The Effects of Pharmacological and Non-Pharmacological Interventions on Symptom Management and Quality of Life among Breast Cancer Survivors Undergoing Adjuvant Endocrine Therapy: A Systematic Review

 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction and Summary
2.4. Critical Appraisal
3. Results
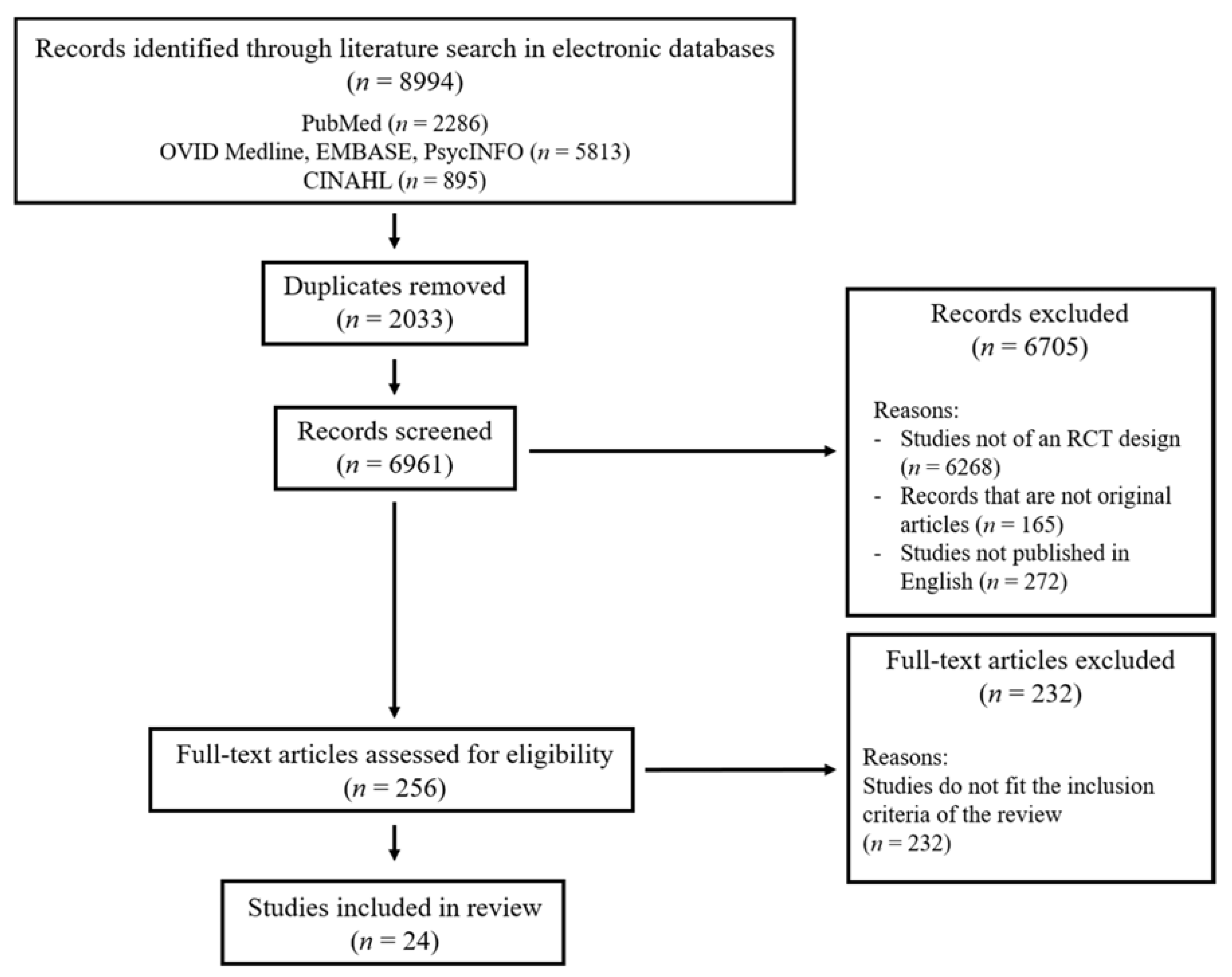
3.1. Search Results
3.2. Methodological Quality of Included Studies
3.3. Effects of Interventions on Patient Outcomes
3.3.1. Menopausal Symptoms
Hot Flashes
Night Sweats
Vaginal Atrophy
3.3.2. Sexual Dysfunction
3.3.3. Joint Symptoms
3.3.4. Fatigue
3.3.5. Sleep Disturbance
3.3.6. QOL/HRQOL
3.3.7. Functional Ability
4. Discussion
Implications
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hershman, D.L.; Shao, T.; Kushi, L.H.; Buono, D.; Tsai, W.Y.; Fehrenbacher, L.; Kwan, M.; Gomez, S.L.; Neugut, A.I. Early discontinuation and non-adherence to adjuvant hormonal therapy are associated with increased mortality in women with breast cancer. Breast Cancer Res. Treat. 2011, 126, 529–537. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harbeck, N.; Gnant, M. Breast Cancer. Lancet 2017, 389, 1134–1150. [Google Scholar] [CrossRef]
- Chan, C.W.H.; Law, B.M.H.; So, W.K.W.; Chow, K.M.; Waye, M.M.Y. Novel Strategies on Personalized Medicine for Breast Cancer Treatment: An Update. Int. J. Mol. Sci. 2017, 18, 2423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haque, R.; Ahmed, S.A.; Fisher, A.; Avila, C.C.; Shi, J.; Guo, A.; Craig Cheetham, T.; Schottinger, J.E. Effectiveness of aromatase inhibitors and tamoxifen in reducing subsequent breast cancer. Cancer Med. 2012, 1, 318–327. [Google Scholar] [CrossRef] [PubMed]
- Early Breast Cancer Trialists’ Collaborative Group (EBCTCG). Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: An overview of the randomised trials. Lancet 2005, 365, 1687–1717. [Google Scholar] [CrossRef]
- Gotay, C.; Dunn, J. Adherence to long-term adjuvant hormonal therapy for breast cancer. Expert Rev. Pharm. Outcomes Res. 2011, 11, 709–715. [Google Scholar] [CrossRef]
- Van Herk-Sukel, M.P.; van de Poll-Franse, L.V.; Voogd, A.C.; Nieuwenhuijzen, G.A.; Coebergh, J.W.; Herings, R.M. Half of breast cancer patients discontinue tamoxifen and any endocrine treatment before the end of the recommended treatment period of 5 years: A population-based analysis. Breast Cancer Res. Treat. 2010, 122, 843–851. [Google Scholar] [CrossRef] [Green Version]
- Miaskowski, C.; Shockney, L.; Chlebowski, R.T. Adherence to oral endocrine therapy for breast cancer: A nursing perspective. Clin. J. Oncol. Nurs. 2008, 12, 213–221. [Google Scholar] [CrossRef]
- Garreau, J.R.; Delamelena, T.; Walts, D.; Karamlou, K.; Johnson, N. Side effects of aromatase inhibitors versus tamoxifen: The patients’ perspective. Am. J. Surg. 2006, 192, 496–498. [Google Scholar] [CrossRef]
- Henry, N.L.; Giles, J.T.; Ang, D.; Mohan, M.; Dadabhoy, D.; Robarge, J.; Hayden, J.; Lemler, S.; Shahverdi, K.; Powers, P.; et al. Prospective characterization of musculoskeletal symptoms in early stage breast cancer patients treated with aromatase inhibitors. Breast Cancer Res. Treat. 2008, 111, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Fallowfield, L.J.; Kilburn, L.S.; Langridge, C.; Snowdon, C.F.; Bliss, J.M.; Coombes, R.C.; IES Trial Steering Committee. Long-term assessment of quality of life in the Intergroup Exemestane Study: 5 years post-randomisation. Br. J. Cancer 2012, 106, 1062–1067. [Google Scholar] [CrossRef] [Green Version]
