1. Background
Globally, approximately over 290,000 maternal deaths every year and about 99% of the global maternal mortality rates occur in developing countries, with the Sub-Saharan Africa (SSA) region reporting two-thirds (66%) of maternal deaths [
1]. Evidence has conveyed that women’s health is critical for the health of the entire family and health service utilisation is paramount [
1]. However, little attention has been focused on women’s empowerment in the utilisation of family planning in SSA [
1].
The fifth Sustainable Development Goal (SDG) is to achieve gender equality and empowerment of all women and girls [
2]. Reducing gender inequality is a vital policy agenda globally and access and rights to resources are essential for women’s health. The effects of gender inequities persist throughout all phases of women’s lives and play a role in determining years of education, opportunities for career and employment, age at marriage and number and timing of children [
3,
4]. Consequently, gender inequities compromise the rights, safety, well-being and health of women and girls. Gender inequity affects sexual and reproductive health outcomes including unintended and teenage pregnancy, an increased incidence of human immunodeficiency virus (HIV), increased rates of violence against women and girls and increased vulnerability to other sexual risk behaviours [
1,
4,
5,
6]. Women’s inequality in accessing various services is a public health challenge and a human rights violation, and reverting this is critical to achieving SDG targets, including health [
3,
5,
7]. Women’s increased political participation, control of resources including land, access to employment and education are crucial for promoting sustainable development [
8].
Greater gender equality can lead to improvements in health and quality of life for women and their family members by numerous pathways [
4,
9,
10]. Evidence suggests that gender equality or women’s empowerment positively influences family planning use [
1,
3]. Gender inequities limit women’s access to good-quality family planning services. They also hinder women’s ability to negotiate family planning and use contraception effectively. In addition, traditional gender roles generally place greater barriers to women’s access to family planning services [
1,
4,
11,
12].
The implicit assumption is that in most societies, particularly in SSA including Ethiopia, men control the women of their social class, especially in their households, families and health service utilisation including use of family planning [
2,
3,
13]. At the same time, improved health outcomes for women can help to strengthen their empowerment [
1,
14]. Healthy women are more able to actively participate in society and improve economic development by participating in their own social and economic interests [
1,
14,
15]. They are also more likely to have greater bargaining power and control over resources within the household [
1,
14,
16].
Maternal, neonatal and child health (MNCH) specifically focuses on women’s health and children and infants under the age of five. Family planning contributes to women’s health by ensuring women are educated about fertility and contraceptive use so that they can make decisions about their family size [
11]. There has been increased investment towards family planning for women’s health. However, the unmet needs for family planning have declined slowly in many Sub-Saharan African (SSA) countries including Ethiopia [
17]. Investing in family planning is one of the smart investments for development as population dynamics have a fundamental influence on the pillars of sustainable development [
18,
19]. Most importantly, the use of modern contraceptives is known to be highly cost-effective and has poverty-reducing effects, as demonstrated in earlier studies [
18,
20,
21]. Modern contraceptives also assist women in their personal decisions about family size [
11]. Despite family planning’s benefits to women’s health, changes in maternal and child health for women in Ethiopia are limited [
22], however, over the last two decades, Ethiopia has made progress in the areas of maternal, neonatal and child health (MNCH) including reproductive health [
19,
23,
24].
Notable achievements in maternal and child health include a 67% drop in the under-five mortality rate from 1990 estimates, which contributed to an increase in average life expectancy from 45 to 64 years in 2016; the maternal mortality ratio being reduced by 71% to 420/100,000 live births; and the contraceptive prevalence rate being increased from 3% to 36%, leading to a reduction in the total fertility rate from 7.7 in the 1990s to 4.1 in 2014. Modern contraceptive use for currently married women has steadily increased over the last 16 years in Ethiopia from 6% in 2000 to 35% in 2016 [
19,
23,
24]. Regardless, the progress of contraceptive use remains slow [
19,
24]. Contraceptive use is not uniform across regions and population groups and particularly in Ethiopia [
19,
24].
