
Health Inequalities in Children and Adolescents: A Scoping Review of the Mediating and Moderating Effects of Family Characteristics


 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
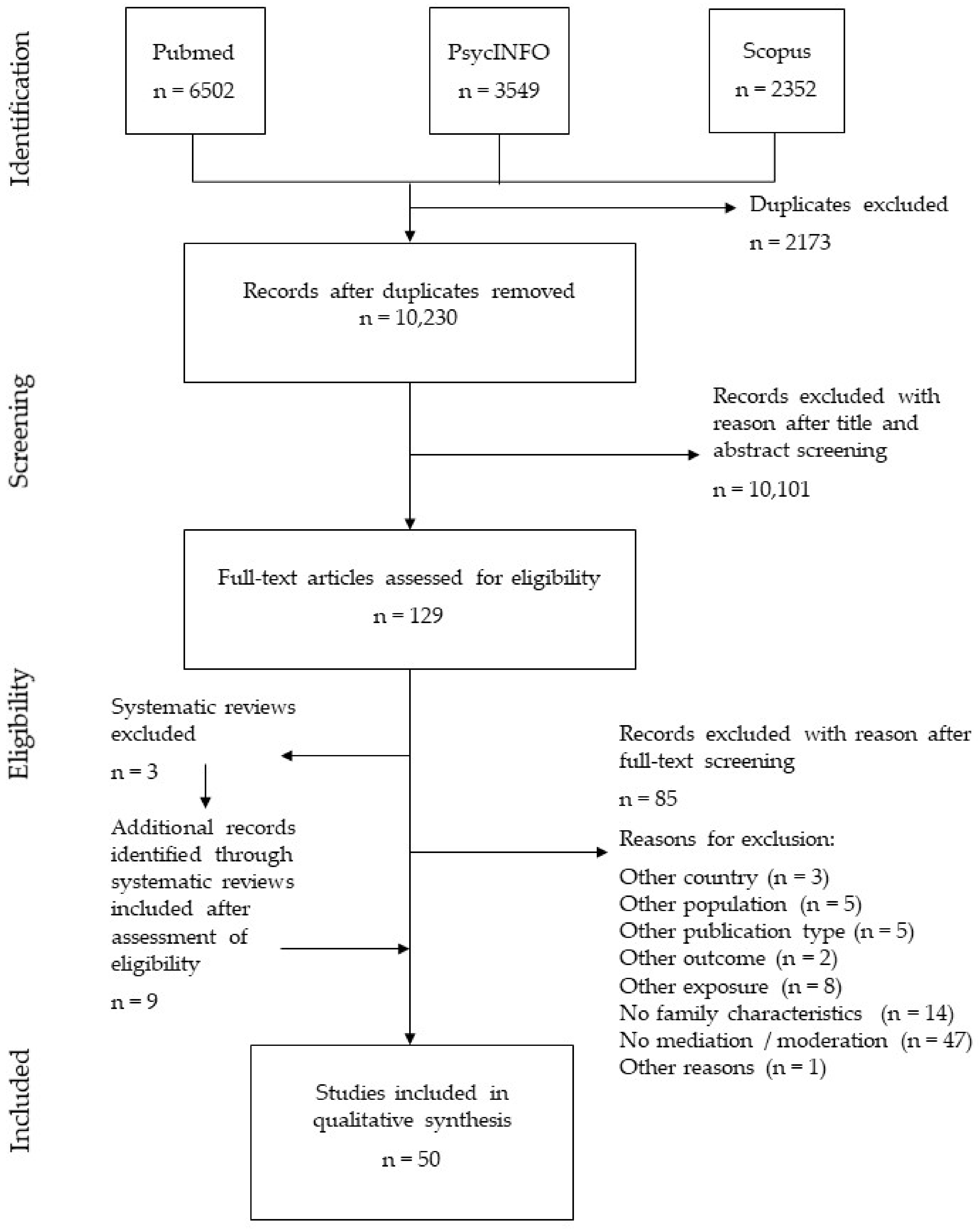
2.3. Selection of Sources of Evidence
2.4. Data Charting Process
2.5. Evidence Synthesis
3. Results
- parenting practices (parenting behavior, parenting style, feeding practices, effective parenting, parental involvement, parental support, family environment, parental monitoring, parental acceptance, parental control) [37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66],
- physical activity [53].
3.1. Mediation Effects
3.1.1. Parenting Practices
3.1.2. Parental Mental Health
3.1.3. Parent-Child Relationship
3.1.4. Family Structure
3.1.5. Parental Health and Health Behavior
3.1.6. Family Conflict and Distress
3.2. Moderation Effects
3.2.1. Parenting Practices
3.2.2. Parental Mental Health
3.2.3. Parent-Child Relationship
3.2.4. Family Structure
3.2.5. Family Conflict and Distress
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Final Search Strategy for PubMed
References
- CSDH. Closing the Gap in a Generation: Health Equity through Action on the Social Determinants of Health. Final Report of the Commission on Social Determinants of Health; Word Health Organization: Geneva, Switzerland, 2008. [Google Scholar]
- Pillas, D.; Marmot, M.; Naicker, K.; Goldblatt, P.; Morrison, J.; Pikhart, H. Social inequalities in early childhood health and development: A European-wide systematic review. Pediatr. Res. 2014, 76, 418–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazroo, J. Class and health inequality in later life: Patterns, mechanisms and implications for policy. Int. J. Environ. Res. Public Health 2017, 14, 1533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lampert, T.; Hoebel, J.; Kuntz, B.; Finger, J.D.; Hölling, H.; Lange, M.; Mauz, E.; Mensink, G.; Poethko-Müller, C.; Schienkiewitz, A.; et al. Health inequalities among children and adolescents in Germany. Developments over time and trends from the KiGGS study. J. Health Monit. 2019, 4, 15–37. [Google Scholar] [CrossRef]
- Elgar, F.J.; Pförtner, T.-K.; Moor, I.; De Clercq, B.; Stevens, G.W.J.M.; Currie, C. Socioeconomic inequalities in adolescent health 2002–2010: A time-series analysis of 34 countries participating in the health behaviour in school-aged children study. Lancet 2015, 385, 2088–2095. [Google Scholar] [CrossRef] [Green Version]
- Mackenbach, J.P.; Stirbu, I.; Roskam, A.-J.R.; Schaap, M.M.; Menvielle, G.; Leinsalu, M.; Kunst, A.E. socioeconomic inequalities in health in 22 European countries. N. Engl. J. Med. 2008, 358, 2468–2481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Currie, C.; Zanotti, C.; Morgan, A.; Currie, D.; de Looze, M.; Roberts, C.; Samdal, O.; Smith, O.R.F.; Barnekow, V. Social Determinants of Health and Well-Being among Young People. Health Behaviour in School-Aged Children (HBSC) Study: International Report from the 2009/2010 Survey; WHO Regional Office for Europe: Copenhagen, Denmark, 2012. [Google Scholar]
- Ben-Shlomo, Y.; Kuh, D. A life course approach to chronic disease epidemiology: Conceptual models, empirical challenges and interdisciplinary perspectives. Int. J. Epidemiol. 2002, 31, 285–293. [Google Scholar] [CrossRef]
- Case, A.; Fertig, A.; Paxson, C. The lasting impact of childhood health and circumstance. J. Health Econ. 2005, 24, 365–389. [Google Scholar] [CrossRef] [Green Version]
- Human Early Learning Partnership; Commission on Social Determinants of Health. Early Child Development: A Powerful Equalizer: Final Report for the World Health Organization’s Commission on the Social Determinants of Health; Siddiqi, A., Irwin, L.G., Hertzman, C., Eds.; Human Early Learning Partnership: Vancouver, BC, Canada, 2007. [Google Scholar]
- Barker, D.J. Fetal origins of coronary heart disease. BMJ Clin. Res. Ed. 1995, 311, 171–174. [Google Scholar] [CrossRef]
