1. Introduction
Although many years have passed since the discovery of the HIV/AIDS disease, it still represents a significant global problem [
1,
2]. At the end of 2018, approximately 37.9 million people worldwide were infected with HIV. Despite the worldwide availability of testing, 21% of all HIV+ patients are not aware of their condition [
3]. The Czech Republic counts among countries with a relatively low incidence of this disease; nevertheless, it belongs, at the same time, to the list of countries with a rapid increase in the number of new cases of HIV infection over the last few years [
4,
5]. The number of new cases has grown approximately three times from 1186 in 2008 to 3368 in 2018 [
6]. HIV infection remains, despite significant advancements in treatment, an incurable disease, which is not preventable by vaccination. Hence, primary prevention of HIV infection plays an important role and, at the same time, remains the most effective and most economical preventive measure. Raising awareness among the youth, general public, and specific populations with a high risk of infection using training and education about sexually transmitted diseases (hereinafter referred to as STDs), including HIV/AIDS, is the cornerstone of primary prevention measures [
7,
8,
9,
10,
11].
In addition to the education of pupils and students of primary and secondary schools, educational events, peer programmes, and lectures with an HIV+ lecturer, primary HIV/AIDS prevention also includes services of AIDS counselling, contact centres, and exchange of used injection needles as a part of the harm reduction programme [
12,
13,
14,
15]. In the area of raising awareness and education, it is necessary to apply preventive measures especially towards the youth (in particular, in the areas of prevention of disease transmission, risk behaviour, and promotion of safe sex); it is also important to motivate and encourage responsibility for one’s acts, using condoms, and healthy behaviour [
16].
The Public Health Institute in Ostrava has implemented educational events for schools, including the interactive programme Playfully about STDs (PaSTDs), the aim of which is to raise awareness about the possibilities of preventing the transmission of the HIV virus and other sexually transmitted diseases in young people, and to support the development of responsible and desirable behaviour in the area of STD prevention, including HIV, and, thus, to reduce risky behaviour [
17,
18].
The aim of the study is to present students’ knowledge of HIV/AIDS and the effectiveness of the PaSTDs educational programme in raising awareness and knowledge regarding prevention of HIV and STDs in adolescents. The basic hypothesis is that this programme represents an effective tool of primary prevention and that after its completion, the participants’ knowledge about the problems of HIV and STDs increases.
2. Materials and Methods
2.1. Design
An educational programme aimed at the prevention of HIV and STDs in adolescents between 13 and 19 years of age is underway in the Moravian-Silesian Region in the Czech Republic. All grammar and secondary schools (a total of 457 schools) in the region have been offered the possibility to take part in the programme; their participation was voluntary. Over 2 years (2018–2019), students from 31 schools in the Moravian-Silesian Region, Czech Republic, participated in the programme. A total of 1264 students aged 13 to 19 present on the day of the educational programme at the school participated in the programme.
The programme consists of an educational lecture (two lessons) and a game with interactive elements, during which the pupils from each class are divided into 4 groups and perform 8 tasks with various educational tools (magnetic board and magnetic cards, samples of contraception methods, models of penis for training of condom handling), for which they receive points in the form of special “bouncing balls” [
17]. A more detailed description of the course of the programme can be found in
Appendix A.
2.2. Measures
An anonymous paired questionnaire (input/output) was used to assess the efficacy of the programme. The input questionnaire, with a unique ID, was distributed among the students prior to commencement of the educational programme; this questionnaire served as the baseline evaluation of participants’ knowledge about the problems of HIV before education. The questionnaire contains 12 questions, beginning with the data about the participant—sex and age. The student subsequently answers 10 test questions on sexually transmitted diseases, choosing from multiple-choice options (the answer “I don’t know” is always one of the options). After education, the students filled in the output questionnaire with the same ID and with questions identical to those in the input questionnaire, supplemented with the possibility to evaluate the programme on a scale from 1 to 5 and to add an open comment.
The questionnaire used in this study was based on the one published in our previous pilot study about the educational programme [
17]. In addition, two questions (8, 9, see
Appendix A) in the questionnaire were changed during data collection.
2.3. Data and Variables
A total of 1264 students participated in the preventive programme; 54 students were excluded from the analysed sample due to incomplete/incorrect filling of the questionnaires (e.g., ticking multiple options in single-choice questions or using ambiguous indicators). The questionnaire was also excluded from analysis if the pair (input and output part of the questionnaire) was incomplete. The final sample consists of 1210 students.
