Fruit and Vegetable Intake and All-Cause Mortality in a Chinese Population: The China Health and Nutrition Survey

 ,
,
Abstract
:1. Introduction
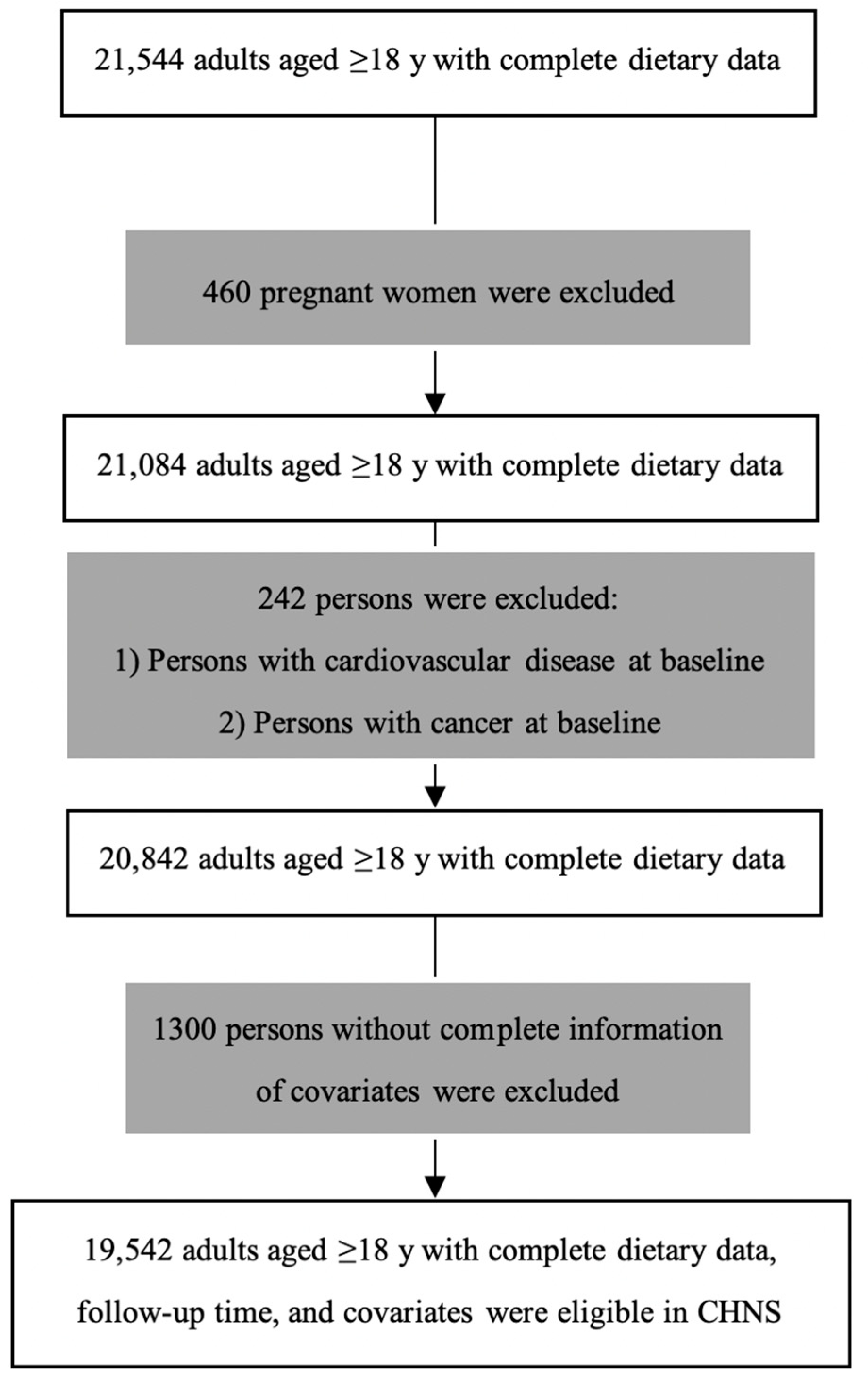
2. Methods
2.1. Data Source
2.2. Measurement
2.2.1. Exposure
2.2.2. Outcome
2.2.3. Covariates
2.3. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
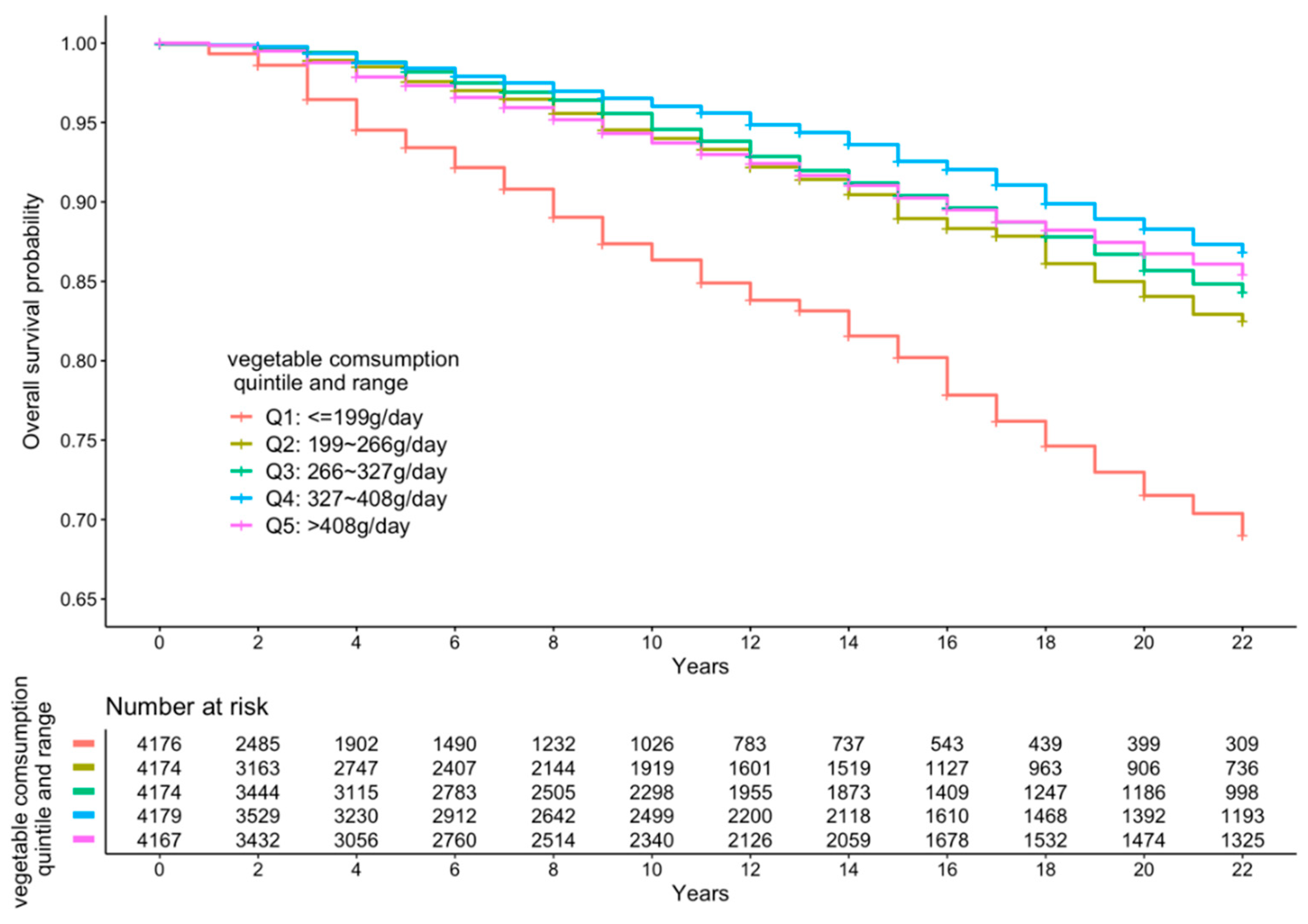
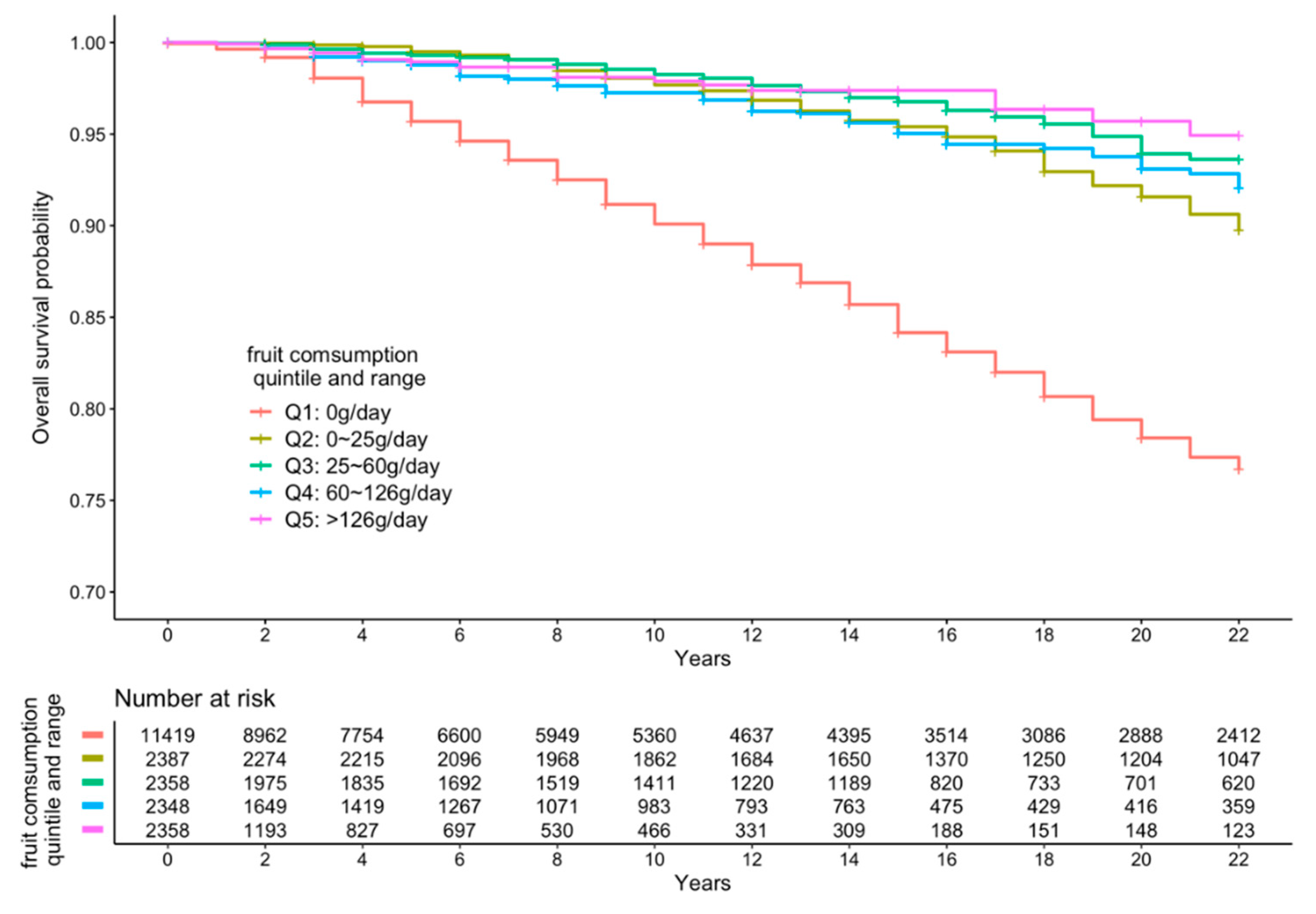
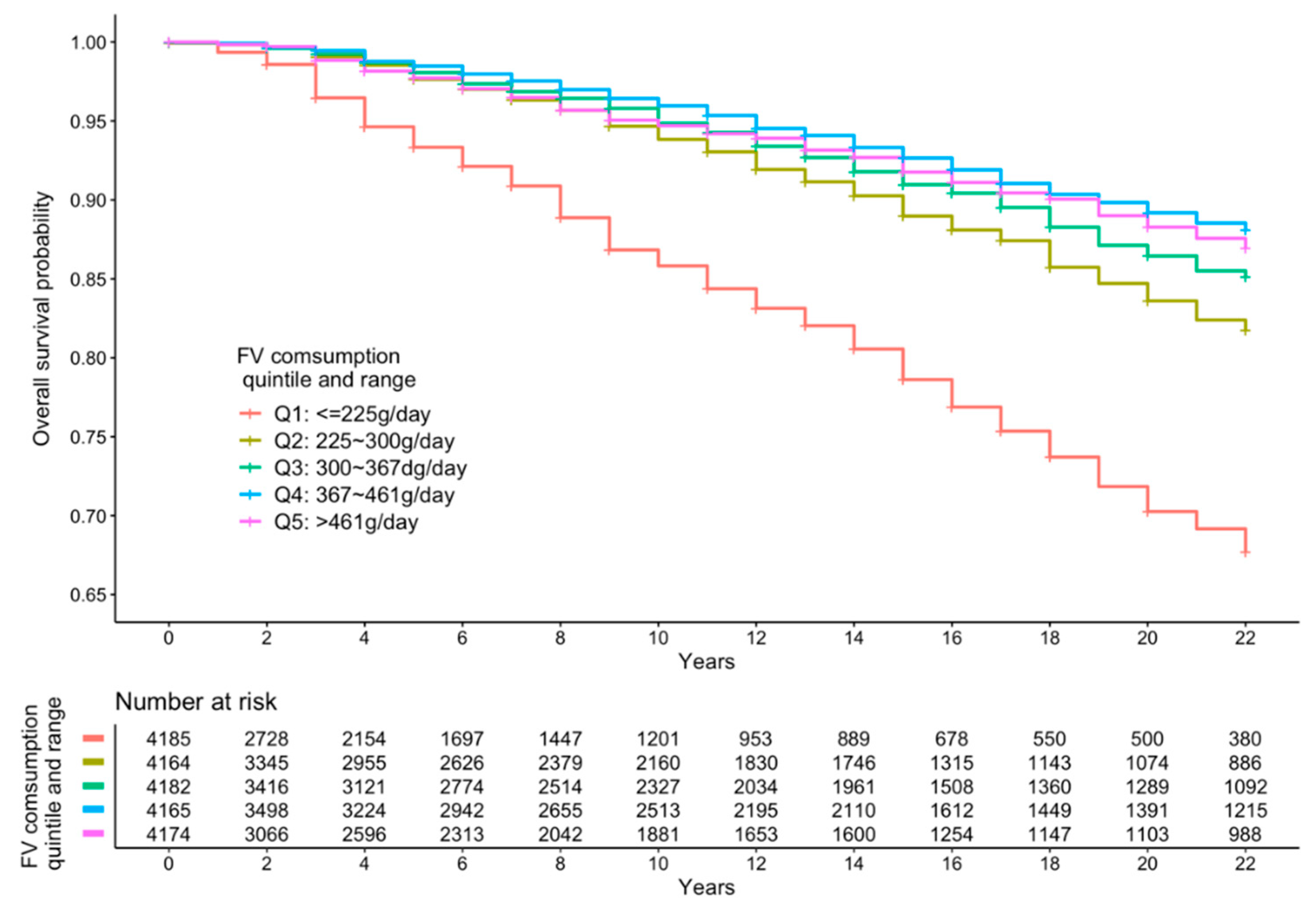
3.2. FV Intake and All-Cause Mortality
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dhandevi, P.; Jeewon, R. Fruit and vegetable intake: Benefits and progress of nutrition education interventions-narrative review article. Iran. J. Public Health 2015, 44, 1309. [Google Scholar]
- Li, X.-T.; Liao, W.; Yu, H.-J.; Liu, M.-W.; Yuan, S.; Tang, B.-W.; Yang, X.-H.; Song, Y.; Huang, Y.; Cheng, S.-L.; et al. Combined effects of fruit and vegetables intake and physical activity on the risk of metabolic syndrome among Chinese adults. PLoS ONE 2017, 12, e0188533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xiao, H.-J.; Liang, H.; Wang, J.-B.; Huang, C.-Y.; Wei, W.-Q.; Boniol, M.; Qiao, Y.-L.; Boffetta, P. Attributable causes of cancer in China: Fruit and vegetable. Chin. J. Cancer Res. 2011, 23, 171–176. [Google Scholar] [CrossRef] [Green Version]
- Yang, Y. Expert Interpretation-New Dietary Guidelines (3) Eat More Fruits and Vegetables, Milk, Soybeans. Available online: http://dg.cnsoc.org/article/04/8a2389fd575f695101577a3abfdd02d7.html (accessed on 10 August 2019).