- Ben-Shlomo, Y.; Cooper, R.; Kuh, D. The last two decades of life course epidemiology, and its relevance for research on ageing. Int. J. Epidemiol. 2016, 45, 973–988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krieger, N. Epidemiology and the People’s Health: Theory and Context; Oxford University Press: New York, NY, USA, 2011. [Google Scholar]
- Krieger, N. Theories for social epidemiology in the 21st century: An ecosocial perspective. Int. J. Epidemiol. 2001, 30, 668–677. [Google Scholar] [CrossRef]
- Blum, R.W.; Bastos, F.I.P.M.; Kabiru, C.W.; Le, L.C. Adolescent health in the 21st century. Lancet 2012, 379, 1567–1568. [Google Scholar] [CrossRef]
- Viner, R.M.; Ozer, E.M.; Denny, S.; Marmot, M.; Resnick, M.; Fatusi, A.; Currie, C. Adolescence and the social determinants of health. Lancet 2012, 379, 1641–1652. [Google Scholar] [CrossRef]
- Richter, M.; Dragano, N. Micro, macro, but what about meso? The institutional context of health inequalities. Int. J. Public Health 2018, 63, 163–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bronfenbrenner, U. Ecology of the family as a context for human development: Research perspectives. Dev. Psychol. 1986, 22, 723–742. [Google Scholar] [CrossRef]
- Raphael, D. Determinants of health of North-American adolescents: Evolving definitions, recent findings, and proposed research agenda. J. Adolesc. Health 1996, 19, 6–16. [Google Scholar] [CrossRef]
- Kramer, M.R.; Schneider, E.B.; Kane, J.B.; Margerison-Zilko, C.; Jones-Smith, J.; King, K.; Davis-Kean, P.; Grzywacz, J.G. Getting under the skin: Children’s health disparities as embodiment of social class. Popul. Res. Policy Rev. 2017, 36, 671–697. [Google Scholar] [CrossRef] [Green Version]
- Mack, K.Y.; Peck, J.H.; Leiber, M.J. The effects of family structure and family processes on externalizing and internalizing behaviors of male and female youth: A longitudinal examination. Deviant Behav. 2015, 36, 740–764. [Google Scholar] [CrossRef]
- Case, A.; Paxson, C. Parental behavior and child health. Health Aff. 2002, 21, 164–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rattay, P.; von der Lippe, E.; Mauz, E.; Richter, F.; Hölling, H.; Lange, C.; Lampert, T. Health and health risk behaviour of adolescents—Differences according to family structure. Results of the German KiGGS cohort study. PLoS ONE 2018, 13, e0192968. [Google Scholar] [CrossRef]
- Conger, R.D.; Conger, K.J.; Martin, M.J. Socioeconomic status, family processes, and individual development. J. Marriage Fam. 2010, 72, 685–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation analysis. Annu. Rev. Psychol. 2007, 58, 593–614. [Google Scholar] [CrossRef]
- Hayes, A.F.; Rockwood, N.J. Regression-based statistical mediation and moderation analysis in clinical research: Observations, recommendations, and implementation. Behav. Res. Ther. 2017, 98, 39–57. [Google Scholar] [CrossRef] [PubMed]
- Conger, R.D.; Conger, K.J.; Elder, G.H., Jr.; Lorenz, F.O.; Simons, R.L.; Whitbeck, L.B. A family process model of economic hardship and adjustment of early adolescent boys. Child Dev. 1992, 63, 526–541. [Google Scholar] [CrossRef] [PubMed]
- Gard, A.M.; McLoyd, V.C.; Mitchell, C.; Hyde, L.W. Evaluation of a longitudinal family stress model in a population-based cohort. Soc. Dev. 2020, 29, 1155–1175. [Google Scholar] [CrossRef] [PubMed]
- United Nations. World Economic Situation and Prospects—Statistical Annex. Available online: https://www.un.org/development/desa/dpad/wp-content/uploads/sites/45/WESP2020_Annex.pdf (accessed on 16 April 2021).
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [Green Version]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. Theory Pract. 2005, 8, 19–32. [Google Scholar] [CrossRef] [Green Version]
- Wachtler, B.; Hoffmann, S.; Rattay, P.; Sander, L. Systematic Review of Qualitative and Quantitative Studies on the Mediating and Moderating Role of Family Characteristics on Health Inequalities in School-Aged Children and Adolescents in Countries with Developed Economies. Available online: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020165614 (accessed on 14 April 2021).