Research Hypothesis
The concept of women’s empowerment is complex, as there is considerable variation in its conceptualisation. Most definitions link empowerment with the power or freedom used to achieve desired outcomes [
25]. The World Bank goes beyond this and defines empowerment as the “expansion of freedom of choice and action to shape one’s life” [
26]. Kabeer (1999) defines women’s empowerment as a “process by which those who have been denied the ability to make strategic life choices acquire such an ability.” [
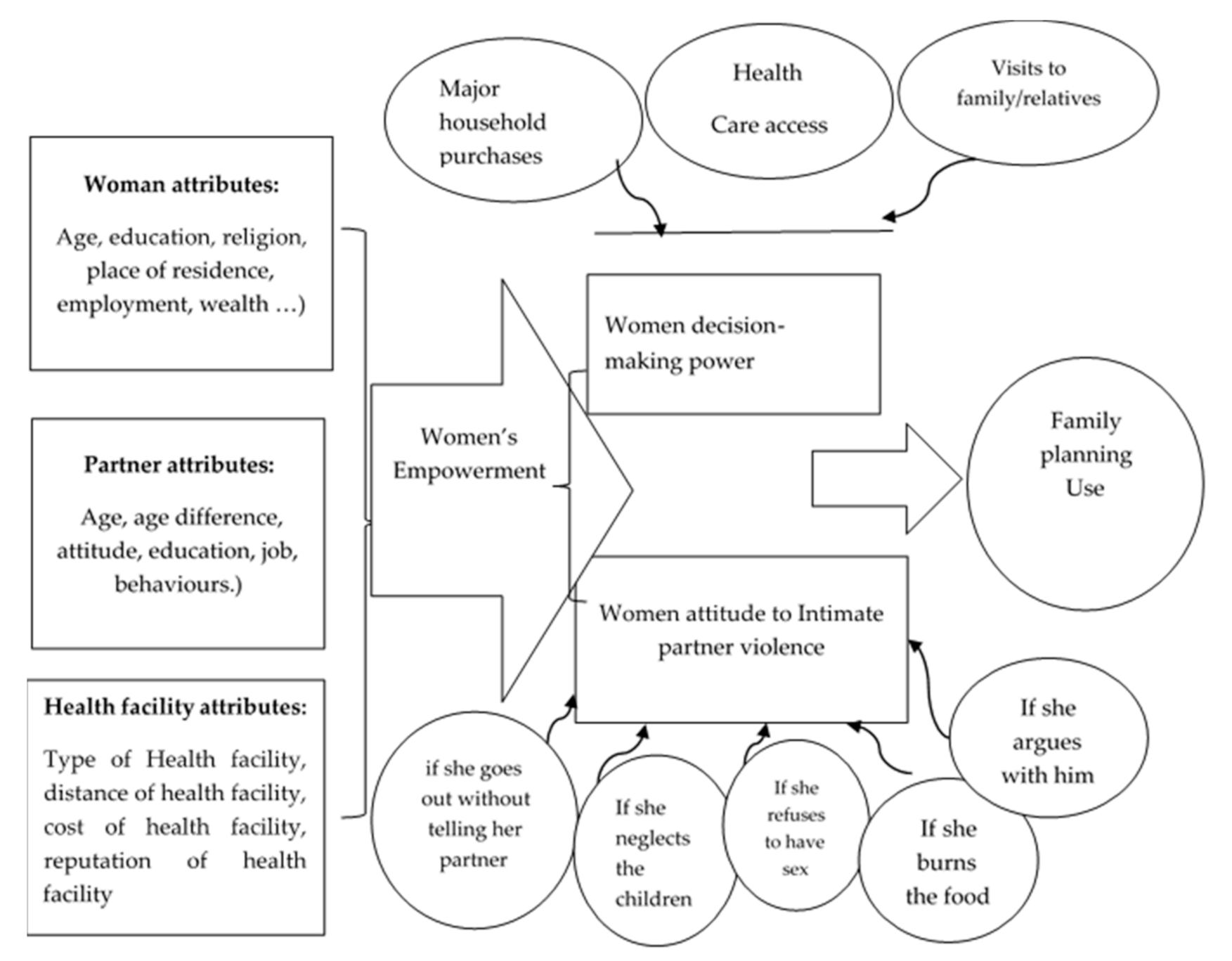
1] Among many frameworks proposed to measure empowerment, the framework proposed by Maholtra, Schuler and Boender (2002) is amongst one of the most comprehensive, in which women’s empowerment is measured in five dimensions and at different levels [
27]. The framework suggests that women’s empowerment could be exercised in five different arenas: household economy, socio-cultural activities, legal activities, politics and psychology.
