Examination of Transition Readiness, Medication Adherence, and Resilience in Pediatric Chronic Illness Populations: A Pilot Study

Abstract
:1. Introduction
2. Methods
2.1. Study Design and Participants
2.2. Measures
2.3. Data Analytic Plan
3. Results
3.1. Description of Sample
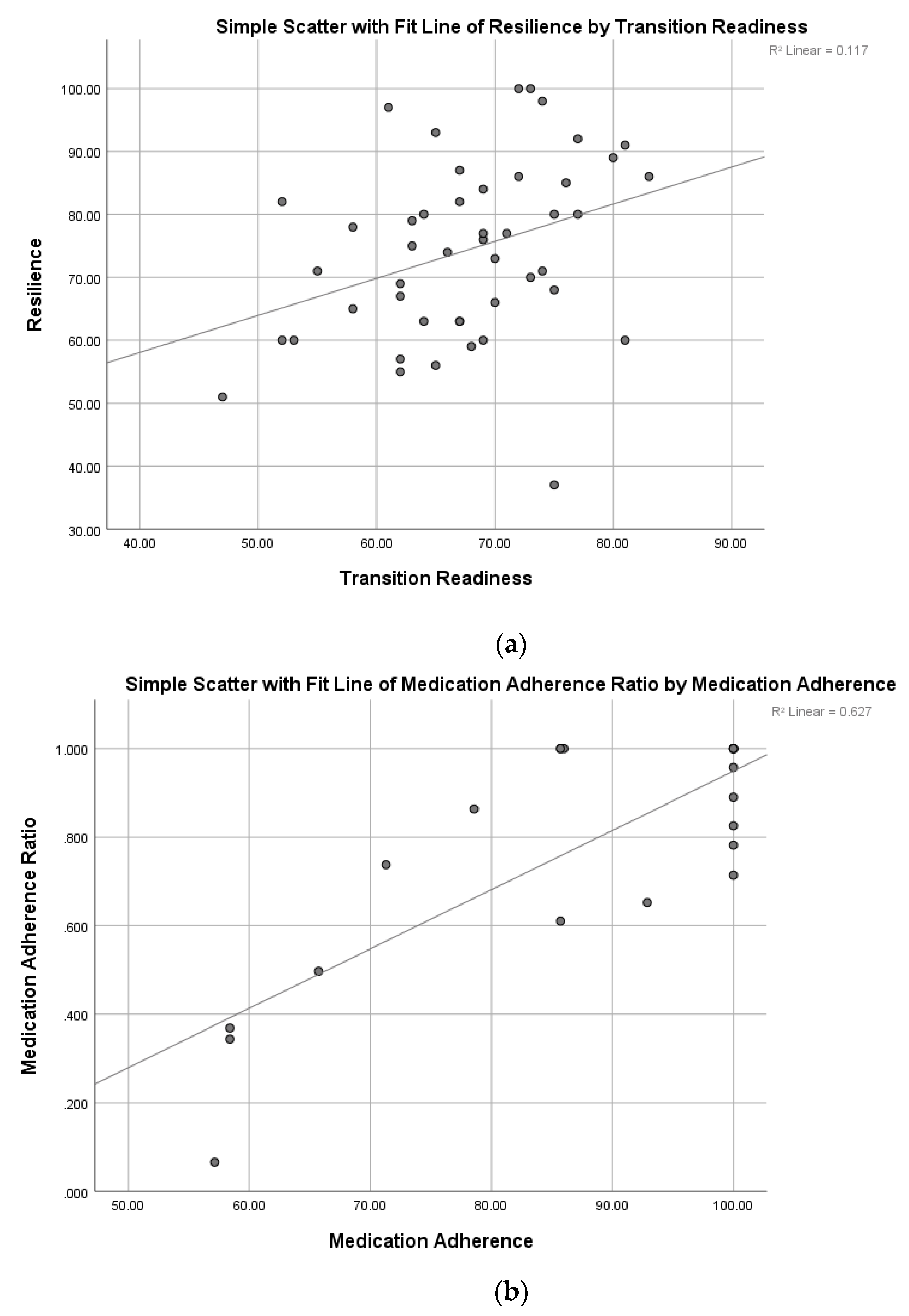
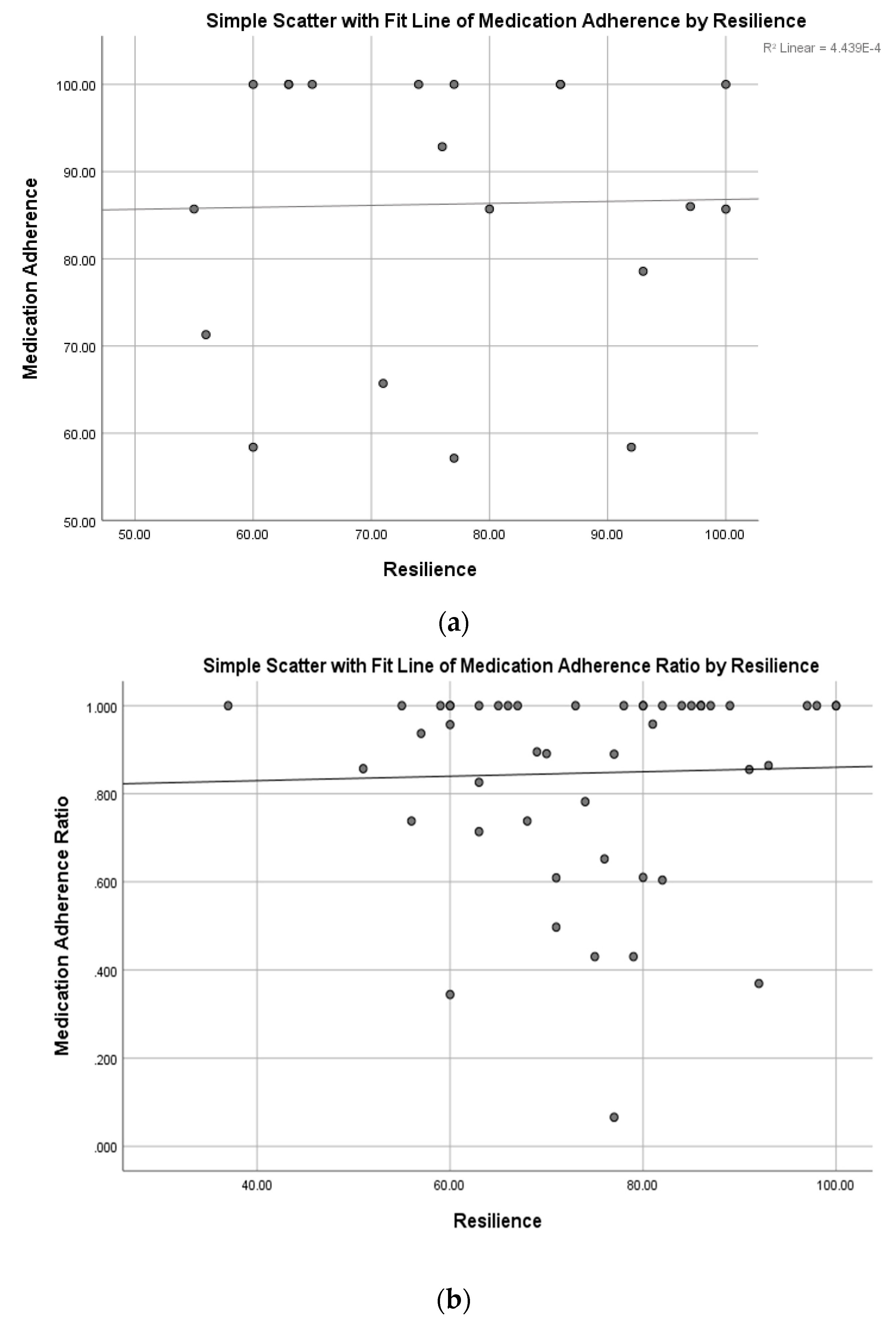
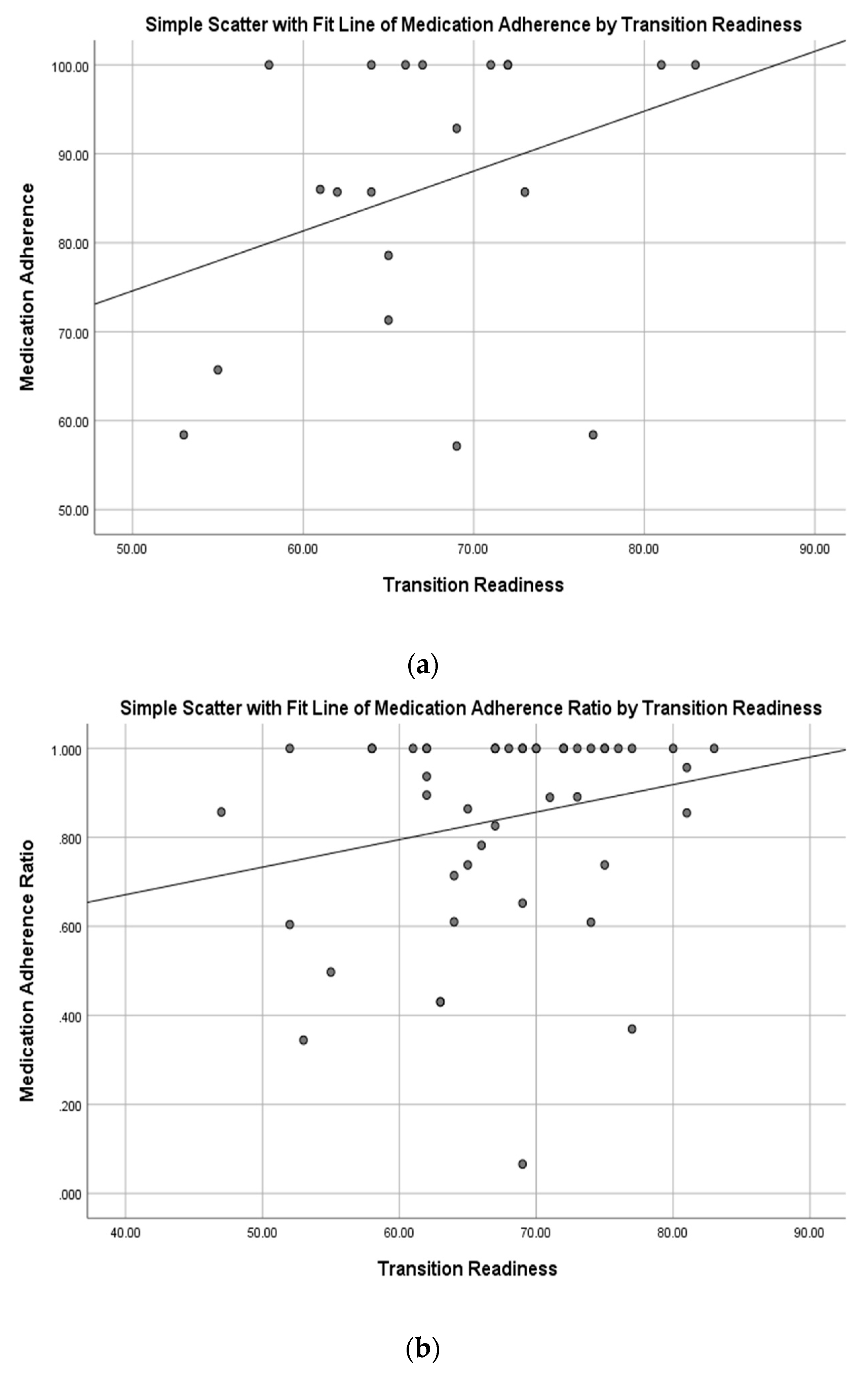
3.2. Multivariate Correlation Analysis
3.3. Regression Analysis
3.4. Mediation Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Britto, M.T.; DeVellis, R.F.; Hornung, R.W.; DeFriese, G.H.; Atherton, H.D.; Slap, G.B. Health care preferences and priorities of adolescents with chronic illnesses. Pediatrics 2004, 114, 1272–1280. [Google Scholar] [CrossRef]
- Sawyer, S.M.; Drew, S.; Yeo, M.S.; Britto, M.T. Adolescents with a chronic condition: Challenges living, challenges treating. Lancet 2007, 369, 1481–1489. [Google Scholar] [CrossRef]
- Tong, A.; Henning, P.; Wong, G.; McTaggart, S.; Mackie, F.; Carroll, R.P.; Craig, J.C. Experiences and perspectives of adolescents and young adults with advanced CKD. Am. J. Kidney Dis. 2013, 61, 375–384. [Google Scholar] [CrossRef]
- Modi, A.C.; Pai, A.L.; Hommel, K.A.; Hood, K.K.; Cortina, S.; Hilliard, M.E.; Guilfoyle, S.M.; Gray, W.N.; Drotar, D. Pediatric self-management: A frameword for research, practice, and policy. Pediatrics 2012, 14, e473–e485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anderson, B.J.; Holmbeck, G.; Iannotti, R.J.; McKay, S.V.; Lochrie, A.; Volkening, L.K.; Laffel, L. Dyadic measures of the parent–child relationship during the transition to adolescence and glycemic control in children with type 1 diabetes. Fam. Syst. Health 2009, 27, 141. [Google Scholar] [CrossRef] [PubMed]
