
Respiratory Telerehabilitation of Boys and Young Men with Duchenne Muscular Dystrophy in the COVID-19 Pandemic †

 and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.3. Telerehabilitation Exercises
- Breath stacking (positive inspiratory pressure): Patients were asked to take a maximal inhale, and then, without exhaling, to take another 1–3 breaths, and hold for 5 s. Boys were instructed to repeat the exercise 5 times. The aim of the exercise was to increase lung volume. The same exercise was presented with the use of balloons; patients were instructed to inhale the air from a balloon, without exhaling, and try to hold as much air in the lungs as possible for 5 s, repeating 5 times.
- Glossopharyngeal breathing: Patients were instructed to push a series of small volumes of air with their tongue and pharynx into the lungs by saying ”cat” in Polish. Patients were encouraged to repeat the exercise 5 times.
- Positive expiratory pressure: Inflating the balloon. Patients were instructed to inflate the balloon by inhaling by nose and exhaling by mouth, repeating the exercise 3 times. Caregivers were encouraged to try different types of balloons in order to find optimally elastic material (optimal resistance).
2.4. Data by Questionnaire
2.5. Statistical Analysis
3. Results
3.1. Participants Characteristics
3.2. Exercises
3.2.1. Performance of the Exercises
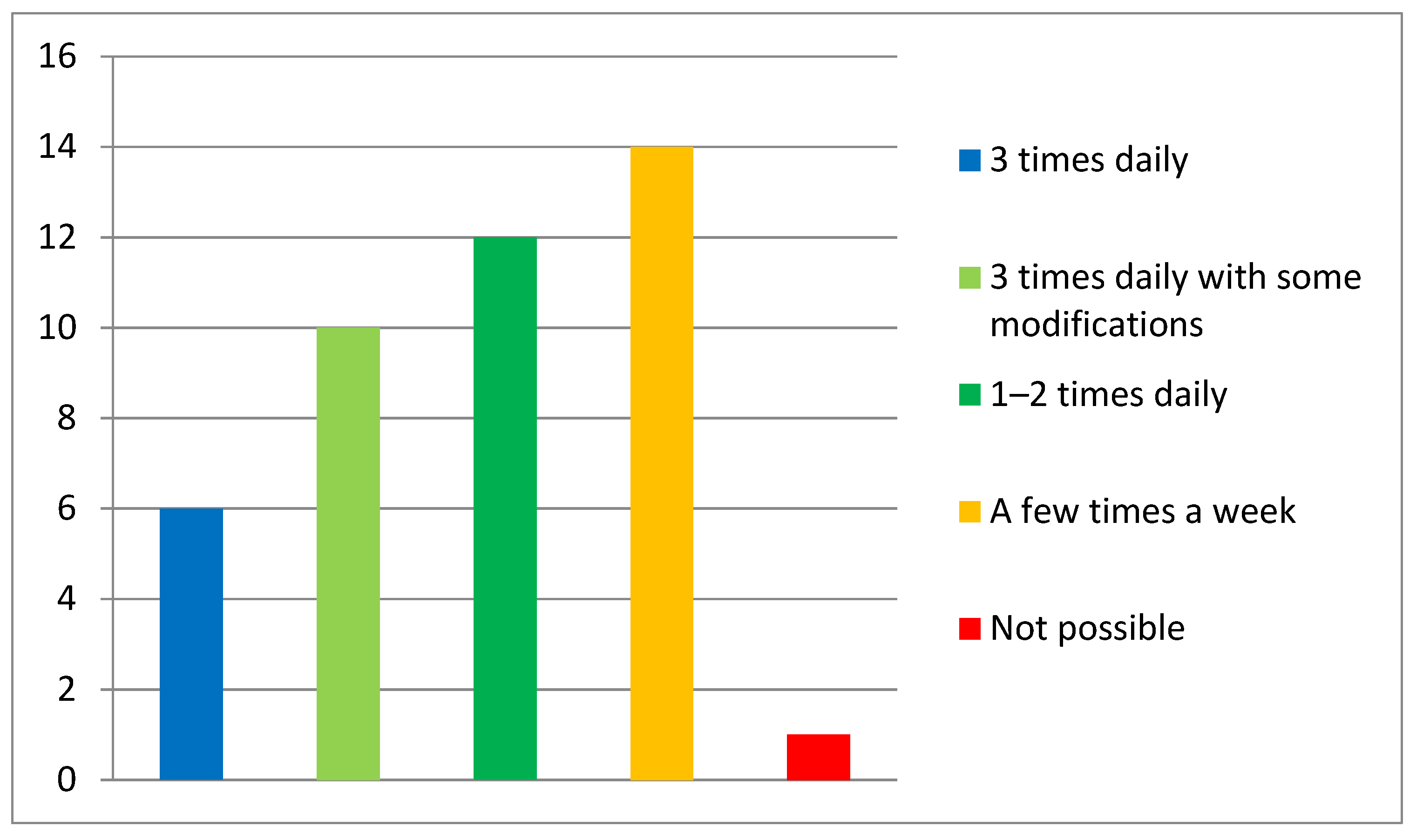
3.2.2. Possibility and Frequency
3.2.3. Difficulty
3.3. Additional Consultations
3.4. Satisfaction, Appropriateness, and Intelligibility
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Birnkrant, D.J.; Bushby, K.; Bann, C.M.; Apkon, S.D.; Blackwell, A.; Brumbaugh, D.; Case, L.E.; Clemens, P.R.; Hadjiyannakis, S.; Pandya, S.; et al. Diagnosis and management of Duchenne muscular dystrophy, part 1: Diagnosis, and neuromuscular, rehabilitation, endocrine, and gastrointestinal and nutritional management. Lancet Neurol. 2018, 17, 251–267. [Google Scholar] [CrossRef] [Green Version]
- Wasilewska, E.; Małgorzewicz, S.; Sobierajska-rek, A.; Jabło, J. Transition from Childhood to Adulthood in Patients with Duchenne Muscular Dystrophy. Medicina 2020, 56, 426. [Google Scholar] [CrossRef]
- Balaban, B.; Matthews, D.J.; Clayton, G.H.; Carry, T. Corticosteroid treatment and functional improvement in Duchenne muscular dystrophy: Long-term effect. Am. J. Phys. Med. Rehabil. 2005, 84, 843–850. [Google Scholar] [CrossRef]