- Schover, L.R.; Baum, G.P.; Fuson, L.A.; Brewster, A.; Melhem-Bertrandt, A. Sexual problems during the first 2 years of adjuvant treatment with aromatase inhibitors. J. Sex. Med. 2014, 11, 3102–3111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Awan, A.; Esfahani, K. Endocrine therapy for breast cancer in the primary care setting. Curr. Oncol. 2018, 25, 285–291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, Q.J.; O’Dea, A.P.; Sharma, P. Musculoskeletal adverse events associated with adjuvant aromatase inhibitors. J. Oncol. 2010, 2010, 654348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aiello Bowles, E.J.; Boudreau, D.M.; Chubak, J.; Yu, O.; Fujii, M.; Chestnut, J.; Buist, D.S. Patient-reported discontinuation of endocrine therapy and related adverse effects among women with early-stage breast cancer. J. Oncol. Pract. 2012, 8, e149–e157. [Google Scholar] [CrossRef] [Green Version]
- Makubate, B.; Donnan, P.T.; Dewar, J.A.; Thompson, A.M.; McCowan, C. Cohort study of adherence to adjuvant endocrine therapy, breast cancer recurrence and mortality. Br. J. Cancer 2013, 108, 1515–1524. [Google Scholar] [CrossRef] [Green Version]
- McCowan, C.; Wang, S.; Thompson, A.M.; Makubate, B.; Petrie, D.J. The value of high adherence to tamoxifen in women with breast cancer: A community-based cohort study. Br. J. Cancer 2013, 109, 1172–1180. [Google Scholar] [CrossRef] [Green Version]
- Simpson, B. Hot flash pharmacotherapy in breast cancer survivors: A literature review. Can. Pharm. J. 2004, 137, 36–45. [Google Scholar]
- Coleman, R.E.; Bolten, W.W.; Lansdown, M.; Dale, S.; Jackisch, C.; Merkel, D.; Maass, N.; Hadji, P. Aromatase inhibitor-induced arthralgia: Clinical experience and treatment recommendations. Cancer Treat. Rev. 2008, 34, 275–282. [Google Scholar] [CrossRef]
- Bae, K.; Yoo, H.S.; Lamoury, G.; Boyle, F.; Rosenthal, D.S.; Oh, B. Acupuncture for Aromatase Inhibitor-Induced Arthralgia: A Systematic Review. Integr. Cancer Ther. 2015, 14, 496–502. [Google Scholar] [CrossRef]
- Chen, L.; Lin, C.C.; Huang, T.W.; Kuan, Y.C.; Huang, Y.H.; Chen, H.C.; Kao, C.Y.; Su, C.M.; Tam, K.W. Effect of acupuncture on aromatase inhibitor-induced arthralgia in patients with breast cancer: A meta-analysis of randomized controlled trials. Breast 2017, 33, 132–138. [Google Scholar] [CrossRef]
- Rada, G.; Capurro, D.; Pantoja, T.; Corbalán, J.; Moreno, G.; Letelier, L.M.; Vera, C. Non-hormonal interventions for hot flushes in women with a history of breast cancer. Cochrane Database Syst. Rev. 2010, CD004923. [Google Scholar] [CrossRef] [PubMed]
- Chan, C.W.H.; Au Yeung, E.; Law, B.M.H. Effectiveness of Physical Activity Interventions on Pregnancy-Related Outcomes among Pregnant Women: A Systematic Review. Int. J. Environ. Res. Public Health 2019, 16, 1840. [Google Scholar] [CrossRef] [Green Version]
- Quality Assessment Tool for Quantitative Studies Dictionary. Available online: https://merst.ca/wp-content/uploads/2018/02/qualilty-assessment-dictionary_2017.pdf (accessed on 14 March 2020).