- Annunziato, R.A.; Emre, S.; Shneider, B.; Barton, C.; Dugan, C.A.; Shemesh, E. Adherence and medical outcomes in pediatric liver transplant recipients who transition to adult services. Pediatr. Transplant. 2007, 11, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Annunziato, R.A.; Emre, S.; Shneider, B.L.; Dugan, C.A.; Aytaman, Y.; McKay, M.M.; Shemesh, E. Transitioning health care responsibility from caregivers to patient: A pilot study aiming to facilitate medication adherence during this process. Pediatr. Transplant. 2008, 12, 309–315. [Google Scholar] [CrossRef] [PubMed]
- Buford, T.A. Transfer of asthma management responsibility from parents to their school-age children. J. Pediatr. Nurs. 2004, 19, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Carlsen, K.; Haddad, N.; Gordon, J.; Phan, B.L.; Pittman, N.; Benkov, K.; Dubinsky, M.C.; Keefer, L. Self-efficacy and resilience are useful predictors of transition readiness scores in adolescents with inflammatory bowel diseases. Inflamm. Bowel Dis. 2017, 23, 341–346. [Google Scholar] [CrossRef]
- Cohen, S.E.; Hooper, S.R.; Javalkar, K.; Haberman, C.; Fenton, N.; Lai, H.; Mahan, J.D.; Massengill, S.; Kelly, M.; Cantú, G. Self-management and transition readiness assessment: Concurrent, predictive and discriminant validation of the STARx questionnaire. J. Pediatr. Nurs. 2015, 30, 668–676. [Google Scholar] [CrossRef]
- Fenton, N.; Ferris, M.; Ko, Z.; Javalkar, K.; Hooper, S.R. The relationship of health care transition readiness to disease-related characteristics, psychosocial factors, and health care outcomes: Preliminary findings in adolescents with chronic kidney disease. J. Pediatr. Rehabil. Med. 2015, 8, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Steinbeck, K.S.; Brodie, L.; Towns, S.J. Transition in chronic illness: Who is going where? J. Paediatr. Child Health 2008, 44, 478–482. [Google Scholar] [CrossRef]
- Pai, A.L.; Ostendorf, H.M. Treatment adherence in adolescents and young adults affected by chronic illness during the health care transition from pediatric to adult health care: A literature review. Child. Health Care 2011, 40, 16–33. [Google Scholar] [CrossRef]
- Tuchman, L.K.; Slap, G.; Britto, M. Transition to adult care: Experiences and expectations of adolescents with a chronic illness. Child Care Health Dev. 2008, 34, 557–563. [Google Scholar] [CrossRef] [PubMed]
