
Short-Term Effects of a Respiratory Telerehabilitation Program in Confined COVID-19 Patients in the Acute Phase: A Pilot Study

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
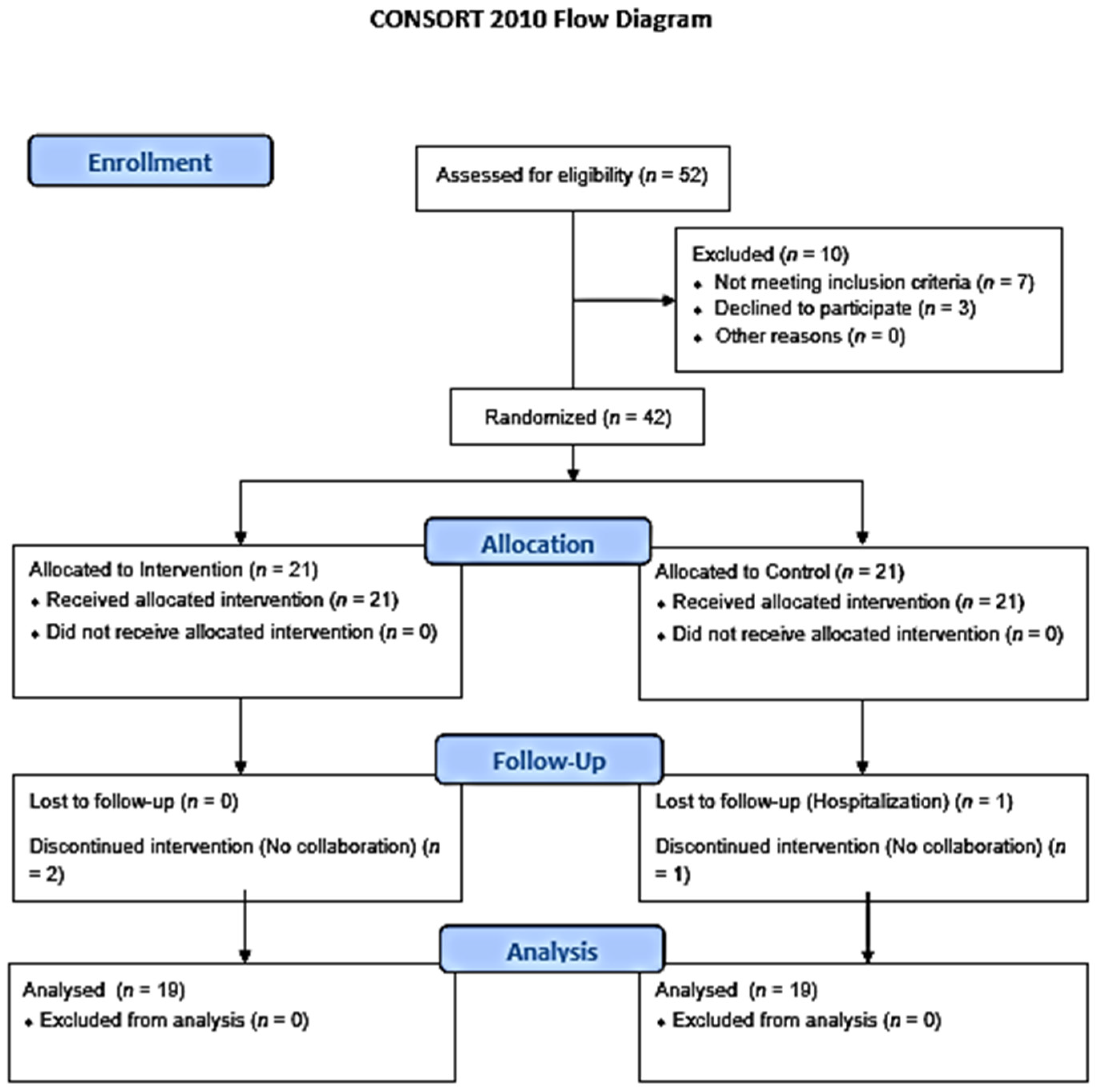
2.1. Trial Design
2.2. Sample Selection
2.3. Inclusion Criteria
- Aged 18–75 years.
