
Shift Work and Dry Eye Disease in the Korean Working Population: A Population-Based Cross-Sectional Study


Abstract
:1. Introduction
2. Materials and Methods
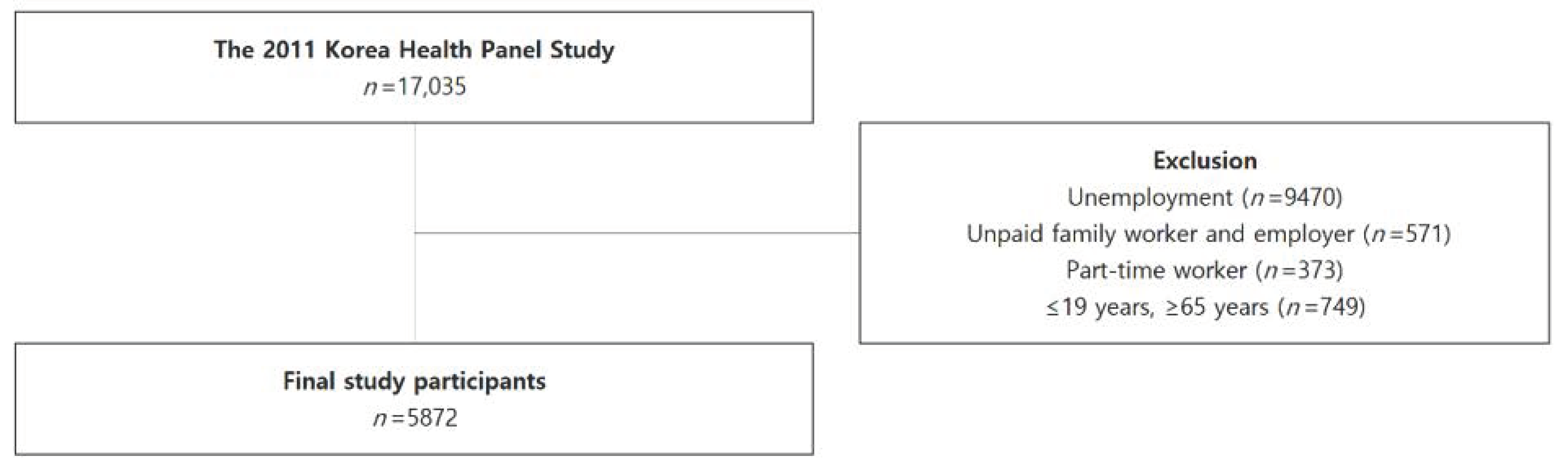
2.1. Study Participants
2.2. Main Exposures and Outcomes
2.3. Covariate
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Participants
3.2. Association between Shift Work and DED
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
| Crude OR (95% CI) | Adjusted OR a (95% CI) | p-Value for Interaction | |
|---|---|---|---|
| Shift worker | |||
| Male | |||
| <40 yeras | 2.647 (0.719–8.025) | 2.907 (0.782–8.933) | 0.3047 |
| ≥40 years | 1.184 (0.606–2.116) | 1.141 (0.516–2.256) | |
| Female | |||
| <40 yeras | 2.760 (0.901–7.003) | 3.545 (1.132–9.349) | 0.0336 |
| ≥40 years | 0.586 (0.204–1.330) | 0.584 (0.174–1.463) |
| Crude OR (95% CI) | Adjusted OR a (95% CI) | p-Value for Interaction | |
|---|---|---|---|
| Shift worker | |||
| Overall | 1.050 (0.678–1.560) | 1.127 (0.725–1.683) | |
| Subgroup for age group | |||
| <40 yeras | 2.323 (1.031–4.736) | 3.061 (1.336–6.395) | 0.0242 |
| ≥40 years | 0.817 (0.475–1.317) | 0.934 (0.539–1.515) | |
| Subgroup for sex | |||
| Male | 1.350 (0.757–2.256) | 1.380 (0.771–2.321) | 0.4523 |
| Female | 0.972 (0.470–1.794) | 1.068 (0.513–1.994) |
References
- Chia, E.M.; Mitchell, P.; Rochtchina, E.; Lee, A.J.; Maroun, R.; Wang, J.J. Prevalence and associations of dry eye syndrome in an older population: The blue mountains eye study. Clin. Exp. Ophthalmol. 2003, 31, 229–232. [Google Scholar] [CrossRef]
- McCarty, C.A.; Bansal, A.K.; Livingston, P.M.; Stanislavsky, Y.L.; Taylor, H.R. The epidemiology of dry eye in melbourne, australia. Ophthalmology 1998, 105, 1114–1119. [Google Scholar] [CrossRef]
- Craig, J.P.; Nelson, J.D.; Azar, D.T.; Belmonte, C.; Bron, A.J.; Chauhan, S.K.; de Paiva, C.S.; Gomes, J.A.P.; Hammitt, K.M.; Jones, L.; et al. Tfos dews ii report executive summary. Ocul. Surf. 2017, 15, 802–812. [Google Scholar] [CrossRef]
- Yamada, M.; Mizuno, Y.; Shigeyasu, C. Impact of dry eye on work productivity. Clin. Outcomes Res. 2012, 4, 307–312. [Google Scholar] [CrossRef] [Green Version]
- Ayaki, M.; Kawashima, M.; Negishi, K.; Tsubota, K. High prevalence of sleep and mood disorders in dry eye patients: Survey of 1000 eye clinic visitors. Neuropsychiatr. Dis. Treat. 2015, 11, 889–894. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The epidemiology of dry eye disease: Report of the epidemiology subcommittee of the international dry eye workshop (2007). Ocul. Surf. 2007, 5, 93–107. [CrossRef]