- Zhao, L.; Fang, Y.; He, Y.; Yu, D.; Guo, Q.; Yu, W.; Zhao, W. Trends of food intake among Chinese population in 1992–2012. J. Hyg. Res. 2016, 45, 522–526. [Google Scholar]
- Li, Y.C.; Jiang, B.; Zhang, M.; Huang, Z.J.; Qian DE, N.G.; Zhou, M.G.; Wang, L.M. Vegetable and fruit intake among Chinese adults and associated factors: A nationally representative study of 170,847 adults. Biomed. Environ. Sci. 2017, 30, 863–874. [Google Scholar] [PubMed]
- Kaur, H.; Aeri, B.T. Protective Impact of Fruits and Vegetable Intake on Cardiovascular Risk Factors-A Review. J. Clin. Diagn. Res. 2019, 13, 6–9. [Google Scholar]
- Yahia, E.M. The Contribution of Fruit and Vegetable Intake to Human Health. In Fruit and Vegetable Phytochemicals; Wiley: Hoboken, NJ, USA, 2010; pp. 3–51. [Google Scholar]
- Du, H.; Li, L.; Bennett, D.; Yang, L.; Guo, Y.; Key, T.J.; Chen, J. Fresh fruit intake and all-cause and cause-specific mortality: Findings from the China Kadoorie Biobank. Int. J. Epidemiol. 2017, 46, 1444–1455. [Google Scholar] [CrossRef] [Green Version]
- Aune, D.; Giovannucci, E.; Boffetta, P.; Fadnes, L.T.; Keum, N.; Norat, T.; Greenwood, D.C.; Riboli, E.; Vatten, L.J.; Tonstad, S. Fruit and vegetable intake and the risk of cardiovascular disease, total cancer and all-cause mortality—A systematic review and dose-response meta-analysis of prospective studies. Int. J. Epidemiol. 2017, 46, 1029–1056. [Google Scholar] [CrossRef]
- Du, H.; Li, L.; Bennett, D.; Guo, Y.; Key, T.J.; Bian, Z.; Chen, J. Fresh Fruit Intake and Major Cardiovascular Disease in China. N. Eng. J. Med. 2016, 374, 1332–1343. [Google Scholar] [CrossRef]
- Nechuta, S.J.; Shu, X.-O.; Li, H.-L.; Yang, G.; Xiang, Y.-B.; Cai, H.; Chow, W.-H.; Ji, B.; Zhang, X.; Wen, W.; et al. Combined Impact of Lifestyle-Related Factors on Total and Cause-Specific Mortality among Chinese Women: Prospective Cohort Study. PLoS Med. 2010, 7, e1000339. [Google Scholar] [CrossRef]
- Wang, Y.; Yan, R.; Yin, L.; Chen, H.; Li, W. A8560 Fruit, vegetable, and legume intake and mortality risk among China adults. J. Hypertens. 2018, 36, e309. [Google Scholar] [CrossRef]
- Popkin, B.; Du, S.; Zhai, F.; Zhang, B. Cohort Profile: The China Health and Nutrition Survey--monitoring and understanding socio-economic and health change in China, 1989–2011. Int. J. Epidemiol. 2009, 39, 1435–1440. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, B.; Bauman, A.; Gale, J.; Banks, E.; Kritharides, L.; Ding, D. Fruit and vegetable intake and all-cause mortality: Evidence from a large Australian cohort study. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 9. [Google Scholar] [CrossRef]
- Batis, C.; Sotres-Alvarez, D.; Gordon-Larsen, P.; Mendez, M.A.; Adair, L.; Popkin, B. Longitudinal analysis of dietary patterns in Chinese adults from 1991 to 2009. Br. J. Nutr. 2014, 111, 1441–1451. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Ouyang, Y.; Liu, J.; Zhu, M.; Zhao, G.; Bao, W.; Hu, F.B. Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: Systematic review and dose-response meta-analysis of prospective cohort studies. BMJ 2014, 349, g4490. [Google Scholar] [CrossRef] [Green Version]
- Pan, X.-D.; Wu, P.-G.; Jiang, X.-G. Levels and potential health risk of heavy metals in marketed vegetables in Zhejiang, China. Sci. Rep. 2016, 6, 20317. [Google Scholar] [CrossRef] [Green Version]
