
High Levels of Fine Particulate Matter (PM2.5) Concentrations from Burning Solid Fuels in Rural Households of Butajira, Ethiopia

 , and
, and
Abstract
:1. Introduction
2. Methods and Materials
2.1. Study Design and Period
2.2. Study Area and Recruitment of Households
2.3. Interview Based on Questionnaires
2.4. Quantification and Monitoring of PM2.5
2.5. Particulate Matter Data Quality Assurance
2.6. Statistical Analysis
2.7. Ethical Approval
3. Results
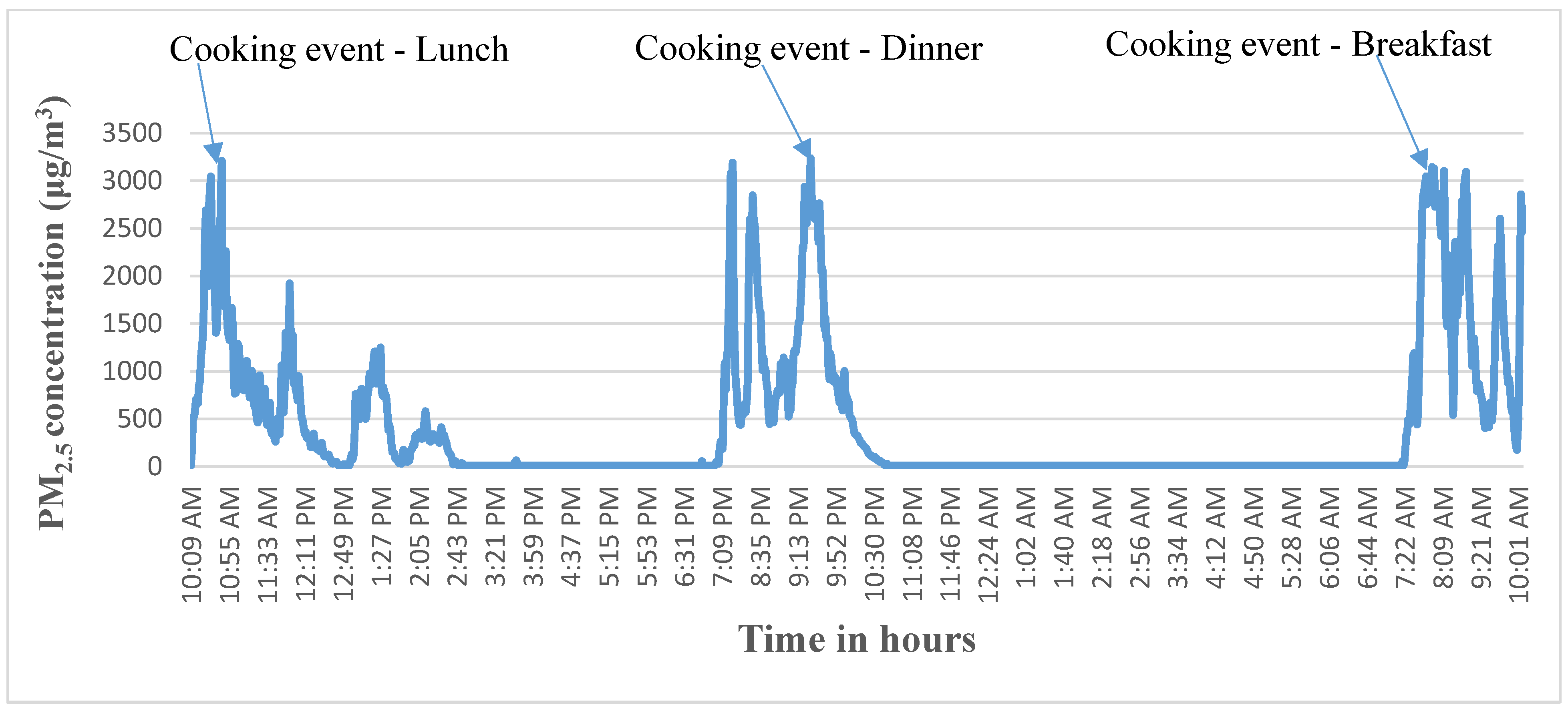
3.1. Mean PM2.5 Concentration in Relation to Cooking and Housing Conditions
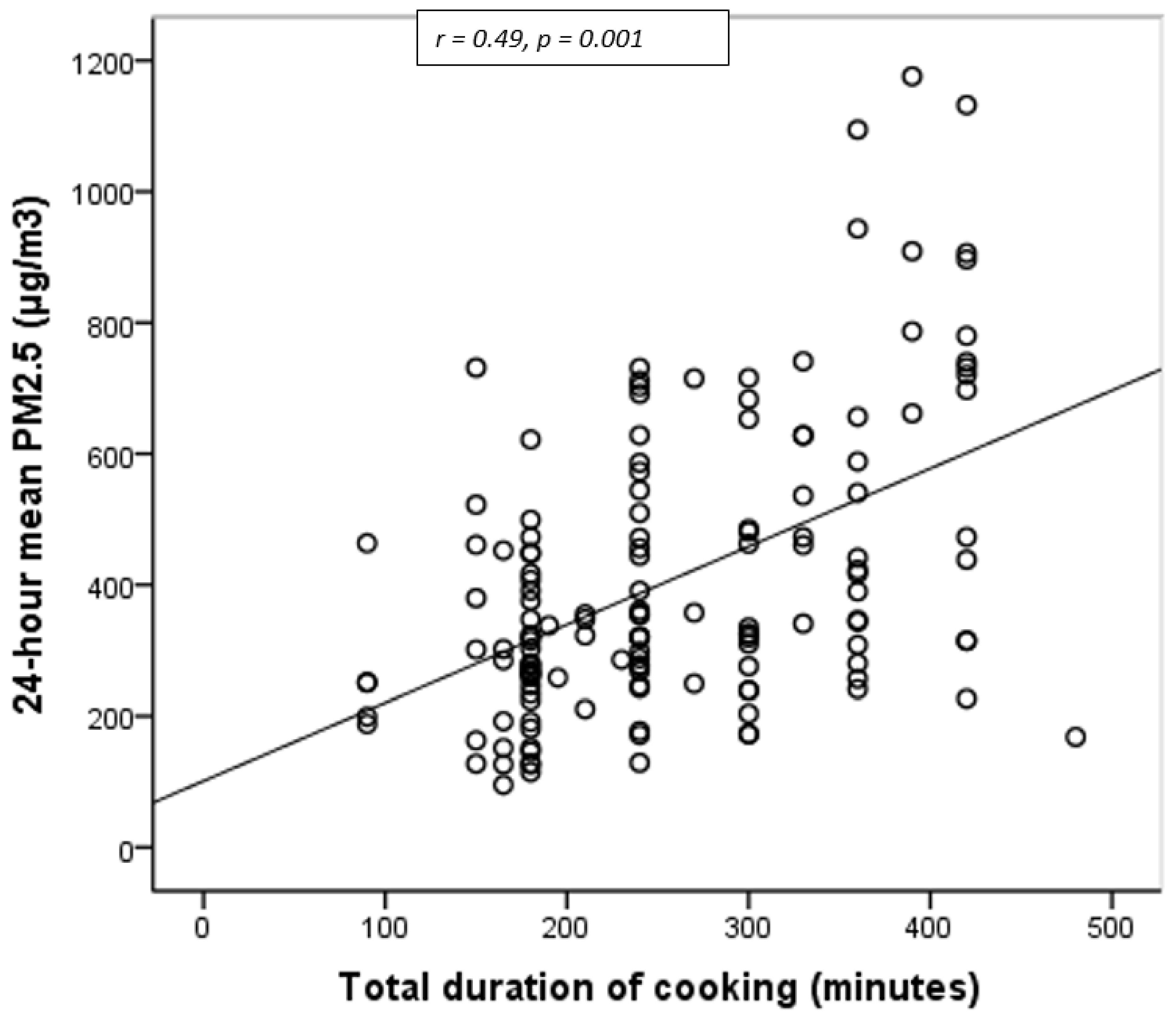
3.2. Correlation between 24-h Mean PM2.5 and Total Duration of Cooking
4. Discussion
5. Conclusions and Recommendation
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Household Air Pollution and Health. Available online: http://www.who.int/mediacentre/factsheets/fs292/en/ (accessed on 17 July 2020).