- Patients with positive polymerase chain reaction (PCR) test and/or antigen test results in the last forty days were in home confinement. We amplified the period to 40 days due to delays both in the performance and in the reception of the test results caused by the collapse in the Spanish Health System.
2.4. Exclusion Criteria
2.5. Interventions
2.5.1. Group 1: Breathing Exercise Group
2.5.2. Group 2: Control Group
2.5.3. Procedure for Adverse Effects
2.5.4. Outcome Measures
- Multidimensional Dyspnoea-12 (MD12). We used the already validated Spanish version of this test, a valid and reliable instrument to study the multidimensional nature of dyspnoea [22].
- Borg Scale (BS). The modified version of the Borg Scale of perceived effort (0–10) [25,26] measures the entire range of activities that the individual perceives when exercising. This scale gives criteria to make adjustments to the intensity of exercise, that is, to the workload, thus forecasting and dictating the different exercise powers in sports and medical rehabilitation. Patients completed the BS at the end of the 30STST [27].
2.5.5. Randomization
2.5.6. Blinding
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McCloskey, B.; Zumla, A.; Ippolito, G.; Blumberg, L.; Arbon, P.; Cicero, A.; Endericks, T.; Lim, P.L.; Borodina, M. Mass gathering events and reducing further global spread of COVID-19: A political and public health dilemma. Lancet 2020, 395, 1096–1099. [Google Scholar] [CrossRef]
- Turolla, A.; Rossettini, G.; Viceconti, A.; Palese, A.; Geri, T. Musculoskeletal Physical Therapy During the COVID-19 Pandemic: Is Telerehabilitation the Answer? Phys. Ther. 2020, 100, 1260–1264. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020. [Google Scholar] [CrossRef] [Green Version]
- Sepúlveda-Loyola, W.; Rodríguez-Sánchez, I.; Pérez-Rodríguez, P.; Ganz, F.; Torralba, R.; Oliveira, D.V.; Rodríguez-Mañas, L. Impact of Social Isolation Due to COVID-19 on Health in Older People: Mental and Physical Effects and Recommendations. J. Nutr. Health Aging 2020, 24, 938–947. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Kream, R.M.; Stefano, G.B. Long-Term Respiratory and Neurological Sequelae of COVID-19. Med. Sci. Monit. 2020, 26, e928996. [Google Scholar] [CrossRef] [PubMed]
- Calabrese, F.; Pezzuto, F.; Fortarezza, F.; Hofman, P.; Kern, I.; Panizo, A.; von der Thüsen, J.; Timofeev, S.; Gorkiewicz, G.; Lunardi, F. Pulmonary pathology and COVID-19: Lessons from autopsy. The experience of European Pulmonary Pathologists. Virchows Arch. 2020, 477, 359–372. [Google Scholar] [CrossRef] [PubMed]
- Zampogna, E.; Paneroni, M.; Cherubino, F.; Pignatti, P.; Rudi, M.; Casu, G.; Vitacca, M.; Spanevello, A.; Visca, D. Effectiveness of a Pulmonary Rehabilitation Program on Persistent Asthma Stratified for Severity. Respir. Care 2019, 64, 1523–1530. [Google Scholar] [CrossRef] [PubMed]
- Cameron-Tucker, H.L.; Wood-Baker, R.; Owen, C.; Joseph, L.; Walters, E.H. Chronic disease self-management and exercise in COPD as pulmonary rehabilitation: A randomized controlled trial. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 513–523. [Google Scholar] [CrossRef] [Green Version]