- DeNisco, S. Exploring the relationship between resilience and diabetes outcomes in African Americans. J. Am. Acad. Nurse Pract. 2011, 23, 602–610. [Google Scholar] [CrossRef]
- Yi-Frazier, J.P.; Yaptangco, M.; Semana, S.; Buscaino, E.; Thompson, V.; Cochrane, K.; Tabile, M.; Alving, E.; Rosenberg, A.R. The association of personal resilience with stress, coping, and diabetes outcomes in adolescents with type 1 diabetes: Variable-and person-focused approaches. J. Health Psychol. 2015, 20, 1196–1206. [Google Scholar] [CrossRef] [Green Version]
- Burt, K.B.; Paysnick, A.A. Resilience in the transition to adulthood. Dev. Psychopathol. 2012, 24, 493–505. [Google Scholar] [CrossRef]
- Traub, F.; Boynton-Jarrett, R. Modifiable resilience factors to childhood adversity for clinical pediatric practice. Pediatrics 2017, 139, e20162569. [Google Scholar] [CrossRef]
- Ernst, M.M.; Mellon, M.W. Acceptance and commitment therapy (ACT) to foster resilience in pediatric chronic illness. In Child and Adolescent Resilience Within Medical Contexts; Springer: New York, NY, USA, 2016; pp. 193–207. [Google Scholar]
- Mullins, L.L.; Molzon, E.S.; Suorsa, K.I.; Tackett, A.P.; Pai, A.L.; Chaney, J.M. Models of resilience: Developing psychosocial interventions for parents of children with chronic health conditions. Fam. Relat. 2015, 64, 176–189. [Google Scholar] [CrossRef]
- Hilliard, M.E.; McQuaid, E.L.; Nabors, L.; Hood, K.K. Resilience in Youth and Families Living with Pediatric Health and Developmental Conditions: Introduction to the Special Issue on Resilience; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Hamall, K.M.; Heard, T.R.; Inder, K.J.; McGill, K.M.; Kay-Lambkin, F. The Child Illness and Resilience Program (CHiRP): A study protocol of a stepped care intervention to improve the resilience and wellbeing of families living with childhood chronic illness. BMC Psychol. 2014, 2, 5. [Google Scholar] [CrossRef] [Green Version]