- Courtin, R.; Pereira, B.; Naughton, G.; Chamoux, A.; Chiambaretta, F.; Lanhers, C.; Dutheil, F. Prevalence of dry eye disease in visual display terminal workers: A systematic review and meta-analysis. BMJ Open 2016, 6, e009675. [Google Scholar] [CrossRef] [Green Version]
- Bhatnagar, K.R.; Sapovadia, A.; Gupta, D.; Kumar, P.; Jasani, H. Dry eye syndrome: A rising occupational hazard in tropical countries. Med. J. DY Patil Univ. 2014, 7, 13–18. [Google Scholar] [CrossRef]
- Makateb, A.; Torabifard, H. Dry eye signs and symptoms in night-time workers. J. Curr. Ophthalmol. 2017, 29, 270–273. [Google Scholar] [CrossRef]
- LaDou, J.; Harrison, R. Current Occupational & Environmental Medicine, 4th ed.; McGraw-Hill: New York, NY, USA, 2007; pp. 584–586. [Google Scholar]
- Park, J.-W.; Sun, Y.; Noh, M.-S. The relationship between shift work and depressive symptom. KJFP 2016, 6, 63–69. [Google Scholar] [CrossRef]
- Akerstedt, T. Psychological and psychophysiological effects of shift work. Scand. J. Work Environ. Health 1990, 16 (Suppl. 1), 67–73. [Google Scholar] [CrossRef]
- Proper, K.I.; van de Langenberg, D.; Rodenburg, W.; Vermeulen, R.C.H.; van der Beek, A.J.; van Steeg, H.; van Kerkhof, L.W.M. The relationship between shift work and metabolic risk factors: A systematic review of longitudinal studies. Am. J. Prev. Med. 2016, 50, e147–e157. [Google Scholar] [CrossRef] [PubMed]
- Bonham, M.P.; Bonnell, E.K.; Huggins, C.E. Energy intake of shift workers compared to fixed day workers: A systematic review and meta-analysis. Chronobiol. Int. 2016, 33, 1086–1100. [Google Scholar] [CrossRef] [PubMed]
- Kang, W.; Park, W.J.; Jang, K.H.; Kim, S.H.; Gwon, D.H.; Lim, H.M.; Ahn, J.S.; Moon, J.D. Coronary artery atherosclerosis associated with shift work in chemical plant workers by using coronary ct angiography. Occup. Environ. Med. 2016, 73, 501–505. [Google Scholar] [CrossRef]
- Guillon, M.; Maïssa, C. Tear film evaporation—Effect of age and gender. Cont. Lens Anterior Eye 2010, 33, 171–175. [Google Scholar] [CrossRef]
- Akpek, E.K.; Amescua, G.; Farid, M.; Garcia-Ferrer, F.J.; Lin, A.; Rhee, M.K.; Varu, D.M.; Musch, D.C.; Dunn, S.P.; Mah, F.S.; et al. Dry eye syndrome preferred practice pattern®. Ophthalmology 2019, 126, P286–P334. [Google Scholar] [CrossRef] [Green Version]
- von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P. STROBE Initiative. The strengthening the reporting of observational studies in epidemiology (strobe) statement: Guidelines for reporting observational studies. Int. J. Surg. 2014, 12, 1495–1499. [Google Scholar] [CrossRef] [Green Version]
- Phang, H.S. Work-Life Profiles of Korean Workers: Life-Table Analysis. Available online: https://www.kli.re.kr/klips/selectBbsNttView.do?key=159&bbsNo=47&nttNo=101481 (accessed on 11 March 2021).