The other framework used by Haque et al. (2011) [
28] in Bangladesh consisted of three key dimensions: economic decision making, household decision making and women’s physical mobility. In this framework, women are classified as participating in decision making if they make a decision alone or jointly with their partner. The dynamic and multidimensional nature of women’s empowerment, and its existence at various levels, makes it challenging for researchers to measure empowerment. An attempt was made to assess the overall effect of women’s empowerment and its various dimensions on contraceptive use by adapting the structured framework developed by the DHS program as a standard measurement [
29]. Women’s empowerment measures [
24] are demonstrated in
Figure 1. As shown in
Figure 1, women’s attributes, partner attributes and health facility access might positively affect multiple dimensions of empowerment, which in turn promotes family planning use. Women’s empowerment is hypothesised as a predictor of reproductive health outcomes. It is believed that empowered women are more likely to plan their pregnancies, delay marriage, receive prenatal care and visit a skilled health provider during pregnancy and childbirth. It is hypothesised that empowered women are more likely to use contraception in comparison to women who are not (or are less) empowered.
2. Methodology
2.1. Study Design, Population and Setting
A community-based cross-sectional study was employed to collect relevant data for the study. The study population included all women of the reproductive age group (15–49 years) who were married or living together with a partner and lived in the study area for at least six months preceding the survey.
The study was conducted in selected districts of Jimma Zone, which is located 352 km from the capital Addis Ababa in the southwest of Ethiopia. The zone consists of 20 rural districts and one special town administration (Agaro Town), and 46 small urban and 512 rural kebeles (smallest formal administrative units). The study focused on predominantly Muslim communities [
24].
2.2. Sample and Sampling Procedure
Sample size was calculated using the OpenEPI single proportion formula. A total sample size of 746 respondents was included considering the following assumptions: contraceptive prevalence (63.5%) rate of Ethiopia amongst married women [
22], 5% margin of error (d), design effect (DE) of 2 and 5% non-response rate.
Multistage cluster sampling techniques were employed, where districts and kebeles were considered as the primary and secondary sampling units, and households were selected randomly from the selected district. A total of four districts and eight kebeles were selected randomly. The total sample size was proportionally allocated to each selected kebele based on the number of households in each kebele.
2.3. Data Collection and Measurement Tools
Primary data were collected using a structured questionnaire using mobile applications, ODK/KOBO, where a pretested structured questionnaire with pre-coded answers was uploaded. The questionnaire was adopted and developed from EDHS 2016 [
24], women’s empowerment scale and related literature considering the local context and the nature of the project intervention. Data collection tools were translated into the local language and then translated back to English to check their consistency (
Supplementary File S1). The data are freely available (
Supplementary File S2).
