Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience on Implant Placement Accuracy and Operating Time. An in Vitro Study

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
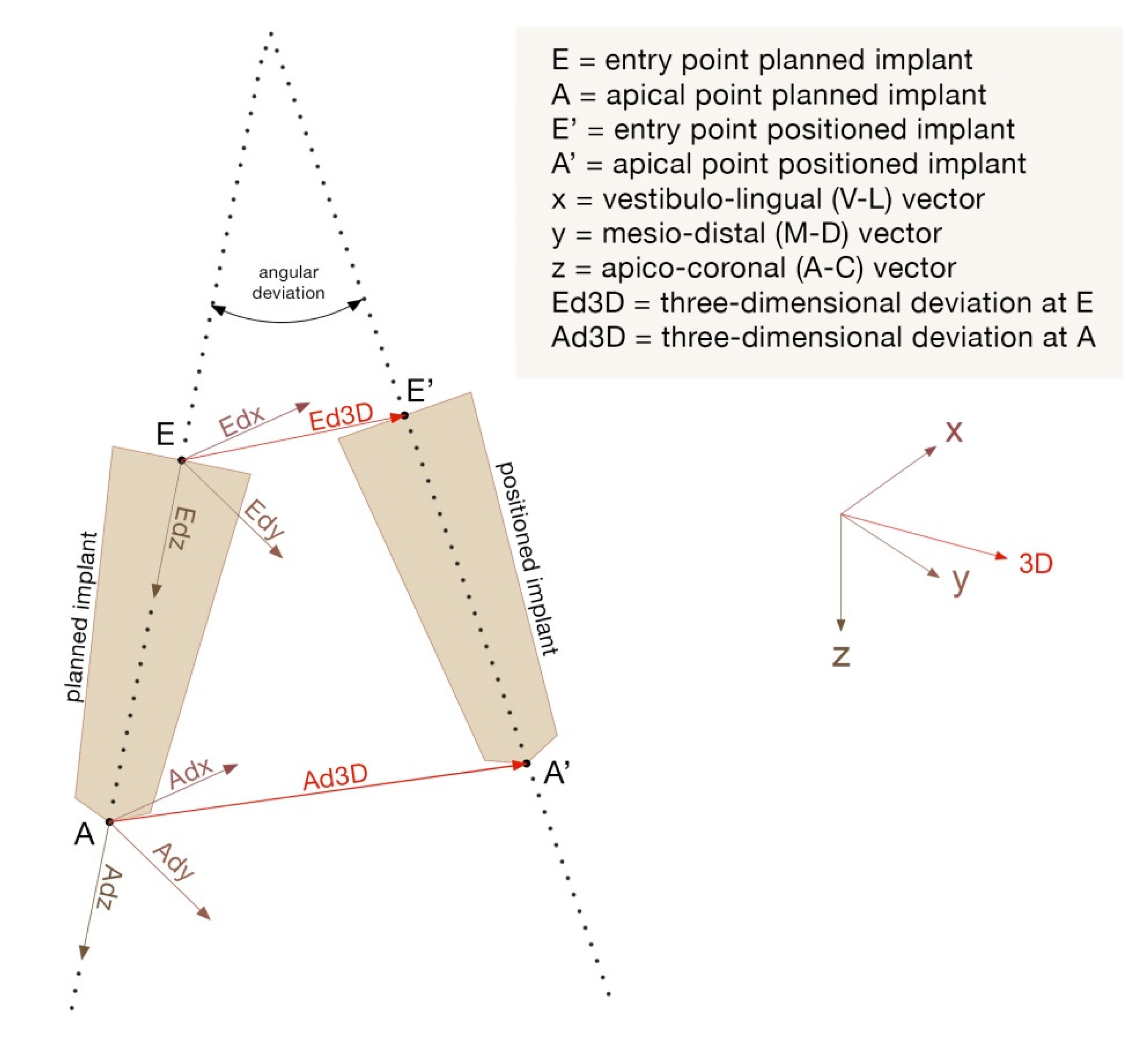
2.1. Outcome Assessment
2.2. Statistical Analysis
3. Results
3.1. Accuracy
3.2. Drilling Time
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hultin, M.; Svensson, K.G.; Trulsson, M. Clinical advantages of computer-guided implant placement: A systematic review. Clin. Oral Implants Res. 2012, 23, 124–135. [Google Scholar] [CrossRef] [PubMed]
- Vercruyssen, M.; Van de Wiele, G.; Teughels, W.; Naert, I.; Jacobs, R.; Quirynen, M. Implant- and patient-centred outcomes of guided surgery, a 1-year follow-up: An RCT comparing guided surgery with conventional implant placement. J. Clin. Periodontol. 2014, 41, 1154–1160. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Emery, R.W.; Cullum, D.R.; Sheikh, A. Implant placement is more accurate using dynamic navigation. J. Oral Maxillofac. Surg. 2017, 75, 1377–1386. [Google Scholar] [CrossRef] [PubMed]
- Colombo, M.; Mangano, C.; Mijiritsky, E.; Krebs, M.; Hauschild, U.; Fortin, T. Clinical applications and effectiveness of guided implant surgery: A critical review based on randomized controlled trials. BMC Oral Health 2017, 17, 150. [Google Scholar] [CrossRef] [PubMed]
- Block, M.S.; Emery, R.W. Static or Dynamic Navigation for Implant Placement-Choosing the Method of Guidance. J. Oral Maxillofac. Surg. 2016, 74, 269–277. [Google Scholar] [CrossRef]
- Bover-Ramos, F.; Viña-Almunia, J.; Cervera-Ballester, J.; Peñarrocha-Diago, M.; García-Mira, B. Accuracy of Implant Placement with Computer-Guided Surgery: A Systematic Review and Meta-Analysis Comparing Cadaver, Clinical, and In Vitro Studies. Int. J. Oral Maxillofac. Implant. 2018, 33, 101–115. [Google Scholar] [CrossRef] [PubMed]
- Stefanelli, L.V.; DeGroot, B.S.; Lipton, D.I.; Mandelaris, G.A. Accuracy of a Dynamic Dental Implant Navigation System in a Private Practice. Int. J. Oral Maxillofac. Implant. 2019, 34, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Cassetta, M.; Bellardini, M. How much does experience in guided implant surgery play a role in accuracy? A randomized controlled pilot study. Oral Maxillofac. Surg. 2017, 46, 922–930. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Leesungbok, R.; Cui, T.; Lee, S.W.; Ahn, S.J. Reliability of a CAD/CAM Surgical Guide for Implant Placement: An In Vitro Comparison of Surgeons’ Experience Levels and Implant Sites. Int. J. Prosthodont. 2017, 30, 367–369. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scherer, U.; Stoetzer, M.; Ruecker, M.; Gellrich, N.C.; von See, C. Template-guided vs. non-guided drilling in site preparation of dental implants. Clin. Oral Investig. 2015, 19, 1339–1346. [Google Scholar] [CrossRef] [PubMed]
- Jorba-García, A.; Figueiredo, R.; González-Barnadas, A.; Camps-Font, O.; Valmaseda-Castellón, E. Accuracy and the role of experience in dynamic computer guided dental implant surgery: An in-vitro study. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e76–e83. [Google Scholar] [CrossRef] [PubMed]
- Golob Deeb, J.; Bencharit, S.; Carrico, C.K.; Lukic, M.; Hawkins, D.; Rener-Sitar, K.; Deeb, G.R. Exploring training dental implant placement using computer-guided implant navigation system for predoctoral students: A pilot study. Eur. J. Dent. Educ. 2019, 23, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Krithikadatta, J.; Gopikrishna, V.; Datta, M. CRIS Guidelines (Checklist for Reporting In-vitro Studies): A concept note on the need for standardized guidelines for improving quality and transparency in reporting in-vitro studies in experimental dental research. J. Conserv. Dent. 2014, 17, 301–304. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kang, S.H.; Lee, J.W.; Lim, S.H.; Kim, Y.H.; Kim, M.K. Verification of the usability of a navigation method in dental implant surgery: In vitro comparison with the stereolithographic surgical guide template method. J. Oral Maxillofac. Surg. 2014, 42, 1530–1535. [Google Scholar] [CrossRef] [PubMed]
- Somogyi-Ganss, E.; Holmes, H.I.; Jokstad, A. Accuracy of a novel prototype dynamic computer-assisted surgery system. Clin. Oral Implant. Res. 2015, 26, 882–890. [Google Scholar] [CrossRef] [PubMed]
- Sun, T.M.; Lan, T.H.; Pan, C.Y.; Lee, H.E. Dental implant navigation system guide the surgery future. Kaohsiung J. Med. Sci 2018, 34, 56–64. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Operator | Coronal Deviation (mm) | Apical Deviation (mm) | Angular Deviation (°) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Edx | Edy | Edz | 3D E | Adx | Ady | Adz | 3D A | ||
