
Oral Health Interventions in Patients with a Mental Health Disorder: A Scoping Review with Critical Appraisal of the Literature

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Stage 1. To Identify the Research Question
2.2. Stage 2. Identifying Relevant Studies
2.3. Stage 3. Study Selection
2.4. Stage 4. Charting the Data
2.5. Stage 5. Collating, Summarizing and Reporting the Results
2.6. Ethics and Dissemination
3. Results
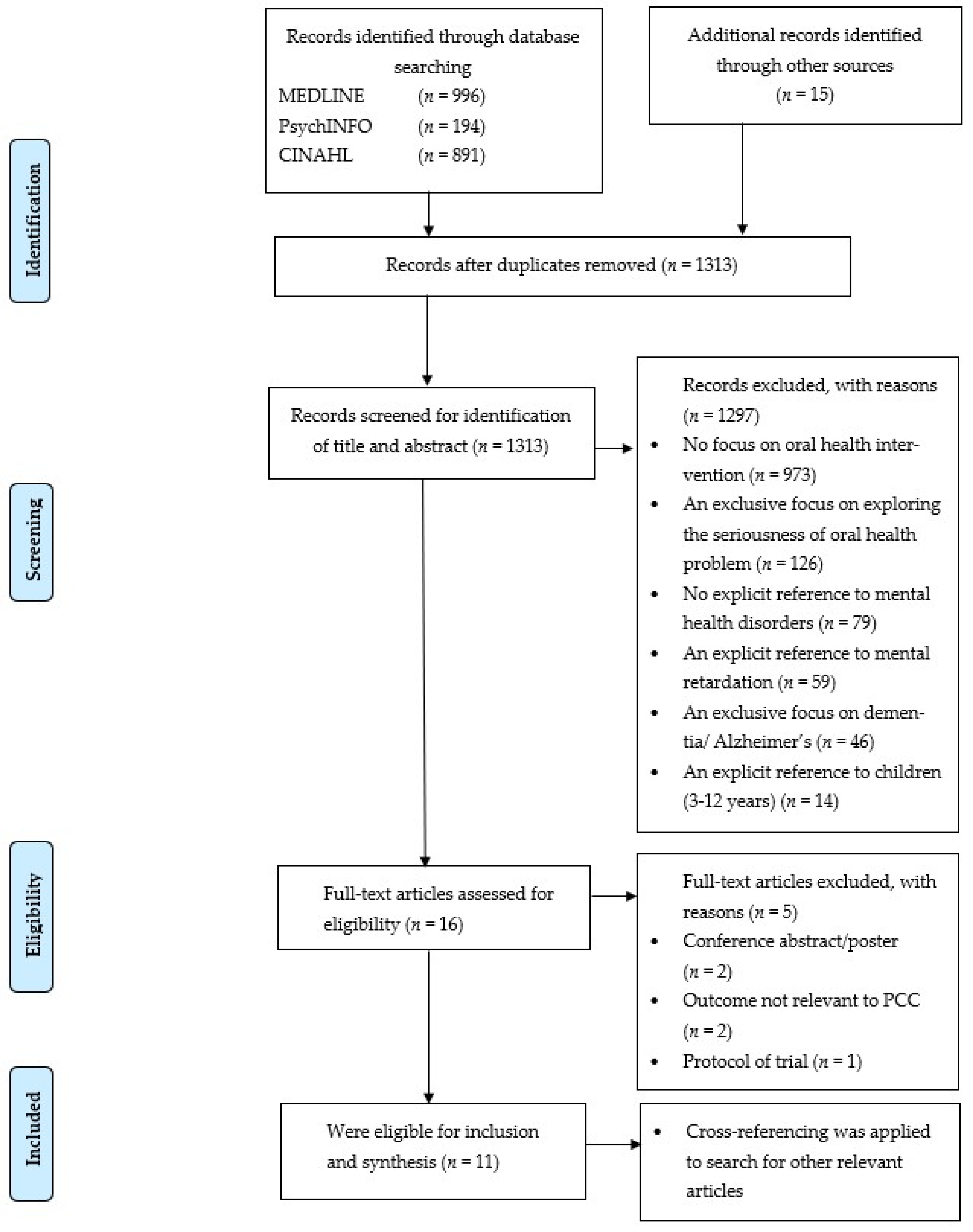
3.1. Literature Search
3.2. Article Information
3.3. Methodological Quality
3.4. Syntheses: Narrative Summary of Themes
3.4.1. Educational Interventions
3.4.2. Physical Interventions
3.4.3. Interventions Combining Behavioural and Educational Elements
3.4.4. Interventions Combining Educational and Physical Elements
4. Discussion
4.1. Reflection on Types of Interventions
4.2. Quality of Included Studies
4.3. Reflection on the Effect of Interventions
4.4. Competences of Mental Health Professionals in Studied Interventions
4.5. Study Strengths and Methodological Considerations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Search Strategy
References
- Petersen, P.E. The World Oral Health Report 2003: Continuous Improvement of Oral Health in the 21st Century—The Approach of the WHO Global Oral Health Programme: The World Oral Health Report 2003. Community Dent. Oral Epidemiol. 2003, 31, 3–24. [Google Scholar] [CrossRef]
- Petersen, P.E. Priorities for Research for Oral Health in the 21st Century—The Approach of the WHO Global Oral Health Programme. Community Dent. Health 2005, 22, 71–74. [Google Scholar]
- Kisely, S.; Quek, L.-H.; Pais, J.; Lalloo, R.; Johnson, N.W.; Lawrence, D. Advanced Dental Disease in People with Severe Mental Illness: Systematic Review and Meta-Analysis. Br. J. Psychiatry 2011, 199, 187–193. [Google Scholar] [CrossRef] [Green Version]
- Cullinan, M.; Ford, P.; Seymour, G. Periodontal Disease and Systemic Health: Current Status. Aust. Dent. J. 2009, 54, S62–S69. [Google Scholar] [CrossRef]
- Kinane, D.F.; Mombelli, A. (Eds.) Periodontal Disease; Frontiers of Oral Biology; S. Karger AG: Basel, Switzerland, 2011; Volume 15, ISBN 978-3-8055-9833-0. [Google Scholar]
- Scannapieco, F.A.; Papandonatos, G.D.; Dunford, R.G. Associations Between Oral Conditions and Respiratory Disease in a National Sample Survey Population. Ann. Periodontol. 1998, 3, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Haffajee, A.D.; Socransky, S.S. Relation of Body Mass Index, Periodontitis and Tannerella forsythia. J. Clin. Periodontol. 2009, 36, 89–99. [Google Scholar] [CrossRef]
