Process Evaluation of a Nutrition and Lifestyle Behavior Peer Support Program for Adults with Metabolic Syndrome



Abstract
:1. Introduction
2. Materials and Methods
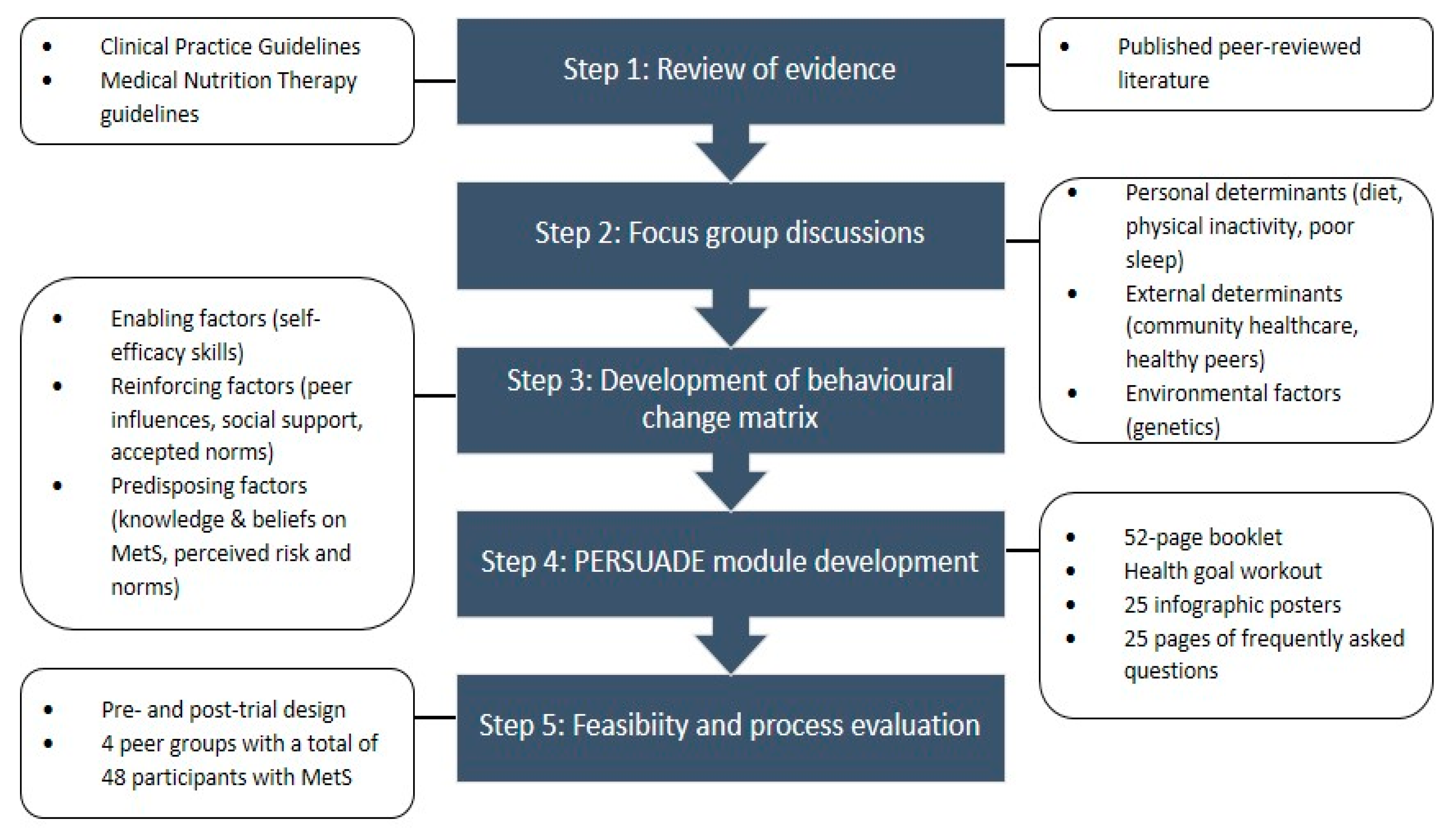
2.1. Step 1: Review of Evidence
2.2. Step 2: Focus Group Discussions
2.3. Step 3: Development of Behavioral Change Matrix
2.4. Step 4: PERSUADE Module Development
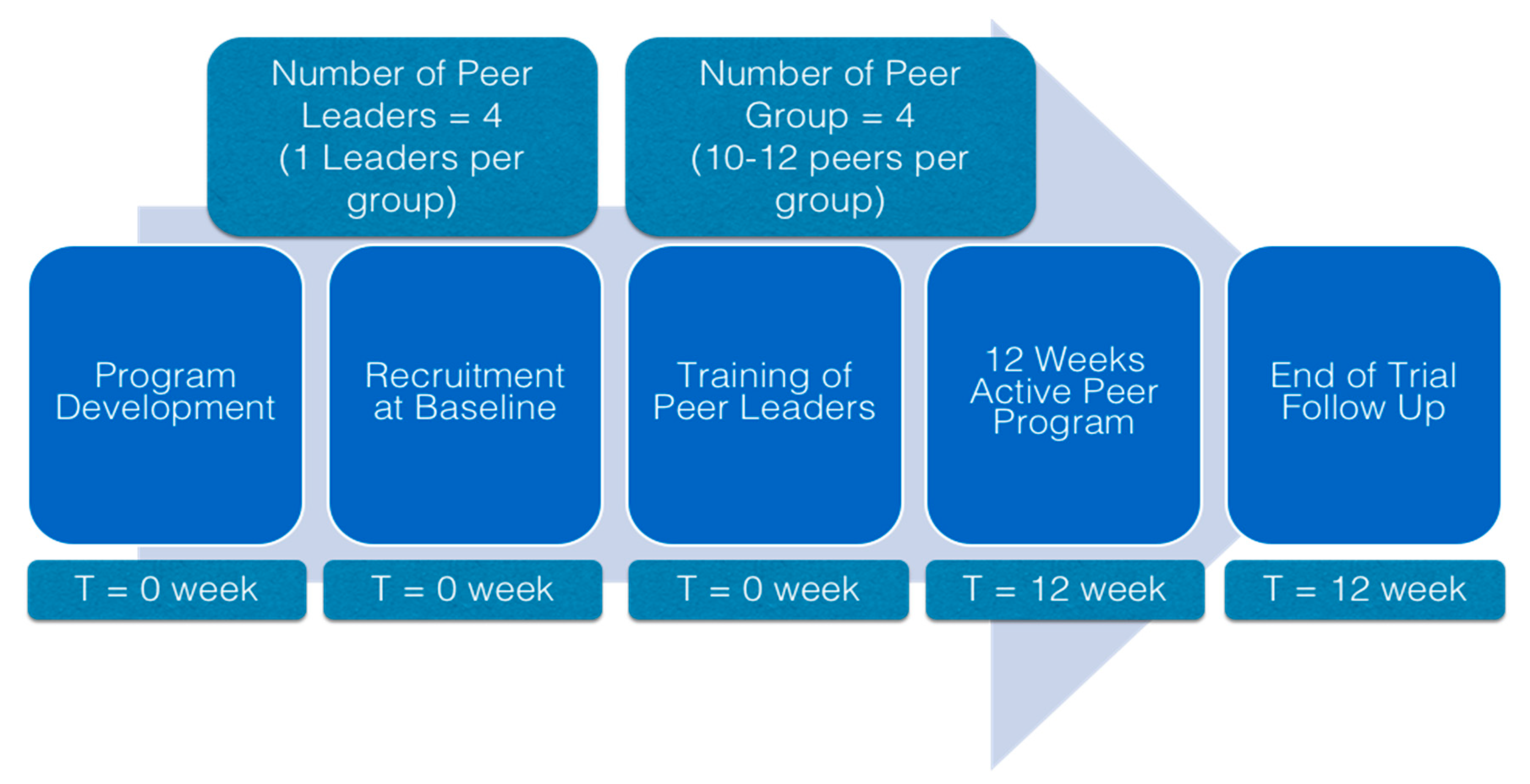
2.5. Step 5: Feasibility and Process Evaluation
2.5.1. Feasibility Trial
2.5.2. Process Evaluation
2.5.3. Statistical Analysis
3. Results
3.1. Study Participants
3.2. Changes in Anthropometric Measures and Metabolic Parameters
3.3. Process Evaluation
3.4. Correlation between Satisfaction and Study Outcomes
4. Discussion
4.1. Outcome of the Feasibility Trial and Process Evaluation
4.1.1. Attention to Emotions
4.1.2. Use of Theoretical Model
4.1.3. Assistance in Daily Health Management
4.1.4. Ongoing Proactive Contact
4.2. Limitation
4.3. Recommendation for Future Research
- Emphasis on modifiable nutrition and lifestyle behavior (dietary pattern, dietary timing, diet variety, diet quality, sleeping pattern, smoking cessation, and physical activity programs).
