Behavioral, Emotional and School Adjustment in Adolescents with and without Developmental Language Disorder (DLD) Is Related to Family Involvement


 ,
, 
Abstract
:1. Introduction
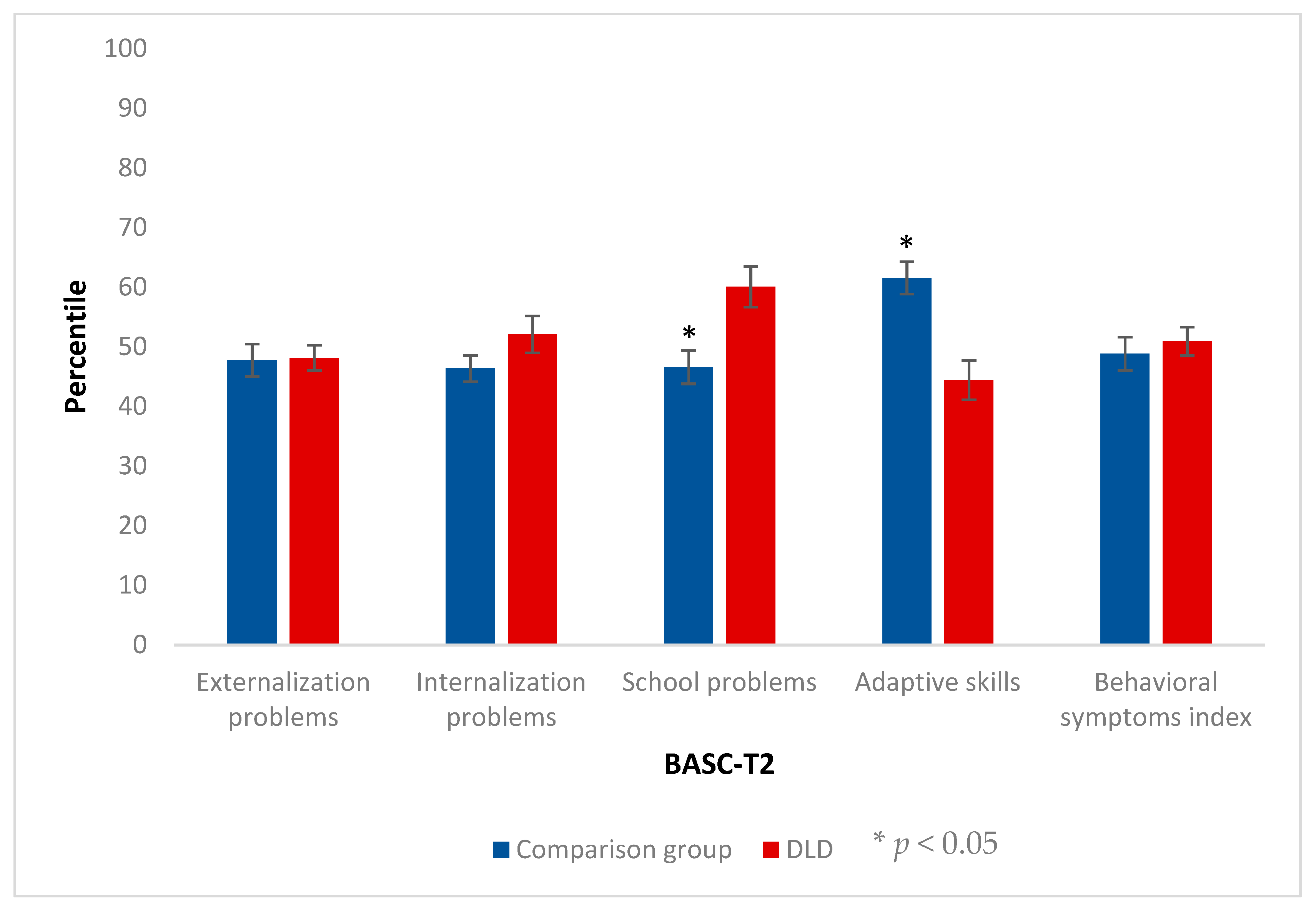
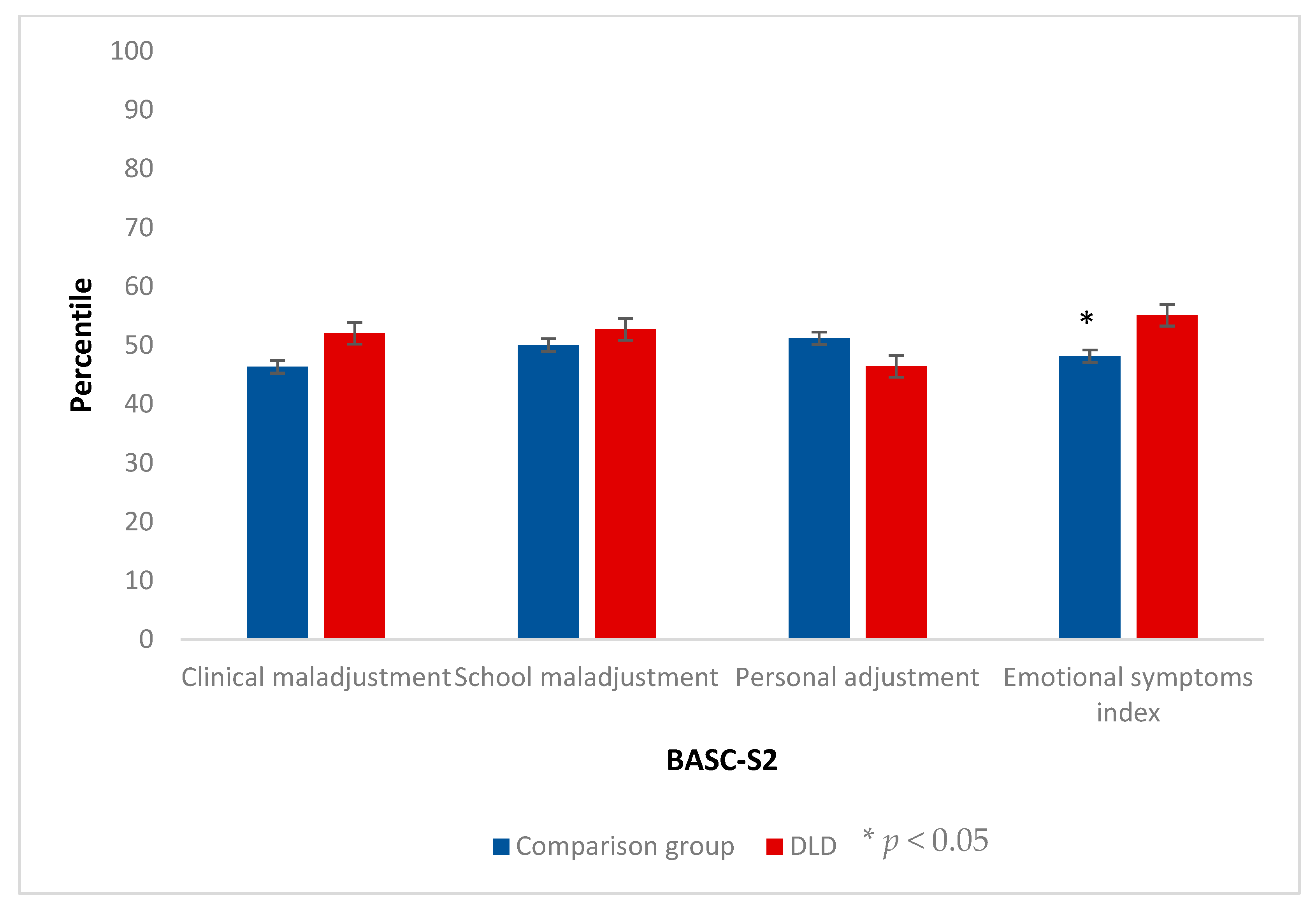
- Adolescents with DLD will present a larger number of behavioral, social and emotional problems, together with worse adaptive skills than their normative peers. This will be reflected in higher scores in the scales of the Behavior Assessment System for Children (BASC) that measure difficulties and lower scores in the scales of the BASC that measure adaptive skills, both self-reported and considering the tutor’s perspective, in contrast to the comparison group.
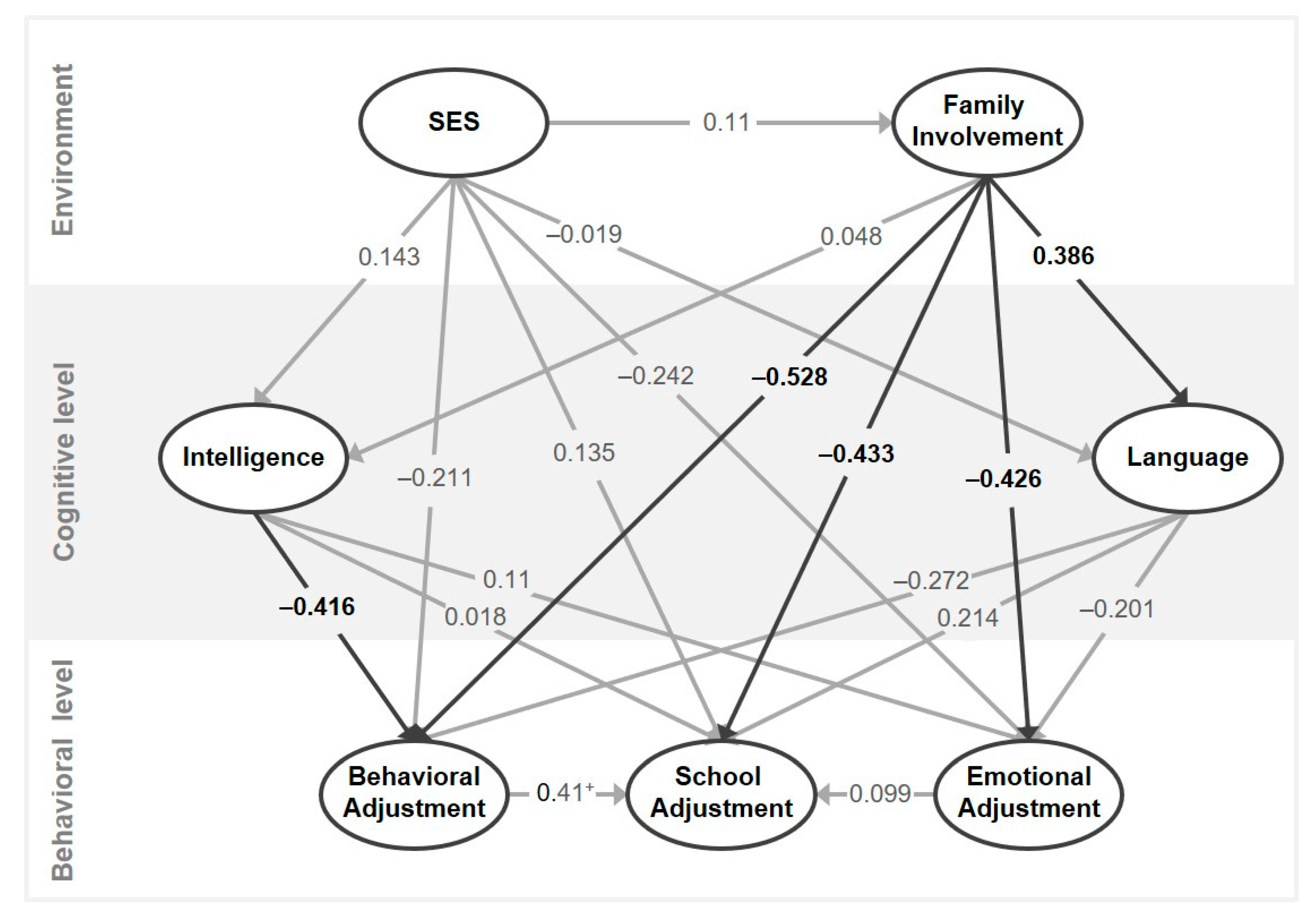
- With respect to the variables related to the family context, we expected that both SES and family involvement will emerge as protective factors against behavioral, emotional and school adjustment difficulties. Thus, we predicted a negative pattern of correlations between SES/family involvement and the variables measuring difficulties by the BASC and positive correlations between adaptive skills measured by the BASC and familiar variables, for both the self-reported version and the tutor’s version.
2. Materials and Methods
2.1. Participants
2.2. Materials
2.3. Procedure
2.3.1. Identification Phase
2.3.2. End of Follow-Up
2.4. Design and Data Analyses
3. Results
3.1. Behavioral, Emotional and School Adaptive Variables
3.2. Relation between SES and Family Involvement with Behavioral, Emotional and Adaptive Skills
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female | Male | Statistic | ||||
|---|---|---|---|---|---|---|
| Comparison Mean(SD) | DLD Mean(SD) | Comparison Mean(SD) | DLD Mean(SD) | Comparison Male-Female | DLD Male-Female | |
| n | 6 | 6 | 8 | 8 | ||
| Age at identification | 5.87 (0.27) | 5.63 (0.17) | 5.82 (0.25) | 5.82 (0.25) | U = 20 | U = 13.5 |
| Age at follow-up | 11.88 (0.27) | 11.63 (0.18) | 11.84 (0.25) | 11.81 (0.26) | U = 20 | U = 14.5 |
| SES | 2 (0.0) | 2 (0.63) | 2 (0.7) | 1.71 (0.49) | U = 12.5 | U = 16 |
| Family involvement | 4.5 (0.55) | 2.5 (1.22) | 3.87 (0.99) | 3.25 (1.28) | U = 15 | U = 15.5 |
| Language used at school | ||||||
| Catalan | 4 | 5 | 4 | 5 | ||
| Spanish | 0 | 0 | 2 | 3 | X2 = 1.75 | X2 = 1.48 |
| Bilingual | 2 | 1 | 2 | 0 | ||
| Family language | ||||||
| Catalan | 4 | 2 | 2 | 1 | ||
| Spanish | 1 | 4 | 6 | 6 | X2 = 5.05 | X2 = 3.79 |
| Bilingual | 1 | 0 | 0 | 1 | ||
| Identification phase at 5 years of age | ||||||
| Nonverbal-IQ (WPPSI) | 115.5 (11.02) | 106.83 (10.74) | 105.87 (12.11) | 98.62 (8.38) | U = 12 | U = 12.5 |