- De Sousa Vieira, A.F.; Mauad, V.A.Q.; Cubero, D.; Santi, P.X.; del Giglio, A. Use of Guarana for Hot Flashes after Breast Cancer: Randomized, Double-Blind, Placebo-Controlled Phase II Trial. J. Nat. Remedies 2019, 19, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Heudel, P.E.; Van Praagh-Doreau, I.; Duvert, B.; Cauvin, I.; Hardy-Bessard, A.C.; Jacquin, J.P.; Stefani, L.; Vincent, L.; Dramais, D.; Guastalla, J.P.; et al. Does a homeopathic medicine reduce hot flushes induced by adjuvant endocrine therapy in localized breast cancer patients? A multicenter randomized placebo-controlled phase III trial. Support. Care Cancer 2019, 27, 1879–1889. [Google Scholar] [CrossRef] [PubMed]
- Kimmick, G.G.; Lovato, J.; McQuellon, R.; Robinson, E.; Muss, H.B. Randomized, double-blind, placebo-controlled, crossover study of sertraline (Zoloft) for the treatment of hot flashes in women with early stage breast cancer taking tamoxifen. Breast J. 2006, 12, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Pandya, K.J.; Raubertas, R.F.; Flynn, P.J.; Hynes, H.E.; Rosenbluth, R.J.; Kirshner, J.J.; Pierce, H.I.; Dragalin, V.; Morrow, G.R. Oral clonidine in postmenopausal patients with breast cancer experiencing tamoxifen-induced hot flashes: A University of Rochester Cancer Center Community Clinical Oncology Program study. Ann. Intern. Med. 2000, 132, 788–793. [Google Scholar] [CrossRef]
- Goldberg, R.M.; Loprinzi, C.L.; O’Fallon, J.R.; Veeder, M.H.; Miser, A.W.; Mailliard, J.A.; Michalak, J.C.; Dose, A.M.; Rowland, K.M., Jr.; Burnham, N.L. Transdermal clonidine for ameliorating tamoxifen-induced hot flashes. J. Clin. Oncol. 1994, 12, 155–158. [Google Scholar] [CrossRef]
- Mann, E.; Smith, M.J.; Hellier, J.; Balabanovic, J.A.; Hamed, H.; Grunfeld, E.A.; Hunter, M.S. Cognitive behavioural treatment for women who have menopausal symptoms after breast cancer treatment (MENOS 1): A randomised controlled trial. Lancet Oncol. 2012, 13, 309–318. [Google Scholar] [CrossRef] [Green Version]
- Keshavarzi, Z.; Janghorban, R.; Alipour, S.; Tahmasebi, S.; Jokar, A. The effect of vitamin D and E vaginal suppositories on tamoxifen-induced vaginal atrophy in women with breast cancer. Support. Care Cancer 2019, 27, 1325–1334. [Google Scholar] [CrossRef]
- Paulo, T.R.S.; Rossi, F.E.; Viezel, J.; Tosello, G.T.; Seidinger, S.C.; Simões, R.R.; de Freitas, R., Jr.; Freitas, I.F., Jr. The impact of an exercise program on quality of life in older breast cancer survivors undergoing aromatase inhibitor therapy: A randomized controlled trial. Health Qual. Life Outcomes 2019, 17, 17. [Google Scholar] [CrossRef] [PubMed]
- Advani, P.; Brewster, A.M.; Baum, G.P.; Schover, L.R. A pilot randomized trial to prevent sexual dysfunction in postmenopausal breast cancer survivors starting adjuvant aromatase inhibitor therapy. J. Cancer Surviv. 2017, 11, 477–485. [Google Scholar] [CrossRef]
- Henry, N.L.; Unger, J.M.; Schott, A.F.; Fehrenbacher, L.; Flynn, P.J.; Prow, D.M.; Sharer, C.W.; Burton, G.V.; Kuzma, C.S.; Moseley, A.; et al. Randomized, Multicenter, Placebo-Controlled Clinical Trial of Duloxetine Versus Placebo for Aromatase Inhibitor-Associated Arthralgias in Early-Stage Breast Cancer: SWOG S1202. J. Clin. Oncol. 2018, 36, 326–332. [Google Scholar] [CrossRef]
- Nyrop, K.A.; Callahan, L.F.; Cleveland, R.J.; Arbeeva, L.L.; Hackney, B.S.; Muss, H.B. Randomized Controlled Trial of a Home-Based Walking Program to Reduce Moderate to Severe Aromatase Inhibitor-Associated Arthralgia in Breast Cancer Survivors. Oncologist 2017, 22, 1238–1249. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, L.Q.; Hopkins-Price, P.; Vicari, S.; Markwell, S.; Pamenter, R.; Courneya, K.S.; Hoelzer, K.; Naritoku, C.; Edson, B.; Jones, L.; et al. Physical activity and health outcomes three months after completing a physical activity behavior change intervention: Persistent and delayed effects. Cancer Epidemiol Biomark. Prev. 2009, 18, 1410–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rogers, L.Q.; Hopkins-Price, P.; Vicari, S.; Pamenter, R.; Courneya, K.S.; Markwell, S.; Verhulst, S.; Hoelzer, K.; Naritoku, C.; Jones, L.; et al. A randomized trial to increase physical activity in breast cancer survivors. Med. Sci. Sports Exerc. 2009, 41, 935–946. [Google Scholar] [CrossRef]
- Irwin, M.L.; Cartmel, B.; Gross, C.P.; Ercolano, E.; Li, F.; Yao, X.; Fiellin, M.; Capozza, S.; Rothbard, M.; Zhou, Y.; et al. Randomized exercise trial of aromatase inhibitor-induced arthralgia in breast cancer survivors. J. Clin. Oncol. 2015, 33, 1104–1111. [Google Scholar] [CrossRef]
- Hershman, D.L.; Unger, J.M.; Crew, K.D.; Awad, D.; Dakhil, S.R.; Gralow, J.; Greenlee, H.; Lew, D.L.; Minasian, L.M.; Till, C.; et al. Randomized Multicenter Placebo-Controlled Trial of Omega-3 Fatty Acids for the Control of Aromatase Inhibitor-Induced Musculoskeletal Pain: SWOG S0927. J. Clin. Oncol. 2015, 33, 1910–1917. [Google Scholar] [CrossRef]
- Hershman, D.L.; Unger, J.M.; Greenlee, H.; Capodice, J.L.; Lew, D.L.; Darke, A.K.; Kengla, A.T.; Melnik, M.K.; Jorgensen, C.W.; Kreisle, W.H.; et al. Effect of Acupuncture vs Sham Acupuncture or Waitlist Control on Joint Pain Related to Aromatase Inhibitors Among Women With Early-Stage Breast Cancer: A Randomized Clinical Trial. JAMA 2018, 320, 167–176. [Google Scholar] [CrossRef] [Green Version]
- Oh, B.; Kimble, B.; Costa, D.S.; Davis, E.; McLean, A.; Orme, K.; Beith, J. Acupuncture for treatment of arthralgia secondary to aromatase inhibitor therapy in women with early breast cancer: Pilot study. Acupunct. Med. 2013, 31, 264–271. [Google Scholar] [CrossRef]
- Crew, K.D.; Capodice, J.L.; Greenlee, H.; Apollo, A.; Jacobson, J.S.; Raptis, G.; Blozie, K.; Sierra, A.; Hershman, D.L. Pilot study of acupuncture for the treatment of joint symptoms related to adjuvant aromatase inhibitor therapy in postmenopausal breast cancer patients. J. Cancer Surviv. 2007, 1, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.K.; Peddle-McIntyre, C.J.; Galvão, D.A.; Hunt, C.; Spry, N.; Newton, R.U. Whole Body Vibration Exposure on Markers of Bone Turnover, Body Composition, and Physical Functioning in Breast Cancer Patients Receiving Aromatase Inhibitor Therapy: A Randomized Controlled Trial. Integr. Cancer Ther. 2018, 17, 968–978. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhao, H.; Zhang, Q.; Zhao, L.; Huang, X.; Wang, J.; Kang, X. Spore Powder of Ganoderma lucidum Improves Cancer-Related Fatigue in Breast Cancer Patients Undergoing Endocrine Therapy: A Pilot Clinical Trial. Evid. Based Complement Alternat. Med. 2012, 2012, 809614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peppone, L.J.; Janelsins, M.C.; Kamen, C.; Mohile, S.G.; Sprod, L.K.; Gewandter, J.S.; Kirshner, J.J.; Gaur, R.; Ruzich, J.; Esparaz, B.T.; et al. The effect of YOCAS©® yoga for musculoskeletal symptoms among breast cancer survivors on hormonal therapy. Breast Cancer Res. Treat. 2015, 150, 597–604. [Google Scholar] [CrossRef]