Data about sex, age (age groups 13–14 years, 15–16 years, 17 and older) and the type of school—a grammar school (GS), a secondary school (SS), or a lower secondary school (LSS)—were collected. Test questions were awarded one point for each correct answer. The maximum was 22 points. The total score was expressed as a percentage of the maximum. The two questions that were changed over the course of data collection (questions 8, 9—
Appendix A) were excluded from the total score. The total score was calculated separately for the input and output questionnaire. Students’ evaluation of the programme quality was on a scale from 1 (the best) to 5 (the worst).
EpiData Software was used for the electronisation of the data from paper questionnaires.
2.4. Data Analysis
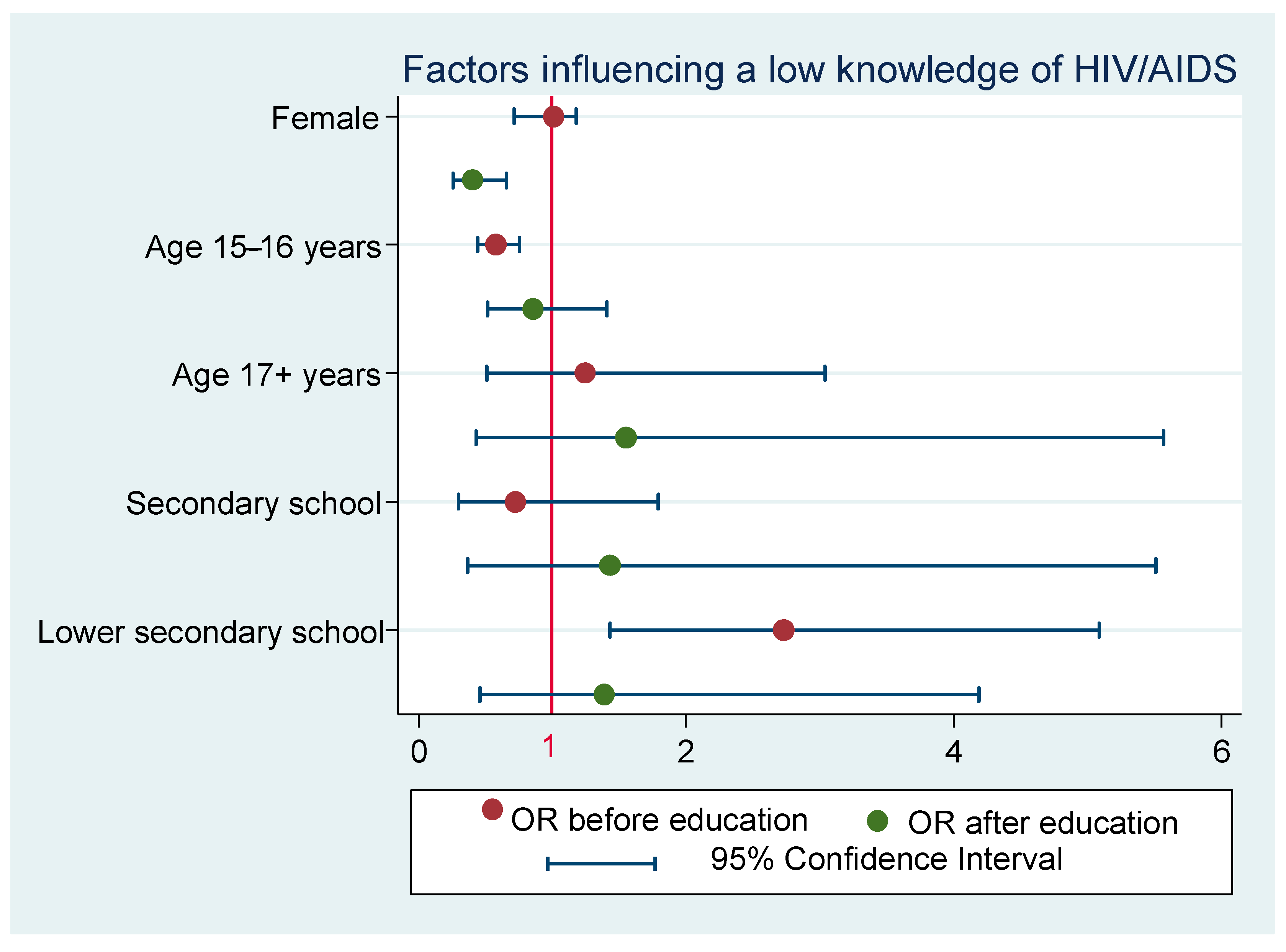
Descriptive statistics was used for the basic presentation of the results. The changes in the proportions of correct answers in each of the test questions were evaluated via the McNemar test. The non-parametric Wilcoxon paired test was used to test the changes in the total score (before and after education). The power of the mean difference between total scores before and after education was calculated based on a one-sample mean test for a one-sided alternative hypothesis (Ha: mean difference > 0). The comparison of the total score by sex, age, and school type was performed using Mann–Whitney and Kruskal–Wallis tests. A model of logistic regression for dichotomous variables was used to evaluate the most significant factors affecting the participants’ knowledge. Low knowledge was defined as a total score of less than 70%. The basic (reference) categories were set as: men (for the sex variable), the youngest students (13–14 years; age variable), and grammar school (the type of school). The results were expressed as odds ratio (OR) with standard error (SE) and 95% confidence interval (CI). Statistical tests were evaluated at the 5% significance level. The Stata software, version 14, was used to analyse the data.