- Ahn, J.; Cho, S.-S.; Kim, H.-R.; Myong, J.-P.; Kang, M.-Y. Comparison of work environment and occupational injury in direct and indirect employment in korea and europe. Ann. Occup. Environ. Med. 2019, 31, e24. [Google Scholar] [CrossRef]
- Spiegel, K.; Leproult, R.; Van Cauter, E. Impact of sleep debt on metabolic and endocrine function. Lancet (Lond. Engl. ) 1999, 354, 1435–1439. [Google Scholar] [CrossRef]
- de Paiva, C.S. Effects of aging in dry eye. Int. Ophthalmol. Clin. 2017, 57, 47–64. [Google Scholar] [CrossRef] [Green Version]
- Magno, M.S.; Utheim, T.P.; Snieder, H.; Hammond, C.J.; Vehof, J. The relationship between dry eye and sleep quality. Ocul. Surf. 2021, 20, 13–19. [Google Scholar] [CrossRef]
- Lekhanont, K.; Rojanaporn, D.; Chuck, R.S.; Vongthongsri, A. Prevalence of dry eye in bangkok, thailand. Cornea 2006, 25, 1162–1167. [Google Scholar] [CrossRef]
- Versura, P.; Campos, E.C. Menopause and dry eye. A possible relationship. Gynecol. Endocrinol.: Off. J. Int. Soc. Gynecol. Endocrinol. 2005, 20, 289–298. [Google Scholar] [CrossRef]
- Schaumberg, D.A.; Dana, R.; Buring, J.E.; Sullivan, D.A. Prevalence of dry eye disease among us men: Estimates from the physicians’ health studies. Arch. Ophthalmol. 2009, 127, 763–768. [Google Scholar] [CrossRef] [Green Version]
- Lin, P.-Y.; Tsai, S.-Y.; Cheng, C.-Y.; Liu, J.-H.; Chou, P.; Hsu, W.-M. Prevalence of dry eye among an elderly chinese population in taiwan: The shihpai eye study. Ophthalmology 2003, 110, 1096–1101. [Google Scholar] [CrossRef]
- Lee, A.J.; Lee, J.; Saw, S.M.; Gazzard, G.; Koh, D.; Widjaja, D.; Tan, D.T.H. Prevalence and risk factors associated with dry eye symptoms: A population based study in indonesia. Br. J. Ophthalmol. 2002, 86, 1347–1351. [Google Scholar] [CrossRef]
- Moss, S.E.; Klein, R.; Klein, B.E. Prevalence of and risk factors for dry eye syndrome. Arch. Ophthalmol. 2000, 118, 1264–1268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shah, D. Healthy worker effect phenomenon. Indian J. Occup Environ. Med. 2009, 13, 77–79. [Google Scholar] [CrossRef]
- Dana, R.; Bradley, J.L.; Guerin, A.; Pivneva, I.; Stillman, I.Ö.; Evans, A.M.; Schaumberg, D.A. Estimated prevalence and incidence of dry eye disease based on coding analysis of a large, all-age united states health care system. Am. J. Ophthalmol. 2019, 202, 47–54. [Google Scholar] [CrossRef] [Green Version]
- Ousler, G.W., 3rd; Rimmer, D.; Smith, L.M.; Abelson, M.B. Use of the controlled adverse environment (cae) in clinical research: A review. Ophthalmol. Ther. 2017, 6, 263–276. [Google Scholar] [CrossRef] [Green Version]
- Uchino, M.; Yokoi, N.; Uchino, Y.; Dogru, M.; Kawashima, M.; Komuro, A.; Sonomura, Y.; Kato, H.; Kinoshita, S.; Schaumberg, D.A.; et al. Prevalence of dry eye disease and its risk factors in visual display terminal users: The osaka study. Am. J. Ophthalmol. 2013, 156, 759–766. [Google Scholar] [CrossRef]