2.4. Data Analysis
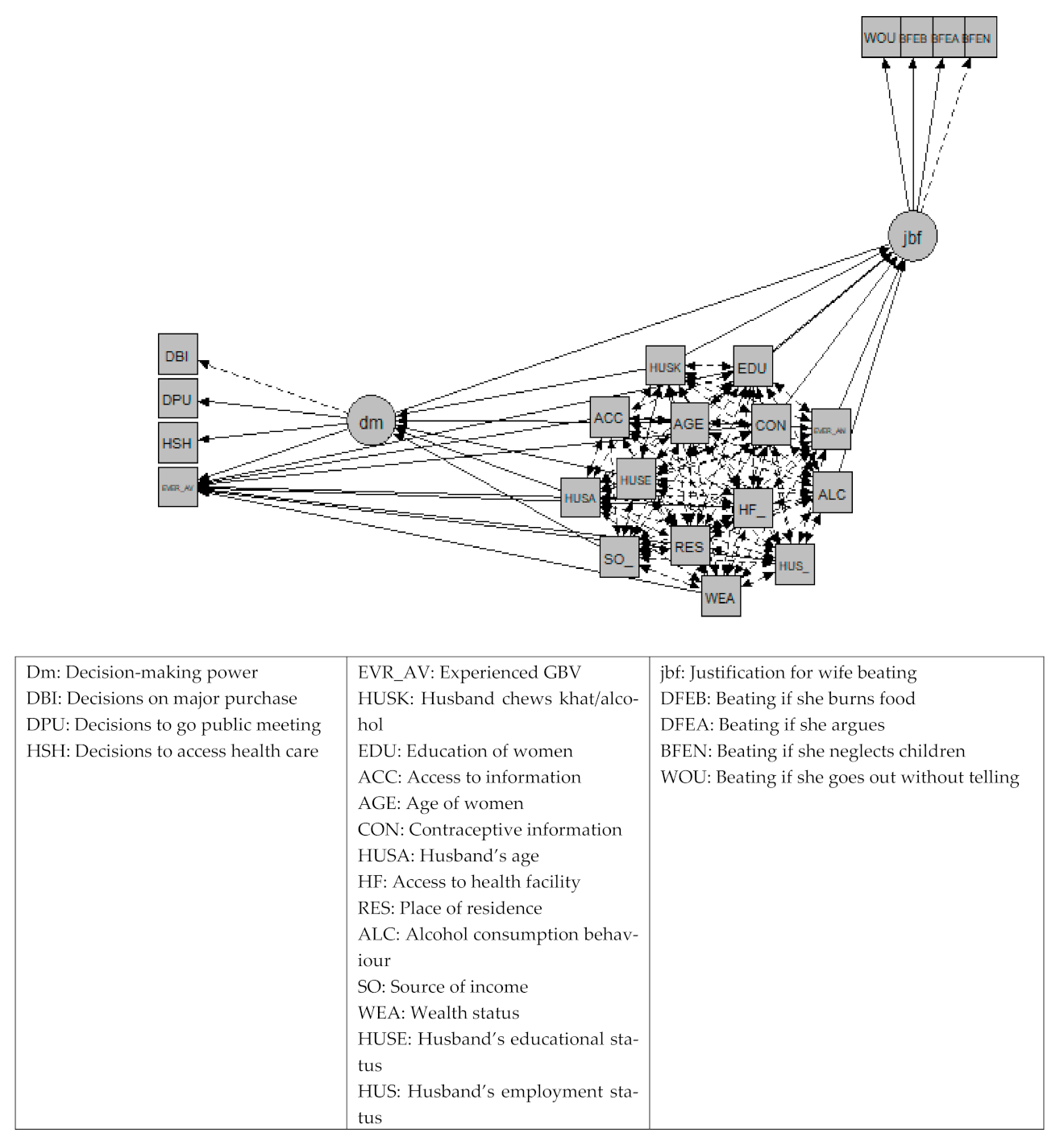
The analysis followed a structural equation model (SEM). Note that the SEM technique is the combination of factor analysis and multiple regression analysis and it is used to analyse the structural relationship between measured variables and latent constructs. The authors preferred this analysis as it is more powerful than regression analyses and it examines linear causal relationships amongst variables, whilst simultaneously accounting for measurement error. Our SEM has two latent constructs, including individual empowerment indicators, to represent each empowerment dimension. The latent variable SEM included family planning use, decision-making power and attitude towards violence as three “endogenous variables” and 12 “exogenous variables”.