- Kerti, M.; Balogh, Z.; Kelemen, K.; Varga, J.T. The relationship between exercise capacity and different functional markers in pulmonary rehabilitation for COPD. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 717–724. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lechowicz, K.; Drożdżal, S.; Machaj, F.; Rosik, J.; Szostak, B.; Zegan-Barańska, M.; Biernawska, J.; Dabrowski, W.; Rotter, I.; Kotfis, K. COVID-19: The Potential Treatment of Pulmonary Fibrosis Associated with SARS-CoV-2 Infection. J. Clin. Med. 2020, 9, 1917. [Google Scholar] [CrossRef]
- Zha, L.; Xu, X.; Wang, D.; Qiao, G.; Zhuang, W.; Huang, S. Modified rehabilitation exercises for mild cases of COVID-19. Ann. Palliat. Med. 2020, 9, 3100–3106. [Google Scholar] [CrossRef]
- Cheng, Y.Y.; Chen, C.M.; Huang, W.C.; Chiang, S.L.; Hsieh, P.C.; Lin, K.L.; Chen, Y.J.; Fu, T.C.; Huang, S.C.; Chen, S.Y.; et al. Rehabilitation programs for patients with COronaVIrus Disease 2019: Consensus statements of Taiwan Academy of Cardiovascular and Pulmonary Rehabilitation. J. Formos Med. Assoc. 2021, 120, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Liu, K.; Zhang, W.; Yang, Y.; Zhang, J.; Li, Y.; Chen, Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complement Ther. Clin. Pract. 2020, 39, 101166. [Google Scholar] [CrossRef]
- Gautam, A.P.; Arena, R.; Dixit, S.; Borghi-Silva, A. Pulmonary rehabilitation in COVID-19 pandemic era: The need for a revised approach. Respirology 2020, 25, 1320–1322. [Google Scholar] [CrossRef]
- Salawu, A.; Green, A.; Crooks, M.G.; Brixey, N.; Ross, D.H.; Sivan, M. A Proposal for Multidisciplinary Tele-Rehabilitation in the Assessment and Rehabilitation of COVID-19 Survivors. Int. J. Environ. Res. Public Health 2020, 17, 4890. [Google Scholar] [CrossRef] [PubMed]
- Wootton, S.L.; King, M.; Alison, J.A.; Mahadev, S.; Chan, A.S.L. COVID-19 rehabilitation delivered via a telehealth pulmonary rehabilitation model: A case series. Respirol. Case Rep. 2020, 8, e00669. [Google Scholar] [CrossRef]
- Criterios de Atención Clínica y de Derivación Hospitalaria de Pacientes Diagnosticados Como Casos Probables de Infección por SARS-CoV-2(SEMFYC) [Internet] 2020. Available online: https://www.semfyc.es/wp-content/uploads/2020/03/Criterios-SARS-COV-2-20200320.pdf (accessed on 8 September 2020).
- Thomas, M.; McKinley, R.K.; Mellor, S.; Watkin, G.; Holloway, E.; Scullion, J.; Shaw, D.E.; Wardlaw, A.; Price, D.; Pavord, I. Breathing exercises for asthma: A randosmied contrlled trial. Thorax 2009, 64, 55–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaskell, D.V.; Webber, B.A. The Brompton Hospital Guide to Chest Physiotherapy, 4th ed.; Blackwell: Oxford, UK, 1980; pp. 14–17. [Google Scholar]
- Ozalevli, S.; Ozden, A.; Itil, O.; Akkoclu, A. Comparison of the sit-to-stand test with 6 min walk test in patients with chronic obstructive pulmonary disease. Respir. Med. 2007, 101, 286–293. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvi, D.; Poffley, E.; Orchard, E.; Tarassenko, L. The Mobile-Based 6-Minute Walk Test: Usability Study and Algorithm Development and Validation. JMIR Mhealth Uhealth 2020, 8, e13756. [Google Scholar] [CrossRef] [Green Version]