- Mao, J.J.; Farrar, J.T.; Bruner, D.; Zee, J.; Bowman, M.; Seluzicki, C.; DeMichele, A.; Xie, S.X. Electroacupuncture for fatigue, sleep, and psychological distress in breast cancer patients with aromatase inhibitor-related arthralgia: A randomized trial. Cancer 2014, 120, 3744–3751. [Google Scholar] [CrossRef]
- Conejo, I.; Pajares, B.; Alba, E.; Cuesta-Vargas, A.I. Effect of neuromuscular taping on musculoskeletal disorders secondary to the use of aromatase inhibitors in breast cancer survivors: A pragmatic randomised clinical trial. BMC Complement. Altern. Med. 2018, 18, 180. [Google Scholar] [CrossRef]
- Rogers, L.Q.; Courneya, K.S.; Oster, R.A.; Anton, P.M.; Robbs, R.S.; Forero, A.; McAuley, E. Physical Activity and Sleep Quality in Breast Cancer Survivors: A Randomized Trial. Med. Sci. Sports Exerc. 2017, 49, 2009–2015. [Google Scholar] [CrossRef]
- Cheng, K.K.F.; Thompson, D.R.; Ling, W.M.; Chan, C.W.H. Measuring symptom prevalence, severity and distress of cancer survivors. Clin. Eff. Nurs. 2006, 9, 154–160. [Google Scholar] [CrossRef]
- Chen, D.; Shiou, W.; Wang, K.; Huang, S.; Shie, Y.; Tsai, C.; Shie, J.; Chen, K. Chemotaxonomy of Triterpenoid Pattern of HPLC of Ganoderma lucidum and Ganoderma tsugae. J. Chin. Chem Soc. 1999, 46, 47–51. [Google Scholar] [CrossRef]
- Zhu, M.; Chang, Q.; Wong, L.K.; Chong, F.S.; Li, R.C. Triterpene antioxidants from ganoderma lucidum. Phytother Res. 1999, 13, 529–531. [Google Scholar] [CrossRef]
- Geng, P.; Siu, K.C.; Wang, Z.; Wu, J.Y. Antifatigue Functions and Mechanisms of Edible and Medicinal Mushrooms. Biomed. Res. Int. 2017, 2017, 9648496. [Google Scholar] [CrossRef] [PubMed]
- Becker, W.C.; Dorflinger, L.; Edmond, S.N.; Islam, L.; Heapy, A.A.; Fraenkel, L. Barriers and facilitators to use of non-pharmacological treatments in chronic pain. BMC Fam. Pract. 2017, 18, 41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakano, J.; Hashizume, K.; Fukushima, T.; Ueno, K.; Matsuura, E.; Ikio, Y.; Ishii, S.; Morishita, S.; Tanaka, K.; Kusuba, Y. Effects of Aerobic and Resistance Exercises on Physical Symptoms in Cancer Patients: A Meta-analysis. Integr. Cancer Ther. 2018, 17, 1048–1058. [Google Scholar] [CrossRef]
- Biau, D.J.; Kernéis, S.; Porcher, R. Statistics in brief: The importance of sample size in the planning and interpretation of medical research. Clin. Orthop. Relat. Res. 2008, 466, 2282–2288. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| “Breast cancer” OR “carcinoma” OR “neoplasm” OR “malignancy” |
| AND |
| “survivorship” OR “survivor” OR “survivors” OR “patient” OR “patients” |
| AND |
| “Tamoxifen” OR “Aromatase inhibitor” OR “endocrine therapy” OR “hormone therapy” OR “hormonal therapy” |
| AND |
| “Intervention” OR “therapy” OR “program” OR “programme” OR “pharmacological” OR “non-pharmacological” |
| AND |
| “quality of life” OR “well-being” OR “well being” OR “symptom” OR “symptoms” OR “side effects” OR “psychological” OR “psychosocial” OR “stress” OR “distress” OR “anxiety” OR “depression” OR “sexuality” OR “sexual function” OR “sexual dysfunction” OR “hot flash” OR “hot flush” OR “vaginal dryness” OR “pain” OR “fatigue” OR “sleep disturbance” OR “joint pain” OR “joint stiffness” OR “functional ability” |
| Author/Year [25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48] | Methodological Quality Rating (EPHPP) | ||||||
|---|---|---|---|---|---|---|---|
| Selection Bias | Study Design | Confounders | Blinding | Data Collection Method | Withdrawals and Dropouts | Overall | |
| Advani et al., 2017 [33] | Moderate | Strong | Strong | Weak | Strong | Strong | Moderate |
| Baker et al., 2018 [43] | Moderate | Strong | Strong | Moderate | Strong | Strong | Strong |
| Conejo et al., 2018 [47] | Moderate | Strong | Strong | Weak | Strong | Strong | Moderate |
| Crew et al., 2007 [42] | Moderate | Weak | Weak | Weak | Strong | Strong | Weak |
| de Sousa et al., 2019 [25] | Moderate | Weak | Strong | Strong | Strong | Moderate | Moderate |
| Goldberg et al., 1994 [29] | Weak | Weak | Strong | Strong | Weak | Weak | Weak |
| Henry et al., 2018 [34] | Weak | Weak | Strong | Strong | Strong | Strong | Weak |
| Hershman et al., 2015 [39] | Weak | Weak | Strong | Strong | Strong | Moderate | Weak |
| Hershman et al., 2018 [40] | Moderate | Weak | Weak | Weak | Strong | Strong | Weak |
| Heudel et al., 2019 [26] | Moderate | Strong | Strong | Strong | Strong | Strong | Strong |
| Irwin et al., 2015 [38] | Moderate | Strong | Strong | Weak | Strong | Strong | Weak |
| Keshavarzi et al., 2019 [31] | Moderate | Strong | Strong | Strong | Strong | Strong | Strong |
| Kimmick et al., 2006 [27] | Weak | Weak | Strong | Strong | Strong | Moderate | Weak |
| Mann et al., 2012 [30] | Moderate | Strong | Strong | Moderate | Strong | Strong | Strong |
| Mao et al., 2014 [46] | Weak | Strong | Strong | Weak | Strong | Strong | Weak |
| Nyrop et al., 2017 [35] | Moderate | Weak | Weak | Weak | Strong | Moderate | Weak |
| Oh et al., 2013 [41] | Moderate | Strong | Strong | Weak | Strong | Strong | Moderate |
| Pandya et al., 2000 [28] | Moderate | Strong | Strong | Strong | Strong | Moderate | Strong |
| Paulo et al., 2019 [32] | Moderate | Weak | Strong | Weak | Strong | Moderate | Weak |
| Peppone et al., 2015 [45] | Weak | Strong | Strong | Weak | Weak | Weak | Weak |
| Rogers et al., 2009 [36] | Moderate | Strong | Strong | Weak | Strong | Strong | Moderate |
| Rogers et al., 2009 [37] | Moderate | Strong | Strong | Weak | Strong | Strong | Moderate |
| Rogers et al., 2017 [48] | Weak | Strong | Strong | Moderate | Strong | Weak | Weak |
| Zhao et al., 2012 [44] | Weak | Weak | Strong | Weak | Strong | Weak | Weak |
| Author/Year/Country | Settings | Participants/Sample Size | Intervention Type | Intervention | Assessed Outcomes of Interest/Data Collection Time Points | Instruments for Outcome Assessments |