- Hoffmann, S.; Wachtler, B.; Sander, L.; Blume, M.; Hilger-Kolb, J.; Herke, M.; Matos Fialho, P.; Pischke, C.; Novelli, A.; Lampert, T.; et al. Health Inequalities among Infants and Pre-School Children: Protocol for a Scoping Review Examining the Moderating and Mediating Role of Contextual and Compositional Family Characteristics; Open Science Network: Vancouver, BC, Canada, 2020. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Popay, J.; Roberts, H.; Sowden, A.; Petticrew, M.; Arai, L.; Rodgers, M.; Britten, N.; Roen, K.; Duffy, S. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews: A Product from the ESRC Methods Programme; Lancaster University: Lancaster, UK, 2006. [Google Scholar]
- Grouven, U.; Bender, R.; Ziegler, A.; Lange, S. Der kappa-koeffizient. Dtsch. Med. Wochenschr. 2007, 132, e65–e68. [Google Scholar] [CrossRef] [Green Version]
- Ashiabi, G.S.; O’Neal, K.K. Children’s health status: Examining the associations among income poverty, material hardship, and parental factors. PLoS ONE 2007, 2, e940. [Google Scholar] [CrossRef] [PubMed]
- Bammann, K.; Gwozdz, W.; Pischke, C.; Eiben, G.; Fernandez-Alvira, J.M.; De Henauw, S.; Lissner, L.; Moreno, L.A.; Pitsiladis, Y.; Reisch, L.; et al. The impact of familial, behavioural and psychosocial factors on the SES gradient for childhood overweight in Europe. A longitudinal study. Int. J. Obes. 2017, 41, 54–60. [Google Scholar] [CrossRef] [Green Version]
- Barrera, M., Jr.; Prelow, H.M.; Dumka, L.E.; Gonzales, N.A.; Knight, G.P.; Michaels, M.L.; Roosa, M.W.; Tein, J.Y. Pathways from family economic conditions to adolescents’ distress: Supportive parenting, stressors outside the family and deviant peers. J. Community Psychol. 2002, 30, 135–152. [Google Scholar] [CrossRef]
- Beiser, M.; Hou, F.; Hyman, I.; Tousignant, M. Poverty, family process, and the mental health of immigrant children in Canada. Am. J. Public Health 2002, 92, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Boe, T.; Sivertsen, B.; Heiervang, E.; Goodman, R.; Lundervold, A.J.; Hysing, M. Socioeconomic status and child mental health: The role of parental emotional well-being and parenting practices. J. Abnorm. Child Psychol. 2014, 42, 705–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, M.; Miller, G.E.; Chen, E. Early life socioeconomic status and metabolic outcomes in adolescents: The role of implicit affect about one’s family. Health Psychol. 2016, 35, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Flouri, E.; Midouhas, E.; Ruddy, A.; Moulton, V. The role of socio-economic disadvantage in the development of comorbid emotional and conduct problems in children with ADHD. Eur. Child Adolesc. Psychiatry 2017, 26, 723–732. [Google Scholar] [CrossRef]
- Gonzales, N.A.; Coxe, S.; Roosa, M.W.; White, R.M.B.; Knight, G.P.; Zeiders, K.H.; Saenz, D. Economic hardship, neighborhood context, and parenting: Prospective effects on Mexican-American adolescent’s mental health. Am. J. Community Psychol. 2011, 47, 98–113. [Google Scholar] [CrossRef] [Green Version]
- Goosby, B.J. Poverty duration, maternal psychological resources, and adolescent socioemotional outcomes. J. Fam. Issues 2007, 28, 1113–1134. [Google Scholar] [CrossRef] [Green Version]
- Grant, K.; Poindexter, L.; Smith, K. Economic stress and psychological distress among urban African American adolescents: The mediating role of parents. J. Prev. Interv. Community 2000, 20, 25–36. [Google Scholar] [CrossRef]
- Grant, K.E.; McCormick, A.; Poindexter, L.; Simpkins, T.; Janda, C.M.; Thomas, K.J.; Campbell, A.; Carleton, R.; Taylor, J. Exposure to violence and parenting as mediators between poverty and psychological symptoms in urban African American adolescents. J. Adolesc. 2005, 28, 507–521. [Google Scholar] [CrossRef]
- Hardaway, C.R.; Cornelius, M.D. Economic hardship and adolescent problem drinking: Family processes as mediating influences. J. Youth Adolesc. 2014, 43, 1191–1202. [Google Scholar] [CrossRef]
- Kavanaugh, S.A.; Neppl, T.K.; Melby, J.N. Economic pressure and depressive symptoms: Testing the family stress model from adolescence to adulthood. J. Fam. Psychol. 2018, 32, 957–965. [Google Scholar] [CrossRef] [PubMed]
- Landers-Potts, M.A.; Wickrama, K.A.S.; Simons, L.G.; Cutrona, C.; Gibbons, F.X.; Simons, R.L.; Conger, R. An extension and moderational analysis of the family stress model focusing on African American adolescents. Fam. Relat. 2015, 64, 233–248. [Google Scholar] [CrossRef]
- Lane, S.P.; Bluestone, C.; Burke, C.T. Trajectories of BMI from early childhood through early adolescence: SES and psychosocial predictors. Br. J. Health Psychol. 2013, 18, 66–82. [Google Scholar] [CrossRef]
- Lee, C.-T.; McClernon, F.J.; Kollins, S.H.; Prybol, K.; Fuemmeler, B.F. Childhood economic strains in predicting substance use in emerging adulthood: Mediation effects of youth self-control and parenting practices. J. Pediatr. Psychol. 2013, 38, 1130–1143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, H. The role of parenting in linking family socioeconomic disadvantage to physical activity in adolescence and young adulthood. Youth Soc. 2014, 46, 255–285. [Google Scholar] [CrossRef]
- Lee, T.K.; Wickrama, K.A.S.; Simons, L.G. Chronic family economic hardship, family processes and progression of mental and physical health symptoms in adolescence. J. Youth Adolesc. 2013, 42, 821–836. [Google Scholar] [CrossRef] [PubMed]
- Li, S.T.; Nussbaum, K.M.; Richards, M.H. Risk and protective factors for urban African-American youth. Am. J. Community Psychol. 2007, 39, 21–35. [Google Scholar] [CrossRef]
- Parkes, A.; Sweeting, H.; Young, R.; Wight, D. Does parenting help to explain socioeconomic inequalities in children’s body mass index trajectories? Longitudinal analysis using the growing up in Scotland study. J. Epidemiol. Community Health 2016, 70, 868–873. [Google Scholar] [CrossRef] [Green Version]