- Batty, G.D.; Jung, K.J.; Mok, Y.; Lee, S.J.; Back, J.H.; Lee, S.; Jee, S.H. Oral Health and Later Coronary Heart Disease: Cohort Study of One Million People. Eur. J. Prev. Cardiol. 2018, 25, 598–605. [Google Scholar] [CrossRef] [Green Version]
- Makkar, H.; Reynolds, M.A.; Wadhawan, A.; Dagdag, A.; Merchant, A.T.; Postolache, T.T. Periodontal, Metabolic, and Cardiovascular Disease: Exploring the Role of Inflammation and Mental Health. Pteridines 2018, 29, 124–163. [Google Scholar] [CrossRef] [PubMed]
- Steel, Z.; Marnane, C.; Iranpour, C.; Chey, T.; Jackson, J.W.; Patel, V.; Silove, D. The Global Prevalence of Common Mental Disorders: A Systematic Review and Meta-Analysis 1980–2013. Int. J. Epidemiol. 2014, 43, 476–493. [Google Scholar] [CrossRef] [Green Version]
- Cormac, I.; Jenkins, P. Understanding the Importance of Oral Health in Psychiatric Patients. Adv. Psychiatr. Treat. 1999, 5, 53–60. [Google Scholar] [CrossRef] [Green Version]
- De Hert, M.; Mauri, M.; Shaw, K.; Wetterling, T.; Doble, A.; Giudicelli, A.; Falissard, B. The METEOR Study of Diabetes and Other Metabolic Disorders in Patients with Schizophrenia Treated with Antipsychotic Drugs. I. Methodology: Metabolic Disorders in Schizophrenia. Int. J. Methods Psychiatr. Res. 2010, 19, 195–210. [Google Scholar] [CrossRef]
- Kuipers, S.; Castelein, S.; Malda, A.; Kronenberg, L.; Boonstra, N. Oral Health Experiences and Needs among Young Adults after a First-Episode Psychosis: A Phenomenological Study. J. Psychiatr. Ment. Health Nurs. 2018, 25, 475–485. [Google Scholar] [CrossRef] [PubMed]
- Mirza, I.; Day, R.; Phelan, M.; Wulff-Cochrane, V. Oral Health of Psychiatric In-Patients: A Point Prevalence Survey of an Inner-City Hospital. Psychiatr. Bull. 2001, 25, 143–145. [Google Scholar] [CrossRef]
- Slack-Smith, L.; Hearn, L.; Scrine, C.; Durey, A. Barriers and Enablers for Oral Health Care for People Affected by Mental Health Disorders. Aust. Dent. J. 2017, 62, 6–13. [Google Scholar] [CrossRef] [Green Version]
- Griffiths Oral Health Care for People with Mental Health Problems_Guidelines and Recommendations. 2000. Available online: http://www.bsdh.org/documents/mental.pdf (accessed on 9 June 2021).