- Champion, W.M.; Connors, L.; Montoya, L.D. Emission factors of fine particulate matter, organic and elemental carbon, carbon monoxide, and carbon dioxide for four solid fuels commonly used in residential heating by the U.S. Navajo Nation. J. Air Waste Manag. Assoc. 2017, 67, 1020–1035. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Du, Y.; Xu, X.; Chu, M.; Guo, Y.; Wang, J. Air particulate matter and cardiovascular disease: The epidemiological, biomedical and clinical evidence. J. Thorac. Dis. 2016, 8, 8–19. [Google Scholar] [CrossRef]
- Smith, K.R.; McCracken, J.P.; Weber, M.W.; Hubbard, A.; Jenny, A.; Thompson, L.M.; Balmes, J.; Diaz, A.; Arana, B.; Bruce, N. Effect of reduction in household air pollution on childhood pneumonia in Guatemala (RESPIRE): A randomised controlled trial. Lancet 2011, 378, 1717–1726. [Google Scholar] [CrossRef]
- Sharma, D.; Jain, S. Impact of intervention of biomass cookstove technologies and kitchen characteristics on indoor air quality and human exposure in rural settings of India. Environ. Int. 2019, 123, 240–255. [Google Scholar] [CrossRef]
- Okello, G.; Devereux, G.; Semple, S. Women and girls in resource poor countries experience much greater exposure to household air pollutants than men: Results from Uganda and Ethiopia. Environ. Int. 2018, 119, 429–437. [Google Scholar] [CrossRef] [PubMed]
- Pramitha, E.; Haryanto, B. Effect of Exposure to 2.5 μm Indoor Particulate Matter on Adult Lung Function in Jakarta. Osong Public Health Res. Perspect. 2019, 10, 51–55. [Google Scholar] [CrossRef]
- Gordon, S.; Bruce, N.G.; Grigg, J.; Hibberd, P.L.; Kurmi, O.P.; Lam, K.B.H.; Mortimer, K.; Asante, K.P.; Balakrishnan, K.; Balmes, J.; et al. Respiratory risks from household air pollution in low and middle income countries. Lancet Respir. Med. 2014, 2, 823–860. [Google Scholar] [CrossRef] [Green Version]
- Cao, Q.; Rui, G.; Liang, Y. Study on PM2.5 pollution and the mortality due to lung cancer in China based on geographic weighted regression model. BMC Public Health 2018, 18, 925. [Google Scholar] [CrossRef] [PubMed]
- Pokhrel, A.K.; Smith, K.R.; Khalakdina, A.; Deuja, A.; Bates, M.N. Case–control study of indoor cooking smoke exposure and cataract in Nepal and India. Int. J. Epidemiol. 2005, 34, 702–708. [Google Scholar] [CrossRef] [Green Version]
- Dherani, M.; Pope, D.; Mascarenhas, M.; Smith, K.R.; Weber, M.; Bruce, N. Indoor air pollution from unprocessed solid fuel use and pneumonia risk in children aged under five years: A systematic review and meta-analysis. Bull. World Health Organ. 2008, 86, 390–398. [Google Scholar]
- Bede-Ojimadu, O.; Orisakwe, O.E. Exposure to Wood Smoke and Associated Health Effects in Sub-Saharan Africa: A Systematic Review. Ann. Glob. Health 2020, 86, 32. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. WHO Air Quality Guidelines for Particulate Matter, Ozone, Nitrogen Dioxide and Sulfur Dioxide: Global Update Summary of Risk Assessment; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Asikainen, A.; Carrer, P.; Kephalopoulos, S.; Fernandes, E.D.O.; Wargocki, P.; Hänninen, O. Reducing burden of disease from residential indoor air exposures in Europe (HEALTHVENT project). Environ. Health 2016, 15, 61–72. [Google Scholar] [CrossRef]
- Desai, M.; Mehta, S.; Smith, K. Indoor Smoke from Solid Fuels: Assessing the Environmental Burden of Disease at National and Local Levels; WHO Environmental Burden of Disease Series, No. 4; World Health Organization: Geneva, Switzerland, 2004. [Google Scholar]
- UN. The World Population Prospects: 2015 Revision; United Nations: New York, NY, USA, 2015; Available online: https://www.un.org/en/development/desa/publications/world-population-prospects-2015-revision.html (accessed on 20 July 2020).