- Huang, A.; Janecki, J.; Galor, A.; Rock, S.; Menendez, D.; Hackam, A.S.; Jeng, B.H.; Kumar, N. Association of the indoor environment with dry eye metrics. JAMA Ophthalmol. 2020, 138, 867–874. [Google Scholar] [CrossRef] [PubMed]

| Non-DED, n (%) | DED, n (%) | p-Value | ||
|---|---|---|---|---|
| Total | 5691 (96.92) | 181 (3.08) | ||
| Age group (years) | ||||
| 20–39 | 1963 (97.95) | 41 (2.05) | 0.0009 | |
| 40–64 | 3728 (96.38) | 140 (3.62) | ||
| Work schedule | ||||
| Daytime worker | 5076 (96.96) | 159 (3.04) | 0.0879 | |
| Shift worker | 615 (96.55) | 22 (3.45) | ||
| Sex | ||||
| Male | 3633 (98.00) | 74 (2.00) | < 0.0001 | |
| Female | 2058 (95.06) | 107 (4.94) | ||
| Occupational classification | ||||
| White collar | 2067 (97.04) | 63 (2.96) | 0.9318 | |
| Pink collar | 1180 (96.80) | 39 (3.20) | ||
| Green collar | 295 (96.41) | 11 (3.59) | ||
| Blue collar | 2136 (96.91) | 68 (3.09) | ||
| Soldier or no information on job | 13 (100.00) | 0 (0.00) | ||
| Smoking status | ||||
| Never-smoker and ex-smoker | 3791 (96.10) | 154 (3.90) | < 0.0001 | |
| Current smoker | 1900 (98.60) | 27 (1.40) | ||
| Alcohol use | ||||
| No | 954 (96.36) | 36 (3.64) | 0.2688 | |
| Yes | 4737 (97.03) | 145 (2.97) | ||
| Connective tissue disease | ||||
| No | 5659 (96.95) | 178 (3.05) | 0.0595 | |
| Yes | 32 (91.43) | 3 (8.57) | ||
| DM | ||||
| No | 5448 (97.08) | 164 (2.92) | 0.001 | |
| Yes | 243 (93.46) | 17 (6.54) | ||
| Acne | ||||
| No | 5673 (96.92) | 180 (3.08) | 0.4489 | |
| Yes | 18 (94.74) | 1 (5.26) | ||
| Gout | ||||
| No | 5652 (96.95) | 178 (3.05) | 0.1385 | |
| Yes | 39 (92.86) | 3 (7.14) | ||
| Crude OR (95% CI) | Adjusted OR a (95% CI) | p-Value for Interaction | |
|---|---|---|---|
| Shift worker | |||
| Overall | 1.142 (0.707–1.758) | 1.202 (0.741–1.860) | |
| Subgroup for age | |||
| <40 years | 2.323 (1.031–4.736) | 3.061 (1.336–6.395) | 0.037 |
| ≥40 years | 0.845 (0.451–1.452) | 0.923 (0.490–1.598) | |
| Subgroup for sex | |||
| Male | 1.507 (0.787–2.676) | 1.431 (0.742–2.563) | 0.449 |
| Female | 1.054 (0.487–2.013) | 1.093 (0.502–2.111) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, J.; Ryu, S.-J.; Song, J.; Kim, H.-R. Shift Work and Dry Eye Disease in the Korean Working Population: A Population-Based Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 5492. https://doi.org/10.3390/ijerph18105492
Ahn J, Ryu S-J, Song J, Kim H-R. Shift Work and Dry Eye Disease in the Korean Working Population: A Population-Based Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2021; 18(10):5492. https://doi.org/10.3390/ijerph18105492
Chicago/Turabian StyleAhn, Joonho, So-Jung Ryu, Jihun Song, and Hyoung-Ryoul Kim. 2021. "Shift Work and Dry Eye Disease in the Korean Working Population: A Population-Based Cross-Sectional Study" International Journal of Environmental Research and Public Health 18, no. 10: 5492. https://doi.org/10.3390/ijerph18105492