
Dimensions of Community Assets for Health. A Systematised Review and Meta-Synthesis

 , ,
, ,  ,
,  and
and 
Abstract
:1. Introduction
Review Question
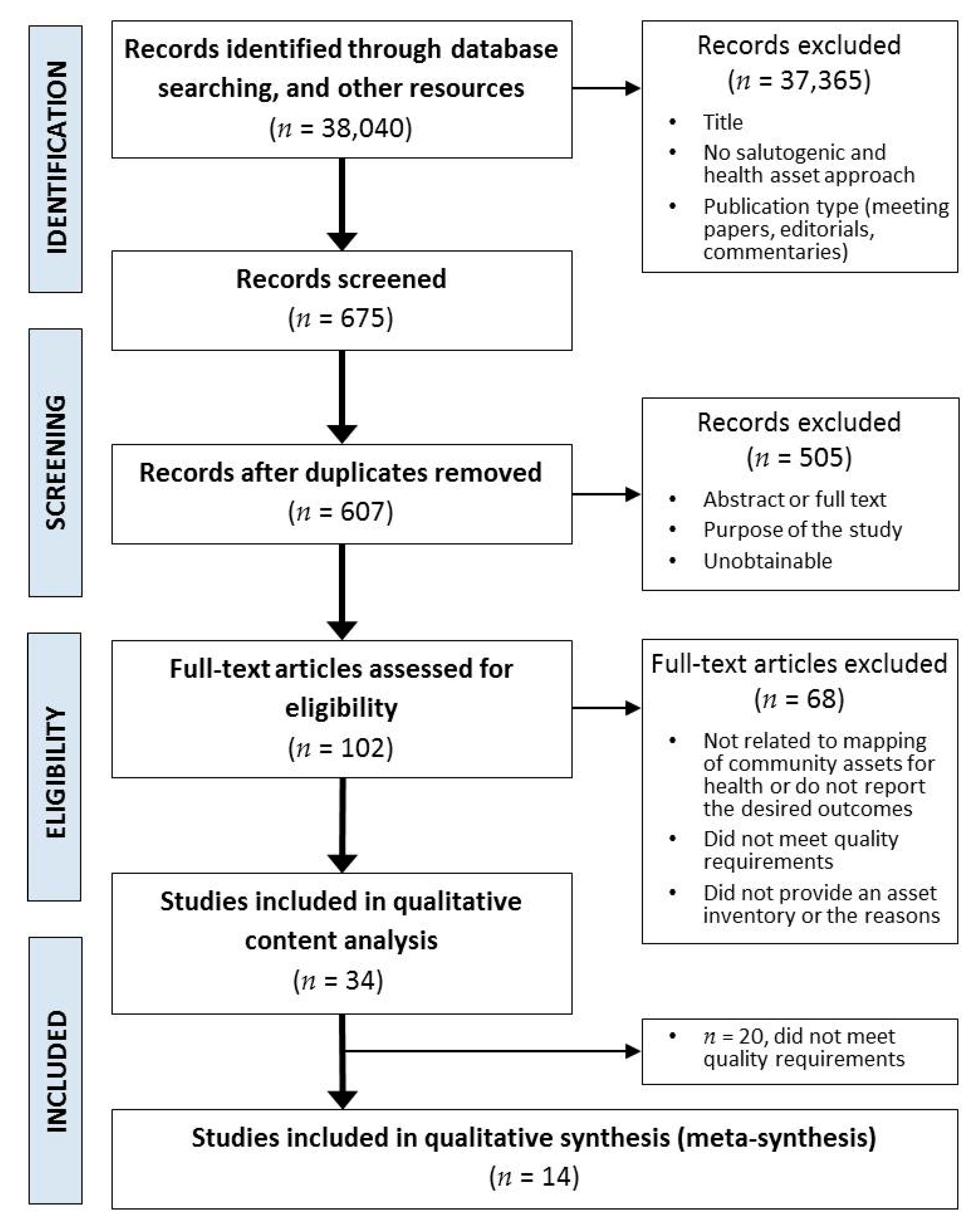
2. Materials and Methods
2.1. Procedure and Framework
2.2. Search Strategy
2.3. Eligibility Criteria
2.3.1. Theoretical Approach or Framework
2.3.2. Types of Study Design
2.3.3. Types of Outcome
2.4. Information Sources
- -
- Web of Science
- -
- Scopus
- -
- MEDLINE (via PubMed)
- -
- EBSCO host
- -
- Cochrane Public Health
- -
- Dialnet
- -
- SciELO
Other Sources
2.5. Selection of Sources of Evidence
- (1)
- Publication information (title, author and date of publication, local place and country);
- (2)
- Study characteristics (design, theoretical and methodological approach, population of interest, objectives of the studies);
- (3)
- Health asset characteristics: type of resources (personal, inter-personal and community assets) and dimensions or factors that defined the assets identified.
2.6. Quality Appraisal of Included Studies
2.7. Synthesis, Content Analysis and Categorisation
3. Results
3.1. Study Characteristics of Included Studies
3.2. “Universal” Characteristics of Community Assets for Health
3.2.1. Utility
3.2.2. Intention
“[…] Among the identifed internal assets were well-being, happiness, a positive attitude towards health, self-confdence, acceptance, respect, self-esteem and the ability to handle difculties and challenges” [42] (p. 258)
3.2.3. Previous Use
3.2.4. Accesibility (Perceived): Affordability, Proximity, Walkability, Connectivity and Legibility
“[…] the long distance, as well as a lack of information are the primary reasons why some societies are excluded from getting access to health services” [62] (p. 6).