- McCreadie, R.G.; Stevens, H.; Henderson, J.; Hall, D.; McCaul, R.; Filik, R.; Young, G.; Sutch, G.; Kanagaratnam, G.; Perrington, S.; et al. The Dental Health of People with Schizophrenia. Acta Psychiatr. Scand. 2004, 110, 306–310. [Google Scholar] [CrossRef]
- Kilbourne, A.M.; Horvitz-Lennon, M.; Post, E.P.; McCarthy, J.F.; Cruz, M.; Welsh, D.; Blow, F.C. Oral Health in Veterans Affairs Patients Diagnosed with Serious Mental Illness. J. Public Health Dent. 2007, 67, 42–48. [Google Scholar] [CrossRef]
- Ponizovsky, A.M.; Zusman, S.P.; Dekel, D.; Masarwa, A.-S.; Ramon, T.; Natapov, L.; Yoffe, R.; Weizman, A.; Grinshpoon, A. Effect of Implementing Dental Services in Israeli Psychiatric Hospitals on the Oral and Dental Health of Inpatients. Psychiatr. Serv. Wash. 2009, 60, 5. [Google Scholar] [CrossRef]
- Sjogren, R.; Nordstrom, G. Oral Health Status of Psychiatric Patients. J. Clin. Nurs. 2000, 9, 632–638. [Google Scholar] [CrossRef]
- Stiefel, D.J.; Truelove, E.L.; Menard, T.W.; Anderson, V.K.; Doyle, P.E.; Mandel, L.S. A Comparison of the Oral Health of Persons with and without Chronic Mental Illness in Community Settings. Spec. Care Dent. 1990, 10, 6–12. [Google Scholar] [CrossRef]
- Friedlander, A.H.; Liberman, R.P. Oral Health Care for the Patient with Schizophrenia. Spec. Care Dent. 1991, 11, 179–183. [Google Scholar] [CrossRef]
- Persson, K.; Axtelius, B.; Söderfeldt, B.; Östman, M. Monitoring Oral Health and Dental Attendance in an Outpatient Psychiatric Population. J. Psychiatr. Ment. Health Nurs. 2009, 16, 263–271. [Google Scholar] [CrossRef]
- Lu, H.-X.; Chen, X.-L.; Wong, M.; Zhu, C.; Ye, W. Oral Health Impact of Halitosis in Chinese Adults. Int. J. Dent. Hyg. 2017, 15, e85–e92. [Google Scholar] [CrossRef]
- Renvert, S.; Noack, M.J.; Lequart, C.; Roldán, S.; Laine, M.L. The Underestimated Problem of Intra-Oral Halitosis in Dental Practice: An Expert Consensus Review. Clin. Cosmet. Investig. Dent. 2020, 12, 251–262. [Google Scholar] [CrossRef]
- Kisely, S.; Baghaie, H.; Lalloo, R.; Siskind, D.; Johnson, N.W. A Systematic Review and Meta-Analysis of the Association Between Poor Oral Health and Severe Mental Illness. Psychosom. Med. 2015, 77, 83–92. [Google Scholar] [CrossRef]
- Dagnew, Z.A.; Abraham, I.A.; Beraki, G.G.; Tesfamariam, E.H.; Mittler, S.; Tesfamichael, Y.Z. Nurses’ Attitude towards Oral Care and Their Practicing Level for Hospitalized Patients in Orotta National Referral Hospital, Asmara-Eritrea: A Cross-Sectional Study. BMC Nurs. 2020, 19, 63. [Google Scholar] [CrossRef]
- de Mey, L.; Çömlekçi, C.; de Reuver, F.; van Waard, I.; van Gool, R.; Scheerman, J.F.M.; van Meijel, B. Oral Hygiene in Patients with Severe Mental Illness: A Pilot Study on the Collaboration between Oral Hygienists and Mental Health Nurses: Oral Hygiene in Patients with Severe Mental Illness: A Pilot Study on the Collaboration Between Oral Hygienists and Mental Health Nurses. Perspect. Psychiatr. Care 2016, 52, 194–200. [Google Scholar] [CrossRef]
- NICE Guideline. Oral Health Promotion: General Dental Practice: Guidance (NG30); National Institute for Health and Care Excellence: London, UK, 2015; pp. 1–39. [Google Scholar]
- Cleves, A.J.; Jones, M.; Morgan, H.E.; Alam, F. Oral Health for Adults in Care Homes: NICE Guideline (NG48); National Institute for Health and Care Excellence: London, UK, 2015. [Google Scholar]
- Kisely, S.; Ehrlich, C.; Kendall, E.; Lawrence, D. Using Avoidable Admissions to Measure Quality of Care for Cardiometabolic and Other Physical Comorbidities of Psychiatric Disorders: A Population-Based, Record-Linkage Analysis. Can. J. Psychiatry 2015, 60, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Peters, M.D.J.; Godfrey, C.M.; Khalil, H.; McInerney, P.; Parker, D.; Soares, C.B. Guidance for Conducting Systematic Scoping Reviews. Int. J. Evid. Based Healthc. 2015, 13, 141–146. [Google Scholar] [CrossRef] [Green Version]
- Arksey, H.; O’Malley, L. Scoping Studies: Towards a Methodological Framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Tufanaru, C.; Munn, Z.; Aromataris, E.; Campbell, J.; Hopp, L. Chapter 3: Systematic Reviews of Effectiveness. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; ISBN 978-0-648-84880-6. [Google Scholar]
- Moola, S.; Munn, Z.; Tufanaru, C.; Aromataris, E.; Sears, K.; Sfetc, R.; Currie, M.; Lisy, K.; Qureshi, R.; Mattis, P.; et al. Chapter 7: Systematic Reviews of Etiology and Risk. In JBI Manual for Evidence Synthesis; Aromataris, E., Munn, Z., Eds.; JBI: Adelaide, Australia, 2020; ISBN 978-0-648-84880-6. [Google Scholar]
- Grant, M.J.; Booth, A. A Typology of Reviews: An Analysis of 14 Review Types and Associated Methodologies: A Typology of Reviews. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Brien, S.E.; Lorenzetti, D.L.; Lewis, S.; Kennedy, J.; Ghali, W.A. Overview of a Formal Scoping Review on Health System Report Cards. Implement. Sci. 2010, 5, 2. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef] [PubMed]