- Aboubacar, B.; Deyi, X.; Razak, M.Y.A.; Leyla, B.H. The Effect of PM2.5 from Household Combustion on Life Expectancy in Sub-Saharan Africa. Int. J. Environ. Res. Public Health 2018, 15, 748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owili, P.O.; Muga, M.A.; Pan, W.-C.; Kuo, H.-W. Cooking fuel and risk of under-five mortality in 23 Sub-Saharan African countries: A population-based study. Int. J. Environ. Health Res. 2017, 27, 191–204. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tamire, M.; Addissie, A.; Kumie, A.; Husmark, E.; Skovbjerg, S.; Andersson, R.; Lärstad, M. Respiratory Symptoms and Lung Function among Ethiopian Women in Relation to Household Fuel Use. Int. J. Environ. Res. Public Health 2019, 17, 41. [Google Scholar] [CrossRef] [Green Version]
- Demelash, H.; Motbainor, A.; Nigatu, D.; Gashaw, K.; Melese, A. Risk factors for low birth weight in Bale zone hospitals, South-East Ethiopia: A case–control study. BMC Pregnancy Childbirth 2015, 15, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Biruck, Y.; Suleiman, H.; Asfaw, A. Household fuel use and acute respiratory infections among younger children: An exposure assessment in Shebedino Wereda, Southern Ethiopia. Afr. J. Health Sci. 2011, 18, 31–36. [Google Scholar]
- Admasie, A.; Kumie, A.; Worku, A. Children under Five from Houses of Unclean Fuel Sources and Poorly Ventilated Houses Have Higher Odds of Suffering from Acute Respiratory Infection in Wolaita-Sodo, Southern Ethiopia: A Case-Control Study. J. Environ. Public Health 2018, 2018, 1–9. [Google Scholar] [CrossRef]
- Gebremariam, T.H.; Binegdie, A.B.; Mitiku, A.S.; Ashagrie, A.W.; Gebrehiwot, K.G.; Huluka, D.K.; Sherman, C.B.; Schluger, N.W. Level of asthma control and risk factors for poor asthma control among clinic patients seen at a Referral Hospital in Addis Ababa, Ethiopia. BMC Res. Notes 2017, 10, 558. [Google Scholar] [CrossRef] [Green Version]
- Shamebo, D.; Sandström, A.; Wall, S. The Butajira Rural Health Project in Ethiopia: Epidemiological Surveillance for Research and Intervention in Primary Health Care. Scand. J. Prim. Health Care 1992, 10, 198–205. [Google Scholar] [CrossRef]
- Pillarisetti, A.; Allen, T.; Ruiz-Mercado, I.; Edwards, R.; Chowdhury, Z.; Garland, C.; Hill, L.D.; Johnson, M.; Litton, C.D.; Lam, N.L.; et al. Small, Smart, Fast, and Cheap: Microchip-Based Sensors to Estimate Air Pollution Exposures in Rural Households. Sensors 2017, 17, 1879. [Google Scholar] [CrossRef]
- Mukhopadhyay, R.; Sambandam, S.; Pillarisetti, A.; Jack, D.; Mukhopadhyay, K.; Balakrishnan, K.; Vaswani, M.; Bates, M.N.; Kinney, P.L.; Arora, N.; et al. Cooking practices, air quality, and the acceptability of advanced cookstoves in Haryana, India: An exploratory study to inform large-scale interventions. Glob. Health Action 2012, 5, 1–13. [Google Scholar] [CrossRef]
- Nasar, Z.A.; Colbeck, I.; Ali, Z.; Ahmad, S. Indoor particulate matter in developing countries: A case study in Pakistan and potential intervention strategies. Environ. Res. Lett. 2013, 8, 024002. [Google Scholar] [CrossRef] [Green Version]
- Dionisio, K.L.; Howie, S.R.C.; Dominici, F.; Fornace, K.; Spengler, J.D.; Adegbola, R.A.; Ezzati, M. Household Concentrations and Exposure of Children to Particulate Matter from Biomass Fuels in The Gambia. Environ. Sci. Technol. 2012, 46, 3519–3527. [Google Scholar] [CrossRef] [Green Version]