2.5. Ethical Considerations
The study was approved by the Ethics Committee of the Faculty of Medicine of the University of Ostrava on the basis of the EC Consent Opinion No. 04/2020.
4. Discussion
In addition to the PaSTDs programme, there is also another project in the Czech Republic educating young people and forming their attitudes in the field of HIV/AIDS prevention. This project is organised by the National Institute of Public Health under the name “Playing Against AIDS”. In this project, all information regarding HIV is presented to students only by means of oral presentations using available tools, and the programme does not include any educational “hands-on” presentation. Participants work in five individual groups, and the significant gaming character is missing. Each group of participants has their own lecturer, and the programme is more personally demanding when compared with the PaSTDs project, requiring only one lecturer for the whole intervention. The PaSTDs project uses an educational game to present the subject and input and output questionnaires to determine the effectiveness of the programme. Nevertheless, based on available sources, both programmes are of high quality, effective, and positively evaluated [
19]. The educational information of PaSTDs was evaluated positively by the students; their interest in the HIV issue manifested especially through the increase in awareness about this problem by more than 15%.
The knowledge level increased in a vast majority of the 1210 participants; therefore, we can consider the programme effective. The programme was most effective in the youngest age group of 13–14-year-olds, where the improvement in the knowledge level was almost 18%. This is most probably caused by the fact that the youngest participants do not have much information and experience yet (as corroborated by their lowest initial result); this result may have also been due to the gaming/competitive character of the programme, which seems to be more attractive to younger participants. The average improvement observed in the 15–16-year-olds was 13.66%. Compared to that, the oldest age group of 17–19-year-olds achieved an average improvement of a mere 8.1%, which is most likely due to the already high level of knowledge the students had before completing the programme. The highest increase in the knowledge level was observed, in particular, in the most important questions, such as what HIV is, whether there is a vaccination against HIV, or whether hormonal contraception provides protection against HIV infection. It is also possible to evaluate the knowledge with respect to sex, which shows that compared to boys, girls not only performed better before the education, but the increase in their knowledge was also higher.
Although most educational programmes dealing with the problem of HIV/AIDS infection and other STDs are primarily aimed at children and youth, these interventions are also important for other population groups. For example, a positive influence of the intervention has been previously confirmed among drug users [
20]. Educational programmes and their implementation play an important role in increasing knowledge and awareness about HIV/AIDS. Although HIV/AIDS infection is not going to disappear completely as a result of these programmes, they may help to reduce the number of new cases of these infections; it is, therefore, appropriate to continue with such programmes, to develop them further and adjust them to the ever-changing requirements [
16].
The positive effect of educational programmes is also supported by a meta-analysis summarising 83 studies from various countries (developed as well as developing), aiming at sex education and the prevention of HIV and other sexually transmitted diseases. The results of the analysis show a positive impact of educational programmes in this area on the behaviour of the adolescent population [
21].
Current findings show that these interventions are effective worldwide. According to a systematic review examining the effect of interventions on the prevention of unwanted pregnancy from 2016, multiple interventions combining education and promotion of contraceptive methods significantly reduce the risk of unintentional pregnancy in adolescents. The review further revealed that educational interventions alone will most probably not result in postponing the beginning of sexual life in adolescents; however, the frequency of condom use increases significantly when compared to individuals who have not been through such an intervention [
22]. This is also why our programme emphasises the importance of using a condom as well and why it also contains a practical demonstration of its use. Another part of the programme is a demonstration of other contraceptive methods, including hormonal contraception, for which it is always clearly emphasised that they provide protection only against unwanted pregnancy but not against HIV and STDs.
This may also be the reason preventive programmes encouraging only sexual abstinence have been lately criticised as ineffective and, in addition, principally not promoting the strategy of safer sex in the sense of STDs prevention (use of condoms) and protection against unwanted pregnancy (use of condoms and other methods of contraception). This criticism is also supported by the findings of a previous study on the effectiveness of interventions aimed solely at sexual abstinence as prevention of HIV infection, which concluded that such programmes are ineffective. The results did not show that these programmes reduce the risk of HIV infection; moreover, these programmes failed to influence the incidence of unprotected vaginal sex, frequency of vaginal sex, number of partners, sexual initiation, or use of condoms [
23].