- Ponnet, K. Financial stress, parent functioning and adolescent problem behavior: An actor-partner interdependence approach to family stress processes in low-, middle-, and high-income families. J. Youth Adolesc. 2014, 43, 1752–1769. [Google Scholar] [CrossRef] [PubMed]
- Salonna, F.; Geckova, A.M.; Zezula, I.; Sleskova, M.; Groothoff, J.W.; Reijneveld, S.A.; Dijk, J.P. Does social support mediate or moderate socioeconomic differences in self-rated health among adolescents? Int. J. Public Health 2012, 57, 609–617. [Google Scholar] [CrossRef] [Green Version]
- Solantaus, T.; Leinonen, J.; Punamaki, R.-L. Children’s mental health in times of economic recession: Replication and extension of the family economic stress model in Finland. Dev. Psychol. 2004, 40, 412–429. [Google Scholar] [CrossRef]
- Taylor, R.D.; Rodriguez, A.U.; Seaton, E.K.; Dominguez, A. Association of financial resources with parenting and adolescent adjustment in African American families. J. Adolesc. Res. 2004, 19, 267–283. [Google Scholar] [CrossRef]
- Tracy, M.; Zimmerman, F.J.; Galea, S.; McCauley, E.; Stoep, A.V. What explains the relation between family poverty and childhood depressive symptoms? J. Psychiatr. Res. 2008, 42, 1163–1175. [Google Scholar] [CrossRef]
- Walper, S. Links of perceived economic deprivation to adolescents’ well-being six years later. Z. Fam. 2009, 21, 107–127. [Google Scholar]
- Votruba-Drzal, E.; Miller, P.; Betancur, L.; Spielvogel, B.; Kruzik, C.; Coley, R.L. Family and community resource and stress processes related to income disparities in school-aged children’s development. J. Educ. Psychol. 2020. [Google Scholar] [CrossRef]
- Zhang, L.; Han, W.J. Childhood deprivation experience, family pathways, and socioemotional functioning. J. Fam. Psychol. 2021, 35, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Gätjens, I.; Hasler, M.; di Giuseppe, R.; Bosy-Westphal, A.; Plachta-Danielzik, S. Family and lifestyle factors mediate the relationship between socioeconomic status and fat mass in children and adolescents. Obes. Facts 2020, 13, 596–607. [Google Scholar] [CrossRef] [PubMed]
- Barnhart, S.; Kilty, K.M.; Loeffler, D. Family structure as a social determinant of child health. J. Poverty 2021, 25, 138–154. [Google Scholar] [CrossRef]
- Amone-P’Olak, K.; Burger, H.; Huisman, M.; Oldehinkel, A.J.; Ormel, J. Parental psychopathology and socioeconomic position predict adolescent offspring’s mental health independently and do not interact: The TRAILS study. J. Epidemiol. Community Health 2011, 65, 57–63. [Google Scholar] [CrossRef]
- Butler, A.C. Poverty and adolescent depressive symptoms. Am. J. Orthopsychiatry 2014, 84, 82–94. [Google Scholar] [CrossRef]
- Forkel, I.; Silbereisen, R.K. Family economic hardship and depressed mood among young adolescents from former East and West Germany. Am. Behav. Sci. 2001, 44, 1955–1971. [Google Scholar] [CrossRef]
- Frasquilho, D.; de Matos, M.G.; Marques, A.; Neville, F.G.; Gaspar, T.; Caldas-de-Almeida, J.M. Unemployment, parental distress and youth emotional well-being: The moderation roles of parent-youth relationship and financial deprivation. Child Psychiatry Hum. Dev. 2016, 47, 751–758. [Google Scholar] [CrossRef]
- Gutman, L.M.; McLoyd, V.C.; Tokoyawa, T. Financial strain, neighborhood stress, parenting behaviors, and adolescent adjustment in urban African American families. J. Res. Adolesc. 2005, 15, 425–449. [Google Scholar] [CrossRef]
- Henninger, W.R.I.V.; Luze, G. Poverty, caregiver depression and stress as predictors of children’s externalizing behaviours in a low-income sample. Child Fam. Soc. Work 2014, 19, 467–479. [Google Scholar] [CrossRef]
- Layte, R.; McCrory, C. Fiscal crises and personal troubles: The great recession in Ireland and family processes. Soc. Psychiatry Psychiatr. Epidemiol. 2018, 53, 987–1001. [Google Scholar] [CrossRef]
- Bacikova-Sleskova, M.; Benka, J.; Orosova, O. Parental employment status and adolescents’ health: The role of financial situation, parent-adolescent relationship and adolescents’ resilience. Psychol. Health 2015, 30, 400–422. [Google Scholar] [CrossRef]
- Georgiades, K.; Boyle, M.H.; Duku, E.; Racine, Y. Tobacco use among immigrant and nonimmigrant adolescents: Individual and family level influences. J. Adolesc. Health 2006, 38, e441–e447. [Google Scholar] [CrossRef] [PubMed]
- Moor, I.; Rathmann, K.; Lenzi, M.; Pfortner, T.-K.; Nagelhout, G.E.; de Looze, M.; Bendtsen, P.; Willemsen, M.; Kannas, L.; Kunst, A.E.; et al. Socioeconomic inequalities in adolescent smoking across 35 countries: A multilevel analysis of the role of family, school and peers. Eur. J. Public Health 2015, 25, 457–463. [Google Scholar] [CrossRef] [PubMed]
- Moor, I.; Rathmann, K.; Stronks, K.; Levin, K.; Spallek, J.; Richter, M. Psychosocial and behavioural factors in the explanation of socioeconomic inequalities in adolescent health: A multilevel analysis in 28 European and North American countries. J. Epidemiol. Community Health 2014, 68, 912–921. [Google Scholar] [CrossRef] [PubMed]
- Ringlever, L.; Otten, R.; de Leeuw, R.N.H.; Engels, R.C.M.E. Effects of parents’ education and occupation on adolescent smoking and the mediating role of smoking-specific parenting and parent smoking. Eur. Addict. Res. 2011, 17, 55–63. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.D.; Budescu, M.; Gebre, A.; Hodzic, I. Family financial pressure and maternal and adolescent socioemotional adjustment: Moderating effects of kin social support in low income African American families. J. Child Fam. Stud. 2014, 23, 242–254. [Google Scholar] [CrossRef]
- Tamura, K.; Morrison, J.; Pikhart, H. Children’s behavioural problems and its associations with socioeconomic position and early parenting environment: Findings from the UK Millennium Cohort Study. Epidemiol. Psychiatr. Sci. 2020, 29, e155. [Google Scholar] [CrossRef]