- LoMauro, A.; Romei, M.; Gandossini, S.; Pascuzzo, R.; Vantini, S.; DAngelo, M.G.; Aliverti, A. Evolution of respiratory function in Duchenne muscular dystrophy from childhood to adulthood. Eur. Respir. J. 2018, 51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoque, R. Sleep-Disordered Breathing in Duchenne Muscular Dystrophy: An Assessment of the Literature. J. Clin. Sleep Med. 2016, 12, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Gayraud, J.; Ramonatxo, M.; Rivier, F.; Humberclaude, V.; Petrof, B.; Matecki, S. Ventilatory parameters and maximal respiratory pressure changes with age in Duchenne muscular dystrophy patients. Pediatr. Pulmonol. 2010, 45, 552–559. [Google Scholar] [CrossRef]
- Biggar, W.D.; Harris, V.A.; Eliasoph, L.; Alman, B. Long-term benefits of deflazacort treatment for boys with Duchenne muscular dystrophy in their second decade. Neuromuscul. Disord. 2006, 16, 249–255. [Google Scholar] [CrossRef]
- Wasilewska, E.; Małgorzewicz, S.; Meyer-Szary, J.; Sledzinska, K.; Niedoszytko, M.B.; Jassem, E.; Wierzba, J. Pulmonary dysfunction in children with Duchenne muscular dystrophy may appear earlier than we thought–analysis using novel methodology based on z-scores. Arch. Med. Sci. 2021. [Google Scholar] [CrossRef]
- Sobierajska-Rek, A.; Mański, Ł.; Jabłońska-Brudło, J.; Śledzińska, K.; Ucińska, A.; Wierzba, J. Establishing a telerehabilitation program for patients with Duchenne muscular dystrophy in the COVID-19 pandemic. Wien. Klin. Wochenschr. 2020, 133, 344–350. [Google Scholar] [CrossRef]
- Case, L.E.; Apkon, S.D.; Eagle, M.; Gulyas, A.; Juel, L.; Matthews, D.; Newton, R.A.; Posselt, H.F. Rehabilitation Management of the Patient With Duchenne Muscular Dystrophy. Pediatrics 2018, 142, S17–S33. [Google Scholar] [CrossRef] [Green Version]
- Veerapandiyan, A.; Wagner, K.R.; Apkon, S.; McDonald, C.M.; Mathews, K.D.; Parsons, J.A.; Wong, B.L.; Eichinger, K.; Shieh, P.B.; Butterfield, R.J.; et al. The care of patients with Duchenne, Becker, and other muscular dystrophies in the COVID-19 pandemic. Muscle Nerve 2020, 62, 41–45. [Google Scholar] [CrossRef]
- Parent Project Foundation, Poland. Available online: https://parentproject.org.pl/ (accessed on 15 January 2021).