| Typical score language (PLON-R) | 59.67 (20.48) | 19.67 (9.69) | 53.12 (25.08) | 20.0 (4.14) | U = 17 | U = 19.5 |
| Language at the end of follow-up (12 years) | ||||||
| Percentile language production (SR NEPSY) | 58.33 (17.22) | 21.83 (20.2) | 62.5 (16.69) | 35.12 (23.7) | U = 19 | U = 16.5 |
| Percentile language comprehension (CEG) | 70.83 (24.98) | 41.67 (30.6) | 59.37 (23.67) | 40.0 (21.21) | U = 16.5 | U = 23 |
References
- Bishop, D.V.M.; Snowling, M.J.; Thompson, P.A.; Greenhalgh, T. CATALISE consortium CATALISE: a multinational and multidisciplinary Delphi consensus study. Identifying language impairments in children. PLoS ONE 2016, 11, e0158753. [Google Scholar] [CrossRef]
- Bishop, D.V.M.; Snowling, M.J.; Thompson, P.A.; Greenhalgh, T. CATALISE-2 consortium Phase 2 of CATALISE: A multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology. J. Child Psychol. Psychiatry 2017, 58, 1068–1080. [Google Scholar] [CrossRef]
- Leonard, L. Children with Specific Language Impairments; MIT Press: Cambridge, MA, USA, 1998. [Google Scholar]
- Font-Jordà, A.; Gamundí, A.; Nicolau Llobera, M.C.; Aguilar-Mediavilla, E. Use of the 2D:4D digit ratio as a biological marker of specific language disorders. An. Pediatría 2018, 89, 361–368. [Google Scholar] [CrossRef]
- Valera-Pozo, M.; Buil-Legaz, L.; Rigo-Carratalà, E.; Casero-Martínez, A.; Aguilar-Mediavilla, E. Habilidades sociales en preadolescentes con trastorno específico del lenguaje. Rev. Logop. Foniatría y Audiol. 2016, 36, 55–63. [Google Scholar] [CrossRef]
- Durkin, K.; Conti-Ramsden, G. Language, Social Behavior, and the Quality of Friendships in Adolescents With and Without a History of Specific Language Impairment. Child Dev. 2007, 78, 1441–1457. [Google Scholar] [CrossRef]
- Eadie, P.; Conway, L.; Hallenstein, B.; Mensah, F.; McKean, C.; Reilly, S. Quality of life in children with developmental language disorder. Int. J. Lang. Commun. Disord. 2018, 53, 799–810. [Google Scholar] [CrossRef]
- Marton, K.; Abramoff, B.; Rosenzweig, S. Social cognition and language in children with specific language impairment (SLI). J. Commun. Disord. 2005, 38, 143–162. [Google Scholar] [CrossRef] [PubMed]
- St Clair, M.C.; Pickles, A.; Durkin, K.; Conti-Ramsden, G. A longitudinal study of behavioral, emotional and social difficulties in individuals with a history of specific language impairment (SLI). J. Commun. Disord. 2011, 44, 186–199. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsay, G.; Dockrell, J.E.; Strand, S. Longitudinal patterns of behaviour problems in children with specific speech and language difficulties: Child and contextual factors. Br. J. Educ. Psychol. 2007, 77, 811–828. [Google Scholar] [CrossRef] [PubMed]