- Rydell, A.-M. Family factors and children’s disruptive behaviour: An investigation of links between demographic characteristics, negative life events and symptoms of ODD and ADHD. Soc. Psychiatry Psychiatr. Epidemiol. 2010, 45, 233–244. [Google Scholar] [CrossRef]
- Spencer, N. Maternal education, lone parenthood, material hardship, maternal smoking, and longstanding respiratory problems in childhood: Testing a hierarchical conceptual framework. J. Epidemiol. Community Health 2005, 59, 842–846. [Google Scholar] [CrossRef] [PubMed]
- Jo, Y. What money can buy: Family income and childhood obesity. Econ. Hum. Biol. 2014, 15, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Soteriades, E.S.; DiFranza, J.R. Parent’s socioeconomic status, adolescents’ disposable income, and adolescents’ smoking status in Massachusetts. Am. J. Public Health 2003, 93, 1155–1160. [Google Scholar] [CrossRef] [PubMed]
- Hammack, P.L.; Robinson, W.L.; Crawford, I.; Li, S.T. Poverty and depressed mood among urban African-American adolescents: A family stress perspective. J. Child Fam. Stud. 2004, 13, 309–323. [Google Scholar] [CrossRef]
- Wadsworth, M.E.; Compas, B.E. Coping with family conflict and economic strain: The adolescent perspective. J. Res. Adolesc. 2002, 12, 243–274. [Google Scholar] [CrossRef]
- Dashiff, C.; DiMicco, W.; Myers, B.; Sheppard, K. Poverty and adolescent mental health. J. Child Adolesc. Psychiatr. Nurs. 2009, 22, 23–32. [Google Scholar] [CrossRef]
- Masarik, A.S.; Conger, R.D. Stress and child development: A review of the Family Stress Model. Curr. Opin. Psychol. 2017, 13, 85–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barnett, M.A. Economic disadvantage in complex family systems: Expansion of family stress models. Clin. Child Fam. Psychol. Rev. 2008, 11, 145–161. [Google Scholar] [CrossRef] [PubMed]
- Patalay, P.; Gage, S.H. Changes in millennial adolescent mental health and health-related behaviours over 10 years: A population cohort comparison study. Int. J. Epidemiol. 2019, 48, 1650–1664. [Google Scholar] [CrossRef] [PubMed]
- Escobar, D.; Jesus, T.F.; Noll, P.; Noll, M. Family and school context: Effects on the mental health of Brazilian students. Int. J. Environ. Res. Public Health 2020, 17, 6042. [Google Scholar] [CrossRef]
- Morgan, K.; Melendez-Torres, G.J.; Bond, A.; Hawkins, J.; Hewitt, G.; Murphy, S.; Moore, G. Socio-economic inequalities in adolescent summer holiday experiences, and mental wellbeing on return to school: Analysis of the school health research network/health behaviour in school-aged children survey in Wales. Int. J. Environ. Res. Public Health 2019, 16, 1107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herke, M.; Moor, I.; Winter, K.; Hoffmann, S.; Spallek, J.; Hilger-Kolb, J.; Pischke, C.; Dragano, N.; Novelli, A.; Richter, M. Role of contextual and compositional characteristics of schools for health inequalities in childhood and adolescence: Protocol for a scoping review. BMJ Open 2020, 10, e038999. [Google Scholar] [CrossRef] [PubMed]
- Matos Fialho, P.M.; Dragano, N.; Reuter, M.; Metzendorf, M.-I.; Richter, B.; Hoffmann, S.; Diehl, K.; Wachtler, B.; Sundmacher, L.; Herke, M.; et al. Mapping the evidence regarding school-to-work/university transition and health inequalities among young adults: A scoping review protocol. BMJ Open 2020, 10, e039831. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Family Category | Author (Year) [Reference] | Country | Sample Age in Years [Mean, (Range)] | Sample Size | Study Design (L, C) | Measure of SEP | Family Characteristics | Child Health Outcome | Results |
|---|---|---|---|---|---|---|---|---|---|
| Parental mental health | Amone-P’Olak (2011) [67] | Netherlands | (11.1–13.6) | 2149 | L | Family SEP index | Parental lifetime psychopathology | Internalizing and externalizing behavior | No moderation |
| Ashiabi (2007) [37] | USA | (6–11) | 9645 | C | Income poverty, material hardship | Parental depression | Subjective health | Mediation | |
| Barrera (2002) [39] | USA | 12.9 (11–15) | 300 | C | Objective economic status, perceived economic hardship | Parents depressive symptoms | Internalizing and externalizing symptoms | Mediation | |
| Beiser (2002) [40] | Canada | (4–11) | 13,349 | C | Poverty | Parental depression | Externalizing and internalizing problems | Mediation (non-immigrant group)/ no mediation (immigrant group) | |
| Boe (2014) [41] | Norway | 11.8 (11–13) | 2043 | C | Family economy | Emotional well-being of the children’s caretakers | Internalizing and externalizing problems | Mediation | |
| Paternal education | Emotional well-being of the children’s caretakers | Internalizing and externalizing problems | No mediation | ||||||
| Maternal education | Emotional well-being of the children’s caretakers | Internalizing and externalizing problems | No mediation | ||||||
| Butler (2014) [68] | USA | (12–17; 12–16) | 1056 | L | Poverty | Mother’s own childhood depression | Depressive symptoms | Mediation | |
| Parental mental health | Forkel (2001) [69] | Germany | 11.49 (10–13) | 304 | C | Income, unstable work, income change, can’t make ends meet, material needs, economic adjustments, economic pressure | Parents depressed mood | Depressed mood | Mediation (West Germany)/ no mediation (East Germany) |
| Goosby (2007) [45] | USA | 12.19 (10–14) | 854 | C | Poverty | Mothers’ psychological resources | Internalized and externalized behavior | Mediation | |
| Grant (2000) [46] | USA | 12.5 (11–15) | 50 | C | Economic stress | Maternal depression | Psychological symptoms | Mediation | |
| Gutman (2005) [71] | USA | 13.5 (11–16) | 305 | C | Income-to-need-ratio, financial strain | Parent psychological distress | Adolescent adjustment | Mediation | |
| Hardaway (2014) [48] | USA | (10.3; 14.4; 16.5) | 300 | L | Economic hardship | Maternal psychological distress | Externalizing behavior | Mediation | |
| Maternal psychological distress | Problem drinking | Mediation | |||||||