- McCracken, J.P.; Schwartz, J.; Díaz, A.; Bruce, N.; Smith, K.R. Longitudinal Relationship between Personal CO and Personal PM2.5 among Women Cooking with Woodfired Cookstoves in Guatemala. PLoS ONE 2013, 8, 55670. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Admasie, A.; Kumie, A.; Worku, A.; Tsehayu, W. Household fine particulate matter (PM2.5) concentrations from cooking fuels: The case in an urban setting, Wolaita Sodo, Ethiopia. Air Qual. Atmos. Health 2019, 12, 755–763. [Google Scholar] [CrossRef]
- Van Vliet, E.D.; Asante, K.; Jack, D.W.; Kinney, P.L.; Whyatt, R.M.; Chillrud, S.N.; Abokyi, L.; Zandoh, C.; Owusu-Agyei, S. Personal exposures to fine particulate matter and black carbon in households cooking with biomass fuels in rural Ghana. Environ. Res. 2013, 127, 40–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balakrishnan, K.; Ghosh, S.; Ganguli, B.; Sambandam, S.; Bruce, N.; Barnes, D.F.; Smith, K.R. State and national household concentrations of PM2.5 from solid cookfuel use: Results from measurements and modeling in India for estimation of the global burden of disease. Environ. Health 2013, 12, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumie, A.; Emmelin, A.; Wahlberg, S.; Berhane, Y.; Ali, A.; Mekonnen, E.; Brandstrom, D. Magnitude of indoor NO2from biomass fuels in rural settings of Ethiopia. Indoor Air 2009, 19, 14–21. [Google Scholar] [CrossRef] [PubMed]
- Teferi Taye, M.; Tadesse, T.; Senay, G.; Block, P. The Grand Ethiopian Renaissance Dam: Source of cooperation or contention? J. Water Resour. Plan. Manag. 2016, 142, 1–5. [Google Scholar]
- Sulaiman, C.; Abdul-Rahim, A. The Impact of Wood Fuel Energy on Economic Growth in Sub-Saharan Africa: Dynamic Macro-Panel Approach. Sustainability 2020, 12, 3280. [Google Scholar] [CrossRef] [Green Version]
- Johnston, H.J.; Mueller, W.; Steinle, S.; Vardoulakis, S.; Tantrakarnapa, K.; Loh, M.; Cherrie, J.W. How Harmful Is Particulate Matter Emitted from Biomass Burning? A Thailand Perspective. Curr. Pollut. Rep. 2019, 5, 353–377. [Google Scholar] [CrossRef] [Green Version]
- Desservettaz, M.; Phillips, F.; Naylor, T.; Price, O.; Samson, S.; Kirkwood, J.; Paton-Walsh, C. Air Quality Impacts of Smoke from Hazard Reduction Burns and Domestic Wood Heating in Western Sydney. Atmosphere 2019, 10, 557. [Google Scholar] [CrossRef] [Green Version]
- Zhang, S.; Yuval, B.D.; Raz, R. Predictors of the Indoor-to-Outdoor Ratio of Particle Number Concentrations in Israel. Atmosphere 2020, 11, 1074. [Google Scholar] [CrossRef]
- Li, S.; Xu, J.; Jiang, Z.; Luo, Y.; Yang, Y.; Yu, J. Correlation between indoor air pollution and adult respiratory health in Zunyi City in Southwest China: Situation in two different seasons. BMC Public Health 2019, 19, 723. [Google Scholar] [CrossRef] [PubMed]
- Gurley, E.S.; Salje, H.; Homaira, N.; Ram, P.K.; Haque, R.; Petri, W.A.; Bresee, J.; Moss, W.J.; Luby, S.P.; Breysse, P.; et al. Seasonal concentrations and determinants of indoor particulate matter in a low-income community in Dhaka, Bangladesh. Environ. Res. 2013, 121, 11–16. [Google Scholar] [CrossRef] [Green Version]
- Tamire, M.; Addissie, A.; Skovbjerg, S.; Andersson, R.; Lärstad, M. Socio-Cultural Reasons and Community Perceptions Regarding Indoor Cooking Using Biomass Fuel and Traditional Stoves in Rural Ethiopia: A Qualitative Study. Int. J. Environ. Res. Public Health 2018, 15, 2035. [Google Scholar] [CrossRef] [Green Version]