- Diago, C.A.; Maestu, L.P.; Bolado, B.A.; Calvo, J.A.; Hernando, M.H.; Bats, I.P.; Balbín, R.A. Translation and validation of the multidimensional dyspnea-12 questionnaire. Traducción y validación del cuestionario multidimensional Disnea-12. Arch Bronconeumol. 2018, 54, 74–78. [Google Scholar]
- Zanini, A.; Aiello, M.; Cherubino, F.; Zampogna, E.; Azzola, A.; Chetta, A.; Spanevello, A. The One Repetition Maximum Test and the Sit-To-Stand Test in the Assessment of a Specific Pulmonary Rehabilitation Program on Peripheral Muscle Strength in COPD Patients. Int. J. Chronic Obstr. Pulm. Dis. 2015, 10, 2423–2430. [Google Scholar] [CrossRef] [Green Version]
- Zanini, A.; Crisafulli, E.; D’Andria, M.; Gregorini, C.; Cherubino, F.; Zampogna, E.; Azzola, A.; Spanevello, A.; Schiavone, N.; Chetta, A. Minimum Clinically Important Difference in 30-s Sit-to-Stand Test After Pulmonary Rehabilitation in Subjects with COPD. Respir. Care 2019, 64, 1261–1269. [Google Scholar] [CrossRef]
- Wilson, R.C.; Jones, P.W. A comparison of the visual analogue scale and modified Borg scale for the measurement of dyspnoea during exercise. Clin. Sci. 1989, 76, 277–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef]
- Williams, N. The Borg Rating of Perceived Exertion (RPE) scale. Occup. Med. 2017, 67, 404–405. [Google Scholar] [CrossRef] [Green Version]
- Ganapathy, K. Telemedicine and Neurological Practice in the COVID-19 Era. Neurol. India 2020, 68, 555–559. [Google Scholar] [CrossRef] [PubMed]
- Scherrenberg, M.; Wilhelm, M.; Hansen, D.; Völler, H.; Cornelissen, V.; Frederix, I.; Kemps, H.; Dendale, P. The future is now: A call for action for cardiac telerehabilitation in the COVID-19 pandemic from the secondary prevention and rehabilitation section of the European Association of Preventive Cardiology. Eur. J. Prev. Cardiol. 2020, 2047487320939671. [Google Scholar] [CrossRef]
- Cottrell, M.A.; Russell, T.G. Telehealth for musculoskeletal physiotherapy. Musculoskelet. Sci. Pract. 2020, 48, 102193. [Google Scholar] [CrossRef]
- Mukaino, M.; Tatemoto, T.; Kumazawa, N.; Tanabe, S.; Katoh, M.; Saitoh, E.; Otaka, Y. An Affordable, User-friendly Telerehabilitation System Assembled Using Existing Technologies for Individuals Isolated With COVID-19: Development and Feasibility Study. JMIR Rehabil. Assist. Technol. 2020, 7, e24960. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.J.; Chau, B.; Lui, M.; Lam, G.T.; Lin, N.; Humbert, S. Physical Medicine and Rehabilitation and Pulmonary Rehabilitation for COVID-19. Am. J. Phys. Med. Rehabil. 2020, 99, 769–774. [Google Scholar] [CrossRef]
- Curci, C.; Pisano, F.; Bonacci, E.; Camozzi, D.M.; Ceravolo, C.; Bergonzi, R.; De Franceschi, S.; Moro, P.; Guarnieri, R.; Ferrillo, M.; et al. Early rehabilitation in post-acute COVID-19 patients: Data from an Italian COVID-19 Rehabilitation Unit and proposal of a treatment protocol. Eur. J. Phys. Rehabil. Med. 2020, 56, 633–641. [Google Scholar] [CrossRef]
- Polastri, M.; Nava, S.; Clini, E.; Vitacca, M.; Gosselink, R. COVID-19 and pulmonary rehabilitation: Preparing for phase three. Eur. Respir. J. 2020, 55, 2001822. [Google Scholar] [CrossRef] [PubMed]