|---|---|---|---|---|---|---|
| de Sousa Vieira et al., 2019 [25]; Brazil | Not specified | Breast cancer patients (stage unknown) undergoing adjuvant hormone therapy using either tamoxifen or anastrozole. N = 40 Intervention: 20 Control: 20 Duration of adjuvant endocrine therapy undergone by subjects: All participants: At least 3 months (not specified for each group) | Pharmacological intervention | Pharmacological intervention with tablets of a medicinal plant extract (Paullinia cupana or Guarana) Intervention: Intake of tablets containing 37.5 mg of an active ingredient of guarana (PC-18) twice daily for 4 weeks. Control: Intake of placebo tablets for 4 weeks |
|
|
| Heudel et al., 2019 [26]; France | Not specified | Patients with localized breast cancer (stage unknown), receiving adjuvant endocrine therapy with tamoxifen or aromatase inhibitors N = 138 Intervention: 65 Control: 73 Duration of adjuvant endocrine therapy undergone by subjects: All participants: At least 1 month (not specified for each group) | Pharmacological intervention | Pharmacological intervention with a homeopathic medicine named Actheane® Intervention: Intake of Actheane® tablets twice a day for a period of 8–10 weeks. Control: Intake of placebo tablets, twice a day for a period of 8–10 weeks. |
|
|
| Keshavarzi et al., 2019 [31]; Iran | Local breast clinic | Patients with stage I–II breast cancer, undergoing tamoxifen therapy N = 96 Vitamin D group: 32 Vitamin E group: 32 Placebo group: 32 Duration of adjuvant endocrine therapy undergone by subjects: Vitamin D group: 23.6 ± 17.5 months Vitamin E group: 30.4 ± 21 months Control group: 16.6 ± 12.5 months | Miscellaneous intervention | Vitamin D/vitamin E vaginal suppository intervention Intervention: Participants were provided with vaginal suppositories supplemented with either 0.025 mg vitamin D or 1 mg vitamin E, and were instructed to insert one suppository into the vagina every day before bedtime, over the course of 8 weeks. Telephone reminders were given every 3 days. Control: The use of vaginal suppositories supplemented with placebo, instead of vitamin D/E vaginal suppositories. |
Data collected at:
|
|
| Paulo et al., 2019 [32]; Brazil | Not specified | Breast cancer survivors previously diagnosed with stage I–IIIA cancer, undergoing aromatase inhibitor therapy N = 36 Intervention: 18 Control: 18 Duration of adjuvant endocrine therapy undergone by subjects: Intervention group: 19.3 ± 8.3 months Control group: 17.9 ± 11.2 months | Physical activity intervention | Supervised combined exercise training intervention Intervention:
Control: Participation of 45-min sessions of stretching and relaxation exercises twice a week, over the course of 9 months. |
Data collected at:
|
|
| Baker et al., 2018 [43]; Australia | Local institution or hospital department | Breast cancer patients (stage unknown) undergoing aromatase inhibitor therapy N = 31 Intervention: 14 Control: 17 Duration of adjuvant endocrine therapy undergone by subjects: Intervention group: 19 months (median) Control group: 3 months (median) | Miscellaneous intervention | Whole body vibration intervention Intervention:
Control: Usual care |
Data collected at:
|
|
| Conejo et al., 2018 [47]; Spain | Not specified | Breast cancer survivors previously diagnosed with stage I–IIIA cancer, undergoing aromatase inhibitor therapy N = 40 Intervention: 20 Control: 20 Duration of adjuvant endocrine therapy undergone by subjects: Intervention group: 15.25 months (mean) Control group: 19.55 months (mean) | Miscellaneous intervention | Neuromuscular taping intervention Intervention:
Control: Sham neuromuscular taping over body parts where pain was felt for 7 days Provision of health advice, focusing on active lifestyles |
Data collected at:
|
|
| Henry et al., 2018 [34]; USA | Not specified | Breast cancer patients (stages I–III), receiving aromatase inhibitor therapy N = 299 Intervention: 150 Control: 149 Duration of adjuvant endocrine therapy undergone by subjects: All participants: 47.9 ± 36.3 weeks (not specified for each group) | Pharmacological intervention | Pharmacological intervention with Duloxetine Intervention: Intake of 1 capsule containing 30 mg duloxetine per day for 1 week. Intake of 2 of the capsule described above for the subsequent 11 weeks. Thereafter, patients took 1 capsule daily for one further week. Control: Intake of placebo containing sugar spheres over the schedule described above |
Data collected at:
|
|
| Hershman et al., 2018 [40]; USA | 11 Academic and community sites—sites not specified | Breast cancer patients, undergoing aromatase inhibitor therapy N = 226 Intervention: True acupuncture = 110 Control Groups: Sham Acupuncture = 59 Waiting list = 57 Duration of adjuvant endocrine therapy undergone by subjects: All participants: At least 1 month (not specified for each group) | Acupuncture intervention | Acupuncture intervention Intervention Group: 12 sessions of true acupuncture over the first 6 weeks. Each session lasted for 30-45 min. Six more weekly sessions of true acupuncture were held over the next 6 weeks. Control Group 1: Sham Acupuncture Sessions of sham acupuncture based on the schedule presented above. Control Group 2: The waitlist control group Delayed treatment using true acupuncture received by intervention group |
|
|
| Advani et al., 2017 [33]; USA | Not specified | Localized breast cancer patients (early stage), receiving adjuvant endocrine therapy with aromatase inhibitor N = 57 Control group: Usual Care Group: 21 Intervention groups: Active Group-H:18 Active Group-P:18 Duration of adjuvant endocrine therapy undergone by subjects: All participants: Less than 4 weeks (not specified for each group) | Multimodal intervention | A multimodal intervention involving sexual counseling, and use of vaginal moisturizers, lubricants, and/or dilator
Intervention:
Control: Usual Care |
Data collected at:
|
|
| Nyrop et al., 2017 [35]; USA | Participants’ home | Breast cancer survivors previously diagnosed with stage 0–III cancer, undergoing aromatase inhibitor therapy N = 62 Intervention: 31 Control: 31 Duration of adjuvant endocrine therapy undergone by subjects: All participants: 1.7 ± 1.43 years (not specified for each group) | Physical activity intervention | Home-based walking program Intervention:
Control: Wait-list control, receiving intervention after post-intervention data collection |
Data collected at:
|
|
| Rogers et al., 2017 [48]; USA | Local institutions, with home-based exercises | Breast cancer survivors (stages I–IIIA), receiving hormonal therapy N = 222 Intervention: 110 Control: 112 Duration of adjuvant endocrine therapy undergone by subjects: Not specified | Physical activity intervention | Physical activity behavior change intervention (Better Exercise Adherence after Treatment for Cancer) Intervention:
Control: Usual care |
Data collected at:
|
|
| Hershman et al., 2015 [39]; USA | Not specified | Breast cancer survivors (stages I–III), receiving adjuvant aromatase inhibitor therapy N = 262 Intervention: 131 Control: 131 Duration of adjuvant endocrine therapy undergone by subjects: Intervention group: 1.1 years (median) Control group: 1.3 years (median) | Dietary intervention | Dietary intervention with omega-3 fatty acids Intervention: Intake of 6 capsules containing 3.3 g omega-3 fatty acid (eicosapentaenoic acid and docosahexaenoic acid) per day, over a period of 24 weeks. Control: Intake of placebo capsule containing soybean oil and corn oil, 6 per day over 24 weeks. |
Data collected at:
|
|
| Irwin et al., 2015 [38], USA | Local health club and home-based | Breast cancer Survivors (stages I–III), undergoing aromatase inhibitor therapy N = 121 Intervention group = 61 Control Group = 60 Duration of adjuvant endocrine therapy undergone by subjects: Intervention group: 1.9 ± 2.9 years Control group: 1.8 ± 1.3 years | Physical activity intervention | Year-long exercise intervention Intervention Group: Participation in a supervised resistance exercise program with sessions held twice a week, and a home-based aerobic exercise program (brisk walking or stationary cycling) of 150 min per week. The program lasted for 1 year. Control Group Usual care Participants in both groups were given education booklets with information on breast cancer-related symptoms including lymphedema and fatigue |
Data collected at
|
|
| Peppone et al., 2015 [45]; USA | Community-based and group-based | Breast cancer survivors (stages 0–III) receiving either tamoxifen or aromatase inhibitor therapy N = 167 Intervention: 75 Control: 92 Duration of adjuvant endocrine therapy undergone by subjects: Not specified | Psychotherapeutic intervention | Yoga intervention Intervention: Attendance to group sessions of yoga, involving breathing and mindfulness exercises and physical alignment postures. Each session lasted 75 min, and was held twice a week over a period of 4 weeks. Control: Wait-list control, receiving standard care during the intervention period. |
Data collected at:
| Selected items from:
|
| Mao et al., 2014 [46], USA | Tertiary care academic medical center | Breast cancer patients (stages I–III), currently undergoing aromatase inhibitor therapy N = 67 Intervention = 22 Sham acupuncture control group = 22 Waitlist Control = 23 Duration of adjuvant endocrine therapy undergone by subjects: Intervention group: 26.9 ± 17.3 months Sham acupuncture control group: 19.5 ± 16.9 months Control group: 31.1 ± 22.1 months | Acupuncture intervention | Electroacupuncture (EA) intervention Intervention Undertake 30-min electroacupuncture sessions, held twice a week for 2 weeks, then weekly for 6 more weeks Sham Electroacupuncture (SA) Undertake 30-min electroacupuncture sessions, held twice a week for 2 weeks, then weekly for 6 more weeks, but with non-penetrating needles. Waitlist Control Usual care |
Data collected at:
|
|
| Oh et al., 2013 [41], Australia | Tertiary Teaching Hospital | Breast cancer patients (stages I–IIIa), undergoing aromatase inhibitor therapy N = 29 Intervention group = 14 Sham Electroacupuncture control group = 15 Duration of adjuvant endocrine therapy undergone by subjects: All participants: At least 6 months | Acupuncture intervention | Electroacupuncture (EA) intervention Intervention Group: Undertake 20-min sessions of real electroacupuncture twice weekly for 6 weeks, using acupuncture needles Control Group: Undertake 20-min sessions of sham electroacupuncture twice weekly for 6 weeks, using sham acupuncture needles that do not penetrate the skin |
Data collected at:
|
|
| Mann et al., 2012 [30]; United Kingdom | Not specified | Breast cancer survivors (stage unknown), undergoing endocrine therapy N = 96 Intervention: 47 Control: 49 Duration of adjuvant endocrine therapy undergone by subjects: Not specified | Psychotherapeutic intervention | Cognitive behavioral therapy (CBT) Intervention: Attendance to six 90-min group-based CBT sessions, held once a week, over a period of 6 weeks. These sessions included the provision of psycho-education via presentations and handouts, group discussions and homework assignments. Control: Usual care |
Data collected at:
|
|
| Zhao et al., 2012 [44]; China | Not specified | Breast cancer survivors previously diagnosed with stage I–IIIA cancer, having completed or undergoing endocrine therapy N = 48 Intervention: 25 Control: 23 Duration of adjuvant endocrine therapy undergone by subjects: All participants: 6 months–5 years (not specified for each group) | Pharmacological intervention | Pharmacological intervention with spore powder of G. lucidum Intervention: Intake of 1000 mg spore powder of G. lucidum three times a day for 4 weeks Control: Intake of placebo, three times a day for 4 weeks |
Data collected at:
|
|
| Rogers et al., 2009 [36]; USA | Not specified | Breast cancer survivors (stages I–IIIA), currently on aromatase inhibitor therapy or estrogen receptor modulator therapy N = 41 Intervention: 21 Control: 20 Duration of adjuvant endocrine therapy undergone by subjects: All participants: 18 ± 17 months (not specified for each group) | Physical activity intervention | Physical activity behavior change intervention (The BEAT Cancer Program) Intervention:
Control: Usual care |
Data collected at:
|
|
| Rogers et al., 2009 [37]; USA | Not specified | Same as Rogers et al, 2009 [36] | Physical activity intervention | Same as Rogers et al., 2009 [36] |
Data collected at:
|
|
| Crew et al., 2007 [42]; USA | Not specified | Breast cancer survivors (stages I–IIIa), undertaking aromatase inhibitor therapy N = 21 Intervention: Not mentioned Control: Not mentioned Duration of adjuvant endocrine therapy undergone by subjects: All participants: At least 6 months (not specified for each group) | Acupuncture intervention | Acupuncture intervention Intervention: Acupuncture session lasting 30 min, performed two times a week for six weeks. Control: Wait-list control |