- Yew, S.G.K.; O’Kearney, R. Emotional and behavioural outcomes later in childhood and adolescence for children with specific language impairments: meta-analyses of controlled prospective studies. J. Child Psychol. Psychiatry 2013, 54, 516–524. [Google Scholar] [CrossRef] [PubMed]
- Yew, S.G.K.; O’Kearney, R. Early language impairments and developmental pathways of emotional problems across childhood. Int. J. Lang. Commun. Disord. 2015, 50, 358–373. [Google Scholar] [PubMed]
- Bakopoulou, I.; Dockrell, J.E. The role of social cognition and prosocial behaviour in relation to the socio-emotional functioning of primary aged children with specific language impairment. Res. Dev. Disabil. 2016, 49–50, 354–370. [Google Scholar] [CrossRef] [PubMed]
- Özcebe, E.; Noyan Erbas, A.; Karahan Tiğrak, T. Analysis of behavioural characteristics of children with developmental language disorders. Int. J. Speech. Lang. Pathol. 2019, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Mccabe, P.C. Social and Behavioral Correlates of Preschoolers. Psychology 2005, 42. [Google Scholar]
- Spaulding, T.J.; Plante, E.; Vance, R. Sustained selective attention skills of preschool children with specific language impairment: Evidence for separate attentional capacities. J. Speech, Lang. Hear. Res. 2008, 51, 16–34. [Google Scholar] [CrossRef]
- Aguilar-Mediavilla, E.; Buil-Legaz, L.; Pérez-Castelló, J.A.; Rigo-Carratalà, E.; Adrover-Roig, D. Early preschool processing abilities predict subsequent reading outcomes in bilingual Spanish-Catalan children with Specific Language Impairment (SLI). J. Commun. Disord. 2014, 50, 19–35. [Google Scholar] [CrossRef]
- Van den Bedem, N.P.; Dockrell, J.E.; Alphen, P.M.; Rooij, M.; Samson, A.C.; Harjunen, E.L.; Rieffe, C. Depressive symptoms and emotion regulation strategies in children with and without developmental language disorder: a longitudinal study. Int. J. Lang. Commun. Disord. 2018, 53, 1110–1123. [Google Scholar] [CrossRef]
- Durkin, K.; Conti-Ramsden, G. Young people with specific language impairment: A review of social and emotional functioning in adolescence. Child Lang. Teach. Ther. 2010, 26, 105–121. [Google Scholar] [CrossRef]
- Conti-Ramsden, G.; Botting, N. Emotional health in adolescents with and without a history of specific language impairment (SLI). J. Child Psychol. Psychiatry Allied Discip. 2008, 49, 516–525. [Google Scholar] [CrossRef]
- Conti-Ramsden, G.; Mok, P.L.H.H.; Pickles, A.; Durkin, K. Adolescents with a history of specific language impairment (SLI): Strengths and difficulties in social, emotional and behavioral functioning. Res. Dev. Disabil. 2013, 34, 4161–4169. [Google Scholar] [CrossRef]