- Seligman, M.E. Building resilience. Harv. Bus. Rev. 2011, 89, 100–106. [Google Scholar] [PubMed]
- Luthar, S.S.; Cicchetti, D.; Becker, B. The construct of resilience: A critical evaluation and guidelines for future work. Child Dev. 2000, 71, 543–562. [Google Scholar] [CrossRef] [PubMed]
- Wagnild, G. A review of the Resilience Scale. J. Nurs. Meas. 2009, 17, 105–113. [Google Scholar] [CrossRef] [PubMed]
- Reiss, J.G.; Gibson, R.W.; Walker, L.R. Health care transition: Youth, family, and provider perspectives. Pediatrics 2005, 115, 112–120. [Google Scholar] [CrossRef] [PubMed]
- Stern, M.; Russell, C.; Lamanna, J.; Bitsko, M.; Godder, K.; Mazzeo, S.; Thompson, A.; Ewing, L. Promoting healthy transitions for children coming off active cancer treatment. In Proceedings of the Society for International Oncology in Pediatrics, Boston, MA, USA, 15 October 2010. [Google Scholar]
- Weissberg-Benchell, J.; Wolpert, H.; Anderson, B.J. Transitioning from pediatric to adult care: A new approach to the post-adolescent young person with type 1 diabetes. Diabetes Care 2007, 30, 2441–2446. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Drotar, D.; Rohan, J.M. Pediatric Adherence and Health Behavior Change. In The Oxford Handbook of Health Communication, Behavior Change, and Treatment Adherence; Martin, L.R., DiMatteo, M.R., Eds.; Oxford University Press: New York, NY, USA, 2013; pp. 387–407. [Google Scholar]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson resilience scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Jorgensen, I.E.; Seedat, S. Factor Structure of the Connor-Davidson Resilience Scale in South African Adolescents; De Gruyter: Berlin, Germany, 2008. [Google Scholar]
- Perera, H.N.; Ganguly, R. Construct validity of scores from the connor–davidson resilience scale in a sample of postsecondary students with disabilities. Assessment 2018, 25, 193–205. [Google Scholar] [CrossRef] [Green Version]
- Yu, X.-N.; Lau, J.T.; Mak, W.W.; Zhang, J.; Lui, W.W. Factor structure and psychometric properties of the Connor-Davidson Resilience Scale among Chinese adolescents. Compr. Psychiatry 2011, 52, 218–224. [Google Scholar] [CrossRef]