- Peters, M.D.J.; Marnie, C.; Tricco, A.C.; Pollock, D.; Munn, Z.; Alexander, L.; McInerney, P.; Godfrey, C.M.; Khalil, H. Updated Methodological Guidance for the Conduct of Scoping Reviews. JBI Evid. Synth. 2020, 18, 2119–2126. [Google Scholar] [CrossRef] [PubMed]
- Glick, M.; Williams, D.M.; Kleinman, D.V.; Vujicic, M.; Watt, R.G.; Weyant, R.J. A New Definition for Oral Health Developed by the FDI World Dental Federation Opens the Door to a Universal Definition of Oral Health. Br. Dent. J. 2016, 221, 792–793. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders (DSM-5); American Psychiatric Asociation: Washington, DC, USA, 2013. [Google Scholar] [CrossRef]
- Lawrence, A.; Houghton, J.; Thomas, J. Where Is the Evidence: Realising the Value of Grey Literature for Public Policy and Practice; Swinburne Institute for Social Research: Melbourne, Australia, 2014. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater Reliability: The Kappa Statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Adams, C.E.; Wells, N.C.; Clifton, A.; Jones, H.; Simpson, J.; Tosh, G.; Callaghan, P.; Liddle, P.; Guo, B.; Furtado, V.; et al. Monitoring Oral Health of People in Early Intervention for Psychosis (EIP) Teams: The Extended Three Shires Randomised Trial. Int. J. Nurs. Stud. 2018, 77, 106–114. [Google Scholar] [CrossRef] [Green Version]
- Almomani, F.; Brown, C.; Williams, K.B. The Effect of an Oral Health Promotion Program for People with Psychiatric Disabilities. Psychiatr. Rehabil. J. 2006, 29, 274–281. [Google Scholar] [CrossRef]
- Almomani, F.; Williams, K.; Catley, D.; Brown, C. Effects of an Oral Health Promotion Program in People with Mental Illness. J. Dent. Res. 2009, 88, 648–652. [Google Scholar] [CrossRef]
- Kuo, M.-W.; Yeh, S.-H.; Chang, H.-M.; Teng, P.-R. Effectiveness of Oral Health Promotion Program for Persons with Severe Mental Illness: A Cluster Randomized Controlled Study. BMC Oral Health 2020, 20, 290. [Google Scholar] [CrossRef]
- Singhal, V.; Heuer, A.J.; York, J.; Gill, K.J. The Effects of Oral Health Instruction, and the Use of a Battery-Operated Toothbrush on Oral Health of Persons with Serious Mental Illness: A Quasi-Experimental Study. Community Ment. Health J. 2021, 57, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Mori, Y.; Amano, A.; Akiyama, S.; Morisaki, I. Effects of Short Professional Mechanical Tooth-Cleaning (PMTC) Program in Young Adults with Mental Disabilities. Spec. Care Dent. 2000, 20, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Barbadoro, P.; Lucrezi, D.; Prospero, E.; Annino, I. Improvement of Knowledge, Attitude, and Behavior about Oral Health in a Population of Alcohol Addicted Persons. Alcohol Alcohol 2008, 43, 347–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khokhar, W.; Williams, K.; Odeyemi, O.; Clarke, T.; Tarrant, C.; Clifton, A. Open Wide: A Dental Health and Toothbrush Exchange Project at an Inpatient Recovery and Rehabilitation Unit. Ment. Health Rev. J. 2011, 16, 36–41. [Google Scholar] [CrossRef]
- Silverstein, L.S.; Haggerty, C.; Sams, L.; Phillips, C.; Roberts, M.W. Impact of an Oral Health Education Intervention among a Group of Patients with Eating Disorders (Anorexia Nervosa and Bulimia Nervosa). J. Eat. Disord. 2019, 7, 29. [Google Scholar] [CrossRef] [PubMed]
- Yoshii, H.; Kitamura, N.; Akazawa, K.; Saito, H. Effects of an Educational Intervention on Oral Hygiene and Self-Care among People with Mental Illness in Japan: A Longitudinal Study. BMC Oral Health 2017, 17, 81. [Google Scholar] [CrossRef] [Green Version]
- Lam, P.C.; John, D.A.; Galfalvy, H.; Kunzel, C.; Lewis-Fernández, R. Oral Health–Related Quality of Life Among Publicly Insured Mental Health Service Outpatients with Serious Mental Illness. Psychiatr. Serv. 2019, 70, 1101–1109. [Google Scholar] [CrossRef]
- Alqahtani, F.; Al Khalifah, G.; Oyebode, O.; Orji, R. Apps for Mental Health: An Evaluation of Behavior Change Strategies and Recommendations for Future Development. Front. Artif. Intell. 2019, 2, 30. [Google Scholar] [CrossRef] [Green Version]
- Kay, E.J.; Locker, D. Is Dental Health Education Effective? A Systematic Review of Current Evidence. Community Dent. Oral Epidemiol. 1996, 24, 231–235. [Google Scholar] [CrossRef]
- Juni, P. Systematic Reviews in Health Care: Assessing the Quality of Controlled Clinical Trials. BMJ 2001, 323, 42–46. [Google Scholar] [CrossRef]
- Probst, P.; Grummich, K.; Heger, P.; Zaschke, S.; Knebel, P.; Ulrich, A.; Büchler, M.W.; Diener, M.K. Blinding in Randomized Controlled Trials in General and Abdominal Surgery: Protocol for a Systematic Review and Empirical Study. Syst. Rev. 2016, 5, 48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schweizer, M.L.; Braun, B.I.; Milstone, A.M. Research Methods in Healthcare Epidemiology and Antimicrobial Stewardship—Quasi-Experimental Designs. Infect. Control Hosp. Epidemiol. 2016, 37, 1135–1140. [Google Scholar] [CrossRef] [Green Version]