- Xu, X.; Li, L.; Huang, X.; Lin, H.; Liu, G.; Xu, D.; Jiang, J. Survey of Four Groups of Cumulative Pesticide Residues in 12 Vegetables in 15 Provinces in China. J. Food Prot. 2018, 81, 377–385. [Google Scholar] [CrossRef]
- Engwa, G.A.; Ferdinand, P.U.; Nwalo, F.N.; Unachukwu, M.N. Mechanism and Health Effects of Heavy Metal Toxicity in Humans. In Poisoning in the Modern World–New Tricks for an Old Dog? IntechOpen: London, UK, 2019. [Google Scholar]
- Kim, K.-H.; Kabir, E.; Jahan, S.A. Exposure to pesticides and the associated human health effects. Sci. Total. Environ. 2017, 575, 525–535. [Google Scholar] [CrossRef]
- Okuda, N.; Miura, K.; Okayama, A.; Okamura, T.; Abbott, R.D.; Nishi, N.; Fujiyoshi, A.; Kita, Y.; Nakamura, Y.; Miyagawa, N.; et al. Fruit and vegetable intake and mortality from cardiovascular disease in Japan: A 24-year follow-up of the NIPPON DATA80 Study. Eur. J. Clin. Nutr. 2015, 69, 482–488. [Google Scholar] [CrossRef]
- Choi, Y.; Lee, J.E.; Bae, J.-M.; Li, Z.-M.; Kim, D.-H.; Lee, M.-S.; Ahn, Y.-O.; Shin, M.-H. Vegetable Intake, but Not Fruit Intake, Is Associated with a Reduction in the Risk of Cancer Incidence and Mortality in Middle-Aged Korean Men. J. Nutr. 2015, 145, 1249–1255. [Google Scholar] [CrossRef] [Green Version]
- Oyebode, O.; Gordondseagu, V.L.Z.; Walker, A.; Mindell, J.S. Fruit and vegetable consumption and all-cause, cancer and CVD mortality: Analysis of Health Survey for England data. J. Epidemiol. Community Health 2014, 68, 856–862. [Google Scholar] [CrossRef]
- Leenders, M.; Sluijs, I.; Ros, M.M.; Boshuizen, H.C.; Siersema, P.D.; Ferrari, P.; Clavel-Chapelon, F. Fruit and Vegetable Intake and Mortality European Prospective Investigation into Cancer and Nutrition. Am. J. Epidemiol. 2013, 178, 590–602. [Google Scholar] [CrossRef]
- Bellavia, A.; Larsson, S.C.; Bottai, M.; Wolk, A.; Orsini, N. Fruit and vegetable intake and all-cause mortality: A dose-response analysis. Am. J. Clin. Nutr. 2013, 98, 454–459. [Google Scholar] [CrossRef]
- Zhang, X.; Shu, X.O.; Xiang, Y.B.; Yang, G.; Li, H.; Gao, J.; Zheng, W. Cruciferous vegetable intake is associated with a reduced risk of total and cardiovascular disease mortality. Am. J. Clin. Nutr. 2011, 94, 240–246. [Google Scholar] [CrossRef]
- Nakamura, K.; Nagata, C.; Oba, S.; Takatsuka, N.; Shimizu, H. Fruit and Vegetable Intake and Mortality from Cardiovascular Disease Are Inversely Associated in Japanese Women but Not in Men. J. Nutr. 2008, 138, 1129–1134. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall | Quintiles of Fruit Intake | Quintiles of Vegetable Intake | Quintiles of Combined FV Intake | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | Q1 | Q2 | Q3 | Q4 | Q5 | Q1 | Q2 | Q3 | Q4 | Q5 | ||
| Number of subjects | 19,542 | 10,444 | 2332 | 2251 | 2245 | 2270 | 3840 | 3891 | 3924 | 3957 | 3930 | 3800 | 3885 | 3934 | 3944 | 3979 |
| Age (mean (SD)) | 41.04 (15.37) | 40.87 (16.03) | 40.15 (14.00) | 40.15 (14.56) | 41.61 (14.60) | 43.09 (14.94) | 44.23 (17.27) | 41.79 (15.61) | 40.68 (14.76) | 39.39 (14.29) | 39.22 (14.21) | 44.00 (17.46) | 41.69 (15.66) | 40.06 (14.67) | 39.35 (13.93) | 40.25 (14.52) |
| Age group (%) | ||||||||||||||||
| 18–24 | 2895 (14.8) | 1815 (17.4) | 283 (12.1) | 300 (13.3) | 252 (11.2) | 245 (10.8) | 546 (14.2) | 529 (13.6) | 556 (14.2) | 612 (15.5) | 652 (16.6) | 579 (15.2) | 548 (14.1) | 578 (14.7) | 574 (14.6) | 616 (15.5) |