| Henninger (2014) [72] | USA | (10–11) | 1067 | L | Poverty | Caregiver depression | Externalizing behavior | Mediation | |
| Parental stress | Externalizing behavior | Mediation | |||||||
| Kavanaugh (2018) [49] | USA | (13–14; 15–18; 27–30) | 451 | L | Economic pressure | Maternal depressive symptoms | Depressive symptoms | Mediation | |
| Landers-Potts (2015) [50] | USA | T1: 10.5 (10–12); T2: 12.5 (12–14) | 422 | L | Family income, negative financial events index, economic pressure | Parental depressive symptoms | Internalizing symptoms | Mediation | |
| Parental mental health | Lane (2013) [51] | USA | (0–11) | 1238 | L | Income | Maternal depression | BMI | Mediation |
| Layte (2018) [73] | Ireland | (9–13) | 6272 | C | Objective and subjective economic recession | Maternal and paternal depression | Child psychological adjustment | Mediation | |
| Ponnet (2014) [57] | Belgium | 14.27 (11–17) | 798 | C | Education, financial stress | Depressive symptoms | Externalizing behaviors | Mediation | |
| Solantaus (2004) [59] | Finland | 12.6 | 527 | C | Economic hardship, economic pressure, making ends meet, family expenditures | Maternal and paternal mental health | Mental health | Mediation | |
| Taylor (2004) [60] | USA | 14.74 (12–18) | 200 | C | Financial resources and employment | Optimism | Depressive symptoms | No mediation | |
| Depressive symptomatology | Depressive symptoms | No mediation | |||||||
| Zhang (2021) [64] | USA | Kindergarten, Grade 1, 3, 5, 8 | 9250 | L | Poverty, income volatility | Parenting depressive symptoms | External locus of control, negative self-concept, internalizing behavior | Mediation | |
| Parental health and health behavior | Bammann (2017) [38] | Belgium, Germany, Sweden, Estonia, Spain | 7.82 (2–11) | 5819 | C | Socioeconomic status | Parental BMI | BMI | Mediation |
| Parental health and health behavior | Gätjens (2020) [65] | Germany | 6.2, 9.9, 14.5 | 4772 | C | Parental education | Maternal and paternal BMI | Weight status and body composition | Mediation |
| Smoking habits | Weight status and body composition | Mediation (age 9–16), no mediation (age 5–7) | |||||||
| Georgiades (2006) [75] | Canada | (12–18) | 5401 | C | Socioeconomic status | Parental tobacco use | Tobacco use | Mediation | |
| Jo (2014) [83] | USA | 14.22 | 6913 | L | Income | Rules about TV watching, frequency of doctor/dentist visits, and family meal routines | Obesity | Mediation | |
| Parkes (2016) [56] | Scotland | (3.8–7.5) | 2957 | L | Maternal education level | Unhealthy eating | BMI | Mediation | |
| Ringlever (2011) [78] | The Netherlands | 15.22 | 358 | L | Parents educational attainment and current occupational status | Smoking status | Adolescents’ smoking behavior | No mediation | |
| Parents smoking | Adolescents’ smoking behavior | No mediation | |||||||
| Soteriades (2003) [84] | USA | (12–17) | 1308 | C | Parental educational attainment and household income | Smoking of parents | Smoking | Mediation | |
| Spencer (2005) [82] | UK | (0–11) | 7926 | C | Maternal education, material hardship, family scores on hardship | Maternal smoking | Respiratory illness | No mediation | |
| Parenting practices | Ashiabi (2007) [37] | USA | (6–11) | 9645 | C | Income poverty, material hardship | Positive parenting behavior | Subjective health | Mediation |
| Bammann (2017) [38] | Belgium, Germany, Sweden, Estonia, Spain | 7.82 (2–11) | 5819 | C | Socioeconomic status | Parental feeding practices | BMI | Mediation | |
| Barnhart (2020) [66] | USA | Married mothers: 15.53; unmarried mothers: 15.58 | 3146 | L | Maternal economic hardship | Parenting Stress | Self-rated health | No Mediation | |
| Barrera (2002) [39] | USA | 12.9 (11–15) | 300 | C | Objective economic status, perceived economic hardship | Parental support | Internalizing and externalizing symptoms | Mediation | |
| Beiser (2002) [40] | Canada | (4–11) | 13,349 | C | Poverty | Ineffective parenting | Externalizing and internalizing problems | Mediation (non-immigrant group)/ no mediation (immigrant group) | |
| Boe (2014) [41] | Norway | 2043 | C | Maternal education | Negative discipline | Internalizing and externalizing problems | Mediation | ||
| Paternal education | Negative discipline | Internalizing and externalizing problems | No mediation | ||||||
| Family economy | Negative discipline | Internalizing and externalizing problems | Mediation | ||||||
| Parenting practices | Chan (2016) [42] | Canada | 14.53 (13–16) | 259 | C | Household crowding | Quality of childhood family environment | Metabolic outcomes | Moderation |
| Flouri (2017) [43] | UK | (3–11) | 180 | L | Family socio-economic disadvantage index | Harsh parental discipline, quality of emotional support | Emotional and conduct problems | No mediation | |
| Gätjens (2020) [65] | Germany | 6.2, 9.9, 14.5 | 4772 | C | Parental education | Shared meals | Weight status and body composition | Mediation (age 13–16), no mediation (age 5–11) | |
| Media consumption | Weight status and body composition | Mediation (age 5–11), no mediation (age 13–16) | |||||||
| Physical activity in a sport club of children | Weight status and body composition | Mediation (age 9–16), no mediation (age 5–7) | |||||||
| Gonzales (2011) [44] | USA | 10.43 (9–12) | 750 | L | Perceived Economic Hardship | Warm and harsh parenting | Internalizing symptoms | No Mediation | |
| Externalizing symptoms | Mediation | ||||||||
| Goosby (2007) [45] | USA | 12.19 (10–14) | 854 | C | Poverty | Mastery | Internalized and externalized behavior | Mediation | |
| Parental support | Internalized and externalized behavior | Mediation | |||||||
| Grant (2000) [46] | USA | 12.5 (11–15) | 50 | C | Economic Stress | Parenting | Psychological symptoms | Mediation | |
| Grant (2005) [47] | USA | 12.89 (11–15) | 105 | C | Poverty, economic stressors | Neglectful/ distant parenting and inconsistent discipline | Psychological symptoms | No mediation | |