- Howards, P.P. An Overview of Confounding. Part 1: The Concept and How to Address It. Acta Obstet. Gynecol. Scand. 2018, 97, 394–399. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jager, K.J.; Zoccali, C.; MacLeod, A.; Dekker, F.W. Confounding: What It Is and How to Deal with It. Kidney Int. 2008, 73, 256–260. [Google Scholar] [CrossRef] [Green Version]
- Cirelli, T.; de Oliveira, G.J.P.L.; Nogueira, A.V.B.; Ribaldo, I.J.P.; Furuta, E.Y.D.; Cirelli, J.A. Effect of Electric, Ultrasonic and Manual Toothbrushes on Biofilm Removal and Gingivitis Control: In Vitro and Parallel Randomized Controlled Clinical Trial Study. Braz. J. Oral Sci. 2021, 20, e219280. [Google Scholar] [CrossRef]
- Lee, D.-S.; Kim, M.; Nam, S.-H.; Kang, M.-S.; Lee, S.-A. Effects of Oral Probiotics on Subjective Halitosis, Oral Health, and Psychosocial Health of College Students: A Randomized, Double-Blind, Placebo-Controlled Study. Int. J. Environ. Res. Public. Health 2021, 18, 1143. [Google Scholar] [CrossRef] [PubMed]
- Edward, K.-L.; Felstead, B.; Mahoney, A.-M. Hospitalized Mental Health Patients and Oral Health: Oral Health. J. Psychiatr. Ment. Health Nurs. 2012, 19, 419–425. [Google Scholar] [CrossRef] [PubMed]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic Review or Scoping Review? Guidance for Authors When Choosing between a Systematic or Scoping Review Approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | I Educational Intervention | II Physical Intervention | III Interventions Combining Behavioral and Educational Elements | IV Interventions Combining Educational and Physical Elements | ||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Prof | Patient Group | Prof | Patient Group | Prof | Patient Group | Prof | Patient Group | |||||||||||||||||||||||||||||||||
| SMI | PSD | PD | MD | AD | ASD | ED | SAD | SMI | PSD | PD | MD | AD | ASD | ED | SAD | SMI | PSD | PD | MD | AD | ASD | ED | SAD | SMI | PSD | PD | MD | AD | ASD | ED | SAD | |||||||||
| Randomised controlled trials | ||||||||||||||||||||||||||||||||||||||||
| Adams et al. [45] | x | x | ||||||||||||||||||||||||||||||||||||||
| Almomani et al. [46] | x | x | ||||||||||||||||||||||||||||||||||||||
| Almomani et al. [47] | x | x | ||||||||||||||||||||||||||||||||||||||
| Kuo et al. [48] | x | |||||||||||||||||||||||||||||||||||||||
| Quasi-experi-mental studies | ||||||||||||||||||||||||||||||||||||||||
| Barbadoro et al. [51] | x | |||||||||||||||||||||||||||||||||||||||
| Khokhar et al. [52] | x | |||||||||||||||||||||||||||||||||||||||
| De Meij et al. [28] | x | x | x | x | x | x | ||||||||||||||||||||||||||||||||||
| Mori et al. [50] | x | |||||||||||||||||||||||||||||||||||||||
| Silverstein et al. [53] | x | |||||||||||||||||||||||||||||||||||||||
| Singal et al. [49] | x | |||||||||||||||||||||||||||||||||||||||
| Cohort study | ||||||||||||||||||||||||||||||||||||||||
| Yoshii et al. [54] | x | x | x | |||||||||||||||||||||||||||||||||||||
| First Author, Year Publication | Total N | Type of Study | Population | Age in Years | Gender % Man | Setting (Recruitment)/Country | Type of Oral Health Interventions | Outcome | Measurement Instrument | Assessment Time |
|---|---|---|---|---|---|---|---|---|---|---|
| Adams et al. [45] | 35 EIP teams and their service users (N = > 1682) | RCT | Suspected psychosis Outpatients | 15–56 | 66% | EIP Teams, Manchester, United Kingdom | Interventions combining behavioural and educational elements | Behaviour towards oral health | Oral health: OIDP checklist Behaviour: general questionnaire: registered with dentist, routine check-up | Baseline, 12 months |
| Knowledge: dental awareness training | Owning a toothbrush, cleaning teeth twice a day, urgent dental treatment. | |||||||||
| Almomani et al. [46] | N = 50 | RCT | Schizophrenia Bipolar disorder, depression Outpatients | 19–61 | 46% | Communitysupport programme, Kansas, USA | Interventions combining behavioural and educational elements | Behaviour: oral health instruct-tions and reminder system. Knowledge: dental education | Plaque: Quigley-Hein plaque index. Knowledge: Questionnaire oral hygiene | Baseline, 4 weeks |
| Almomani et al. [47] | N = 60 | RCT | Schizophrenia Bipolar disorder, depression Outpatients | 22–58 | 50% | Community support programme, Kansas, USA | Interventions combining behavioural and educational elements | Behaviour in oral health: MI Knowledge on oral health. | Behaviour: TRSQ Plaque: Quigley-Hein plaque index. Knowledge: 15-item oral health knowledge questionnaire. | Baseline, 4 weeks, 8 weeks |
| Kuo et al. [48] | N = 58 | RCT | SMI Inpatients | 20–80 | 100% | Two psychiatric wards of a general hospital, Taiwan | Interventions combining behavioural and educational elements | Plaque accumulation | Plaque: Plaque control record | 12 weeks |
| Oral health promotion programme: oral health knowledge, attitude and behaviour | Knowledge, behaviour, attitude: 35 item questionnaire | |||||||||