- Voci, S.C.; Beitchman, J.H.; Brownlie, E.B.; Wilson, B. Social anxiety in late adolescence: The importance of early childhood language impairment. J. Anxiety Disord. 2006, 20, 915–930. [Google Scholar] [CrossRef] [PubMed]
- St Clair, M.C.; Forrest, C.L.; Yew, S.G.K.; Gibson, J.L. Early Risk Factors and Emotional Difficulties in Children at Risk of Developmental Language Disorder: A Population Cohort Study. J. Speech, Lang. Hear. Res. 2019, 62, 2750–2771. [Google Scholar] [CrossRef] [PubMed]
- Samson, A.C.; van den Bedem, N.P.; Dukes, D.; Rieffe, C. Positive Aspects of Emotional Competence in Preventing Internalizing Symptoms in Children with and without Developmental Language Disorder: A Longitudinal Approach. J. Autism Dev. Disord. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadman, R.; Durkin, K.; Conti-Ramsden, G. Social stress in young people with specific language impairment. J. Adolesc. 2011, 34, 421–431. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wadman, R.; Durkin, K.; Conti-Ramsden, G. Self-Esteem, Shyness, and Sociability in Adolescents With Specific Language Impairment (SLI). J. Speech, Lang. Hear. Res. 2008, 51, 938–952. [Google Scholar] [CrossRef] [Green Version]
- Lindsay, G.; Dockrell, J.; Palikara, O. Self-esteem of adolescents with specific language impairment as they move from compulsory education. Int. J. Lang. Commun. Disord. 2010, 45, 561–571. [Google Scholar] [CrossRef]
- Conti-Ramsden, G.; Mok, P.; Durkin, K.; Pickles, A.; Toseeb, U.; Botting, N. Do emotional difficulties and peer problems occur together from childhood to adolescence? The case of children with a history of developmental language disorder (DLD). Eur. Child Adolesc. Psychiatry 2019, 28, 993–1004. [Google Scholar] [CrossRef] [Green Version]
- Auza-Benavides, A.; Peñaloza, C.; Murata, C. The influence of maternal education on the linguistic abilities of monolingual Spanish-speaking children with and without Specific Language Impairment. Atyp. Lang. Dev. Roman. Lang. 2019, 93–112. [Google Scholar]
- Aguado, G. Retardo del lenguaje. In Manual de Logopedia; Peña-Casanova, J., Ed.; Elsevier-Masson: Barcelona, Spain, 2014. [Google Scholar]
- Hirsh-Pasek, K.; Adamson, L.B.; Bakeman, R.; Owen, M.T.; Golinkoff, R.M.; Pace, A.; Yust, P.K.S.; Suma, K. The Contribution of Early Communication Quality to Low-Income Children’s Language Success. Psychol. Sci. 2015, 26, 1071–1083. [Google Scholar] [CrossRef]
- Gilkerson, J.; Richards, J.A.; Warren, S.F.; Montgomery, J.K.; Greenwood, C.R.; Kimbrough Oller, D.; Hansen, J.H.L.; Paul, T.D. Mapping the Early Language Environment Using All-Day Recordings and Automated Analysis. Am. J. Speech-Language Pathol. 2017, 26, 248–265. [Google Scholar] [CrossRef]