- Pilishvili, T.; Loo, J.D.; Schrag, S.; Stanistreet, D.; Christensen, B.; Yip, F.; Nyagol, R.; Quick, R.; Sage, M.; Bruce, N. Effectiveness of Six Improved Cookstoves in Reducing Household Air Pollution and Their Acceptability in Rural Western Kenya. PLoS ONE 2016, 11, e0165529. [Google Scholar] [CrossRef] [Green Version]
- Begum, B. Comparison of a Traditional Cook Stove with Improved Cook Stoves Based on Their Emission Characteristics. Nucl. Sci. Appl. 2015, 24, 1–4. [Google Scholar]
- Mamuye, F.; Lemma, B.; Woldeamanuel, T. Emissions and fuel use performance of two improved stoves and determinants of their adoption in Dodola, southeastern Ethiopia. Sustain. Environ. Res. 2018, 28, 32–38. [Google Scholar] [CrossRef]
- Yip, F.; Christensen, B.; Sircar, K.; Naeher, L.; Bruce, N.; Pennise, D.; Lozier, M.; Pilishvili, T.; Farrar, J.L.; Stanistreet, D.; et al. Assessment of traditional and improved stove use on household air pollution and personal exposures in rural western Kenya. Environ. Int. 2017, 99, 185–191. [Google Scholar] [CrossRef]
- Embiale, A.; Chandravanshi, B.S.; Zewge, F.; Sahle-Demessie, E. Indoor air pollution from cook-stoves during Injera baking in Ethiopia, exposure, and health risk assessment. Arch. Environ. Occup. Health 2021, 76, 103–115. [Google Scholar] [CrossRef]
- Thomas, E.; Wickramasinghe, K.; Mendis, S.; Roberts, N.; Foster, C. Improved stove interventions to reduce household air pollution in low and middle income countries: A descriptive systematic review Environmental health. BMC Public Health 2015, 15, 650. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adane, M.M.; Alene, G.D.; Mereta, S.T. Biomass-fuelled improved cookstove intervention to prevent household air pollution in Northwest Ethiopia: A cluster randomized controlled trial. Environ. Health Prev. Med. 2021, 26, 1–15. [Google Scholar] [CrossRef]
- Balakrishnan, K.; Sambandam, S.; Ghosh, S.; Mukhopadhyay, K.; Vaswani, M.; Arora, N.K.; Jack, D.; Pillariseti, A.; Bates, M.N.; Smith, K.R. Household Air Pollution Exposures of Pregnant Women Receiving Advanced Combustion Cookstoves in India: Implications for Intervention. Ann. Glob. Health 2015, 81, 375–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanbata, H.; Asfaw, A.; Kumie, A. Indoor air pollution in slum neighbourhoods of Addis Ababa, Ethiopia. Atmos. Environ. 2014, 89, 230–234. [Google Scholar] [CrossRef]
- Mortimer, K.; Ndamala, C.B.; Naunje, A.W.; Malava, J.; Katundu, C.; Weston, W.; Havens, D.; Pope, D.; Bruce, N.G.; Nyirenda, M.; et al. A cleaner burning biomass-fuelled cookstove intervention to prevent pneumonia in children under 5 years old in rural Malawi (the Cooking and Pneumonia Study): A cluster randomised controlled trial. Lancet 2017, 389, 167–175. [Google Scholar] [CrossRef] [Green Version]
- Majdan, M.; Svaro, M.; Muendo, R.; Taylor, M.; Kralova, Z. Effectiveness of various ventilation systems in reducing exposure to biomass related particles: A real-life experiment. Ann. Trop. Med. Public Health 2015, 8, 45. [Google Scholar] [CrossRef]
- Parajuli, I.; Lee, H.; Shrestha, K.R. Indoor Air Quality and ventilation assessment of rural mountainous households of Nepal. Int. J. Sustain. Built Environ. 2016, 5, 301–311. [Google Scholar] [CrossRef] [Green Version]