| Barbadoro et al. [51] | N = 76 | QES | Alcohol-addiction Inpatients | Not clear | 76.3% | Residential rehabilitation clinic, Italy | Educational intervention | Knowledge on oral health and risk factors. | Knowledge: 10-item test assessing knowledge and consciousness | 12 months |
| Khokhar et al. [52] | N = 59 | QES | SMI Inpatients | 22–76 | 68% | Heather Close Recovery Unit, Mansfield, UK | Educational intervention | Knowledge on importance of dental care | General questionnaire: Access to toothbrushes, registered at dentist, dentures checked in last 5 years. Knowledge of basic oral hygiene. | 12 months |
| De Mey et al. [28] | N = 27 (Pr) N = 24 (P) | QES | Psychotic, Personality Mood, Anxiety, Autism disorders | 22–69 | Not known | Mental health organisation, the Netherlands | Interventions combining educational and physical elements | Knowledge nurses: oral care and tools, diseases, alcohol, smoking and drugs | Nurses knowledge: 20-items knowledge of oral hygiene. | Baseline, 5 weeks |
| Outpatients | Oral health in patients. | Oral health: Patients: Dental plaque index. Gingival bleeding index | ||||||||
| Mori et al. [50] | N = 10 | QES | Autism, mental health retardation, Hydrocephalus Outpatients | 21–29 | 90% | Special care dentistry, Osaka University Dental Hospital, Japan | Physical intervention | Oral health: reduction of bleeding sites on probing | Caries activity test (pH-meter) Debris index, Probing depth, bleeding on probing | Baseline, 2 weeks, 6 weeks, 14 weeks |
| Silverstein et al. [53] | N = 67 | QES | AN-BP and BN Inpatients | 13–50 | Hospital eating disorder clinic, North Carolina | Educational intervention | Knowledge on oral health and habits, hygiene practices. | Oral health knowledge, oral habits, oral health behaviours and habits since diagnosis, self-perception. | Baseline, and after following the programme. | |
| Singhal et al. [49] | N-87 | QES | SMI Outpatients | 18–83 | Not known | Rural and urban outpatient mental wellness centre, New Jersey USA | Interventions Combining Behavioural and Educational Elements | Oral hygiene education and battery-operated toothbrush or manual toothbrush | Oral health: Quigley-Hein plaque index and gingival index | Baseline, 12 weeks |
| Level of negative symptoms related to SMI | Self-evaluation of negative symptoms survey (SNS) | |||||||||
| Yoshii et al. [54] | N = 390 | Cohort study | Mental illness, Psychotic and mood disorders Outpatients | 20–80 | Not known | Psychiatric day-care centres, Japan | Educational intervention | Knowledge: cause of tooth loss, dental caries, dental cleaning periodontal disease and routine dental check-ups. | Knowledge: 20-item selfcare questionnaire | Baseline, 1 week, 1 month, 3 months, 6 months. |
| First Author, Year Publication | Intervention Group (N) | Control Group (N) | Intervention | Comparator | Results | Effect +/− |
|---|---|---|---|---|---|---|
| Adams et al. [45] | 18 EIP teams | 17 EIP teams | Dental awareness training. Dental checklist. Oral hygiene information sheet with oral hygiene tips and information on how to find a dentist. | Standard care. One year after intervention: Dental awareness training, checklist and oral hygiene information sheet. | No significant differences were found in: registered with dentist (p = 0.44), routine check-up (p = 0.18), owning a toothbrush (p = 0.99), cleaning teeth twice a day (p = 0.68), urgent dental treatment (p = 0.11), OIDP checklist: no prospective data collected. | − |
| Almomani et al. [46] | N = 20 | N = 22 | Dental education. Oral hygiene instructions. Mechanical toothbrush. Reminder system. | Mechanical toothbrushes. | Q.H. plaque index: The improvement in the intervention group was significantly higher than the control group (p = 0.026). Of them, 95% reported that reminders and oral health promotion were helpful | + |
| Almomani et al. [47] | N = 30 | N = 30 | Brief MI sessions on motivation and confidence, personal values. Educational sessions: exploring advantages and disadvantages oral hygiene, effects of SMI on oral health. Two pamphlets summarizing the info from education and instruction in using a mechanical toothbrush. Weekly phone calls (for 4 weeks). | Educational sessions: exploring advantages and disadvantages oral hygiene, effects SMI on oral health. Two pamphlets summarising the info from education and instruction in using a mechanical toothbrush. Weekly phone calls (for 4 weeks). | Q.H. plaque index: scores from the inter-vention group were improved from base-line to 4 wks (p < 0.01) and from 4–8 wks (p < 0.01) and had significantly less plaque than control group after 8 weeks (p < 0.01). TRSQ: Oral health knowledge improved in both groups from baseline to 4 wks (p < 0.01). From 4–8 wks, the improvement in the inter-vention group was significantly higher (p < 0.01). | + + |