- Romeo, R.R.; Leonard, J.A.; Robinson, S.T.; West, M.R.; Mackey, A.P.; Rowe, M.L.; Gabrieli, J.D.E. Beyond the 30-million-word gap: Children’s conversational exposure is associated with language-related brain function. Psychol. Sci. 2018, 1. [Google Scholar] [CrossRef] [PubMed]
- Durham, R.E.; Farkas, G.; Hammer, C.S.; Bruce Tomblin, J.; Catts, H.W. Kindergarten oral language skill: A key variable in the intergenerational transmission of socioeconomic status. Res. Soc. Stratif. Mobil. 2007, 25, 294–305. [Google Scholar] [CrossRef]
- Reilly, S.; Wake, M.; Ukoumunne, O.C.; Bavin, E.; Prior, M.; Cini, E.; Conway, L.; Eadie, P.; Bretherton, L. Predicting language outcomes at 4 years of age: findings from Early Language in Victoria Study. Pediatrics 2010, 126, e1530-7. [Google Scholar] [CrossRef] [PubMed]
- Manz, P.H.; Fantuzzo, J.W.; Power, T.J. Multidimensional assessment of family involvement among urban elementary students. J. Sch. Psychol. 2004, 42, 461–475. [Google Scholar] [CrossRef]
- Serna, C.; Martínez, I. Parental Involvement as a Protective Factor in School Adjustment among Retained and Promoted Secondary Students. Sustainability 2019, 11, 7080. [Google Scholar] [CrossRef] [Green Version]
- Assous, A.; Borghini, A.; Levi-Rueff, M.; Rittori, G.; Rousselot-Pailley, B.; Gosme, C.; Zigante, F.; Golse, B.; Falissard, B.; Robel, L. Children with mixed developmental language disorder have more insecure patterns of attachment. BMC Psychol. 2018, 6, 54. [Google Scholar] [CrossRef]
- Cicchetti, D.; Carlson, V. Children Maltreatment: Theory and Research on the Causes and Consequences of Child Abuse and Neglect; Cambridge University Press: Cambridge, MA, USA, 1989. [Google Scholar]
- Wairimu, M.J.; Macharia, S.M.; Muiru, A. Analysis of Parental Involvement and Self-Esteem on Secondary School Students in Kieni West Sub-County, Nyeri County, Kenya. J. Educ. Pract. 2016, 7, 82–98. [Google Scholar]
- El Nokali, N.E.; Bachman, H.J.; Votruba-Drzal, E. Parent Involvement and Children’s Academic and Social Development in Elementary School. Child Dev. 2010, 81, 988–1005. [Google Scholar] [CrossRef] [Green Version]
- Sureda García, I.; Valera-Pozo, M.; Aguilar-Mediavilla, E. Afectación del lenguaje debido a variables sociales y emocionales. In Dificultades del Lenguaje en los Trastornos del Desarrollo Vol III: Factores de Riesgo y Dificultades Comórbidas; Editorial UOC: Barcelona, Spain, 2019; pp. 23–71. [Google Scholar]
- Edwards, O.W.; Mumford, V.E.; Serra-Roldan, R. A positive youth development model for students considered at-risk. Sch. Psychol. Int. 2007, 28, 29–45. [Google Scholar] [CrossRef]