- Increase the study period from 3 months to a year to promote permanent lifestyle changes.
- Incorporate technology in monitoring behavioral changes. Improve the rate of acceptance and adherence by including visually possible changes and a tracking system.
- Improve peer leader training to ensure they are ready and inspiring.
- Develop a stratified community-based sampling strategy in improve collective changes.
- Ensure that each peer group is made up of peers with similar socioeconomic background to ensure their timely and relevant discussion throughout the period.
- Conduct a needs assessment to gauge the societal or cultural needs of a community before adapting PERSUADE.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C., Jr.; et al. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institute for Public Health. National Health and Morbidity Survey 2015 (NHMS 2015). Vol. II: Non-Communicable Diseases, Risk Factors & Other Health Problems; Ministry of Health Malaysia: Kuala Lumpur, Malaysia, 2015.
- Ghee, L.K.; Kooi, C.W. A review of metabolic syndrome research in Malaysia. Med. J. Malaysia 2016, 71, 20–28. [Google Scholar]
- Brown, T.; Smith, S.; Bhopal, R.; Kasim, A.; Summerbell, C. Diet and physical activity interventions to prevent or treat obesity in South Asian children and adults: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2015, 12, 566–594. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohamad Nor, N.S.; Ambak, R.; Mohd Zaki, N.; Abdul Aziz, N.S.; Cheong, S.M.; Abd Razak, M.A.; Yusof, M.; Ahmad, M.H.; Baharuddin, A.; Megat Radzi, M.R.; et al. An update on obesity research pattern among adults in Malaysia: A scoping review. BMC Womens Health 2018, 18 (Suppl. 1), 114. [Google Scholar] [CrossRef]
- Iqbal, S.P.; Ramadas, A.; Fatt, Q.K.; Shin, H.L.; Onn, W.Y.; Kadir, K.A. Relationship of sociodemographic and lifestyle factors and diet habits with metabolic syndrome (MetS) among three ethnic groups of the Malaysian population. PLoS ONE 2020, 15, e0224054. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodriguez-Monforte, M.; Sanchez, E.; Barrio, F.; Costa, B.; Flores-Mateo, G. Metabolic syndrome and dietary patterns: A systematic review and meta-analysis of observational studies. Eur. J. Nutr. 2017, 56, 925–947. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, R.G.D.; Guedes, D.P. Physical activity, sedentary behavior, cardiorespiratory fitness and metabolic syndrome in adolescents: Systematic review and meta-analysis of observational evidence. PLoS ONE 2016, 11, e0168503. [Google Scholar] [CrossRef]
- Ju, S.Y.; Choi, W.S. Sleep duration and metabolic syndrome in adult populations: A meta-analysis of observational studies. Nutr. Diabetes 2013, 3. [Google Scholar] [CrossRef]
- Chee Huei, P.; Saad, H.A.; Barakatun Nisak, M.Y.; Mohd Nasir, M.T. Effectiveness of physical activity intervention among government employees with metabolic syndrome. J. Exerc. Sci. Fit. 2017, 15, 55–62. [Google Scholar] [CrossRef]
- Haw, J.S.; Galaviz, K.I.; Straus, A.N.; Kowalski, A.J.; Magee, M.J.; Weber, M.B.; Wei, J.; Narayan, K.M.V.; Ali, M.K. Long-term sustainability of diabetes prevention approaches: A systematic review and meta-analysis of randomized clinical trials. JAMA Intern. Med. 2017, 177, 1808–1817. [Google Scholar] [CrossRef]