- Vignos, P.J.J.; Spencer, G.E.J.; Archibald, K.C. Management of progressive muscular dystrophy in childhood. JAMA 1963, 184, 89–96. [Google Scholar] [CrossRef]
- Brooke, M.H.; Griggs, R.C.; Mendell, J.R.; Fenichel, G.M.; Shumate, J.B.; Pellegrino, R.J. Clinical trial in Duchenne dystrophy. I. The design of the protocol. Muscle Nerve 1981, 4, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Rochester, C.L.; Vogiatzis, I.; Holland, A.E.; Lareau, S.C.; Marciniuk, D.D.; Puhan, M.A.; Spruit, M.A.; Masefield, S.; Casaburi, R.; Clini, E.M.; et al. An Official American Thoracic Society/European Respiratory Society Policy Statement: Enhancing Implementation, Use, and Delivery of Pulmonary Rehabilitation. Am. J. Respir. Crit. Care Med. 2015, 192, 1373–1386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hansen, H.; Bieler, T.; Beyer, N.; Kallemose, T.; Wilcke, J.T.; Østergaard, L.M.; Frost Andeassen, H.; Martinez, G.; Lavesen, M.; Frølich, A.; et al. Supervised pulmonary tele-rehabilitation versus pulmonary rehabilitation in severe COPD: A randomised multicentre trial. Thorax 2020, 75, 413–421. [Google Scholar] [CrossRef] [Green Version]
- Tousignant, M.; Marquis, N.; Pagé, C.; Imukuze, N.; Métivier, A.; St-Onge, V.; Tremblay, A. In-home Telerehabilitation for Older Persons with Chronic Obstructive Pulmonary Disease: A Pilot Study. Int. J. Telerehabilit. 2012, 4, 15–24. [Google Scholar] [CrossRef] [Green Version]
- Bourne, S.; DeVos, R.; North, M.; Chauhan, A.; Green, B.; Brown, T.; Cornelius, V.; Wilkinson, T. Online versus face-to-face pulmonary rehabilitation for patients with chronic obstructive pulmonary disease: Randomised controlled trial. BMJ Open 2017, 7, e014580. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Camden, C.; Pratte, G.; Fallon, F.; Couture, M.; Berbari, J.; Tousignant, M. Diversity of practices in telerehabilitation for children with disabilities and effective intervention characteristics: Results from a systematic review. Disabil. Rehabil. 2020, 42, 3424–3436. [Google Scholar] [CrossRef] [PubMed]
- Tanner, K.; Bican, R.; Boster, J.; Christensen, C.; Coffman, C.; Fallieras, K.; Long, R.; Mansfield, C.; O’Rourke, S.; Pauline, L.; et al. Feasibility and Acceptability of Clinical Pediatric Telerehabilitation Services. Int. J. Telerehabilit. 2020, 12, 43–52. [Google Scholar] [CrossRef]
- Topin, N.; Matecki, S.; Le Bris, S.; Rivier, F.; Echenne, B.; Prefaut, C.; Ramonatxo, M. Dose-dependent effect of individualized respiratory muscule training in children with Duchenne muscular dystrophy. Neuromuscul. Disord. 2002, 12, 576–583. [Google Scholar] [CrossRef]
- Rodrigues, M.R.; Carvalho, C.R.; Santaella, D.F.; Lorenzi-Filho, G.; Marie, S.K.N. Effects of yoga breathing exercises on pulmonary function in patients with Duchenne muscular dystrophy: An exploratory analysis. J. Bras. Pneumol. 2014, 40, 128–133. [Google Scholar] [CrossRef] [Green Version]
- Maltais, F. Glossopharyngeal breathing. Am. J. Respir. Crit. Care Med. 2011, 184, 381. [Google Scholar] [CrossRef] [PubMed]
- Marques, T.B.C.; Neves, J.d.C.; Portes, L.A.; Salge, J.M.; Zanoteli, E.; Reed, U.C. Air stacking: Effects on pulmonary function in patients with spinal muscular atrophy and in patients with congenital muscular dystrophy. J. Bras. Pneumol. 2014, 40, 528–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagevik Olsén, M.; Lannefors, L.; Westerdahl, E. Positive expiratory pressure-Common clinical applications and physiological effects. Respir. Med. 2015, 109, 297–307. [Google Scholar] [CrossRef] [Green Version]