“[…] Transport and connectivity was a dimension that the professionals considered health enhancing. The professionals regarded the traffic infrastructure”[29] (p. 7)
“Lack of accessible and reliable public transportation may increase the need for financial resources, to have extra time or having to roll long distances to get to the asset of interest”[73] (p. 7).
“Poor transport and communication infrastructure in many rural communities are noted to exclude many from having adequate access to healthcare”[62] (p. 6).
“Accessible information and resources shared between organisations in the community […] Available in print and on line”[34] (p. 311)
“[…] large food purchases were sometimes made at supermarkets outside of town to access a wider range of foods at potentially lower prices”[75] (p. 3).
3.2.5. Identity
3.2.6. Design
3.2.7. Safety (Perceived and Objective)
“Safety concerns ranged from environmental hazards and limitations of the physical environment (e.g., few parks and green areas; poor maintenance of existing parks) to neighborhood threats (e.g., thefts, gangs, vandalism) and domestic violence.”[91] (p. 5).
“[…] adolescents felt afraid to use those green spaces because ofthe presence of gang activity and drug sales. Youth expressed the need for more safe recreation facilities that are appropriate for adolescents and equipped…”[76] (p. 8).
3.2.8. Diversity
3.2.9. Public
3.2.10. Sustainability
“[…] the capacity of a system to maintain structure and function when faced with shocks and change” “[…] resilience-building in social-ecological systems are structured scenarios and active adaptive management”[95] (p. 49).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Antonovsky, A. Health, Stress, and Coping. New Perspectives on Mental and Physical Well-Being, 3rd ed.; Jossey-Bass Publishers: San Francisco, CA, USA, 1979. [Google Scholar]
- Antonovsky, A. Unraveling the Mystery of Health: How People Manage Stress and Stay Well; Jossey-Bass Publishers: San Francisco, CA, USA, 2012. [Google Scholar]
- Kretzmann, J.P.; McKnight, J.L. Building Communities from the Inside Out: A Path toward Finding and Mobilizing a Community’s Assets; School of Education and Social Policy Northwestern University: Evanston, IL, USA, 1993. [Google Scholar]
- Eriksson, M.; Lindström, B. Bringing it all together: The salutogenic response to some of the most pertinent public health dilemmas. In Health Assets in a Global Context: Theory, Methods, Action; Morgan, A., Favies, M., Ziglio, E., Eds.; Springer: New York, NY, USA, 2010; Chapter 18; pp. 339–351. [Google Scholar] [CrossRef]
- Morgan, A.; Ziglio, E. Revitalising the evidence base for public health: An assets model. Promot. Educ. 2007, 14, 17–22. [Google Scholar] [CrossRef]
- Scales, P.C.; Leffert, N. Developmental Assets: A Synthesis of the Scientific Research on Adolescent Development, 2nd ed.; Search Institute: Minneapolis, MN, USA, 1999; 281p, ISBN 1-57482-338-8. [Google Scholar]
- Antonovsky, A. The salutogenic model as a theory to guide health promotion. Health Promot. Int. 1996, 11, 11–18. [Google Scholar] [CrossRef]
- Mittelmark, M.B.; Sagy, S.; Eriksson, M.; Bauer, G.F.; Pelikan, J.M.; Lindström, B.; Espnes, G.A. The Handbook of Salutogenesis; Springer: Cham, Switzerland, 2017; p. 461. Available online: https://www.ncbi.nlm.nih.gov/books/NBK435831/ (accessed on 20 March 2018).
- Rotegård, A.K.; Moore, S.M.; Fagermoen, M.S.; Ruland, C.M. Health assets: A concept analysis. Int. J. Nurs. Stud. 2010, 47, 513–525. [Google Scholar] [CrossRef] [Green Version]
- Aviñó Juan-Ulpiano, A.R. Mapeo de Activos en Salud en dos Barrios Vulnerables y su Dinamización en una Intervención Comunitaria Participativa. Ph.D. Thesis, Universidad de Valencia, Valencia, Spain, 2017. Available online: http://roderic.uv.es/handle/10550/60804 (accessed on 2 April 2018).