Data collected at:
|
|
| Kimmick et al., 2006 [27]; USA | Not specified | Breast cancer survivors (stages 0–IIIB), receiving tamoxifen therapy N = 62 Intervention: 33 Control: 29 Duration of adjuvant endocrine therapy undergone by subjects: Not specified | Pharmacological intervention (a crossover trial) | Pharmacological intervention with the antidepressant sertraline Intervention: Intake of 50 mg sertraline per day, over a period of 6 weeks. Intervention participants then took the placebo tablets per day for the next 6 weeks. Control: Intake of placebo tablet per day, over a period of 6 weeks. Control participants then took 50 mg sertraline per day for the next 6 weeks. |
Data collected at:
|
|
| Pandya et al., 2000 [28]; USA | University of Rochester Cancer Centre | Breast cancer survivors (stage unknown), receiving adjuvant tamoxifen therapy N = 198 Intervention: 99 Control: 99 Duration of adjuvant endocrine therapy undergone by subjects: All participants: At 1 month (not specified for each group) | Pharmacological intervention | Pharmacological intervention with clonidine Intervention: Intake of 0.1 mg oral clonidine, once daily, for a period of 8 weeks. Control: Intake of 0.1 mg placebo, once daily, for a period of 8 weeks. |
Data collected at:
|
|
| Goldberg et al., 1994 [29]; USA | Not specified | Breast cancer patients (stage unknown), receiving tamoxifen therapy N = 110 Intervention: 55 Control: 55 Duration of adjuvant endocrine therapy undergone by subjects: Not specified | Pharmacological intervention | Pharmacological intervention with transdermal clonidine Intervention: Administered transdermal clonidine patch (equivalent to the oral dose of 0.1 mg of the drug) daily for a period of 4 weeks, then intervention participants were administered the placebo transdermally daily for the next 4 weeks. Control: Administered the placebo patch to be used daily for a period of 4 weeks, then control participants were administered the transdermal clonidine patch (equivalent to the oral dose of 0.1 mg of the drug), used daily for the next 4 weeks. |
Data collected at:
|
|
| Menopausal Symptom/Issue | Intervention Type | Intervention Name | Major Findings on Intervention Effects on Symptom * | Reference |
|---|---|---|---|---|
| Hot flashes | Pharmacological intervention | Pharmacological intervention with tablets of a medicinal plant extract (Paullinia cupana or Guarana) |
| de Sousa Vieira et al., 2019 [25] |
| Pharmacological intervention with a homeopathic medicine named Actheane® | (T1: 4 weeks after randomization; T2: 8 weeks after randomization)
| Heudel et al., 2019 [26] | ||
| Pharmacological intervention with the antidepressant sertraline | Before cross-over at 6 weeks after start of intervention (T1)
| Kimmick et al., 2006 [27] | ||
| Pharmacological intervention with clonidine | (T1: 4 weeks after randomization; T2: 8 weeks after randomization; T3: 12 weeks after randomization)
| Pandya et al., 2000 [28] | ||
| Pharmacological intervention with transdermal clonidine |
| Goldberg et al., 1994 [29] | ||
| Psychotherapeutic intervention | Cognitive behavioral therapy | (T1: 9 weeks after randomization; T2: 26 weeks after randomization)
| Mann et al., 2012 [30] | |
| Night sweats | Psychotherapeutic intervention | Cognitive behavioral therapy | (T1: 9 weeks after randomization; T2: 26 weeks after randomization)
| Mann et al., 2012 [30] |
| Vaginal atrophy | Miscellaneous intervention | Vitamin D/vitamin E vaginal suppository intervention | (T1: 2 weeks after start of intervention; T2: 4 weeks after start of intervention; T3: 8 weeks after start of intervention) Within-group comparison
| Keshavarzi et al., 2019 [31] |
| Sexual issues | Pharmacological intervention | Pharmacological intervention with tablets of a medicinal plant extract (Paullinia cupana or Guarana) |
| de Sousa Vieira et al., 2019 [25] |
| Physical activity intervention | Supervised combined exercise training intervention |
| Paulo et al., 2019 [32] | |
| Multimodal intervention | A multimodal intervention involving sexual counseling, and use of vaginal moisturizers, lubricants, and/or dilator | (T1: 6 months after randomization; T2: 12 months after randomization)
| Advani et al., 2017 [33] |
| Intervention Type | Intervention Name | Major Findings on Intervention Effects on Symptom * | Reference |
|---|---|---|---|
| Pharmacological intervention | Pharmacological intervention with Duloxetine | (T1: 2 weeks after randomization; T2: 6 weeks after randomization; T3:12 weeks after randomization; T4: 24 weeks after randomization)
| Henry et al., 2018 [34] |
| Physical activity intervention | Home-based walking program | (T1: immediate post-intervention; T2: 6 months post-intervention) Within-group comparisons Intervention group
| Nyrop et al., 2017 [35] |
| Physical activity behavior change intervention (The BEAT Cancer Program)—pilot study | (T1: immediate post-intervention; T2: 3 months post-intervention)
| Rogers et al., 2009 [36] Rogers et al., 2009 [37] | |
| Year-long exercise intervention | (T1: 3 months after randomization; T2: 6 months after randomization; T3: 9 months after randomization; T4: 12 months after randomization)
| Irwin et al., 2015 [38] | |
| Dietary intervention | Dietary intervention with omega-3 fatty acids | (T1: Week 6 of intervention; T2: Week 12 of intervention; T3: Week 24 of intervention/immediate post-intervention) Within-group comparisons
Between-group comparisons
| Hershman et al., 2015 [39] |
| Acupuncture intervention | Acupuncture intervention | (T1: 6 weeks after randomization; T2: 12 weeks after randomization) Worst joint pain score
Average joint pain
| Hershman et al, 2018 [40] |
| Electro-acupuncture intervention | (T1: Immediate post-intervention; T2: 6 months post-intervention)
| Oh et al., 2013 [41] | |
| Acupuncture intervention | Within-group comparisons
| Crew et al., 2007 [42] | |
| Miscellaneous intervention | Whole body vibration intervention | No significant differences in the joint pain levels (p = 0.334), joint stiffness levels (p = 0.224) or level of physical dysfunction of joints (p = 0.063) of participants between groups at post-intervention. | Baker et al., 2018 [43] |