- Birnkrant, D.J.; Bushby, K.; Bann, C.M.; Alman, B.A.; Apkon, S.D.; Blackwell, A.; Case, L.E.; Cripe, L.; Hadjiyannakis, S.; Olson, A.K.; et al. Diagnosis and management of Duchenne muscular dystrophy, part 2: Respiratory, cardiac, bone health, and orthopaedic management. Lancet Neurol. 2018, 17, 347–361. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Ambulatory Status VS | N = 45 (%) | Upper Limb Functional Status BS | N = 45 (%) |
|---|---|---|---|
| Walks and climbs stairs without assistance. | 9 (20) | Can abduct the arms in a full circle until they touch above the head. | 25 (55.5) |
| Walks and climbs stairs with railing or assistance. | 12 (26.7) | Can raise arms above head only by flexing the elbow. | 12 (26.7) |
| Walks and climbs stairs slowly with aid or railing (more than 25 s for 8 steps). | 4 (8.9) | Cannot raise hands above head, but can raise a glass of water to the mouth. | 3 (6.7) |
| Walks unassisted, rises from chair, cannot climb stairs. | 2 (4.4) | Cannot raise hands to the mouth but can use hands to hold a pen or pick up coins from the table. | 3 (6.7) |
| Uses a wheelchair. | 18 (40) | Cannot raise hands to the mouth and has no useful function of hands. | 2 (4.4) |
| Able to Perform 3 Times Daily | Able to Perform 1–2 Times Daily | Able to Perform a Few Times a Week | Not Able to Perform | p Value * | |
|---|---|---|---|---|---|
| N = 45 | 18 | 12 | 14 | 1 | |
| Mean age (SD) | 12.83 (5.9) | 11.83 (5.52) | 8.25 (4.89) | 4 | 0.08 |
| Median VS (IQR) | 3 (8.0) | 6 (7.0) | 2 (2.0) | 2 | 0.51 |
| Median BS (IQR) | 1 (2.0) | 2 (1.0) | 1 (1.0) | 2 | 0.39 |
| Able to Perform All Exercises | Able to Perform after Practicing | Able to Perform after Modifications | Not Able to Perform | p Value * | |
|---|---|---|---|---|---|
| N = 45 | 5 | 22 | 16 | 2 | |
| Mean age (SD) | 12.83 (5.9) | 11.83 (5.52) | 8.25 (4.89) | 4 | 0.50 |
| Median VS (IQR) | 3 (1) | 2.5 (7) | 2.5 (7) | 1.5 (1) | 0.59 |
| Median BS (IQR) | 1 (0) | 1 (1) | 2 (1) | 1 (0) | 0.30 |
| Satisfaction | Appropriateness | Intelligibility | |
|---|---|---|---|
| Number of participants | 4 | 6 | 1 |
| Mean age (SD) | 7.25 (4.97) | 7.66 (4.40) | 21.0 |
| Median VS (IQR) | 2.5 (4.0) | 3.0 (1.0) | 9.0 |
| Median BS (IQR) | 1.0 (0.0) | 1.0 (0.0) | 1.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sobierajska-Rek, A.; Mański, Ł.; Jabłońska-Brudło, J.; Śledzińska, K.; Wasilewska, E.; Szalewska, D. Respiratory Telerehabilitation of Boys and Young Men with Duchenne Muscular Dystrophy in the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 6179. https://doi.org/10.3390/ijerph18126179
Sobierajska-Rek A, Mański Ł, Jabłońska-Brudło J, Śledzińska K, Wasilewska E, Szalewska D. Respiratory Telerehabilitation of Boys and Young Men with Duchenne Muscular Dystrophy in the COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(12):6179. https://doi.org/10.3390/ijerph18126179
Chicago/Turabian StyleSobierajska-Rek, Agnieszka, Łukasz Mański, Joanna Jabłońska-Brudło, Karolina Śledzińska, Eliza Wasilewska, and Dominika Szalewska. 2021. "Respiratory Telerehabilitation of Boys and Young Men with Duchenne Muscular Dystrophy in the COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 12: 6179. https://doi.org/10.3390/ijerph18126179