| Kuo et al. [48] | N = 27 | N = 31 | Oral health programme: group education in 5 sessions: structure of oral cavity and teeth; importance of oral health; pathogenesis of caries and periodontal diseases; Bass toothbrushing method; and oral hygiene. Pictures of toothbrushing methods were posted on the mirror in each bathroom. Individual instructions in Bass toothbrushing method and one-on-one training in Bass toothbrushing technique were given. Participants were checked for correctness. Individual behavioural modification: participants received tokens for successful brushing. | Nursing care as usual | After 12 weeks, the mean dental plaque index significantly improved, compared to that of the control group (p < 0.001). Oral health knowledge, oral health attitude and oral health behaviour were statistically significant improved after 12 weeks, compared to those in the control group (p < 0.001). No significant differences between intervention and control group on consumption of sugary beverage and dentist-visiting behaviour after the intervention. | + + − |
| Barbadoro et al. [51] | N = 76 | No control group | After oral examination with DMFT: participants received a report with clinical findings. Lecture about alcohol, tobacco smoke in oral health pathology, oral cancer prevention strategies (de, secondary and tertiary). Brochure on oral health. | No comparator. | 10-item test assessing knowledge and consciousness: there was an improvement of 25% in exact answers between the pre-test/post-test (p < 0.001). Participants showed a significant improvement in toothbrushing after every meal (p < 0.001). Female, age >49 year, years of alcohol addiction had more risk of high DMFT (4.33/1.85/6.13). | + |
| Khokhar et al. [52] | N = 59 | No control group | Staff: education on importance of dental care and inclusion in care planning. Patients: provided with toothbrushes, toothpaste and mouthwash. Informa-tion and advice on basic dental hygiene by visual aids, posters and demonstration models. Registration status with dental practices. List of local dental practitioners was provided. | No comparator. | Access to toothbrushes increased from 68% to 86%. Knowledge of basic oral hygiene was improved from 55% to 61%. Brushing twice daily increased from 29% to 38%. There was a small increase from 34% to 39% of patients registered at dentist. There was no change in patients who had their dentures checked within the last 5 years. | + |
| De Mey et al. [28] | N = 27 (Pr) N = 24 (P) | No control group | Nurses: PowerPoint presentation about oral care, available tools, oral diseases (gingivitis, periodontal disease and caries), and oral health related to smoking, alcohol and drugs. Cleaning methods and tools were demonstrated by an O.H. Patients: an O.H. set up a treatment plan after oral examination. Toothbrush and fluoridated toothpaste. Concrete instructions on brushing and cleaning. Images were used of the toothbrush in different positions. Instruction card. | No comparator | Nurses: knowledge was significantly improved (p < 0.001). Patients: Dental plaque index was significantly improved on plaque index/6 (p ≤ 0.001), and plaque index/2 (p < 0.001). Concerning gingival bleeding index there was a significant change (p < 0.05). No significant changes were observed in bleeding index/2. | + |
| Mori et al. [50] | N = 10 | No control group | Six sextant evaluation for PMTC. Six teeth were stained with Red Coat and DI. PMTC procedure was strictly according Axelsson’s method. | No comparator. | Probing depth was significantly decreased at PMTC VI (p < 0.05). A reduction of the total number of bleeding sites on probing was significantly different (p < 0.05). | + |
| Silverstein et al. [53] | N = 67 | No control group | Educational programme (Smiles Matter). Weekly presentations: general oral health education, aesthetics, effects of eating disorders, oral pain, nutrition for oral health. | No comparator. | Patients who reported regular visits to the dentist were significantly more likely to respond that teeth had a positive effect on how they looked to themselves (p = 0.03), looking to others (p = 0.03), kissing (p = 0.04), their general health (p = 0.01), romantic relationships (p = 0.04) and general happiness (p < 0.001). | + + |
| Singhal et al. [49] | N = 41 | N = 47 | Group A: oral hygiene education and a battery-operated Arm and Hammer Truly Radiant Spin Brush. Group C: oral hygiene education as well as the Sun Star Gum ultrasoft manual toothbrush. C. Participants in group A and C received oral hygiene instructions and included video demonstrations. Observation were made while performing oral hygiene with their toothbrushes sitting in the dental chair. Dental plaque index and individual modifications were made. | Group B only received the same battery-operated toothbrush as group A. Group D received the same manual toothbrush as Group B. Next, participants received and were instructed to use Crest Cavity Protection toothpaste. A calendar and stickers were provided. | A statistically significant effect is found on the type of toothbrush participants used (p < 0.05). Interaction of home care instructions and type of toothbrush were not found. A significant effect is found on gingival index associated with the mechanical toothbrush (p < 0.05). No statistically significant changes were found in plaque index based on type of toothbrush. The mean change in plaque and gingival index were not significantly different based on the provision of oral home care instructions. | + − + − − |