- Pritchett, A.M.; Foreyt, J.P.; Mann, D.L. Treatment of the metabolic syndrome: The impact of lifestyle modification. Curr. Atheroscler. Rep. 2005, 7, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Bourke, L.; Sohanpal, R.; Nanton, V.; Crank, H.; Rosario, D.J.; Saxton, J.M. A qualitative study evaluating experiences of a lifestyle intervention in men with prostate cancer undergoing androgen suppression therapy. Trials 2012, 13, 208. [Google Scholar] [CrossRef] [PubMed]
- Cormie, P.; Turner, B.; Kaczmarek, E.; Drake, D.; Chambers, S.K. A Qualitative exploration of the experience of men with prostate cancer involved in supervised exercise programs. Oncol. Nurs Forum 2015, 42, 24–32. [Google Scholar] [CrossRef] [Green Version]
- Bastawrous, M.M.; Gignac, M.A.M.; Kapral, M.; Cameron, J.I. When daughters become caregivers to a parent who has suffered a stroke: A qualitative exploration of how the parent-child relationship influences caregiver wellbeing. Cerebrovasc. Dis. 2011, 31, 188–189. [Google Scholar]
- Fisher, E.B.; Ballesteros, J.; Bhushan, N.; Coufal, M.M.; Kowitt, S.D.; McDonough, A.M.; Parada, H.; Robinette, J.B.; Sokol, R.L.; Tang, P.Y.; et al. Key features of peer support in chronic disease prevention and management. Health Aff. 2015, 34, 1523–1530. [Google Scholar] [CrossRef]
- Leahey, T.M.; Kumar, R.; Weinberg, B.M.; Wing, R.R. Teammates and social influence affect weight loss outcomes in a team-based weight loss competition. Obesity 2012, 20, 1413–1418. [Google Scholar] [CrossRef] [Green Version]
- Piatt, G.A.; Seidel, M.C.; Powell, R.; Zgibor, J.C. The Effect of community-based peer support in achieving and maintaining weight loss following lifestyle intervention. Diabetes 2012, 61, A89. [Google Scholar]
- Odgers-Jewell, K.; Ball, L.E.; Kelly, J.T.; Isenring, E.A.; Reidlinger, D.P.; Thomas, R. Effectiveness of group-based self-management education for individuals with type 2 diabetes: A systematic review with meta-analyses and meta-regression. Diabet. Med. 2017, 34, 1027–1039. [Google Scholar] [CrossRef]
- Krishnamoorthy, Y.; Sakthivel, M.; Sarveswaran, G.; Eliyas, S.K. Effectiveness of peer led intervention in improvement of clinical outcomes among diabetes mellitus and hypertension patients- A systematic review and meta-analysis. Prim. Care Diabetes 2019, 13, 158–169. [Google Scholar] [CrossRef]
- Lee, M.K.; Suh, S.-R. Effects of peer-led interventions for patients with cancer: A meta-analysis. Oncol. Nurs Forum 2018, 45, 217–236. [Google Scholar] [CrossRef]
- Ministry of Health. National Strategic Plan for Non-Communicable Disease (NSP-NCD) 2010–2014; Ministry of Health: Kuala Lumpur, Malaysia, 2010.
- National Coordinating Committee on Food and Nutrition. Malaysian Dietary Guidelines; Ministry of Health: Putrajaya, Malaysia, 2010.
- Ministry of Health. Clinical Practice Guidelines: Primary & Secondary Prevention of Cardiovascular Disease; Ministry of Health: Putrajaya, Malaysia, 2017.
- Ministry of Health. Clinical Practice Guidelines: Management of Type 2 Diabetes Mellitus, 5th ed.; Ministry of Health: Putrajaya, Malaysia, 2015.
- Ministry of Health. Clinical Practice Guidelines: Management of Obesity; Ministry of Health: Putrajaya, Malaysia, 2004.