| 25–34 | 5073 (26.0) | 2595 (24.8) | 662 (28.4) | 657 (29.2) | 603 (26.9) | 556 (24.5) | 857 (22.3) | 1015 (26.1) | 1033 (26.3) | 1135 (28.7) | 1033 (26.3) | 846 (22.3) | 984 (25.3) | 1111 (28.2) | 1125 (28.5) | 1007 (25.3) |
| 35–44 | 4182 (21.4) | 2104 (20.1) | 590 (25.3) | 504 (22.4) | 528 (23.5) | 456 (20.1) | 650 (16.9) | 789 (20.3) | 908 (23.1) | 890 (22.5) | 945 (24.0) | 637 (16.8) | 816 (21.0) | 868 (22.1) | 945 (24.0) | 916 (23.0) |
| 45–54 | 3077 (15.7) | 1525 (14.6) | 380 (16.3) | 365 (16.2) | 367 (16.3) | 440 (19.4) | 608 (15.8) | 592 (15.2) | 619 (15.8) | 611 (15.4) | 647 (16.5) | 551 (14.5) | 587 (15.1) | 619 (15.7) | 646 (16.4) | 674 (16.9) |
| 55–64 | 2675 (13.7) | 1420 (13.6) | 274 (11.7) | 284 (12.6) | 319 (14.2) | 378 (16.7) | 620 (16.1) | 612 (15.7) | 534 (13.6) | 474 (12.0) | 435 (11.1) | 625 (16.4) | 590 (15.2) | 502 (12.8) | 442 (11.2) | 516 (13.0) |
| 65+ | 1640 (8.4) | 985 (9.4) | 143 (6.1) | 141 (6.3) | 176 (7.8) | 195 (8.6) | 559 (14.6) | 354 (9.1) | 274 (7.0) | 235 (5.9) | 218 (5.5) | 562 (14.8) | 360 (9.3) | 256 (6.5) | 212 (5.4) | 250 (6.3) |
| Sex = female (%) | 10,532 (53.9) | 5353 (51.3) | 1261 (54.1) | 1251 (55.6) | 1288 (57.4) | 1379 (60.7) | 2296 (59.8) | 2174 (55.9) | 2183 (55.6) | 2057 (52.0) | 1822 (46.4) | 2155 (56.7) | 2188 (56.3) | 2141 (54.4) | 2076 (52.6) | 1972 (49.6) |
| Body mass index (mean (SD)) | 23.09 (3.42) | 22.78 (3.25) | 22.96 (4.18) | 23.42 (3.23) | 23.62 (3.34) | 23.82 (3.38) | 23.35 (3.69) | 23.05 (3.21) | 23.05 (3.21) | 23.06 (3.13) | 22.86 (3.80) | 23.12 (3.57) | 23.03 (3.23) | 23.06 (3.16) | 23.06 (3.16) | 23.17 (3.84) |
| BMI category (%) | ||||||||||||||||
| underweight | 904 (4.6) | 599 (5.7) | 93 (4.0) | 65 (2.9) | 73 (3.3) | 74 (3.3) | 225 (5.9) | 153 (3.9) | 169 (4.3) | 168 (4.2) | 189 (4.8) | 236 (6.2) | 177 (4.6) | 151 (3.8) | 167 (4.2) | 173 (4.3) |
| normal weight | 11,886 (60.8) | 6642 (63.6) | 1491 (63.9) | 1333 (59.2) | 1223 (54.5) | 1197 (52.7) | 2162 (56.3) | 2349 (60.4) | 2400 (61.2) | 2419 (61.1) | 2556 (65.0) | 2213 (58.2) | 2383 (61.3) | 2450 (62.3) | 2428 (61.6) | 2412 (60.6) |
| overweight | 5330 (27.3) | 2546 (24.4) | 614 (26.3) | 672 (29.9) | 732 (32.6) | 766 (33.7) | 1094 (28.5) | 1095 (28.1) | 1079 (27.5) | 1119 (28.3) | 943 (24.0) | 1039 (27.3) | 1052 (27.1) | 1056 (26.8) | 1076 (27.3) | 1107 (27.8) |
| obese | 1422 (7.3) | 657 (6.3) | 134 (5.7) | 181 (8.0) | 217 (9.7) | 233 (10.3) | 359 (9.3) | 294 (7.6) | 276 (7.0) | 251 (6.3) | 242 (6.2) | 312 (8.2) | 273 (7.0) | 277 (7.0) | 273 (6.9) | 287 (7.2) |
| Education (%) | ||||||||||||||||
| Primary or junior high school | 14,235 (72.8) | 8330 (79.8) | 1929 (82.7) | 1598 (71.0) | 1318 (58.7) | 1060 (46.7) | 2429 (63.3) | 2718 (69.9) | 2957 (75.4) | 3001 (75.8) | 3130 (79.6) | 2661 (70.0) | 2907 (74.8) | 2962 (75.3) | 2934 (74.4) | 2771 (69.6) |
| High school or equal | 3823 (19.6) | 1656 (15.9) | 340 (14.6) | 505 (22.4) | 612 (27.3) | 710 (31.3) | 904 (23.5) | 842 (21.6) | 716 (18.2) | 749 (18.9) | 612 (15.6) | 782 (20.6) | 727 (18.7) | 730 (18.6) | 769 (19.5) | 815 (20.5) |
| College and university | 1484 (7.6) | 458 (4.4) | 63 (2.7) | 148 (6.6) | 315 (14.0) | 500 (22.0) | 507 (13.2) | 331 (8.5) | 251 (6.4) | 207 (5.2) | 188 (4.8) | 357 (9.4) | 251 (6.5) | 242 (6.2) | 241 (6.1) | 393 (9.9) |