- Sun, J.; Liu, J.; Li, H.; Shang, C.; Li, T.; Ji, W.; Wu, J.; Han, X.; Shi, Z. Pulmonary rehabilitation focusing on the regulation of respiratory movement can improve prognosis of severe patients with COVID-19. Ann. Palliat. Med. 2021. [Google Scholar] [CrossRef]
- Oliveira, T.L.; Melo, I.S.; Cardoso-Sousa, L.; Santos, I.A.; El Zoghbi, M.B.; Shimoura, C.G.; Georjutti, R.P.; Castro, O.W.; Goulart, L.R.; Jardim, A.C.G.; et al. Pathophysiology of SARS-CoV-2 in Lung of Diabetic Patients. Front. Physiol. 2020, 11, 587013. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.L.; Yang, T. Pulmonary rehabilitation for patients with coronavirus disease 2019 (COVID-19). Chronic Dis. Transl. Med. 2020, 6, 79–86. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Group | Z | |
|---|---|---|---|
| Intervention | Control | p | |
| Age (i) | 40.79 ± 9.84 | 40.32 ± 12.53 | 0.056 a |
| Gender (ii) (male, female; %) | 52.6 (10/19); 47.4 (9/19) | 57.9 (11/19); 42.1 (8/19) | 0.744 c |
| BS (i) | 41.95 ± 4.03 | 48.17 ± 3.48 | 0.082 a |
| MD12 (i) | 12.26 ± 5.92 | 9.74 ± 7.26 | 0.054 a |
| 30STST (i) | 12.68 ± 5.33 | 11.42 ± 3.06 | 0.076 a |
| 6MWT (i) | 374.72 ± 151.59 | 393.00 ± 124.60 | 0.042 b |
| Variables | Intervention | Valor p | Control | Valor p |
|---|---|---|---|---|
| BS | ||||
| Pre | 5.58 ± 2.32 | 4.58 ± 1.89 | 0.292 | |
| Post | 2.95 ± 1.27 | <0.001 * | 4.26 ± 1.85 | |
| MD12 | ||||
| Pre | 12.26 ± 5.92 | 9.74 ± 7.26 | 0.822 | |
| Post | 5.89 ± 3.48 | <0.001 * | 9.79 ± 7.47 | |
| 30STST | ||||
| Pre | 12.68 ± 5.33 | 11.42 ± 3.06 | ||
| Post | 14.00 ± 5.47 | 0.001 * | 11.11 ± 3.78 | 0.629 |
| 6MWT | ||||
| Pre | 374.72 ± 151.59 | 393.00 ± 124.60 | ||
| Post | 487.58 ± 133.36 | 0.006 * | 399.00 ± 126.07 | 0.144 |
| Variables | Intervention | Control | f/R2 | p |
|---|---|---|---|---|
| BS_DIF | ||||
| −2.63 ± −1.05 | −0.32 ± −0.04 | 31.338/0.465 | <0.001 * | |
| MD12_DIF | ||||
| −6.37 ± −2.44 | 0.05 ± 0.21 | 66.711/0.650 | <0.001 * | |
| 30STST_DIF | ||||
| 1.32 ± 0.14 | −0.31 ± 0.72 | 11.946/0.249 | 0.001 * | |
| 6MWT_DIF | ||||
| 112.86 ± −18.23 | 6.00 ± 1.47 | 9.279/0.205 | 0.007 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzalez-Gerez, J.J.; Saavedra-Hernandez, M.; Anarte-Lazo, E.; Bernal-Utrera, C.; Perez-Ale, M.; Rodriguez-Blanco, C. Short-Term Effects of a Respiratory Telerehabilitation Program in Confined COVID-19 Patients in the Acute Phase: A Pilot Study. Int. J. Environ. Res. Public Health 2021, 18, 7511. https://doi.org/10.3390/ijerph18147511
Gonzalez-Gerez JJ, Saavedra-Hernandez M, Anarte-Lazo E, Bernal-Utrera C, Perez-Ale M, Rodriguez-Blanco C. Short-Term Effects of a Respiratory Telerehabilitation Program in Confined COVID-19 Patients in the Acute Phase: A Pilot Study. International Journal of Environmental Research and Public Health. 2021; 18(14):7511. https://doi.org/10.3390/ijerph18147511
Chicago/Turabian StyleGonzalez-Gerez, Juan Jose, Manuel Saavedra-Hernandez, Ernesto Anarte-Lazo, Carlos Bernal-Utrera, Manuel Perez-Ale, and Cleofas Rodriguez-Blanco. 2021. "Short-Term Effects of a Respiratory Telerehabilitation Program in Confined COVID-19 Patients in the Acute Phase: A Pilot Study" International Journal of Environmental Research and Public Health 18, no. 14: 7511. https://doi.org/10.3390/ijerph18147511