- Zelikovsky, N.; Schast, A.P.; Palmer, J.A.; Meyers, K.E.C. Perceived barriers to adherence among adolescent renal transplant candidates. Pediatr. Transplant. 2008, 12, 300–308. [Google Scholar] [CrossRef]
- Zelikovsky, N.; Schast, A.P. Eliciting accurate reports of adherence in a clinical interview: Development of the Medical Adherence Measure. Pediatr. Nurs. 2008, 34, 143–146. [Google Scholar]
- Lam, W.Y.; Fresco, P. Medication adherence measures: An overview. BioMed Res. Int. 2015, 2015, 217047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riekert, K.A.; Drotar, D. Adherence to medical treatment in pediatric chronic illness: Critical issues and unanswered questions. In Promoting Adherence to Medical Treatment in Childhood Chronic Illness: Concepts, Methods, and Interventions; Drotar, D., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2000; pp. 3–32. [Google Scholar]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach; Guilford Publications: New York, NY, USA, 2017. [Google Scholar]
- Gerson, A.C.; Wentz, A.; Abraham, A.G.; Mendley, S.R.; Hooper, S.R.; Butler, R.W.; Gipson, D.S.; Lande, M.B.; Shinnar, S.; Moxey-Mims, M.M. Health-related quality of life of children with mild to moderate chronic kidney disease. Pediatrics 2010, 125, e349–e357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hilliard, M.; Harris, M.; Weissberg-Benchell, J. Diabetes resilience: A model of risk and protection in type 1 diabetes. Curr. Diab. Rep. 2012, 12, 739–748. [Google Scholar] [CrossRef] [PubMed]
- DiMatteo, M.R.; Giordani, P.J.; Lepper, H.S.; Croghan, T.W. Patient adherence and medical treatment outcomes: A meta-analysis. Med. Care 2002, 40, 794–811. [Google Scholar] [CrossRef]
- DiMatteo, M.R.; Haskard, K.B. Further challenges in adherence research: Measurements, methodologies, and mental health care. Med. Care 2006, 44, 297–299. [Google Scholar] [CrossRef]