| Intervention Type | Intervention Name | Major Findings on Intervention Effects on Fatigue * | Reference |
|---|---|---|---|
| Pharmacological intervention | Pharmacological intervention with spore powder of G. lucidum |
| Zhao et al., 2012 [44] |
| Physical activity intervention | Supervised combined exercise training intervention |
| Paulo et al., 2019 [32] |
| Home-based walking program | (T1: immediate post-intervention; T2: 6 months post-intervention) Within-group comparisons
| Nyrop et al., 2017 [35] | |
| Psychotherapeutic intervention | Yoga intervention |
| Peppone et al., 2015 [45] |
| Acupuncture intervention | Electro-acupuncture intervention | (T1: Week 2 of intervention; T2: Week 4 of intervention; T3: Week 8 of intervention/immediate post-intervention; T4: 4 weeks post-intervention)
| Mao et al., 2014 [46] |
| Miscellaneous intervention | Whole body vibration intervention |
| Baker et al., 2018 [43] |
| Neuromuscular taping intervention | (T1: 1 week after start of intervention/immediate post-intervention; T2: 5 weeks after start of intervention/4 weeks post-intervention) Within-group comparisons Intervention group
| Conejo et al., 2018 [47] |
| Intervention Type | Intervention Name | Major Findings on Intervention Effects on Sleep Disturbance * | Reference |
|---|---|---|---|
| Physical activity intervention | Supervised combined exercise training intervention |
| Paulo et al., 2019 [32] |
| Physical activity behavior change intervention (The BEAT Cancer Program) | (T1: immediate post-intervention; T2: 3 months post-intervention) Within-group comparisons Intervention group
| Rogers et al., 2017 [48] | |
| Physical activity behavior change intervention (The BEAT Cancer Program)—pilot study | (T1: immediate post-intervention; T2: 3 months post-intervention)
| Rogers et al., 2009 [36] Rogers et al., 2009 [37] | |
| Psychotherapeutic intervention | Cognitive behavioral therapy | (T1: 9 weeks after randomization; T2: 26 weeks after randomization)
| Mann et al., 2012 [30] |
| Acupuncture intervention | Electro-acupuncture intervention | (T1: Week 2 of intervention; T2: Week 4 of intervention; T3: Week 8 of intervention/immediate post-intervention; T4: 4 weeks post-intervention)
| Mao et al., 2014 [46] |
| Miscellaneous intervention | Neuromuscular taping intervention | (T1: 1 week after start of intervention/immediate post-intervention; T2: 5 weeks after start of intervention/4 weeks post-intervention) Within-group comparisons Intervention group
Between-group comparisons
| Conejo et al., 2018 [47] |
| Outcome | Intervention Type | Intervention Name | Major Findings on Intervention Effects on QOL/Functional Ability * | Reference |
|---|---|---|---|---|
| QOL | Pharmacological intervention | Pharmacological intervention with tablets of a medicinal plant extract (Paullinia cupana or Guarana) |
| de Sousa Vieira et al., 2019 [25] |
| Pharmacological intervention with Duloxetine |
| Henry et al., 2018 [34] | ||
| Pharmacological intervention with spore powder of G. lucidum |
| Zhao et al., 2012 [44] | ||
| Pharmacological intervention with the antidepressant sertraline | (T1: Before cross-over at 6 weeks after start of intervention; T2: After cross-over at 12 weeks after start of intervention)
| Kimmick et al., 2006 [27] | ||
| Pharmacological intervention with clonidine | (T1: 4 weeks after randomization; T2: 8 weeks after randomization; T3: 12 weeks after randomization)
| Pandya et al., 2000 [28] | ||
| Physical activity intervention | Supervised combined exercise training intervention | (T1: 12 weeks after start of intervention; T2: 24 weeks after start of intervention; T3: 36 weeks after start of intervention)
| Paulo et al., 2019 [32] | |
| Home-based walking program | (T1: immediate post-intervention; T2: 6 weeks post-intervention) Within-group comparisons Intervention group
Between-group comparisons
| Nyrop et al., 2017 [35] | ||
| Physical activity behavior change intervention (The BEAT Cancer Program)—pilot study | (T1: immediate post-intervention; T2: 3 months post-intervention)
| Rogers et al., 2009 [36] Rogers et al., 2009 [37] | ||
| Psychotherapeutic intervention | Cognitive behavioral therapy | (T1: 9 weeks after randomization; T2: 26 weeks after randomization)
| Mann et al., 2012 [30] | |
| Acupuncture intervention | Electro-acupuncture intervention | (T1: Immediate post-intervention; T2: 6 months post-intervention)
| Oh et al., 2013 [41] | |
| Acupuncture intervention | Within-group comparison
| Crew et al., 2007 [42] | ||
| Miscellaneous intervention | Neuromuscular taping intervention | (T1: 1 week after start of intervention/immediate post-intervention; T2: 5 weeks after start of intervention/4 weeks post-intervention) Within-group comparisons Intervention group
No significant improvement was observed for all QOL domains at T1 and T2 (p ≥ 0.41). Between-group comparisons
| Conejo et al., 2018 [47] | |
| Functional ability | Physical activity intervention | Home-based walking program |
| Nyrop et al., 2017 [35] |
| Miscellaneous intervention | Whole body vibration intervention |
| Baker et al., 2018 [43] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, C.W.H.; Tai, D.; Kwong, S.; Chow, K.M.; Chan, D.N.S.; Law, B.M.H. The Effects of Pharmacological and Non-Pharmacological Interventions on Symptom Management and Quality of Life among Breast Cancer Survivors Undergoing Adjuvant Endocrine Therapy: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 2950. https://doi.org/10.3390/ijerph17082950
Chan CWH, Tai D, Kwong S, Chow KM, Chan DNS, Law BMH. The Effects of Pharmacological and Non-Pharmacological Interventions on Symptom Management and Quality of Life among Breast Cancer Survivors Undergoing Adjuvant Endocrine Therapy: A Systematic Review. International Journal of Environmental Research and Public Health. 2020; 17(8):2950. https://doi.org/10.3390/ijerph17082950
Chicago/Turabian StyleChan, Carmen W.H., Daria Tai, Stephanie Kwong, Ka Ming Chow, Dorothy N.S. Chan, and Bernard M.H. Law. 2020. "The Effects of Pharmacological and Non-Pharmacological Interventions on Symptom Management and Quality of Life among Breast Cancer Survivors Undergoing Adjuvant Endocrine Therapy: A Systematic Review" International Journal of Environmental Research and Public Health 17, no. 8: 2950. https://doi.org/10.3390/ijerph17082950