| Evaluation and instruction per visit. Participants received and were instructed to use Crest Cavity Protection toothpaste. A calendar and stickers were provided. Participants were asked to perform oral care twice daily (morning and before bedtime) at home for four weeks and affix a sticker to the calendar for that particular day. | Participants were asked to perform oral care twice daily (morning and before bedtime) at home for four weeks and affix a sticker to the calendar for that particular day. | There was no correlation between negative symptoms and the post-test mean plaque index and the post-test gingival index. Frequency of brushing and the mean change of plaque index and gingival index were not correlated. There was no significant impact of smoking on the mean change in plaque index and gingival index. | − − − | |||
| Yoshii et al. [54] | N = 390 | No control group | Educational programme: (1) cause of tooth loss, (2) dental caries, (3) dental cleaning, (4) periodontal disease, (5) routine dental check-ups. This was in a 30 min-slideshow of 37 slides. Photos of patients’ mouths were used. | No comparator. | The educational programme showed a significant improvement in the use of fluoride toothpaste at 6 months after the intervention (p = 0.001). The daily use of interdental brushes or floss was significantly improved 6 months after the intervention (p = 0.025). There was no change in frequency of visits to the dentist. | + − |
| Randomised Controlled Trials 1 | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Randomi- sation for assignment to treatment group | Allocation conceal- ment | Similar treatment groups at baseline | Participants blind to treatment assignment | Delivering treatment blind to treatment assignment | Outcome assessors blind to treatment assignment | Treatment groups treated identically | Follow-up complete or differences adequately analysed | Analysed in groups to which they were randomised | Outcomes measured in same way | Outcome measure- ments reliable | Appro- priate statistical analyses used | Appro-priate design | |
| Adams et al. [45] |  | | |  |  | | | | | | | | |
| Almomani et al. [46] | | | | | | | | | | | | | |
| Almomani et al. [47] | | | | | | | | | | | | | |
| Kuo et al. [48] | | | | | | | | | | | | | |
| Quasi-experimental studies 2 | |||||||||||||
| Are the ‘cause’ and the ‘effects’ clear | Participants included in comparisons similar | Receiving simi- lar treatment, other than intervention | Was there a control group? | Multiple measurementsof the out- come pre- and post | Follow-up complete or differences described | Outcomes measured in same way | Outcome measure- ments reliable | Appropriate statistical analyses used | |||||
| Barbadoro et al. [51] | | | | | | | | | | ||||
| Khokhar et al. [52] | | | | | | | | | | ||||
| De Mey et al. [28] | | | | | | | | | | ||||
| Mori et al. [50] | | | | | | | | | | ||||
| Silverstein et al. [53] | | | | | | | | | | ||||
| Singhal et al. [49] | | | | | | | | | | ||||
| Cohort study 3 | |||||||||||||
| Groups simi- lar and recruited from the same population | Exposures measured similarly to assign people | Exposures measured valid and reliable | Confoun- ding factors identified | Strategies to deal with confounders stated | Groups free of the out- come at the start of the study | Outcomes measured in a valid and reliable way | Was follow-up time reported and sufficient | Follow-up complete, reasons to loss explored | Strategies to address incomplete, follow-up utilised | Appropriate statistical analyses used | |||
| Yoshii et al. [54] |  | | | | | | | | | | | ||
= yes, = no, = unclear, = not applicable.Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuipers, S.; Boonstra, N.; Kronenberg, L.; Keuning-Plantinga, A.; Castelein, S. Oral Health Interventions in Patients with a Mental Health Disorder: A Scoping Review with Critical Appraisal of the Literature. Int. J. Environ. Res. Public Health 2021, 18, 8113. https://doi.org/10.3390/ijerph18158113
Kuipers S, Boonstra N, Kronenberg L, Keuning-Plantinga A, Castelein S. Oral Health Interventions in Patients with a Mental Health Disorder: A Scoping Review with Critical Appraisal of the Literature. International Journal of Environmental Research and Public Health. 2021; 18(15):8113. https://doi.org/10.3390/ijerph18158113
Chicago/Turabian StyleKuipers, Sonja, Nynke Boonstra, Linda Kronenberg, Annette Keuning-Plantinga, and Stynke Castelein. 2021. "Oral Health Interventions in Patients with a Mental Health Disorder: A Scoping Review with Critical Appraisal of the Literature" International Journal of Environmental Research and Public Health 18, no. 15: 8113. https://doi.org/10.3390/ijerph18158113