- Ministry of Health. Clinical Practice Guidelines: Management of Dyslipidaemia; Ministry of Health: Kuala Lumpur, Malaysia, 2017.
- Ministry of Health. Clinical Practice Guidelines: Management of Hypertension; Ministry of Health: Putrajaya, Malaysia, 2013.
- Malaysian Dietitians’ Association. Malaysian Medical Nutrition Therapy for Type 2 Diabetes; Malaysian Dietitians’ Association: Kuala Lumpur, Malaysia, 2005. [Google Scholar]
- Malaysian Dietitians’ Association. Medical Nutrition Therapy for Hyperlipidemia; Malaysian Dietitians’ Association: Kuala Lumpur, Malaysia, 2005. [Google Scholar]
- Malaysian Dietitians’ Association. Medical Nutrition Therapy for Hypertension; Malaysian Dietitians’ Association: Kuala Lumpur, Malaysia, 2005. [Google Scholar]
- Bassi, N.; Karagodin, I.; Wang, S.; Vassallo, P.; Priyanath, A.; Massaro, E.; Stone, N.J. Lifestyle modification for metabolic syndrome: A systematic review. Am. J. Med. 2014, 127, 1242.e1-10. [Google Scholar] [CrossRef] [PubMed]
- Ricanati, E.H.W.; Golubic, M.; Yang, D.S.; Saager, L.; Mascha, E.J.; Roizen, M.F. Mitigating preventable chronic disease: Progress report of the Cleveland Clinic’s Lifestyle 180 program. Nutr. Metab. 2011, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosenstock, I.M. The Health Belief Model: Explaining health behavior through expectancies. In Health Behavior and Health Education: Theory, Research, and Practice; Glanz, K., Lewis, F.M., Rimer, B.K., Eds.; Jossey-Bass: San Francisco, CA, USA, 1990. [Google Scholar]
- Wdowik, M.J.; Kendall, P.A.; Harris, M.A.; Auld, G. Expanded Health Belief Model predicts diabetes self-management in college students. J. Nutr. Educ. 2001, 33, 17–23. [Google Scholar] [CrossRef]
- Ramli, A.S.; Daher, A.M.; Nor-Ashikin, M.N.K.; Mat-Nasir, N.; Ng, K.K.; Miskan, M.; Ambiga, K.S.; Ariffin, F.; Mazapuspavina, M.Y.; Abdul-Razak, S.; et al. JIS definition identified more Malaysian adults with metabolic syndrome compared to the NCEP-ATP III and IDF Criteria. Biomed Res. Int. 2013, 2013, 760963. [Google Scholar] [CrossRef]
- World Health Organization. Report on a WHO Consultation on the Epidemiology of Obesity; World Health Organization: Warsaw, Poland, 1987. [Google Scholar]
- Lin, C.H.; Chiang, S.L.; Tzeng, W.C.; Chiang, L.C. Systematic review of impact of lifestyle-modification programs on metabolic risks and patient-reported outcomes in adults with metabolic syndrome. Worldviews Evid. Based Nurs. 2014, 11, 361–368. [Google Scholar] [CrossRef]
- Berezina, A.; Belyaeva, O.; Berkovich, O.; Baranova, E.; Shlyakhto, E. Comparative effectiveness of weight loss interventions and prevention of cardiovascular disease in patients with abdominal obesity. Eur. Heart J. 2013, 34, 146–147. [Google Scholar] [CrossRef] [Green Version]
- Su, T.T.; Majid, H.A.; Nahar, A.M.; Azizan, N.A.; Hairi, F.M.; Thangiah, N.; Dahlui, M.; Bulgiba, A.; Murray, L.J. The effectiveness of a life style modification and peer support home blood pressure monitoring in control of hypertension: Protocol for a cluster randomized controlled trial. BMC Public Health 2014, 14 (Suppl. 3), S4. [Google Scholar] [CrossRef] [Green Version]
- Khan, F.; Pathan, F.; Huda, N.; Saleh, F. Effectiveness of diabetes education on improving glycaemic achievement by professionals versus peers. Diabetologia 2011, 54, S34. [Google Scholar]