- Jakes, S.; Hardison-Moody, A.; Bowen, S.; Blevins, J. Engaging community change: The critical role of values in asset mapping. Community Dev. 2015, 46, 392–406. [Google Scholar] [CrossRef]
- Glasgow Centre for Population Health. Putting Asset Based Approaches into Action: Identification, Mobilisation and Meas-urement of Assets; Briefing Paper Concept Series 10; Glasgow Centre for Population Health: Glasgow, UK, 2012; pp. 2–24. [Google Scholar]
- Stokols, D.; Grzywacz, J.G.; McMahan, S.; Phillips, K. Increasing the Health Promotive Capacity of Human Environments. Am. J. Health Promot. 2003, 18, 4–13. [Google Scholar] [CrossRef] [Green Version]
- Kramer, S.; Amos, T.; Lazarus, S.; Seedat, M. The Philosophical Assumptions, Utility and Challenges of Asset Mapping Approaches to Community Engagement. J. Psychol. Afr. 2012, 22, 537–544. [Google Scholar] [CrossRef]
- Antonovsky, A. Complexity, conflict, chaos, coherence, coercion and civility. Soc. Sci. Med. 1993, 37, 969–974. [Google Scholar] [CrossRef]
- Lazarus, S. Does the Positive Psychology Movement Have Legs? Psychol. Inq. 2009, 14, 93–109. [Google Scholar] [CrossRef]
- Lindström, B.; Eriksson, M. Guía del Autoestopista Salutogénico. Camino Salutogénico Hacia la Promoción de la Salud; Càtedra de Promoció de la Salut de la Universitat de Girona: Girona, Spain, 2011. [Google Scholar] [CrossRef]
- van Kamp, I.; Leidelmeijer, K.; Marsman, G.; de Hollander, A. Urban environmental quality and human well-being. Landsc. Urban Plan. 2003, 65, 5–18. [Google Scholar] [CrossRef]
- Friedli, L. ‘What we’ve tried, hasn’t worked’: The politics of assets based public health1. Crit. Public Health 2013, 23, 131–145. [Google Scholar] [CrossRef]
- Foot, J. What Makes Us Healthy? The Asset Approach in Practice: Evidence, Action, Evaluation. 2012. Available online: http://www.janefoot.co.uk (accessed on 13 March 2020).
- Booth, A. Clear and present questions: Formulating questions for evidence based practice. Libr. Hi Tech 2006, 24, 355–368. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [Green Version]
- Stige, B.; Malterud, K.; Midtgarden, T. Toward an agenda for evaluation of qualitative research. Qual. Health Res. 2009, 19, 1504–1516. [Google Scholar] [CrossRef]
- O’Connor, J.P.; Alfrey, L.; Hall, C.; Burke, G. Intergenerational understandings of personal, social and community assets for health. Health Place 2019, 57, 218–227. [Google Scholar] [CrossRef] [PubMed]
- Mosavel, M.; Gough, M.Z.; Ferrell, D. Using Asset Mapping to Engage Youth in Community-Based Participatory Research: The WE Project. Prog. Community Health Partnersh. Res. Educ. Action 2018, 12, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Casado, L.; Paredes-carbonell, J.J.; López-Sánchez, P.; Morgan, A. Mapa de Activos para la Salud y la Convivencia. Propuestas de Acción Desde la Intersectorialidad. Index Enferm. 2017, 26, 1–12. [Google Scholar]
- Broeder, L.D.; Uiters, E.; Hofland, A.; Wagemakers, A.; Schuit, A.J. Local professionals’ perceptions of health assets in a low-SES Dutch neighbourhood: A qualitative study. BMC Public Health 2018, 18, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Florian, J.; Roy, N.M.S.O.; Quintiliani, L.M.; Truong, V.; Feng, Y.; Bloch, P.P.; Russinova, Z.L.; Lasser, K.E. Using Photovoice and Asset Mapping to Inform a Community-Based Diabetes Intervention, Boston, Massachusetts, 2015. Prev. Chronic Dis. 2016, 13, E107. [Google Scholar] [CrossRef] [Green Version]
- Cutts, T.; Langdon, S.; Meza, F.R.; Hochwalt, B.; Pichardo-Geisinger, R.; Sowell, B.; Chapman, J.; Dorton, L.B.; Kennett, B.; Jones, M.T. Community Health Asset Mapping Partnership Engages Hispanic/Latino Health Seekers and Providers. North Carol. Med. J. 2016, 77, 160–167. [Google Scholar] [CrossRef] [Green Version]
- Jabeen, H. Adapting the assets of urban low-income households with climate extremes: Experience from Dhaka. Int. J. Urban Sustain. Dev. 2014, 7, 72–88. [Google Scholar] [CrossRef]
- Pérez-Wilson, P.; Hernán, M.; Morgan, A.R.; Mena, A. Health assets for adolescents: Opinions from a neighbourhood in Spain. Health Promot. Int. 2015, 30, 552–562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthiesen, M.; Froggatt, K.; Owen, E.; Ashton, J.R. End-of-life conversations and care: An asset-based model for community engagement. BMJ Support. Palliat. Care 2014, 4, 306–312. [Google Scholar] [CrossRef]
- DyckFehderau, D.; Holt, N.L.; Ball, G.D.; Willows, N.D. Feasibility study of asset mapping with children: Identifying how the community environment shapes activity and food choices in Alexander First Nation. Rural. Remote. Health 2013, 13, 1–11. [Google Scholar]
- Greetham, J.; Charkin, D.; Laird, H.; Butterell, D. Growing Communities from the Inside out. Piloting an Asset Based Approach to JSNAs within the Wakefield District: Methods and Findings. NHS Wakefield District. 2012. Available online: https://saludcomunitaria.files.wordpress.com/2014/05/growing-communities-from-the-inside-out-jsnas-in-the-wakefield-district.pdf (accessed on 23 March 2018).
- Lazarus, S.; Naidoo, T.; Demas, G.; Williams, L.; Sauls, D.; Filander, F.; Reagan, K.; Annuske, K.; Searle, K.; Jamie-Lee, M.; et al. Railton Community Assessment Project: Research Report; Universidad de Stellenbosch: Railton, South Africa, 2010; Available online: https://scholar.sun.ac.za/handle/10019.1/19361 (accessed on 10 April 2018).