| 1 | 0.77 ± 0.60 a | 0.65 ± 0.39 a | 0.88 ± 1.12 a | 1.55 ± 1.08 a | 0.73 ± 0.49 a | 0.53 ± 0.37 a | 0.72 ± 0.91 a | 1.44 ± 0.95 a | 2.93 ± 1.50 a |
| 2 | 0.84 ± 0.53 a | 0.87 ± 0.67 a | 0.85 ± 0.61 a | 1.68 ± 0.69 a | 0.53 ± 0.43 a | 0.81 ± 0.61 ab | 0.84 ± 0.66 a | 1.47 ± 0.68 a | 3.54 ± 2.33 a |
| 3 | 0.54 ± 0.42 a | 0.91 ± 0.75 a | 0.51 ± 0.40 a | 1.35 ± 0.67 a | 0.58 ± 0.44 a | 1.17 ± 0.81 b | 0.48 ± 0.40 a | 1.59 ± 0.74 a | 4.51 ± 2.74 ab |
| 4 | 0.81 ± 0.52 a | 1.06 ± 0.71 a | 0.75 ± 0.57 a | 1.74 ± 0.64 a | 1.26 ± 0.64 b | 0.84 ± 0.54 ab | 0.77 ± 0.60 a | 1.92 ± 0.51 a | 5.90 ± 2.38 b |
| Tot | 0.74 ± 0.53 | 0.87 ± 0.65 | 0.75 ± 0.74 | 1.58 ± 0.80 | 0.78 ± 0.58 | 0.84 ± 0.64 | 0.70 ± 0.67 | 1.61 ± 0.75 | 4.24 ± 2.52 |
| Operator | N | Mean (s) | Standard Deviation | Standard Error | Mean Confidence Interval 95% | Min (s) | Max (s) | |
|---|---|---|---|---|---|---|---|---|
| Lower Limit | Upper Limit | |||||||
| 1 | 28 | 43.35 a | 14.75 | 2.78 | 37.63 | 49.07 | 24.00 | 83.69 |
| 2 | 28 | 51.50 ab | 19.35 | 3.65 | 44.00 | 59.01 | 28.18 | 96.14 |
| 3 | 28 | 62.47 b | 16.97 | 3.20 | 55.89 | 69.05 | 28.74 | 95.24 |
| 4 | 28 | 58.32 b | 24.05 | 4.54 | 49.88 | 68.53 | 32.15 | 125.00 |
| Tot | 112 | 54.13 | 20.24 | 1.91 | 50.34 | 57.92 | 24.00 | 125.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pellegrino, G.; Bellini, P.; Cavallini, P.F.; Ferri, A.; Zacchino, A.; Taraschi, V.; Marchetti, C.; Consolo, U. Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience on Implant Placement Accuracy and Operating Time. An in Vitro Study. Int. J. Environ. Res. Public Health 2020, 17, 2153. https://doi.org/10.3390/ijerph17062153
Pellegrino G, Bellini P, Cavallini PF, Ferri A, Zacchino A, Taraschi V, Marchetti C, Consolo U. Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience on Implant Placement Accuracy and Operating Time. An in Vitro Study. International Journal of Environmental Research and Public Health. 2020; 17(6):2153. https://doi.org/10.3390/ijerph17062153
Chicago/Turabian StylePellegrino, Gerardo, Pierantonio Bellini, Pier Francesco Cavallini, Agnese Ferri, Andrea Zacchino, Valerio Taraschi, Claudio Marchetti, and Ugo Consolo. 2020. "Dynamic Navigation in Dental Implantology: The Influence of Surgical Experience on Implant Placement Accuracy and Operating Time. An in Vitro Study" International Journal of Environmental Research and Public Health 17, no. 6: 2153. https://doi.org/10.3390/ijerph17062153