| Hardaway (2014) [48] | USA | 10.3 / 14.4 / 16.5 | 300 | L | Economic hardship | Supportive parenting | Externalizing behavior & problem drinking | Mediation | |
| Parenting practices | Kavanaugh (2018) [49] | USA | (13–14; 15–18; 27–30) | 451 | L | Economic pressure | Mother harsh parenting | Depressive symptoms | Mediation |
| Landers-Potts (2015) [50] | USA | T1: 10.5 (10–12); T2: 12.5 (12–14) | 422 | L | Family income, negative financial events index, economic pressure | Nurturant-involved parenting | Internalizing symptoms | Mediation | |
| Lane (2013) [51] | USA | (0–11) | 1238 | L | Income | Parenting behavior | BMI | Mediation | |
| Income | Parenting style | BMI | Mediation | ||||||
| Lee (2013) [52] | USA | (7–17) | 1285 | L | Economic strains | Parenting | Regular smoking | No mediation | |
| Parenting | Heavy episodic drinking | No mediation | |||||||
| Parenting | Marijuana use | No mediation | |||||||
| Lee (2013) [54] | USA | 12.7 | 451 | L | Chronic family economic hardship | Parenting support | Anxiety symptoms | Mediation, no moderation | |
| Chronic family economic hardship | Parenting support | Physical complaints | No mediation, no moderation | ||||||
| Chronic family economic hardship | Parenting support | Depressive symptoms | Mediation | ||||||
| Lee (2014) [53] | USA | Female 14.89; male 15.10 (11–20) | 9799 | L | Family socioeconomic disadvantage | Parental control | Physical activity | Mediation | |
| Parenting practices | Li (2007) [55] | USA | 11.95 (10–15) | 263 | C | Family income, poverty level | Family support | Externalizing and Internalizing Symptoms | Moderation |
| Family income, poverty level | Helpfulness of family | Externalizing and Internalizing Symptoms | Moderation | ||||||
| Parkes (2016) [56] | Scotland | (3.8–7.5) | 2957 | L | Maternal education level | Positive mealtime interaction | BMI | Mediation | |
| Informal mealtime setting | BMI | Mediation | |||||||
| Bedroom TV | BMI | Mediation | |||||||
| Ponnet (2014) [57] | Belgium | 14.27 (11–17) | 798 | C | Education, financial stress | Positive parenting | Externalizing behaviors | Mediation | |
| Salonna (2012) [58] | Slovakia | 16.85 | 1865 | C | Family affluence | Social support of father | Self-rated health of girls and boys | Mediation/ no moderation | |
| Perceived financial strain | Social support of father | Self-rated health of boys | Mediation/ no moderation | ||||||
| Solantaus (2004) [59] | Finland | 12.6 | 527 | C | Economic hardship, economic pressure, making ends meet, family expenditures | Parenting quality | Mental health | Mediation | |
| Taylor (2004) [60] | USA | 14.74 (12–18) | 200 | C | Financial resources and employment | Family organization | Depressive symptoms | No mediation | |
| Tracy (2008) [61] | USA | (11–13) | 457 | L | Income | Parental support | Depressive symptoms | Mediation | |
| Votruba-Drzal (2020) [63] | USA | 9.09 | 17,600 | L | Income | Corporal punishment | Externalizing behavior problems | Mediation | |
| Parenting practices | Walper (2009) [62] | Germany | 14.2 (9–19) | 358 | C | Parental education, financial hardship, economic deprivation | Maternal negative communication | Somatic complaints, self esteem | Mediation (girls) / no mediation (boys) |
| Depressive symptoms | No mediation | ||||||||
| Zhang (2021) [64] | USA | Kindergarten, Grade 1, 3, 5, 8 | 9250 | L | Poverty and income volatility | Parenting style | External locus of control, negative self-concept, internalizing behavior | No mediation | |
| Cognitively stimulating materials | External locus of control, negative self-concept, internalizing behavior | Mediation | |||||||
| Parent school involvement | External locus of control, negative self-concept | Mediation | |||||||
| Internalizing behavior | No mediation | ||||||||
| Family structure | Barnhart (2020) [66] | USA | Married mother: 15.53; unmarried mothers 15.58 | 3146 | L | Maternal economic hardship | Married/ unmarried mothers | Self-rated health | Moderation |
| Barrera (2002) [39] | USA | 12.9 (11–15) | 300 | C | Objective economic status, perceived economic hardship | One or two-parent families | Internalizing and externalizing symptoms | Mediation, moderation | |
| Beiser (2002) [40] | Canada | (4–11) | 13,349 | C | Poverty | Single-parent status | Externalizing and internalizing problems | Mediation (non-immigrant group)/ no mediation (immigrant group) | |
| Family structure | Butler (2014) [68] | USA | (12–17; 12–16) | 1056 | L | Poverty | Single- and two-parent families | Depressive symptoms | No moderation |
| Moor (2015) [76] | 35 European and North American countries | 15 | 52,907 | C | Family affluence scale | Family structure | Smoking | Mediation | |
| Rydell (2010) [81] | Sweden | 10 | 1206 | C | Education | Family structure | ADHD symptoms and ODD symptoms | Moderation | |
| Spencer (2005) [82] | UK | (0–11) | 7926 | C | Maternal education, material hardship, family scores on hardship | Lone parenthood | Respiratory illness | Mediation | |
| Tracy (2008) [61] | USA | (11–13) | 457 | L | Income | Marital status | Depressive symptoms | Mediation | |
| Income | number of adults living in the household | Depressive symptoms | Mediation | ||||||
| Walper (2009) [62] | Germany | 14.2 (9–19) | 358 | C | Parental education, financial hardship, economic deprivation | Family structure | Adolescent well-being | Mediation | |
| Parent-Child-Relationship | Bacikova-Sleskova (2015) [74] | Slovakia | 14.3 (11–17) | 2799 | C | Parental employment status, financial strain | Closeness | Subjective health status | No mediation |
| Conflict | Subjective health status | No mediation | |||||||
| Support | Subjective health status | No mediation | |||||||
| Communication | Subjective health status | No mediation | |||||||
| Perception of parents | Subjective health status | No mediation | |||||||
| Monitoring | Subjective health status | No mediation | |||||||