Thus, it is clearly apparent that it is more effective to lead adolescents towards responsible sexual behaviour than trying to force them into sexual abstinence as the only means of prevention. This is also indicated by the meta-analysis published in 2011, which concentrated directly on interventions intended to reduce the sexual risks of HIV infection in adolescents. A total of 98 interventions from 67 studies were included in this meta-analysis; these were completed in total by 51,240 adolescents aged 11–19 years. The findings show that the incidence of sexually transmitted diseases decreased among those who completed the education when compared with controls; additional results included more frequent use of condoms, delaying sexual intercourse or decreasing its frequency, and upgrading the skills required for applying the principles of safe sex and obtaining prophylactic protection [
24].
Another study performed in Tanzania investigated the degree to which education based on games and gamification (i.e., using gaming elements and principles in education) could improve the education of adolescent students on sexual health when compared with the traditional style of education. A total of 120 students from secondary schools took part in the programme. The average score after completing the test for education based on games and gamification, which reached 79% in both these educational methods, was significantly higher than in the control group, where it reached only 51%. This study suggests that the investigated innovative approaches to education may improve education on sexual health in the adolescent population. These methods may potentially contribute, in particular, to improving behaviour in the area of sexual health and increasing the knowledge of adolescents, especially in contexts where discussions concerning sexual problems present a taboo [
25]. This is also why involving gaming elements is used in our programme—the intention is to increase the attractiveness of the programme and to eliminate possible shame and shyness in the participants.
Should we consider the generalisability of the results, it is likely that a similar effect in the form of improving the participants’ knowledge could also be observed in the target age group of 13–19-year-olds in other regions of the Czech Republic. Possible use of the programme in other countries clearly depends on the contents of the educational programmes at schools in individual countries, especially the inclusion of subjects similar to the Health Education subject taught in the Czech Republic. However, this subject is taught at schools for one year only and, considering the answers to some questions in the questionnaire, it is possible to claim that the problems of HIV and STDs are not given sufficient attention in the course of standard school education. Similar findings were also observed in the questionnaire survey performed by the National Institute of Public Health in 2015, which revealed that adolescents are not sufficiently educated in this area and that more attention needs to be paid to these topics in the future [
26]. According to another study from 2014, school educational programmes about HIV/AIDs are an important and effective means of influencing the knowledge, attitudes, and behaviour of young people regarding health issues related to sex. The study showed that educational programmes about HIV/AIDS at schools may effectively reduce the risky behaviour of young people. The authors also propose that education in the area of HIV/AIDS prevention should ideally start before puberty, or, at the latest, before the first sexual intercourse [
15]. We also tend to support this conclusion, considering the highest effectiveness observed in the youngest age group of our programme.
The PaSTDs programme should be based on the principle of double transmission of information—the first time during the educational lecture, and the second time during the game. In addition, the effectiveness is also supported by the initial questionnaire before the programme as students who did not know answers to individual test questions were more likely to extract the answers from the given lecture.
Limitations: The greatest limitation of this programme may be the fact that it represents a one-off intervention only and there is no further monitoring, for example, of the length of knowledge persistence, or of possible effects on the future risky behaviour of the participants. However, these drawbacks are mainly caused by a lack of financial means invested in the area of prevention and, in our case, also the limited staffing of the programme. The first and greatest obstacle in the implementation of the programme was the lack of interest in the programme at some schools. We propose performing a repeated intervention in the already educated pupils in order to discover whether the knowledge persists on a long-term basis. The programme is currently interrupted due to the complete closure of schools in the Czech Republic caused by the coronavirus pandemic; nevertheless, we expect it to continue when the situation permits.
5. Conclusions
Taking into consideration the presented results, it is possible to conclude that the programme leads to increased knowledge in the participants and, as such, can be considered an effective tool of primary prevention in the sense of increasing awareness about the problem of HIV and STDs by 15.5% on average (from 74.0% to 89.5%).
The programme was observed to be more effective in lower age categories (the score in the age group of 13–14-year-olds improved by 17.92%). Evaluation of knowledge according to sex (M/F) shows that girls achieved a higher success rate of answers before education and, at the same time, manifested a higher increase in knowledge after education than boys.
The participating students showed great sympathy with the educational programme; their interest in this problem corresponds to a significant increase in knowledge observed especially among the youngest participants. This is also why we propose to focus further interventions, in particular, on this youngest age group of 13–14-year-olds.


 ,
, 
{kind=link}