- Morton, J.B. Understanding Developmental Disorders; Blackwell Publishing: Hoboken, NJ, USA, 2004. [Google Scholar]
- Frederickson, N.; Cline, T. Special Educational Needs, Inclusion and Diversity: A Textbook; Open University Press: Buckinghan, UK, 2002. [Google Scholar]
- Durkin, K.; Conti-Ramsden, G.; Simkin, Z. Functional outcomes of adolescents with a history of specific language impairment (SLI) with and without autistic symptomatology. J. Autism Dev. Disord. 2012, 42, 123–138. [Google Scholar] [CrossRef]
- Aguinaga, G.; Armentia López de Suso, L.; Fraile, A.; Olangua, P.; Uriz, N. Prueba de Lenguaje Oral de Navarra-Revisada (PLON-R); TEA: Madrid, Spain, 2004. [Google Scholar]
- Mendoza-Lara, E.; Carballo García, G.; Muñoz, J.; Fresneda, M. CEG: Test de Comprensión de Estructuras Gramaticales; TEA Ediciones: Madrid, Spain, 2005. [Google Scholar]
- Aguilar-Alonso, Á.; Torres-Viñals, M.; Aguilar-Mediavilla, E. The first Spanish version of the NEPSY for the assessment of the neuropsychological development in a sample of Spanish children. UB J. Psychol. 2014, 44, 185–198. [Google Scholar]
- Korkman, M.; Kirk, U.; Kemp, S. NEPSY: Developmental Neuropsychological Assessment; Psychological Corp.: San Antonio, TX, USA, 1998. [Google Scholar]
- Conti-Ramsden, G.; Botting, N.; Faragher, B. Psycholinguistic markers for Specific Language Impairment (SLI). J. Child Psychol. Psychiatry 2001, 42, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Leclercq, A.-L.L.; Quémart, P.; Magis, D.; Maillart, C. The sentence repetition task: A powerful diagnostic tool for French children with specific language impairment. Res. Dev. Disabil. 2014, 35, 3423–3430. [Google Scholar] [CrossRef] [PubMed]
- Muñoz, J.; Carballo, G.; Fresneda, M.D.; Mendoza, E. Grammatical comprehension in Spanish-speaking children with Specific Language Impairment (SLI). Span. J. Psychol. 2014, 17, E45. [Google Scholar] [CrossRef] [PubMed]
- Stokes, S.F.; Wong, A.M.; Fletcher, P.; Leonard, L.B. Nonword Repetition and Sentence Repetition as Clinical Markers of Specific Language Impairment: The Case of Cantonese. J. Speech, Lang. Hear. Res. 2006, 49, 219–237. [Google Scholar] [CrossRef]
- Wechsler, D.; de la Cruz, M. V Escala de Inteligencia de Wechsler Para Preescolar y Primaria: WPPSI; TEA: Madrid, Spain, 2001. [Google Scholar]
- Reynolds, C.R.; Kamphaus, C.W. Behavior Assessment System for Children (BASC); American Guidance Services: Circle Pine, MN, USA, 1992. [Google Scholar]
- González, J.; Fernández, S.; Pérez, E.; Santamaría, P. Adaptación Española del Sistema de Evaluación de la Conducta en Niños y Adolescentes: BASC; TEA Ediciones: Madrid, España, 2004. [Google Scholar]