| Individual average income † | ||||||||||||||||
| Q1 | 4884 (25.0) | 3290 (31.5) | 796 (34.1) | 454 (20.2) | 217 (9.7) | 127 (5.6) | 570 (14.8) | 819 (21.0) | 973 (24.8) | 1149 (29.0) | 1373 (34.9) | 730 (19.2) | 971 (25.0) | 1048 (26.6) | 1128 (28.6) | 1007 (25.3) |
| Q2 | 4901 (25.1) | 2805 (26.9) | 789 (33.8) | 617 (27.4) | 466 (20.8) | 224 (9.9) | 797 (20.8) | 1006 (25.9) | 1086 (27.7) | 1100 (27.8) | 912 (23.2) | 932 (24.5) | 1078 (27.7) | 1109 (28.2) | 1027 (26.0) | 755 (19.0) |
| Q3 | 4757 (24.3) | 2359 (22.6) | 549 (23.5) | 685 (30.4) | 666 (29.7) | 498 (21.9) | 866 (22.6) | 1032 (26.5) | 1085 (27.7) | 959 (24.2) | 815 (20.7) | 901 (23.7) | 981 (25.3) | 1003 (25.5) | 1003 (25.4) | 869 (21.8) |
| Q4 | 5000 (25.6) | 1990 (19.1) | 198 (8.5) | 495 (22.0) | 896 (39.9) | 1421 (62.6) | 1607 (41.8) | 1034 (26.6) | 780 (19.9) | 749 (18.9) | 830 (21.1) | 1237 (32.6) | 855 (22.0) | 774 (19.7) | 786 (19.9) | 1348 (33.9) |
| Marital status = married (%) | 16,416 (84.0) | 8465 (81.1) | 2050 (87.9) | 1982 (88.0) | 1956 (87.1) | 1963 (86.5) | 3074 (80.1) | 3246 (83.4) | 3375 (86.0) | 3416 (86.3) | 3305 (84.1) | 3015 (79.3) | 3250 (83.7) | 3353 (85.2) | 3401 (86.2) | 3397 (85.4) |
| Residence = urban (%) | 11,324 (57.9) | 6910 (66.2) | 1455 (62.4) | 1197 (53.2) | 986 (43.9) | 776 (34.2) | 1953 (50.9) | 2138 (54.9) | 2313 (58.9) | 2425 (61.3) | 2495 (63.5) | 2126 (55.9) | 2314 (59.6) | 2357 (59.9) | 2351 (59.6) | 2176 (54.7) |
| Urban index ‡ (mean (SD)) | 58.59 (22.75) | 53.72 (21.97) | 51.11 (19.11) | 59.86 (21.31) | 68.69 (20.44) | 77.44 (19.25) | 66.95 (21.47) | 61.90 (21.64) | 58.31 (21.63) | 54.61 (21.97) | 51.44 (23.66) | 63.00 (21.55) | 58.56 (21.42) | 56.95 (21.93) | 55.30 (22.40) | 59.30 (25.39) |
| Smoking status | ||||||||||||||||
| Current | 2920 (14.9) | 1537 (14.7) | 201 (8.6) | 337 (15.0) | 405 (18.0) | 440 (19.4) | 684 (17.8) | 610 (15.7) | 507 (12.9) | 537 (13.6) | 582 (14.8) | 674 (17.7) | 543 (14.0) | 517 (13.1) | 515 (13.1) | 671 (16.9) |
| Not current (never, past) | 7565 (38.7) | 3433 (32.9) | 491 (21.1) | 887 (39.4) | 1200 (53.5) | 1554 (68.5) | 1966 (51.2) | 1564 (40.2) | 1454 (37.1) | 1364 (34.5) | 1217 (31.0) | 1672 (44.0) | 1406 (36.2) | 1392 (35.4) | 1404 (35.6) | 1691 (42.5) |
| Not answered | 9057 (46.3) | 5474 (52.4) | 1640 (70.3) | 1027 (45.6) | 640 (28.5) | 276 (12.2) | 1190 (31.0) | 1717 (44.1) | 1963 (50.0) | 2056 (52.0) | 2131 (54.2) | 1454 (38.3) | 1936 (49.8) | 2025 (51.5) | 2025 (51.3) | 1617 (40.6) |
| Alcohol drinking | ||||||||||||||||
| Current | 3603 (18.4) | 1735 (16.6) | 232 (9.9) | 432 (19.2) | 549 (24.5) | 655 (28.9) | 871 (22.7) | 731 (18.8) | 664 (16.9) | 643 (16.2) | 694 (17.7) | 785 (20.7) | 659 (17.0) | 648 (16.5) | 648 (16.4) | 863 (21.7) |
| Not current (never, past) | 6838 (35.0) | 3211 (30.7) | 456 (19.6) | 788 (35.0) | 1052 (46.9) | 1331 (58.6) | 1778 (46.3) | 1429 (36.7) | 1291 (32.9) | 1249 (31.6) | 1091 (27.8) | 1555 (40.9) | 1284 (33.1) | 1251 (31.8) | 1260 (31.9) | 1488 (37.4) |
| Not answered | 9101 (46.6) | 5498 (52.6) | 1644 (70.5) | 1031 (45.8) | 644 (28.7) | 284 (12.5) | 1191 (31.0) | 1731 (44.5) | 1969 (50.2) | 2065 (52.2) | 2145 (54.6) | 1460 (38.4) | 1942 (50.0) | 2035 (51.7) | 2036 (51.6) | 1628 (40.9) |
| Physical activity | ||||||||||||||||