Three endogenous variables: Family planning was measured as ever using contraceptives amongst women who were married or had a male partner. Based on women’s responses, it was coded as a binary response of yes if they did, or no if they never used family planning methods. For example, the following question was asked: Have you ever done something or used any modern contraceptive method to delay or avoid getting pregnant? Household decision-making power was examined as a latent construct consisting of three indicators: women’s participation in decisions regarding their own health care, major household purchases and visits to family/relatives. These questions were asked only to women who were currently married/had a partner. The variables were first recoded to examine if women participated in decisions (i.e., alone/jointly with their husband/partner) or not. A latent variable was constructed from the three binary variables for each decision. Attitudes towards violence were examined as a latent construct consisting of five indicators concerning a woman’s acceptance of a wife’s physical violence by her husband/partner. The survey asked about the following five situations: if she goes out without telling him, neglects the children, refuses to have sex with him, argues with him or burns the food. Each variable was first recoded into binary data (i.e., yes accept, or no).
Twelve exogenous variables: Exogenous variables included: current age of the woman, employment, access to information, access to health facilities, awareness about contraceptives, husband’s/partner’s employment status, source of income for the household, woman’s and her partner educational status, wealth status of the family, residing in an urban or rural area, religion, if the woman faced any form of violence in the past and if she and her partner chewed khat or consumed alcohol. Access to health facilities is multidimensional and the following question was asked: Do you have access to a health facility nearby (health center/health posts)? Each response was recorded either as yes or no as binary data. We also asked questions about distances in kilometres travelled, availability of commodities, quality and satisfaction and cost implications for related health access. In Ethiopia, contraceptive use at public health facilities is free of charge and covered by the government.
2.5. Operational Definitions
Women’s empowerment refers to women who participate in all decision making about major purchases, health care access and visits to family and relatives.
The decision-making skill of women refers to women participating in decision making if they make decisions alone or jointly with their partner.
Gender-based violence refers to any public or private act of sexual and gender-based violence that results in, or is likely to result in, physical, sexual or psychological harm or suffering to women, including threats of such acts, coercion or arbitrary deprivation of liberty [
3].
Access to health facilities refers to nearby access to health facilities from their living residence/community.
Contraceptive use refers to a modern method or device used to prevent pregnancy. Traditional methods of birth control were not included.
Contraceptive awareness refers to being informed about modern contraceptives’ methods, purpose and use.
4. Discussion
This study revealed that women’s empowerment is variable and affects their choice of and access to family planning. In this study, the analysis enabled comparisons and testing of several dimensions simultaneously about women’s family planning use. This study investigated the association between contraceptive use and various components of women’s empowerment (three dimensions of decision-making skills and five dimensions of attitudes to physical violence towards wives). The significant association between women’s empowerment and contraceptive use is consistent with the results from previous studies where women’s empowerment was positively associated with the use of health care services in 67 developing countries [
32] and a study conducted on women’s empowerment as an enabling factor of contraceptive use in Sub-Saharan Africa [
4,
33]. Many individual studies in African countries found the same results, showing that that if women were more empowered, they were more likely to use modern contraception [
4,
10,
12,
15,
34,
35]. We propose to develop an integrated approach, to ensure that women’s empowerment and other attributes improve family planning, rather than proposing a standalone intervention.
The reference point for using family planning services amongst married women and unmarried women is different [
36,
37]. Regardless of their background status, unmarried women will use family planning services to avoid getting pregnant [
15,
19,
24]. Additionally, the influence of a male partner is nonexistent amongst unmarried women [
24]. For unmarried women, the influence of decision-making is also different in comparison to married women. Married women in the Ethiopian context are expected to bear children [
15,
24,
35]. Therefore, the status of a woman’s empowerment (decision-making and violence) amongst married women and unmarried women can affect family planning utilisation preference differently [
37]. The relationship between family planning utilisation preference and empowerment can be measured more effectively amongst married women in comparison to unmarried women [
35,
36,
37].