- Gladman, M.; Lancaster, S. A Review of the Behaviour Assessment System for Children. Sch. Psychol. Int. 2003, 24, 276–291. [Google Scholar] [CrossRef]
- Merenda, P.F. BASC: Behavior Assessment System for Children. Meas. Eval. Couns. Dev. 1996, 28, 229–232. [Google Scholar]
- MacBeth, G.; Razumiejczyk, E.; Ledsema, R. Cliff ’s Delta Calculator: A non-parametric effect size program for two groups of observations. Univ. Psychol. 2011, 10, 545–555. [Google Scholar] [CrossRef]
- Hair, J.F., Jr.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage Publications: London, UK, 2013. [Google Scholar]
- Monecke, A.; Leisch, F. SemPLS: Structural Equation Modeling using Partial Least Squares. J. Stat. Softw. 2012, 48, 1–32. [Google Scholar] [CrossRef] [Green Version]
- Hair, J.F.; Risher, J.J.; Sarstedt, M.; Ringle, C.M. When to use and how to report the results of PLS-SEM. Eur. Bus. Rev. 2019, 31, 2–24. [Google Scholar] [CrossRef]
- Ringle, C.M.; Wende, S.; Becker, J.-M. SmartPLS 3; SmartPLS: Bönningstedt, Germany, 2015; Available online: https://www.smartpls.com/ (accessed on 9 January 2020).
- Wilkins, B.; Boman, P.; Mergler, A. Positive psychological strengths and school engagement in primary school children. Cogent Educ. 2015, 2. [Google Scholar] [CrossRef] [Green Version]
- Aguilar-Mediavilla, E.; Buil-Legaz, L.; López-Penadés, R.; Sánchez-Azanza, V.A.; Adrover-Roig, D. Academic outcomes in bilingual children with developmental language disorder: a longitudinal study. Front. Psychol. 2019, 10, 1–17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conti-Ramsden, G.; Durkin, K.; Simkin, Z.; Knox, E. Specific language impairment and school outcomes. I: Identifying and explaining variability at the end of compulsory education. Int. J. Lang. Commun. Disord. 2010, 44, 15–35. [Google Scholar] [CrossRef]
- Menting, B.; van Lier, P.A.C.; Koot, H.M. Language skills, peer rejection, and the development of externalizing behavior from kindergarten to fourth grade. J. Child Psychol. Psychiatry 2011, 52, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Nelson, J.M.; Harwood, H. Learning disabilities and anxiety: A meta-analysis. J. Learn. Disabil. 2011, 44, 3–17. [Google Scholar] [CrossRef] [PubMed]
- Ackerman, B.P.; Izard, C.E.; Kobak, R.; Brown, E.D.; Smith, C. Relation between reading problems and internalizing behavior in school for preadolescent children from economically disadvantaged families. Child Dev. 2007, 78, 581–596. [Google Scholar] [CrossRef] [PubMed]
- Economía y datos de los países. 2019. Available online: https://datosmacro.expansion.com/paises (accessed on 27 November 2019).