- Guenther, S.; Shadbolt, N.; Roberts, C.; Clark, T. Evaluating peer teaching about chronic disease. Clin. Teach. 2014, 11, 541–545. [Google Scholar] [CrossRef]
- Doull, M.; O’Connor, A.M.; Welch, V.; Tugwell, P.; Wells, G.A. Peer support strategies for improving the health and well-being of individuals with chronic diseases. Cochrane Database Syst. Rev. 2017, 2017, CD005352. [Google Scholar] [CrossRef]
- Fisher, E.B.; Ayala, G.X.; Ibarra, L.; Cherrington, A.L.; Elder, J.P.; Tang, T.S.; Heisler, M.; Safford, M.M.; Simmons, D. Contributions of peer support to health, health care, and prevention: Papers from Peers for Progress. Ann. Fam. Med. 2015, 13, S2–S8. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Behavioral Objectives | Behavioral Determinants | ||
|---|---|---|---|
| Knowledge | Perceived Benefit | Self-Efficacy Skills | |
|
|
|
|
| Components | Scoring Statement | Maximum Score a | Cronbach Alpha (α) |
|---|---|---|---|
| Program adherence |
| 12 | n/a |
| Content satisfaction |
| 30 | 0.921 |
| |||
| |||
| |||
| |||
| |||
| Peer leadership |
| 20 | 0.898 |
| |||
| |||
|
| Baseline | Post-Intervention | P | |
|---|---|---|---|
| Median (IQR) | Median (IQR) | ||
| Body mass index (kg/m2) | 25.62 (5.16) | 24.99 (4.75) | <0.001 ** |
| Waist circumference (cm) | 91.75 (11.40) | 91.25 (11.80) | <0.001 ** |
| Body fat (%) | 28.75 (7.80) | 28.00 (8.40) | 0.060 |
| Systolic blood pressure (mmHg) | 134.5 (23.00) | 128.5 (22.00) | 0.001 * |
| Diastolic blood pressure (mmHg) | 80.0 (17.00) | 81.0 (15.00) | 0.188 |
| Fasting blood glucose (mmol/L) | 8.15 (3.00) | 7.50 (2.80) | <0.001 ** |
| Triglyceride (mmol/L) | 2.71 (0.52) | 1.81 (0.51) | <0.001 ** |
| High-density lipoprotein cholesterol (mmol/L) | 1.11 (0.48) | 1.45 (0.54) | <0.001 ** |
| Changes in Measures | Content | Peer Leadership |
|---|---|---|
| (Baseline Post Intervention) | ρ | ρ |
| Body mass index (kg/m2) | −0.187 | −0.047 |
| Waist circumference (cm) | −0.255 | −0.181 |
| Body fat (%) | 0.348 * | −0.251 |
| Systolic blood pressure (mmHg) | 0.098 | 0.224 |
| Diastolic blood pressure (mmHg) | 0.029 | 0.034 |
| Fasting blood glucose (mmol/L) | 0.026 | 0.011 |
| Triglyceride (mmol/L) | 0.431 * | 0.363 * |
| High-density lipoprotein cholesterol (mmol/L) | 0.004 | 0.073 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mahadzir, M.D.A.; Quek, K.F.; Ramadas, A. Process Evaluation of a Nutrition and Lifestyle Behavior Peer Support Program for Adults with Metabolic Syndrome. Int. J. Environ. Res. Public Health 2020, 17, 2641. https://doi.org/10.3390/ijerph17082641
Mahadzir MDA, Quek KF, Ramadas A. Process Evaluation of a Nutrition and Lifestyle Behavior Peer Support Program for Adults with Metabolic Syndrome. International Journal of Environmental Research and Public Health. 2020; 17(8):2641. https://doi.org/10.3390/ijerph17082641
Chicago/Turabian StyleMahadzir, Muhammad Daniel Azlan, Kia Fatt Quek, and Amutha Ramadas. 2020. "Process Evaluation of a Nutrition and Lifestyle Behavior Peer Support Program for Adults with Metabolic Syndrome" International Journal of Environmental Research and Public Health 17, no. 8: 2641. https://doi.org/10.3390/ijerph17082641