- Weaver, A.M.; Sharmin, I.; Parveen, S.; Crabtree-Ide, C.; Luby, S.P.; Mu, L.; Goswami, D.; Rudra, C.; Ram, P.K.; Fry, A.M.; et al. Pilot Intervention Study of Household Ventilation and Fine Particulate Matter Concentrations in a Low-Income Urban Area, Dhaka, Bangladesh. Am. J. Trop. Med. Hyg. 2017, 97, 615–623. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | Households, n (%) | |
|---|---|---|
| Villages | Dirama | 25 (17) |
| Dobena | 30 (20) | |
| Misrak Meskan | 29 (20) | |
| Shersherebedo | 26 (18) | |
| Wurib | 37 (25) | |
| Type of house | Tukul | 126 (86) |
| Tin | 21 (14) | |
| Family size | Five or less | 54 (37) |
| Six and above | 93 (63) | |
| Season (during data collection) | Rainy (Wet) | 65 (44) |
| Dry | 82 (56) | |
| Frequency of cooking in 24 h | Three times or less | 65 (44) |
| Four times | 82 (56) | |
| Primary fuel type | Wood | 147 (100) |
| Type of stove | Traditional three-clay stove | 100 (68) |
| Improved/moveable | 47 (32) | |
| Secondary fuel type | Crop residue only | 72 (49) |
| Dung only | 2 (1) | |
| Crop residue and dung | 66 (45) | |
| Charcoal | 7 (5) | |
| Duration (minutes) of cooking in 24 h * | Mean (95% CI) | 258 (244–273) |
| PM2.5 (μg/m3) | Mean (95% CI) | 410 (370–450) |
| Median (Min-Max) | 340 (100–1200) | |
| Geometric mean | 360 | |
| 25th percentile | 260 | |
| 75th percentile | 510 | |
| 95th percentile | 850 | |
| Characteristics (n) | Mean PM2.5 in μg/m3 (SD) | 95% CI | p-Value | |
|---|---|---|---|---|
| Family size | Five or less (85) | 390 (210) | 340–430 | 0.208 |
| Six or above (62) | 440 (230) | 380–500 | ||
| Type of house | Tukul house (126) | 420 (220) | 380–430 | 0.092 |
| Tin house (21) | 330 (210) | 240–430 | ||
| Type of stove | Traditional three-clay (100) | 440 (240) | 390–490 | 0.009 * |
| Improved/moveable (47) | 340 (140) | 300–380 | ||
| Door opened during cooking at night | No (52) | 470 (240) | 400–530 | 0.017 * |
| Yes (95) | 380 (200) | 340–530 | ||
| Window open during cooking | No (102) | 430 (230) | 390–480 | 0.032 * |
| Yes (45) | 350 (200) | 300–410 | ||
| Cooking frequency | Three or less (110) | 420 (230) | 370–460 | 0.534 |
| Four times (37) | 390 (193) | 330–450 | ||
| Season of the year | Rainy/Wet (65) | 420 (240) | 360–480 | 0.542 |
| Dry (82) | 400 (210) | 350–440 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tamire, M.; Kumie, A.; Addissie, A.; Ayalew, M.; Boman, J.; Skovbjerg, S.; Andersson, R.; Lärstad, M. High Levels of Fine Particulate Matter (PM2.5) Concentrations from Burning Solid Fuels in Rural Households of Butajira, Ethiopia. Int. J. Environ. Res. Public Health 2021, 18, 6942. https://doi.org/10.3390/ijerph18136942
Tamire M, Kumie A, Addissie A, Ayalew M, Boman J, Skovbjerg S, Andersson R, Lärstad M. High Levels of Fine Particulate Matter (PM2.5) Concentrations from Burning Solid Fuels in Rural Households of Butajira, Ethiopia. International Journal of Environmental Research and Public Health. 2021; 18(13):6942. https://doi.org/10.3390/ijerph18136942
Chicago/Turabian StyleTamire, Mulugeta, Abera Kumie, Adamu Addissie, Mulugeta Ayalew, Johan Boman, Susann Skovbjerg, Rune Andersson, and Mona Lärstad. 2021. "High Levels of Fine Particulate Matter (PM2.5) Concentrations from Burning Solid Fuels in Rural Households of Butajira, Ethiopia" International Journal of Environmental Research and Public Health 18, no. 13: 6942. https://doi.org/10.3390/ijerph18136942