- Maslow, A.H. A theory of human motivation. Psychol. Rev. 1943, 370–396. [Google Scholar] [CrossRef] [Green Version]
- Nase, I.; Berry, J.; Adair, A. Urban design quality and real estate value: In search of a methodological framework. J. Urban Des. 2015, 20, 563–581. [Google Scholar] [CrossRef]
- Collins, S.E.; Witkiewitz, K.; Larimer, M.E. The Theory of Planned Behavior as a Predictor of Growth in Risky College Drinking. J. Stud. Alcohol Drugs 2011, 72, 322–332. [Google Scholar] [CrossRef] [Green Version]
- Wang, D.; Brown, G.; Liu, Y.; Mateo-Babiano, I. A comparison of perceived and geographic access to predict urban park use. Cities 2015, 42, 85–96. [Google Scholar] [CrossRef]
- Soriano-Ayala, E.; Cala, V.C.; Ruiz-Salvador, D. Identification of Cultural and Transcultural Health Assets among Moroccan, Romanian and Spanish Adolescents through Photovoice. J. Immigr. Minor. Health 2019, 22, 255–265. [Google Scholar] [CrossRef]
- Perugini, M.; Bagozzi, R.P. The role of desires and anticipated emotions in goal-directed behaviours: Broadening and deepening the theory of planned behaviour. Br. J. Soc. Psychol. 2001, 40, 79–98. [Google Scholar] [CrossRef] [PubMed]
- Lam, T.; Hsu, C.H.C. Theory of Planned Behavior: Potential Travelers from China. J. Hosp. Tour. Res. 2004, 28, 463–482. [Google Scholar] [CrossRef]
- Park, K. Psychological park accessibility: A systematic literature review of perceptual components affecting park use. Landsc. Res. 2016, 42, 508–520. [Google Scholar] [CrossRef]
- Pirie, G.H. Measuring Accessibility: A Review and Proposal. Environ. Plan. A Econ. Space 1979, 11, 299–312. [Google Scholar] [CrossRef]
- Wu, Y.; Miller, H.J. Computational Tools for Measuring Space-Time Accessibility within Dynamic Flow Transportation Networks. J. Transp. Stat. 2001, 4, 1–14. [Google Scholar]
- Macdonald, L.; Kearns, A.; Ellaway, A. Do residents’ perceptions of being well-placed and objective presence of local amenities match? A case study in West Central Scotland, UK. BMC Public Health 2013, 13, 454. [Google Scholar] [CrossRef] [Green Version]
- Cerin, E.; Conway, T.L.; Adams, M.A.; Barnett, A.; Cain, K.L.; Owen, N.; Christiansen, L.B.; van Dyck, D.; Mitáš, J.; Sarmiento, O.L.; et al. Objectively-assessed neighbourhood destination accessibility and physical activity in adults from 10 countries: An analysis of moderators and perceptions as mediators. Soc. Sci. Med. 2018, 211, 282–293. [Google Scholar] [CrossRef]
- Szpisjak, D.F.; Lamb, C.L.; Klions, K.D. Oxygen Consumption with Mechanical Ventilation in a Field Anesthesia Machine. Anesth. Analg. 2005, 100, 1713–1717. [Google Scholar] [CrossRef] [Green Version]
- Brondeel, R.; Weill, A.; Thomas, F.; Chaix, B. Use of healthcare services in the residence and workplace neighbourhood: The effect of spatial accessibility to healthcare services. Health Place 2014, 30, 127–133. [Google Scholar] [CrossRef]
- Fleischhacker, S.E.; Evenson, K.R.; Rodriguez, D.A.; Ammerman, A.S. A systematic review of fast food access studies. Obes. Rev. 2010, 12, e460–e471. [Google Scholar] [CrossRef]
- Kerr, J.; Norman, G.J.; Adams, M.A.; Ryan, S.; Frank, L.; Sallis, J.F.; Calfas, K.J.; Patrick, K. Do neighborhood environments moderate the effect of physical activity lifestyle interventions in adults? Health Place 2010, 16, 903–908. [Google Scholar] [CrossRef] [Green Version]
- Markevych, I.; Smith, M.P.; Jochner, S.; Standl, M.; Brüske, I.; Von Berg, A.; Bauer, C.-P.; Fuks, K.; Koletzko, S.; Berdel, D.; et al. Neighbourhood and physical activity in German adolescents: GINIplus and LISAplus. Environ. Res. 2016, 147, 284–293. [Google Scholar] [CrossRef] [PubMed]
- Moudon, A.V.; Lee, C.; Cheadle, A.D.; Garvin, C.; Johnson, D.B.; Schmid, T.L.; Weathers, R.D.; Lin, L. Operational Definitions of Walkable Neighborhood: Theoretical and Empirical Insights. J. Phys. Act. Health 2006, 3, S99–S117. [Google Scholar] [CrossRef]
- Peiravian, F.; Derrible, S.; Ijaz, F. Development and application of the Pedestrian Environment Index (PEI). J. Transp. Geogr. 2014, 39, 73–84. [Google Scholar] [CrossRef]
- Frank, L.D.; Schmid, T.L.; Sallis, J.F.; Chapman, J.; Saelens, B.E. Linking objectively measured physical activity with objectively measured urban form. Am. J. Prev. Med. 2005, 28, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Heerman, W.J.; Mitchell, S.J.; Thompson, J.; Martin, N.C.; Sommer, E.C.; Van Bakergem, M.; Taylor, J.L.; Buchowski, M.S.; Barkin, S.L. Parental perception of built environment characteristics and built environment use among Latino families: A cross-sectional study. BMC Public Health 2016, 16, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kirtland, K.A.; Porter, D.E.; Addy, C.L.; Neet, M.J.; Williams, J.E.; Sharpe, P.A.; Neff, L.J.; Kimsey, C.; Ainsworth, B.E. Environmental measures of physical activity supports. Am. J. Prev. Med. 2003, 24, 323–331. [Google Scholar] [CrossRef]