| Beiser (2002) [40] | Canada | (4–11) | 13,349 | C | Poverty | Family dysfunction | Externalizing and internalizing problems | Mediation (non-immigrant group)/ no mediation (immigrant group) | |
| Chan (2016) [42] | Canada | 14.53 (13–16) | 259 | C | Household crowding | Quality of childhood family environment | Metabolic outcomes | No moderation | |
| Flouri (2017) [43] | UK | (3–11) | 180 | L | Family socio-economic disadvantage index | quality of the parent–child relationship | Emotional and conduct problems | No mediation | |
| Forkel (2001) [69] | Germany | 11.49 (10–13) | 304 | C | Income, unstable work, income change, can’t make ends meet, material needs, economic adjustments, economic pressure | Positive family climate | Depressed mood | Mediation (West Germany), no mediation (East Germany) | |
| Parent-Child-Relationship | Tamura (2020) [80] | UK | (9 months to 14 years) | 14,452 | L | SEP (household income, maternal education and maternal occupation) | Child-parent relationship | Externalizing symptoms | Mediation, no moderation |
| Child-parent relationship | Internalizing symptoms | Mediation, moderation | |||||||
| Frasquilho (2016) [70] | Portugal | 15 | 112 | C | Employment Status | Parent-youth-relationship | Emotional problems | Moderation | |
| Georgiades (2006) [75] | Canada | (12–18) | 5401 | C | Socioeconomic status | Family functioning | Tobacco use | Mediation | |
| Gutman (2005) [71] | USA | 13.5 (11–16) | 305 | C | Income-to-need-ratio, financial strain | Parent-adolescent relations | Adolescent adjustment | Mediation | |
| Layte (2018) [73] | Ireland | (9–13) | 6272 | C | Objective and subjective economic recession | Parent-child relationship | Child psychological adjustment | Mediation | |
| Lee (2014) [53] | USA | Female 14.89; male 15.10 (overall 11–20) | 9799 | L | Family socioeconomic disadvantage | Parental control | Physical activity | Mediation | |
| Moor (2015) [76] | 35 European and North American countries | 15 | 52,907 | C | Family affluence scale | Relationship with parents | Smoking | Mediation | |
| Parent-Child-Relationship | Moor (2014) [77] | 28 European and North American high income countries | (11–15) | 29,920 | C | Family affluence scale | Relationship to mother and father | Self-rated health | Mediation |
| Ringlever (2011) [78] | The Netherlands | 15.22 | 358 | L | Parents educational attainment and current occupational status | Frequency of communication, quality of communication | Adolescents’ smoking behavior | No mediation | |
| Solantaus (2004) [59] | Finland | 12.6 | 527 | C | Economic hardship, economic pressure, making ends meet, family expenditures | Marital interaction | Mental health | Mediation | |
| Taylor (2004) [60] | USA | 14.74 (12–18) | 200 | C | Financial resources and employment | Parent-adolescent communication | Depressive symptoms | No mediation | |
| Taylor (2014) [79] | USA | 14.54 (14–18) | 200 | C | Financial pressure | Kin social support | Adolescent depressive symptomatology | No moderation | |
| Kin social support | Adolescent problem behavior | Moderation | |||||||
| Votruba-Drzal (2020) [63] | USA | 9.09 | 17,600 | L | Income | Emotional support | Externalizing symptoms | Mediation | |
| Family Conflict and Distress | Hammack (2014) [85] | USA | median 15 (13–18) | 1704 | C | Poverty | Family stress | Depressed mood | Mediation |
| Kavanaugh (2018) [49] | USA | (13–14; 15–18; 27–30) | 451 | L | Economic pressure | Couple conflict | Depressive symptoms | No mediation | |
| Landers-Potts (2015) [50] | USA | T1: 10.5 (10–12); T2: 12.5 (12–14) | 422 | L | Family income, negative financial events index, economic pressure | Caregiver relationship conflict and withdrawal | Internalizing symptoms | Mediation, moderation | |
| Lee (2013) [54] | USA | 12.7 | 451 | L | Chronic family economic hardship | Marital conflict | Anxiety symptoms | No mediation | |
| Marital conflict | Depressive symptoms | No mediation | |||||||
| Marital conflict | Physical complaints | No mediation | |||||||
| Ponnet (2014) [57] | Belgium | 14.27 (11–17) | 798 | C | Education, financial stress | Interparental conflict | Externalizing behaviors | Mediation | |
| Tamura (2020) [80] | UK | (9 months to 14 years) | 14,452 | L | SEP (household income, maternal education and maternal occupation) | Parent distress | Externalizing symptoms | Mediation, no moderation | |
| Parent distress | Internalizing symptoms | Mediation, no moderation | |||||||
| Wadsworth (2002) [86] | USA | 14.7 | 364 | C | Parental education, parental occupation, economic strain | Family conflicts | Coping with stress | Mediation | |
| Family conflicts | Emotional and behavioral problems | Mediation |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blume, M.; Rattay, P.; Hoffmann, S.; Spallek, J.; Sander, L.; Herr, R.; Richter, M.; Moor, I.; Dragano, N.; Pischke, C.; et al. Health Inequalities in Children and Adolescents: A Scoping Review of the Mediating and Moderating Effects of Family Characteristics. Int. J. Environ. Res. Public Health 2021, 18, 7739. https://doi.org/10.3390/ijerph18157739
Blume M, Rattay P, Hoffmann S, Spallek J, Sander L, Herr R, Richter M, Moor I, Dragano N, Pischke C, et al. Health Inequalities in Children and Adolescents: A Scoping Review of the Mediating and Moderating Effects of Family Characteristics. International Journal of Environmental Research and Public Health. 2021; 18(15):7739. https://doi.org/10.3390/ijerph18157739
Chicago/Turabian StyleBlume, Miriam, Petra Rattay, Stephanie Hoffmann, Jacob Spallek, Lydia Sander, Raphael Herr, Matthias Richter, Irene Moor, Nico Dragano, Claudia Pischke, and et al. 2021. "Health Inequalities in Children and Adolescents: A Scoping Review of the Mediating and Moderating Effects of Family Characteristics" International Journal of Environmental Research and Public Health 18, no. 15: 7739. https://doi.org/10.3390/ijerph18157739