Services being made available for women is not the absolute solution to improve family planning use as this is affected by many factors [
18,
38]. Rather, integrating women’s empowerment, such as improving women’s negotiation skills about the use of family planning services, and educating women about the available family planning services, would boost contraceptive use amongst women [
11,
21,
38]. The empowerment of women is critical in family planning programming to enhance the overall improvement and utilisation of family planning services.
Women’s empowerment had a stronger effect in our analysis when we tested it independently against family planning utilisation. Increased power of making decisions on major household purchases, seeking health care services and attending public meetings were also positively influenced by the older age of the woman and her partner consuming less alcohol, less substance use behaviour and his educational status being higher. One of the most common reasons for not using contraceptives included lack of access to information and health facilities [
39], and this may be attributed to limited access to supplies, in which case health facilities and health care providers have the potential to address and target these challenges. This limited access to health facilities is consistent with our study, resulting in women having limited access to contraceptives and, subsequently, utilisation rates are decreased. Therefore, addressing women’s empowerment could provide a multipronged boost in the utilisation of the services. This could also be related to the cost of transport and lack of understanding about the benefits of using contraceptives.
Similarly, we found that family planning utilisation amongst women living in rural areas was limited, which resonates with other studies [
17,
35]. This could be explained by women residing in rural areas being less educated and having a limited understanding about the significance of family planning. Moreover, rural health facilities may have limited contraceptive supplies for women due to a number of factors, including shortages of supplies, lack of trained health providers and other challenges in the health system [
18].
Some studies have also found that wealthier women are more likely to use contraceptives [
9,
19,
20,
33]. In contrast, our study showed that wealthier women were less likely to use contraceptives. The significance of this finding is that this may be related to women who are wealthier wanting to have more children as they have the capacity to support the children financially without fearing their husband/partner. Additionally, wealthier women are more likely to have more children in the Muslim community [
19,
24,
33]. Furthermore, our study showed that older women were less likely to use contraceptives, although there may be a tendency that wealthier women who are older are less likely to use contraceptives, which is consistent with other studies [
11,
21]. In contrast to our study, increased use of family planning methods was found with higher economic status.
4.1. Strengths and Limitations of the Study
The major strength of this study is the use of the standard measurement for women’s empowerment, which makes the findings of the study comparable with other studies that have used the DHS. Despite the authors employing SEM, this study has some limitations. Prominently, the analyses used cross-sectional data, hence, only associations and no causal relationships were established. The representativeness of the study sample and generalisability of the results are limited due to the omission of women who were unmarried. Additionally, some variability will occur depending upon the context, such as culture, urbanisation, immigration pattern and pastoral nature of the country. Furthermore, social desirability and recall bias could occur in studies that deal with lifetime contraceptive use.
4.2. Conclusion and Recommendations
Based on the findings of this study, it is imperative to note that enhancing women’s empowerment could assist in improving contraceptive utilisation. Women’s empowerment is multifactorial, especially in relation to improved decision making that plays a vital role in health quality outcomes of women. Thus, contraceptive utilisation is of paramount importance in the health of women and their children.
Moreover, this study highlights that not only are the demographic characteristics of a woman and her partner (age and wealth) significant indicators when considering violence but limited access to family planning health facilities also affects contraceptive use for women living in Ethiopia. Future interventions should focus on integrating women’s empowerment through various means such as improving education and economic status and improving negotiation skills for enhanced autonomous decision making regarding family planning use. Further research is warranted regarding the socio-cultural context of women and factors that influence women’s empowerment and family planning use to establish an in-depth understanding so that equitable norms in society are upheld.


 ,
, 



{kind=link}
{kind=link}