- Moudon, A.V.; Hess, P.M.; Snyder, M.C.; Stanilov, K. Effects of Site Design on Pedestrian Travel in Mixed-Use, Medium-Density Environments. Transp. Res. Rec. J. Transp. Res. Board 1997, 1578, 48–55. [Google Scholar] [CrossRef]
- Perchoux, C.; Chaix, B.; Brondeel, R.; Kestens, Y. Residential buffer, perceived neighborhood, and individual activity space: New refinements in the definition of exposure areas—The RECORD Cohort Study. Health Place 2016, 40, 116–122. [Google Scholar] [CrossRef]
- Fenny, A.P.; Kusi, A.; Arhinful, D.K.; Asante, F.A. Factors contributing to low uptake and renewal of health insurance: A qualitative study in Ghana. Glob. Health Res. Policy 2016, 1, 18. [Google Scholar] [CrossRef] [Green Version]
- Cutts, B.B.; Darby, K.J.; Boone, C.G.; Brewis, A. City structure, obesity, and environmental justice: An integrated analysis of physical and social barriers to walkable streets and park access. Soc. Sci. Med. 2009, 69, 1314–1322. [Google Scholar] [CrossRef] [PubMed]
- Lu, Y.; Xiao, Y.; Ye, Y. Urban density, diversity and design: Is more always better for walking? A study from Hong Kong. Prev. Med. 2017, 103, S99–S103. [Google Scholar] [CrossRef]
- Talavera-Garcia, R.; Valenzuela-Montes, L.M. Aproximación a los entornos peatonales a través de una encuesta a la población: Aplicación a la ciudad de Granada. An. Geogr. Univ. Complut. 2018, 38, 239–262. [Google Scholar] [CrossRef]
- Gehl, J. Cities for People; Island Press: Washington, DC, USA, 2010; ISBN 978-1597265737. [Google Scholar]
- Frank, L.D.; Sallis, J.F.; Saelens, B.E.; Leary, L.; Cain, K.; Conway, T.L.; Hess, P.M. The development of a walkability index: Application to the Neighborhood Quality of Life Study. Br. J. Sports Med. 2010, 44, 924–933. [Google Scholar] [CrossRef]
- Millward, H.; Spinney, J.; Scott, D. Active-transport walking behavior: Destinations, durations, distances. J. Transp. Geogr. 2013, 28, 101–110. [Google Scholar] [CrossRef]
- Badland, H.; Whitzman, C.; Lowe, M.; Davern, M.; Aye, L.; Butterworth, I.; Hes, D.; Giles-Corti, B. Urban liveability: Emerging lessons from Australia for exploring the potential for indicators to measure the social determinants of health. Soc. Sci. Med. 2014, 111, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Kytta, M.; Broberg, A.; Tzoulas, T.; Snabb, K. Towards contextually sensitive urban densification: Location-based softGIS knowledge revealing perceived residential environmental quality. Landsc. Urban Plan. 2013, 113, 30–46. [Google Scholar] [CrossRef]
- Kamphuis, C.B.; MacKenbach, J.P.; Giskes, K.; Huisman, M.; Brug, J.; Van Lenthe, F.J. Why do poor people perceive poor neighbourhoods? The role of objective neighbourhood features and psychosocial factors. Health Place 2010, 16, 744–754. [Google Scholar] [CrossRef] [PubMed]
- Walker, R.E.; Keane, C.R.; Burke, J.G. Disparities and access to healthy food in the United States: A review of food deserts literature. Health Place 2010, 16, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Toro-Hernandez, M.L.; Villa-Torres, L.; Mondragón-Barrera, M.A.; Camelo-Castillo, W. Factors that influence the use of community assets by people with physical disabilities: Results of participatory mapping in Envigado, Colombia. BMC Public Health 2020, 20, 1–11. [Google Scholar] [CrossRef]
- Shanks, T.R.W.; Boddie, S.C.; Rice, S. Family-Centered, Community-Based Asset Building: A Strategic Use of Individual Development Accounts. J. Community Pract. 2010, 18, 94–117. [Google Scholar] [CrossRef]
- Seguin, R.A.; Morgan, E.H.; Connor, L.M.; Garner, J.A.; King, A.C.; Sheats, J.L.; Winter, S.J.; Buman, M. Rural Food and Physical Activity Assessment Using an Electronic Tablet-Based Application, New York, 2013–2014. Prev. Chronic Dis. 2015, 12, E102. [Google Scholar] [CrossRef] [Green Version]
- Cubilla-Batista, I.; Andrade, E.L.; Cleary, S.D.; Edberg, M.C.; Evans, W.D.; Simmons, L.K.; Sojo-Lara, G. Picturing Adelante. Soc. Mark. Q. 2016, 23, 18–35. [Google Scholar] [CrossRef]
- Proshansky, H.M. The City and Self-Identity. Environ. Behav. 1978, 10, 147–169. [Google Scholar] [CrossRef]
- Proshansky, H.M.; Fabian, A.K.; Kaminoff, R. Place-identity: Physical world socialization of the self. J Environ. Psychol. 1983, 3, 57–83. [Google Scholar] [CrossRef]
- Lalli, M. Urban-related identity: Theory, measurement, and empirical findings. J. Environ. Psychol. 1992, 12, 285–303. [Google Scholar] [CrossRef]
- Bjork, J.; Albin, M.; Grahn, P.; Jacobsson, H.; Ardo, J.; Wadbro, J.; Ostergren, P.-O.; Skarback, E. Recreational values of the natural environment in relation to neighbourhood satisfaction, physical activity, obesity and wellbeing. J. Epidemiol. Community Health 2008, 62, e2. [Google Scholar] [CrossRef]