| Light | 10,273 (52.6) | 4623 (44.3) | 1015 (43.5) | 1307 (58.1) | 1563 (69.6) | 1765 (77.8) | 2701 (70.3) | 2374 (61.0) | 2067 (52.7) | 1731 (43.7) | 1400 (35.6) | 2454 (64.6) | 2166 (55.8) | 1955 (49.7) | 1821 (46.2) | 1877 (47.2) |
| Moderate | 3537 (18.1) | 2038 (19.5) | 519 (22.3) | 395 (17.5) | 325 (14.5) | 260 (11.5) | 577 (15.0) | 716 (18.4) | 760 (19.4) | 788 (19.9) | 696 (17.7) | 652 (17.2) | 762 (19.6) | 766 (19.5) | 713 (18.1) | 644 (16.2) |
| Heavy | 5732 (29.3) | 3783 (36.2) | 798 (34.2) | 549 (24.4) | 357 (15.9) | 245 (10.8) | 562 (14.6) | 801 (20.6) | 1097 (28.0) | 1438 (36.3) | 1834 (46.7) | 694 (18.3) | 957 (24.6) | 1213 (30.8) | 1410 (35.8) | 1458 (36.6) |
| Calorie intake (kcal/day) (mean (SD)) | 2183.09 (1190.61) | 2228.19 (1287.02) | 2229.97 (546.66) | 2129.02 (582.43) | 2071.18 (1356.15) | 2091.75 (1444.66) | 1993.62 (778.84) | 2178.29 (502.93) | 2238.84 (425.09) | 2370.71 (507.87) | 2511.44 (1175.61) | 1925.57 (1147.12) | 2093.93 (616.98) | 2187.04 (619.84) | 2284.93 (597.35) | 2411.24 (2113.77) |
| Quintiles a | P for Trend | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Q1 | Q2 | Q3 | Q4 | Q5 | |||||||
| Vegetable intake | |||||||||||
| Model 1 (crude) | 1 | Reference | 0.52 | (0.44–0.62) | 0.46 | (0.39–0.54) | 0.37 | (0.31–0.44) | 0.46 | (0.39–0.55) | <0.001 |
| Model 2 b (age, sex adjusted) | 1 | Reference | 0.71 | (0.60–0.85) | 0.74 | (0.62–0.87) | 0.66 | (0.55–0.79) | 0.93 | (0.79–1.11) | 0.311 |
| Model 3 c (adjusted) | 1 | Reference | 0.78 | (0.65,0.93) | 0.75 | (0.63,0.89) | 0.63 | (0.53,0.76) | 0.8 | (0.67,0.96) | 0.234 |
| Fruit intake | |||||||||||
| Model 1 (crude) | 1 | Reference | 0.35 | (0.29–0.41) | 0.19 | (0.15–0.25) | 0.24 | (0.18–0.31) | 0.13 | (0.08–0.21) | <0.001 |
| Model 2 b (age, sex adjusted) | 1 | Reference | 0.34 | (0.29–0.41) | 0.23 | (0.18–0.30) | 0.30 | (0.23–0.39) | 0.13 | (0.08–0.21) | <0.001 |
| Model 3 c (adjusted) | 1 | Reference | 0.36 | (0.30–0.43) | 0.28 | (0.22–0.36) | 0.43 | (0.32–0.57) | 0.24 | (0.15–0.40) | <0.001 |
| FV intake | |||||||||||
| Model 1 (crude) | 1 | Reference | 0.48 | (0.41–0.56) | 0.38 | (0.32–0.44) | 0.29 | (0.25–0.35) | 0.34 | (0.28–0.40) | <0.001 |
| Model 2 b (age, sex adjusted) | 1 | Reference | 0.68 | (0.58–0.8) | 0.61 | (0.52–0.72) | 0.56 | (0.47–0.67) | 0.65 | (0.55–0.78) | <0.001 |
| Model 3 c (adjusted) | 1 | Reference | 0.71 | (0.61–0.84) | 0.63 | (0.54–0.75) | 0.59 | (0.49–0.70) | 0.70 | (0.58–0.85) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gu, Y.; He, Y.; Ali, S.H.; Harper, K.; Dong, H.; Gittelsohn, J. Fruit and Vegetable Intake and All-Cause Mortality in a Chinese Population: The China Health and Nutrition Survey. Int. J. Environ. Res. Public Health 2021, 18, 342. https://doi.org/10.3390/ijerph18010342
Gu Y, He Y, Ali SH, Harper K, Dong H, Gittelsohn J. Fruit and Vegetable Intake and All-Cause Mortality in a Chinese Population: The China Health and Nutrition Survey. International Journal of Environmental Research and Public Health. 2021; 18(1):342. https://doi.org/10.3390/ijerph18010342
Chicago/Turabian StyleGu, Yuxuan, Yansu He, Shahmir H. Ali, Kaitlyn Harper, Hengjin Dong, and Joel Gittelsohn. 2021. "Fruit and Vegetable Intake and All-Cause Mortality in a Chinese Population: The China Health and Nutrition Survey" International Journal of Environmental Research and Public Health 18, no. 1: 342. https://doi.org/10.3390/ijerph18010342