- Martin, L.R.; Haskard-Zolnierek, K.B.; DiMatteo, M.R. Health Behavior Change and Treatment Adherence: Evidence-Based Guidelines for Improving Healthcare; Oxford University Press: New York, NY, USA, 2010. [Google Scholar]
- Kogon, A.J.; Vander Stoep, A.; Weiss, N.S.; Smith, J.; Flynn, J.T.; McCauley, E. Depression and its associated factors in pediatric chronic kidney disease. Pediatr. Nephrol. 2013, 28, 1855–1861. [Google Scholar] [CrossRef] [Green Version]
- DiMatteo, M.R.; Lepper, H.S.; Croghan, T.W. Depression is a risk factor for noncompliance with medical treatment: Meta-analysis of the effects of anxiety and depression on patient adherence. Arch. Intern. Med. 2000, 160, 2101–2107. [Google Scholar] [CrossRef]
- Moreira, J.M.; Soares, C.M.B.M.; Teixeira, A.L.; Silva, A.C.S.; Kummer, A.M. Anxiety, depression, resilience and quality of life in children and adolescents with pre-dialysis chronic kidney disease. Pediatr. Nephrol. 2015, 30, 2153–2162. [Google Scholar] [CrossRef]
- DiMatteo, M.R. Practitioner-family-patient communication in pediatric adherence: Implications for research and clinical practice. In Promoting Adherence to Treatment in Medical Treatment in Chronic Illness: Concepts, Methods, and Interventions; Drotar, D., Ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 2000; pp. 237–258. [Google Scholar]
- Tian, X.; Gao, Q.; Li, G.; Zou, G.; Liu, C.; Kong, L.; Li, P. Resilience is associated with low psychological distress in renal transplant recipients. Gen. Hosp. Psychiatry 2016, 39, 86–90. [Google Scholar] [CrossRef]
- Campbell-Sills, L.; Cohan, S.L.; Stein, M.B. Relationship of resilience to personality, coping, and psychiatric symptoms in young adults. Behav. Res. Ther. 2006, 44, 585–599. [Google Scholar] [CrossRef]
- Seligman, M.E.; Ernst, R.M.; Gillham, J.; Reivich, K.; Linkins, M. Positive education: Positive psychology and classroom interventions. Oxf. Rev. Educ. 2009, 35, 293–311. [Google Scholar] [CrossRef]