- Brown, G. Mapping landscape values and development preferences: A method for tourism and residential development planning. Int. J. Tour. Res. 2006, 8, 101–113. [Google Scholar] [CrossRef]
- Yoo, S.; Kim, D.H. Perceived urban neighborhood environment for physical activity of older adults in Seoul, Korea: A multimethod qualitative study. Prev. Med. 2017, 103, S90–S98. [Google Scholar] [CrossRef] [PubMed]
- Hidalgo, M.; Hernández, B. Place Attachment: Conceptual and Empirical Questions. J. Environ. Psychol. 2001, 21, 273–281. [Google Scholar] [CrossRef]
- Ulrich, R.S.; Addoms, D.L. Psychological and Recreational Benefits of a Residential Park. J. Leis. Res. 1981, 13, 43–65. [Google Scholar] [CrossRef]
- Riger, S.; Lavrakas, P.J. Community ties: Patterns of attachment and social interaction in urban neighborhoods. Am. J. Community Psychol. 1981, 9, 55–66. [Google Scholar] [CrossRef]
- Macmillan, S. Added value of good design. Build. Res. Inf. 2006, 34, 257–271. [Google Scholar] [CrossRef]
- Iwarsson, S.; Ståhl, A. Accessibility, usability and universal design—Positioning and definition of concepts describing person-environment relationships. Disabil. Rehabil. 2003, 25, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Kaczynski, A.T.; Potwarka, L.R.; Saelens, B.E. Association of Park Size, Distance, and Features with Physical Activity in Neighborhood Parks. Am. J. Public Health 2008, 98, 1451–1456. [Google Scholar] [CrossRef] [PubMed]
- Koohsari, M.J.; Mavoa, S.; Villanueva, K.; Sugiyama, T.; Badland, H.; Kaczynski, A.T.; Owen, N.; Giles-Corti, B. Public open space, physical activity, urban design and public health: Concepts, methods and research agenda. Health Place 2015, 33, 75–82. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valderrama-Ulloa, C.; Silva-Castillo, L.; Sandoval-Grandi, C.; Robles-Calderon, C.; Rouault, F. Indoor Environmental Quality in Latin American Buildings: A Systematic Literature Review. Sustainability 2020, 12, 643. [Google Scholar] [CrossRef] [Green Version]
- Messias, D.K.H.; Sharpe, P.A.; Del Castillo-González, L.; Treviño, L.; Parra-Medina, D. Living in Limbo: Latinas’ Assessment of Lower Rio Grande Valley Colonias Communities. Public Health Nurs. 2017, 34, 267–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kahlert, D.; Schlicht, W. Older People’s Perceptions of Pedestrian Friendliness and Traffic Safety: An Experiment Using Computer-Simulated Walking Environments. Int. J. Environ. Res. Public Health 2015, 12, 10066–10078. [Google Scholar] [CrossRef]
- Díez, J.; Valiente, R.; Ramos, C.; García, R.; Gittelsohn, J.; Franco, M. The mismatch between observational measures and residents’ perspectives on the retail food environment: A mixed-methods approach in the Heart Healthy Hoods study. Public Health Nutr. 2017, 20, 2970–2979. [Google Scholar] [CrossRef] [Green Version]
- Evans, S.; Hills, S.; Orme, J. Doing More for Less? Developing Sustainable Systems of Social Care in the Context of Climate Change and Public Spending Cuts. Br. J. Soc. Work. 2011, 42, 744–764. [Google Scholar] [CrossRef] [Green Version]
- Flint, R.W. Seeking Resiliency in the Development of Sustainable Communities. Hum. Ecol. Rev. 2010, 17, 44–57. Available online: http://www.eeeee.net/resiliency_paper.pdf (accessed on 3 October 2019).
- Edwards, J.C.; Feldman, P.H.; Sangl, J.; Polakoff, D.; Stern, G.; Casey, D. Sustainability of partnership projects: A conceptual framework and checklist. Jt. Comm. J. Qual. Patient Saf. 2007, 33, 37–47. [Google Scholar] [CrossRef]
- Ennis, G.; West, D. Exploring the Potential of Social Network Analysis in Asset-based Community Development Practice and Research. Aust. Soc. Work. 2010, 63, 404–417. [Google Scholar] [CrossRef]
- Pons-Vigués, M.; Berenguera, A.; Coma-Auli, N.; Pombo-Ramos, H.; March, S.; Asensio-Martínez, A.; Moreno-Peral, P.; Mora-Simón, S.; Martínez-Andrés, M.; Pujol-Ribera, E. Health-care users, key community informants and primary health care workers’ views on health, health promotion, health assets and deficits: Qualitative study in seven Spanish regions. Int. J. Equity Health 2017, 16, 99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ali, O.; Di Nardo, F.; Harrison, A.; Verma, A. The link between perceived characteristics of neighbourhood green spaces and adults’ physical activity in UK cities: Analysis of the EURO-URHIS 2 Study. Eur. J. Public Health 2017, 27, 761–765. [Google Scholar] [CrossRef]
- Ares, P.; Risler, J. Manual de Mapeo Colectivo: Recursos Cartográficos Críticos para Procesos Territoriales de Creación Colaborativa; Tinta Limón: Buenos Aires, Argentina, 2013; Available online: https://www.miteco.gob.es/es/ceneam/recursos/pag-web/manual-mapeo-colectivo.aspx (accessed on 15 April 2018).