- Lisa, R.; Pola, R.; Franz, P.; Jessica, M. Developmental language disorder: Maternal stress level and behavioural difficulties of children with expressive and mixed receptive-expressive DLD. J. Commun. Disord. 2019, 80, 1–10. [Google Scholar] [CrossRef]




| Comparison Group | DLD | Statistic and p | ||
|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||
| n | 14 | 14 | ||
| Age at identification | 5.85 (0.25) | 5.74 (0.24) | U = 68.5, p = 0.171 | |
| Age at follow-up | 11.85 (0.25) | 11.74 (0.24) | U = 66.5, p = 0.143 | |
| SES | 2 (0.47) | 1.85 (0.55) | U = 56, p = 0.468 | |
| Family involvement | 4.14 (0.83) | 2.93 (1.27) | U = 44, p = 0.011 | |
| Gender | ||||
| Male | 8 | 8 | X2 = 0.00, p = 1.00 | |
| Female | 6 | 6 | ||
| Language used at school | ||||
| Catalan | 8 | 10 | X2 = 2.22, p = 0.329 | |
| Spanish | 2 | 3 | ||
| Bilingual | 4 | 1 | ||
| Family language | ||||
| Catalan | 6 | 3 | X2 = 1.53, p = 0.465 | |
| Spanish | 7 | 10 | ||
| Bilingual | 1 | 1 | ||
| Identification phase at 5 years of age | ||||
| Nonverbal-IQ (WPPSI) | 110 (12.2) | 102.1 (9.9) | U = 63.5, p = 0.112. | |
| Typical score language (PLON-R) | 55.9 (22.6) | 19.8 (6.7) | U = 0.00, p < 0.000 | |
| Language at the end of follow-up (12 years) | ||||
| Percentile language production (SR NEPSY) | 60.7 (16.4) | 29.4 (22.4) | U = 30.5, p = 0.002 | |
| Percentile language comprehension (CEG) | 64.3 (24.0) | 40.7 (24.5) | U = 52.0, p = 0.033 | |
| Both Groups | Comparison Group | DLD Group | ||||
|---|---|---|---|---|---|---|
| SES | Family Involvement | SES | Family Involvement | SES | Family Involvement | |
| Tutor form | ||||||
| Externalization problems | -0.22 | −0.05 | −0.47 | −0.005 | −0.01 | −0.16 |
| Internalization problems | −0.20 | −0.36 * | −0.31 | −0.36 | −0.15 | −0.54 |
| School problems | −0.02 | −0.58 ** | 0.23 | −0.58* | −0.24 | −0.69 ** |
| Adaptive skills | 0.18 | 0.42 ** | −0.23 | 0.37 | 0.44 | 0.31 |
| BSI | −0.24 | −0.46 * | −0.18 | −0.46 | −0.23 | −0.61 * |
| Subject form | ||||||
| Clinical maladjustment | -0.01 | −0.18 | 0.23 | −0.18 | −0.36 | −0.16 |
| School maladjustment | -0.01 | −0.04 | 0.60 | −0.17 | −0.30 | 0.11 |
| Personal adjustment | 0.21 | 0.34 * | 0.00 | 0.65 * | 0.53 | 0.36 |
| ESI | −0.16 | −0.36 * | −0.08 | −0.42 | −0.41 | −0.45 |
| Measurement Model | Structural Model | |||||
|---|---|---|---|---|---|---|
| Indicator Loads | ||||||
| Load | p | A | AVE | VIF | R2 | |
| Environment level | ||||||
| SES | 1 | <0.001 | 1 | 1 | 1 | |
| Family Involvement | 1 | <0.001 | 1 | 1 | 1 | 0.012 |
| Cognitive level | ||||||
| Intelligence (WPPSI) | 1 | <0.001 | 1 | 1 | 1 | 0.024 |
| Language | 0.72 | 0.63 | 0.148 | |||
| Grammar comprehension (CEG) | 0.682 | 0.205 | 1.34 | |||
| Sentence production (SR, NEPSY) | 0.869 | <0.001 | 1.43 | |||
| PLON-R | 0.822 | 0.002 | 1.49 | |||
| Behavioral level | ||||||
| Behavioral adjustment | 1 | <0.001 | 1 | 1 | 1 | 0.428 |
| School adjustment | 1 | <0.001 | 1 | 1 | 1 | 0.703 |
| Emotional adjustment | 1 | <0.001 | 1 | 1 | 1 | 0.348 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Valera-Pozo, M.; Adrover-Roig, D.; Pérez-Castelló, J.A.; Sanchez-Azanza, V.A.; Aguilar-Mediavilla, E. Behavioral, Emotional and School Adjustment in Adolescents with and without Developmental Language Disorder (DLD) Is Related to Family Involvement. Int. J. Environ. Res. Public Health 2020, 17, 1949. https://doi.org/10.3390/ijerph17061949
Valera-Pozo M, Adrover-Roig D, Pérez-Castelló JA, Sanchez-Azanza VA, Aguilar-Mediavilla E. Behavioral, Emotional and School Adjustment in Adolescents with and without Developmental Language Disorder (DLD) Is Related to Family Involvement. International Journal of Environmental Research and Public Health. 2020; 17(6):1949. https://doi.org/10.3390/ijerph17061949
Chicago/Turabian StyleValera-Pozo, Mario, Daniel Adrover-Roig, Josep A. Pérez-Castelló, Victor A. Sanchez-Azanza, and Eva Aguilar-Mediavilla. 2020. "Behavioral, Emotional and School Adjustment in Adolescents with and without Developmental Language Disorder (DLD) Is Related to Family Involvement" International Journal of Environmental Research and Public Health 17, no. 6: 1949. https://doi.org/10.3390/ijerph17061949