) |
| Chor WPD et al. [31] | Staff who were originally working in the ED or UCC before the COVID-19 pandemic also had a higher rate of moderate-to-severe personal burnout as compared to those compared to those deployed from other departments (90.4% versus 9.6%, p = 0.004) |
| Gomez S et al. [32] | Among those with burnout, the strongest driver of burnout was related to workload and job demands. Conversely, meaning in work, social support and community at work, and culture and values of work community appeared to be protective of developing burnout as sources of well-being (p < 0.001). |
| Wahlster S et al. [23] | Adjusted relative risk: aRR [IC 95%] Being female 1.16 (1.01–1.33) p = 0.03 Being a nurse 1.31 (1.13–1.53) p = 0.01 Caring for 10 to 50 patients 1.17 (1.04–1.33) p = 0.01 Caring > 50 patients 1.28 (1.06–1.53) p = 0.01 Poor communication from supervisors 1.30 (1.16–1.46) p < 0.001 Limited availability of PAPRs 1.30 (1.09–1.55) p < 0.001 Lack of nurses 1.18 (1.05–1.33) p = 0.01 Providers in Europe and Central Asia were 14% less likely to report burnout than were providers in North America 0.86 (0.75–1.00) p = 0.04. |
| AXIS Items | Sharma M [25] | Ruiz-Fernàndez MD [26] | de Wit K [27] | Tsan SHE [29] | Azoulay E [24] | Chor WPD [31] | Gomez S [32] | Buselli R [28] | Cao J [33] | Chen R [30] | Wahlster S [23] |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Were the aims/objectives of the study clear? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 | 1 | 1 |
| 2. Was the study design appropriate for the stated aim(s)? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 3. Was the sample size justified | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 |
| 4. Was the target/reference population clearly defined? (Is it clear who the research was about?) | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 5. Was the sample frame taken from an appropriate population base so that it closely represented the target/reference population under investigation? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 6. Was the selection process likely to select subjects/participants that were representative of the target/reference population under investigation? | 0 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| 7. Were measures undertaken to address and categorize non-responders? | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 8. Were the risk factor and outcome variables measured appropriate to the aims of the study? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 9. Were the risk factor and outcome variables measured correctly using instruments/measurements that had been trialed, piloted or published previously? | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 0 |
| 10. Is it clear what was used to determined statistical significance and/or precision estimates? (e.g., p values, CIs)? | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 0 |
| 11. Were the methods (including statistical methods) sufficiently described to enable them to be repeated? | 0 | 1 | 1 | 0 | 1 | 0 | 1 | 1 | 0 | 1 | 1 |
| 12. Were the basic data adequately described? | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 0 | 1 | 1 |
| 13. Does the response rate raise concerns about non-response bias? | 0 | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 0 | 0 | 1 |
| 14. If appropriate, was information about non-responders described? | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 |
| 15. Were the results internally consistent? | 1 | 1 | 1 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 |
| 16. Were the results for the analyses described in the methods, presented? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 17. Were the authors’ discussions and conclusions justified by the results? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 18. Were the limitations of the study discussed? | 1 | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 0 | 1 | 1 |
| 19. Were there any funding sources or conflicts of interest that may affect the authors’ interpretation of the results? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 20. Was ethical approval or consent of participants attained? | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| % satisfied criteria | 60% | 75% | 80% | 65% | 75% | 65% | 80% | 80% | 55% | 80% | 70% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gualano, M.R.; Sinigaglia, T.; Lo Moro, G.; Rousset, S.; Cremona, A.; Bert, F.; Siliquini, R. The Burden of Burnout among Healthcare Professionals of Intensive Care Units and Emergency Departments during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8172. https://doi.org/10.3390/ijerph18158172
Gualano MR, Sinigaglia T, Lo Moro G, Rousset S, Cremona A, Bert F, Siliquini R. The Burden of Burnout among Healthcare Professionals of Intensive Care Units and Emergency Departments during the COVID-19 Pandemic: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(15):8172. https://doi.org/10.3390/ijerph18158172
Chicago/Turabian StyleGualano, Maria Rosaria, Tiziana Sinigaglia, Giuseppina Lo Moro, Stefano Rousset, Agnese Cremona, Fabrizio Bert, and Roberta Siliquini. 2021. "The Burden of Burnout among Healthcare Professionals of Intensive Care Units and Emergency Departments during the COVID-19 Pandemic: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 15: 8172. https://doi.org/10.3390/ijerph18158172