- Sharma, V.; Sood, A.; Prasad, K.; Loehrer, L.; Schroeder, D.; Brent, B. Bibliotherapy to decrease stress and anxiety and increase resilience and mindfulness: A pilot trial. Explor. J. Sci. Health 2014, 10, 248–252. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Child’s/adolescent’s age at baseline (years), M ± SD (range) | 17.3 ± 2.1 years (13.1–22.6 years) |
|---|---|
| Type of diagnosis, n (%) | |
| Nephrology | 31 (62%) |
| Rheumatology | 7 (14%) |
| Hematology | 5 (10%) |
| Oncology | 7 (14%) |
| Duration of diagnosis (years), M ± SD (range) | 6.15 ± 5.0 |
| Child’s gender, n (%) | |
| Male | 21 (42%) |
| Female | 29 (58%) |
| Child’s ethnicity/race, n (%) | |
| Non-Hispanic, Caucasian | 17 (34%) |
| Non-Hispanic, minority | 30 (60%) |
| Hispanic | 3 (6%) |
| Scored measures (M ± SD) | |
| Resilience | 74.67 ± 13.95 |
| Transition readiness | 67.55 ± 8.20 |
| Medication adherence | 86.27% ± 15.98 |
| Medication adherence ratio (pharmacy refill) | 0.84 ± 0.23 |
| Resilience | Transition Readiness | Self-Reported Medication Adherence | Medication Adherence Ratio | |
|---|---|---|---|---|
| Resilience | 1.00 | |||
| Transition readiness | 0.34 * | 1.00 | ||
| Self-reported medication adherence | 0.02 | 0.33 | 1.00 | |
| Medication adherence ratio | 0.03 | 0.22 | 0.79 ** | 1.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verma, T.; Rohan, J. Examination of Transition Readiness, Medication Adherence, and Resilience in Pediatric Chronic Illness Populations: A Pilot Study. Int. J. Environ. Res. Public Health 2020, 17, 1905. https://doi.org/10.3390/ijerph17061905
Verma T, Rohan J. Examination of Transition Readiness, Medication Adherence, and Resilience in Pediatric Chronic Illness Populations: A Pilot Study. International Journal of Environmental Research and Public Health. 2020; 17(6):1905. https://doi.org/10.3390/ijerph17061905
Chicago/Turabian StyleVerma, Tanvi, and Jennifer Rohan. 2020. "Examination of Transition Readiness, Medication Adherence, and Resilience in Pediatric Chronic Illness Populations: A Pilot Study" International Journal of Environmental Research and Public Health 17, no. 6: 1905. https://doi.org/10.3390/ijerph17061905