- Foot, J.; Hopkins, T. A Glass Half-Full: How an Asset Approach Can Improve Community Health and Well-Being; Improvement and Development Agency: London, UK, 2010; Available online: http://www.assetbasedconsulting.net/uploads/publications/A%20glass%20half%20full.pdf (accessed on 23 March 2018).
- Van Bortel, T.; Wickramasinghe, N.D.; Morgan, A.; Martin, S. Health assets in a global context: A systematic review of the literature. BMJ Open 2019, 9, e023810. [Google Scholar] [CrossRef] [Green Version]
- Agdal, R.; Midtgård, I.H.; Meidell, V. Can Asset-Based Community Development with Children and Youth Enhance the Level of Participation in Health Promotion Projects? A Qualitative Meta-Synthesis. Int. J. Environ. Res. Public Health 2019, 16, 3778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bedimo-Rung, A.L.; Mowen, A.J.; Cohen, D.A. The significance of parks to physical activity and public health. Am. J. Prev. Med. 2005, 28, 159–168. [Google Scholar] [CrossRef]
- Project for Public Spaces. Placemaking. What If We Built Our Cities around Places? 2004. Available online: http://www.pps.org (accessed on 15 October 2019).
- Penchansky, R.; Thomas, J.W. The Concept of Access. Med. Care 1981, 19, 127–140. [Google Scholar] [CrossRef]
- Battista, G.A.; Manaugh, K. Stores and mores: Toward socializing walkability. J. Transp. Geogr. 2018, 67, 53–60. [Google Scholar] [CrossRef]
- Smith, C.; Clayden, A.; Dunnett, N. Residential Landscape Sustainability. In Residential Landscape Sustainability; Wiley: Hoboken, NJ, USA, 2008. [Google Scholar]
- Smith, T.; Nelischer, M.; Perkins, N. Quality of an urban community: A framework for understanding the relationship between quality and physical form. Landsc. Urban Plan. 1997, 39, 229–241. [Google Scholar] [CrossRef]


{kind=link}
| Reference Number | Authors, Date | Place and Context | Study Design | Approach | Study Population | Outcomes Inventory/Reasons | Quality Assessment |
|---|---|---|---|---|---|---|---|
| [26] | O’Connor et al. (2019) | Victoria (Australia), n/d. | Qualitative descriptive (focus groups and interviews) | AB 1 | 41 (university of the third age and primary school) | Mixed Yes/yes | ++ |
| [27] | Mosavel et al. (2018) | Petersburg (USA), 2012 | PAR 2 (photovoice and GIS mapping) | CBPR 3 | 22 (young students and university students) | Only community Yes/yes | ++ |
| [28] | Sánchez-Casado et al. (2017) | Valencia city (Spain), May-July 2014 | PAR(mapping workshops) | Salutogenesis; HA | 29 (healthcare managers and professionals) | Mixed Yes/yes | + |
| [29] | Den Broeder et al. (2017) | Amsterdam (Netherlands), n/d. | Qualitative descriptive (nominal groups and interviews) | AB | 21 (health professionals) | Only community Yes/yes | ++ |
| [10] | Aviñó (2017) | Valencia city (Spain), 2010 | PAR (multi-method) | ABCD 4 | Two case studies 106 (professionals and social fabric) | Mixed Yes/yes | ++ |
| [30] | Florian et al. (2016) | Massachusetts (USA), April 2015 | PAR (photovoice and GIS mapping) | CBPR | 17 (patients with diabetes) | Only community Yes/yes | ++ |
| [31] | Cutts et al. (2016) | Erijaville (South Africa) and Memphis (USA), n/d. | PAR (mapping workshops) | CBPR | Two case studies 100 (varied social fabric) | Mixed Yes/yes | ++ |
| [32] | Jabeen (2015) | Dhaka (Bangladesh), Sept.2010 to Mar.2011 | Qualitative descriptive (focus groups and questionnaire) | AB | 180 (dwellings) | Mixed Yes/yes | ++ |
| [33] | Pérez-Wilson et al. (2015) | Granada (Spain), Jun-Sept. 2011 | Qualitative descriptive (focus groups and interviews) | Salutogenesis; HA | 34 (adolescents, teachers and nurses) | Mixed Yes/yes | ++ |
| [11] | Jakes et al. (2015) | North Carolina (USA), 2012-2013 | PAR (mapping workshops and interviews) | HA; CBPR | 84 (varied social fabric) | Only community Yes/yes | ++ |
| [34] | Matthiesen et al. (2014) | Cumbria, Merseyside and Cheshire (England), 2011 | PAR (mapping workshops and community event) | ABCD | Two case studies (93 professionals and 143 organisations) | Mixed Yes/yes | + |
| [35] | DyckFehderau et al. (2013) | Alberta (USA), Aug. 2008 to Oct. 2009 | PAR (photovoice and discussion mapping) | CBPR | Students (11–16 years old) | Only community Yes/yes | + |
| [36] | Greetham et al. (2012) | Wakefield (England), 2010 | PAR (multi-method) | ABCD | 43 (varied social fabric) | Mixed Yes/yes | + |
| [37] | Lazarus et al. (2010) | Swellendam (South Africa) Feb-Nov. 2010 | PAR (multi-method) | CBPR | 295 (varied social fabric) | Mixed Yes/yes | + |
| Source | Link | Origin |
|---|---|---|
| Accessibility | is cause of | Walkability |
| Economic accessibility | is property of | Affordability |
| Adaptability | is property of | Sustainability |
| Appropriation | is part of | Identity |
| Affordability | is property of | Accessibility |
| Physical barriers | is cause of | Walkability |
| Community capital | is associated with | Sustainability |
| Features | is property of | Design |
| Comfort | is associated with | Design |
| Commitment | is property of | Participation |
| Confidence | is cause of | Safety |
| Time availability | is property of | Opportunity |
| Equity/inclusiveness | is property of | Intersectorality |
| Equity/inclusiveness | is associated with | Participation |
| Open spaces | is associated with | Public |
| Aesthetic | is cause of | Walkability |
| Aesthetic | is property of | Design |
| Strategic-reflective | is property of | Organisational structure |
| Organisational structure | is property of | Intersectorality |
| Utility | is associated with | Meaningfulness |
| Previous use | is property of | Utility |
| Attitude | is associated with | Meaningfulness |
| Funcionality | is associated with | Multifunctionality |
| Abilities | is associated with | Walkability |
| Illumination | is cause of | Safety |
| Information | is part of | Legibility |
| Intersectorality | is associated with | Participation |
| Intersectorality | is property of | Sustainability |
| Maintenance | is associated with | Features |
| Maintenance | is cause of | Safety |
| Fresh/nature | is associated with | Peace/calm |
| Opportunity | is property of | Affordability |
| Participation | is cause of | Safety |
| Participation | is associated with | Socialisation |
| Participation | is cause of | Abilities |
| Participation | is cause of | Manageability/control |
| Participation | is cause of | Meaningfulness |
| Participation | is associated with | Identity |
| Stable/durable | is property of | Sustainability |
| Proximity | is cause of | Walkability |
| Safety | is cause of | Walkability |
| Security | is part of | Safety |
| Socialisation | is associated with | Safety |
| Socialisation | is cause of | Abilities |
| Adaptability | is property of | Sustainability |
| Mixed land uses | is cause of | Walkability |
| Variety (offer/service) | is associated with | Funcionality |
| Variety (offer/service) | noname | Multifunctionality |
| Dimension | Categories | Concepts |
|---|---|---|
| Utility | - | Fundamental needs |
| Intention (personal) | Subjective Norm | - |
| Attitude | - | |
| Motivation and desire | - | |
| Previous use | - | - |
| Affordability | Circumstances Opportunity Economic accessibility | - |
| Time | ||
| - | ||
| Proximity | - | - |
| Walkability | - - | Rectitude |
| Integrity | ||
| Connectivity | - | - |
| Legibility | Visibility Transparency/clarity | - |
| - | ||
| Identity | Singularity | - |
| Appropriability | - | |
| Attachment | - | |
| Design | Configuration | Features/Characteristics |
| Aesthetic | ||
| Funcionality | Flexibility | |
| Multifuncionality | ||
| Comfort | - | |
| Safety | Security (perceived) | - |
| Security (objetive) | - | |
| Diversity | - | Quantity |
| - | Variety | |
| Public | Public | - |
| Privacy | - | |
| Sustainability | Durability | Maintenance |
| Economic sustainability | Social cost effectiveness | |
| Environmental sustainability | - | |
| Centrality | Participation | |
| Betweenness centrality | ||
| Closeness | ||
| Equity | - | |
| Inclusiveness | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sáinz-Ruiz, P.A.; Sanz-Valero, J.; Gea-Caballero, V.; Melo, P.; Nguyen, T.H.; Suárez-Máximo, J.D.; Martínez-Riera, J.R. Dimensions of Community Assets for Health. A Systematised Review and Meta-Synthesis. Int. J. Environ. Res. Public Health 2021, 18, 5758. https://doi.org/10.3390/ijerph18115758
Sáinz-Ruiz PA, Sanz-Valero J, Gea-Caballero V, Melo P, Nguyen TH, Suárez-Máximo JD, Martínez-Riera JR. Dimensions of Community Assets for Health. A Systematised Review and Meta-Synthesis. International Journal of Environmental Research and Public Health. 2021; 18(11):5758. https://doi.org/10.3390/ijerph18115758
Chicago/Turabian StyleSáinz-Ruiz, Pablo Alberto, Javier Sanz-Valero, Vicente Gea-Caballero, Pedro Melo, Tam H. Nguyen, Juan Daniel Suárez-Máximo, and José Ramón Martínez-Riera. 2021. "Dimensions of Community Assets for Health. A Systematised Review and Meta-Synthesis" International Journal of Environmental Research and Public Health 18, no. 11: 5758. https://doi.org/10.3390/ijerph18115758